Toe to Ankle Disarticulation
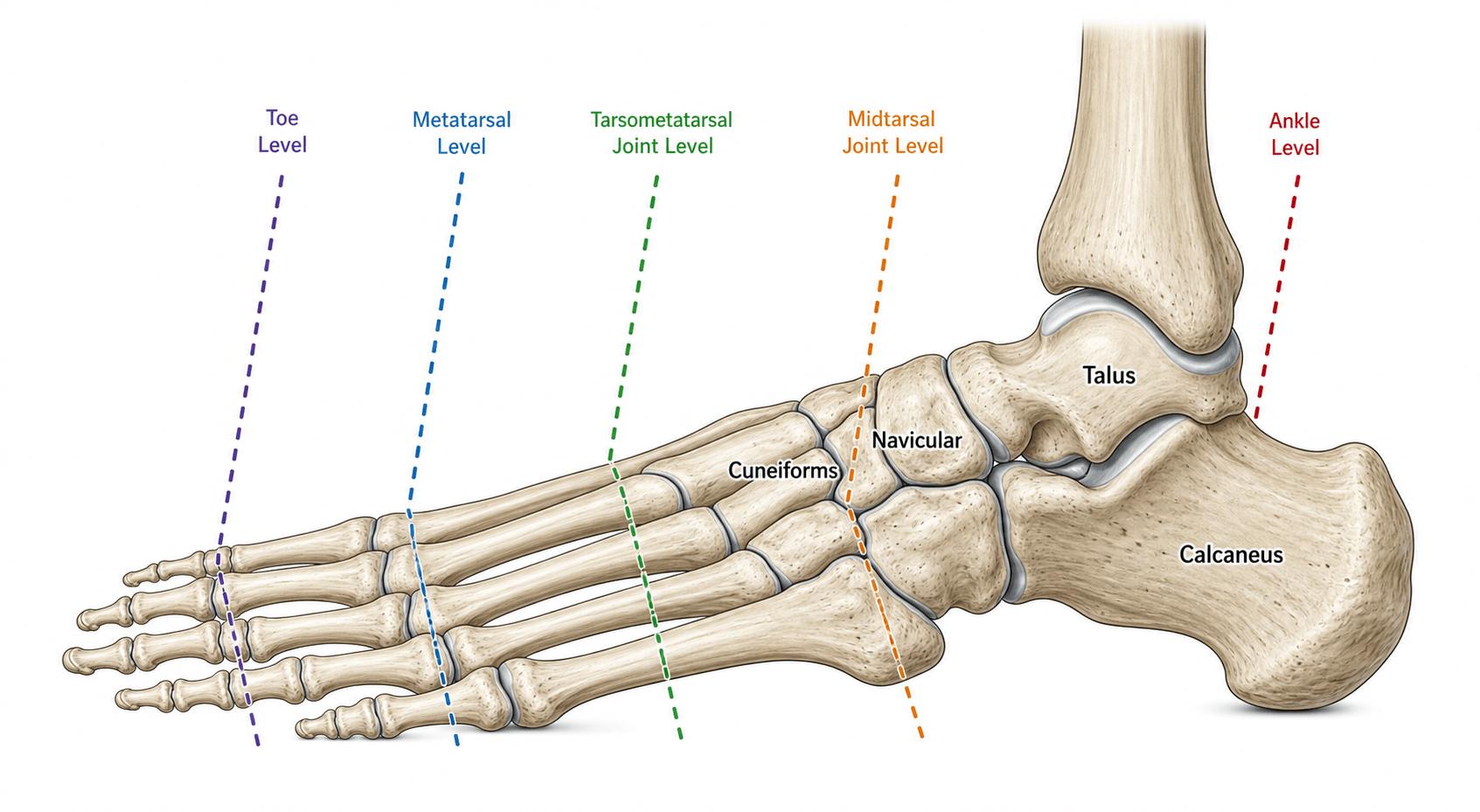
- Partial foot amputation levels from distal to proximal: toe, ray, transmetatarsal (TMA), Lisfranc (tarsometatarsal), Chopart (midtarsal), then ankle disarticulation (Syme) and the calcaneo-tibial Pirogoff/Boyd.
- The principle is to preserve as much functional, durably-healing, end-bearing length as possible.
- Proximal partial-foot amputations (Chopart, and to a lesser extent Lisfranc) lose the dorsiflexors and everters, creating a strong EQUINOVARUS deformity that must be rebalanced (tendo-Achilles lengthening +/- tibialis anterior tendon transfer).
- A Syme amputation depends on a viable, well-anchored HEEL PAD for an end-bearing stump.
- Healing is the dominant concern in dysvascular/diabetic feet; partial foot amputation has high rates of delayed healing and ipsilateral reamputation.
- Compared with transtibial amputation, partial foot amputation has similar quality of life and mobility, while transtibial carries higher mortality (reflecting sicker patients).
- “Chopart amputation classically drifts into equinovarus - plan rebalancing (Achilles lengthening, TA transfer) at the time of surgery.
- “A durable Syme needs the heel pad securely anchored under the tibia and a patent posterior tibial artery.
- “Reamputation is common after partial foot amputation in the dysvascular/diabetic foot - counsel accordingly.
As the amputation moves proximally (Lisfranc → Chopart), the dorsiflexor (tibialis anterior, long extensors) and everter (peroneal) insertions are lost, leaving the intact triceps surae and tibialis posterior unopposed. The result is a powerful equinovarus deformity that ulcerates the stump if not corrected.
Rebalance at the index operation: tendo-Achilles lengthening (to counter equinus) and, for Chopart, tibialis anterior tendon transfer to the talus/midfoot (to restore dorsiflexion). Failure to rebalance is the classic reason a Chopart amputation fails.
The Levels
Forefoot Levels
- Toe amputation: for isolated digital gangrene/osteomyelitis; well tolerated. Loss of the great toe most affects push-off and balance.
- Ray amputation: toe + its metatarsal (e.g. for deep infection tracking up a ray). Border rays (1st, 5th) tolerate ray resection well; central rays narrow the foot.
- Transmetatarsal amputation (TMA): division across all metatarsals (ideally leaving a slightly longer first metatarsal). Good functional level; preserve a robust plantar flap and lengthen the Achilles if there is equinus to prevent forefoot pressure on the stump.
Principles & Decision-Making
Three competing goals govern level selection: preserve functional length (better gait, less energy cost, end-bearing), ensure the wound heals (vascular supply, infection control, soft-tissue coverage), and maintain muscle balance (avoid equinovarus). The most distal level that will reliably heal and stay balanced is usually best.
- Healing assessment: vascular status (pulses, ankle-brachial/toe pressures, transcutaneous oxygen), nutritional and glycaemic optimisation, and infection control are decisive in the dysvascular/diabetic foot.
- Soft tissue: a durable, sensate, well-vascularised plantar/heel flap is the goal; the plantar skin is the ideal weight-bearing surface.
- Balance: plan tendon rebalancing (Achilles lengthening, tibialis anterior transfer) for proximal partial-foot levels.
- The partial-foot vs transtibial decision: when a partial foot amputation is unlikely to heal or remain functional, a transtibial amputation with a good prosthesis may give better, more predictable function - a genuine shared decision.

TRTLCSPartial Foot Levels (distal → proximal)
Hook:Toe, Ray, TMA, Lisfranc, Chopart, Syme - more proximal = more equinovarus.
Evidence Base
Outcomes of Partial Foot vs Transtibial Amputation
- Systematic review of 29 studies on dysvascular partial foot amputation (PFA) versus transtibial amputation (TTA)
- A large proportion of PFA patients experience delayed wound healing and ipsilateral reamputation
- TTA carries higher mortality than PFA - likely reflecting more advanced systemic disease in TTA candidates
- Mobility and quality of life may be similar between PFA and TTA
Quality of Life: Partial Foot vs Transtibial
- Systematic review comparing quality of life in partial foot versus transtibial amputation
- Available evidence suggests quality of life may be similar between the two levels
- Small differences are unlikely to be clinically meaningful
- Evidence is limited - level decisions should be individualised
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient who had a Chopart amputation returns with an ulcer over the front of the stump and the foot pointing down and in. What has happened and how is it prevented/treated?”
Guidelines, Registries & Global Practice
Global Practice Picture
Partial foot amputation is performed worldwide, most often for the dysvascular/diabetic foot. The internationally consistent principles are: choose the most distal level that will reliably heal and stay balanced; rebalance proximal partial-foot levels to prevent equinovarus; secure a durable plantar/heel weight-bearing surface; and frame the partial-foot-versus-transtibial choice as a shared decision based on heal-ability and function.
Side-by-Side Synthesis
- Joint/bone
- Digit / metatarsal
- Key issue
- Great-toe loss affects push-off
- Joint/bone
- Across metatarsals
- Key issue
- Achilles lengthening for equinus
- Joint/bone
- Tarsometatarsal
- Key issue
- Early equinovarus tendency
- Joint/bone
- Midtarsal
- Key issue
- Strong equinovarus - rebalance (Achilles + TA transfer)
- Joint/bone
- Ankle disarticulation
- Key issue
- Heel pad-dependent, end-bearing
- Joint/bone
- Calcaneo-tibial fusion
- Key issue
- Durable end-bearing stump
Levels (distal → proximal)
- Toe / Ray
- Transmetatarsal (TMA)
- Lisfranc (tarsometatarsal)
- Chopart (midtarsal); Syme (ankle); Pirogoff/Boyd
Principles
- Most distal level that heals + stays balanced
- Proximal levels → equinovarus (rebalance)
- Achilles lengthening + tibialis anterior transfer
- Durable plantar/heel weight-bearing surface
Decision
- Healing dominant in dysvascular/diabetic foot
- PFA: high reamputation; TTA: higher mortality (sicker)
- QoL/mobility similar PFA vs TTA
- Shared decision on level