General Anaesthesia for Orthopaedic Surgery
A balanced general anaesthetic delivers four things: unconsciousness (hypnosis), analgesia, amnesia, and muscle relaxation (immobility), while keeping the patient physiologically stable. No single drug does all four well, so a combination is used.
A general anaesthetic abolishes protective airway reflexes. The airway is supported with a supraglottic device (LMA) or secured with a cuffed tracheal tube. The feared scenario is can't intubate, can't oxygenate, which ends in a surgical front-of-neck airway.
Loss of reflexes means gastric contents can be aspirated. Elective fasting reduces this risk; an unfasted or high-risk patient (trauma, pain, pregnancy) needs a rapid sequence induction with cricoid pressure and a fast-acting relaxant.
Many orthopaedic patients are elderly with hip fracture or have an unstable cervical spine. Think about postoperative delirium, cardiac risk, and manual in-line stabilisation of the neck during airway management.
Overview
General anaesthesia is a reversible, drug-induced state in which the patient is unconscious, free of pain, has no memory of the procedure, and is still enough for surgery to proceed safely. It is best thought of as a controlled, temporary coma maintained by a balanced combination of drugs and undone at the end of the operation.
For an orthopaedic trainee, the point of understanding general anaesthesia is not to administer it yourself, but to be a safe and useful partner to the anaesthetist. You should know the phases of an anaesthetic (induction, airway and maintenance, emergence, recovery), the drugs and devices involved, the risks specific to your patients (the elderly hip fracture, the unstable cervical spine, the long bone fracture at risk of fat embolism), and the major complications you may be asked to recognise and help manage.
Three threads recur through this topic and the exam: the airway (how it is managed and what to do when it goes wrong), the general-versus-regional debate (what the evidence actually shows for hip fracture), and postoperative delirium (the commonest complication in your older patients, and largely preventable).
Principles: How a General Anaesthetic Works
The balanced anaesthetic
No single drug provides all four goals (hypnosis, analgesia, amnesia, relaxation) safely, so modern practice uses a balanced technique - several drugs each doing one job at a lower, safer dose. A typical sequence is an intravenous induction agent to put the patient to sleep, an opioid for analgesia, a muscle relaxant to allow intubation, and then a volatile gas or a propofol infusion to keep the patient asleep.
Before any of this, the anaesthetist stratifies perioperative risk. The most widely used shorthand is the ASA physical status grade (I a normal healthy patient, II mild systemic disease, III severe systemic disease, IV a constant threat to life, V moribund, with an E suffix for emergencies) - a higher ASA grade predicts higher perioperative morbidity and mortality and frames how aggressively the patient is optimised before surgery. Many older orthopaedic trauma patients are ASA III or higher, which is exactly why pre-operative medical optimisation and orthogeriatric co-management matter so much.
Induction and maintenance agents
- Role
- Intravenous induction (and infusion for maintenance)
- Key point for the exam
- Smooth induction and fast recovery - causes vasodilation and a drop in blood pressure
- Role
- Intravenous induction
- Key point for the exam
- Fast acting; historically used in rapid sequence induction; can cause hypotension
- Role
- Induction / analgesia
- Key point for the exam
- Maintains blood pressure and airway tone - useful in shock and trauma
- Role
- Maintenance (and gas induction in children)
- Key point for the exam
- Inhaled; all volatiles are malignant hyperthermia triggers
- Role
- Depolarising muscle relaxant
- Key point for the exam
- Very fast onset for rapid sequence; risks hyperkalaemia and malignant hyperthermia; prolonged paralysis (suxamethonium apnoea) in pseudocholinesterase deficiency
- Role
- Non-depolarising muscle relaxants
- Key point for the exam
- Longer acting; rocuronium reversible with sugammadex
Securing the airway
The airway sits at the centre of every general anaesthetic because the drugs abolish the reflexes that normally protect it. Three levels of airway support are used:
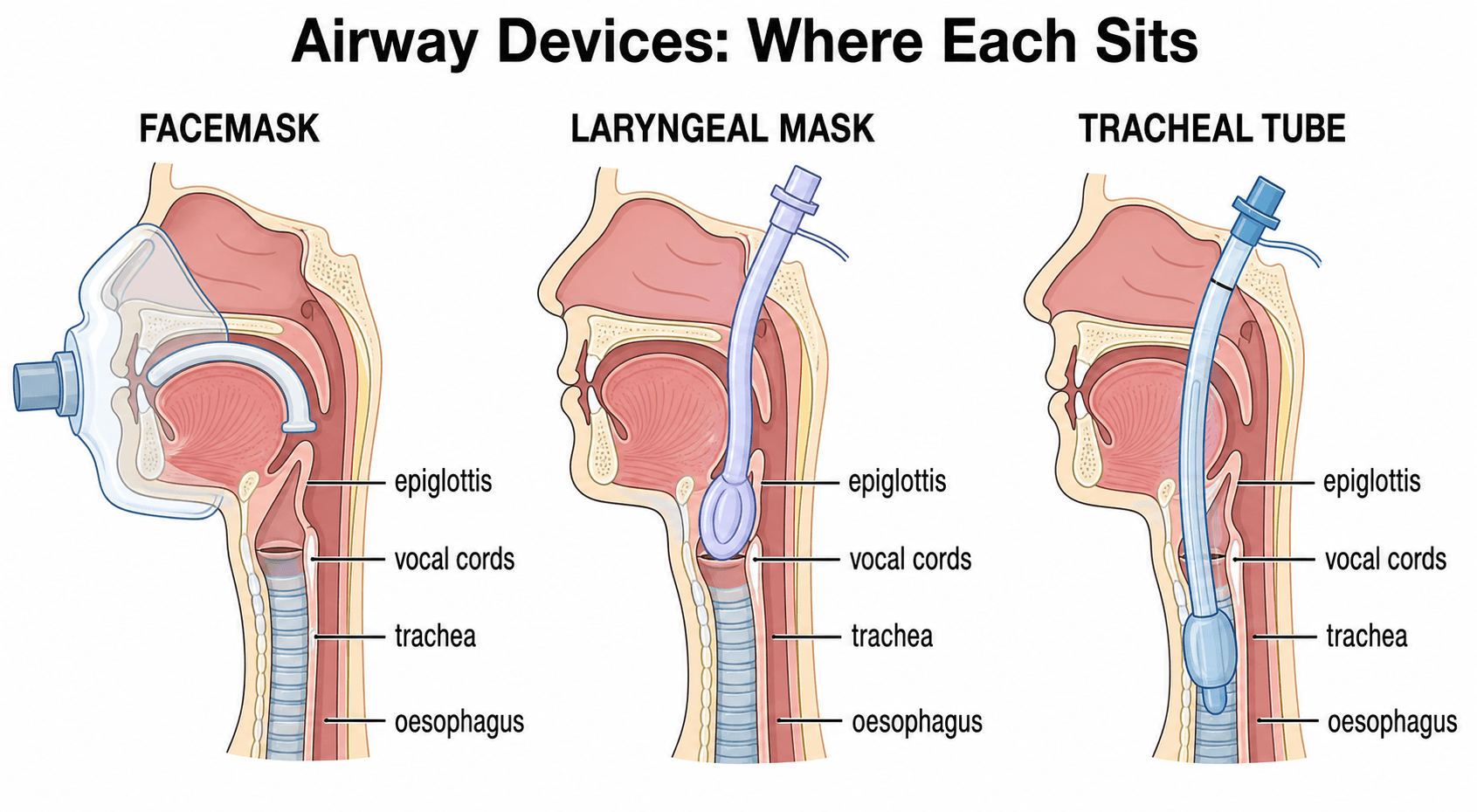
- Facemask / oral airway - for short cases or to oxygenate before intubation.
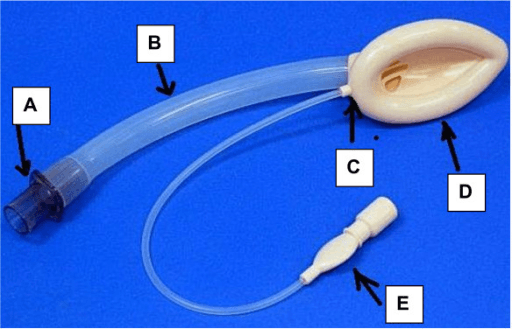
- Supraglottic airway (laryngeal mask) - sits over the laryngeal inlet (see the labelled image above). Quick, less stimulating, but offers only partial protection against aspiration.
- Tracheal (endotracheal) tube - a cuffed tube passed through the cords. It protects against aspiration and allows controlled ventilation, and is the choice for major surgery, the prone position, and the full or at-risk stomach.
The difficult airway
A difficult airway is one where mask ventilation, supraglottic placement or intubation is hard or fails. It is predicted before the case using assessments such as Mallampati grade, mouth opening, thyromental distance and neck movement (the LEMON aids in the memory section). When intubation fails, the anaesthetist follows a stepwise plan, escalating from optimised laryngoscopy and video laryngoscopy (images above) to a supraglottic device, and finally - in a can't intubate, can't oxygenate crisis - to a surgical front-of-neck airway.
The orthopaedic relevance of the difficult airway is the cervical spine. Patients with rheumatoid arthritis, ankylosing spondylitis, a previous cervical fusion, or a suspected unstable injury are all difficult airways. The neck is kept still with manual in-line stabilisation during intubation, and an awake fibreoptic technique may be chosen.
Aspiration and the rapid sequence induction
Because anaesthesia removes the cough and gag reflexes, stomach contents can be regurgitated and aspirated into the lungs. Elective fasting reduces gastric volume, but many orthopaedic patients are not safely fasted - they have eaten before a trauma, or pain and opioids have delayed gastric emptying. In these patients a rapid sequence induction is used: pre-oxygenation, a fast-acting induction agent and relaxant given together, and immediate intubation to secure the airway before contents can be aspirated.
Complications
- When it happens
- Induction and emergence
- Key point
- Escalate through the difficult airway plan to a surgical airway if can't intubate, can't oxygenate
- When it happens
- Induction in the unfasted or at-risk patient
- Key point
- Rapid sequence induction reduces the risk
- When it happens
- After a volatile agent or suxamethonium
- Key point
- Rising temperature, rigidity, rising end-tidal CO2 - treat with dantrolene
- When it happens
- Any time, often to relaxants or antibiotics
- Key point
- Hypotension, bronchospasm, rash - treat with adrenaline
- When it happens
- At cementation/prosthesis insertion in cemented hip arthroplasty
- Key point
- Sudden hypotension, hypoxia, arrhythmia or arrest - warn before cementing; uncemented fixation in high-risk patients
- When it happens
- 24-72 hours after long-bone fracture, reaming or nailing
- Key point
- Hypoxia, confusion and a petechial rash - supportive care; prevent with early fracture stabilisation
- When it happens
- Induction (hypotension) and surgery (blood loss)
- Key point
- Most agents drop blood pressure; the frail elderly tolerate it poorly
- When it happens
- Hours to days after surgery
- Key point
- Commonest complication in older orthopaedic patients - largely preventable
- When it happens
- After emergence
- Key point
- Common and distressing; awareness is rare but a recognised harm
Malignant hyperthermia
Malignant hyperthermia is a rare inherited disorder of skeletal muscle calcium handling (often a ryanodine receptor / RYR1 defect). Exposure to a volatile anaesthetic or suxamethonium triggers uncontrolled muscle metabolism: a rising end-tidal carbon dioxide, muscle rigidity, tachycardia, and a late, rapid rise in temperature. Treatment is to stop the trigger, give 100 percent oxygen, cool the patient, and give intravenous dantrolene. It is a classic basic-science viva because it links genetics, muscle physiology and an emergency.
Postoperative delirium
Delirium is an acute, fluctuating disturbance of attention and awareness. It is the commonest serious complication after major surgery in older patients, it predicts longer stays, loss of independence and higher mortality, and it is largely preventable. Prevention is multi-component (the ORIENT aid above): treat pain but minimise deliriogenic drugs, restore glasses and hearing aids, mobilise and feed early, remove catheters and lines, normalise sleep, and actively look for treatable causes such as hypoxia, infection, electrolyte disturbance and urinary retention.
Positioning injuries
Under general anaesthesia the patient cannot report pain or reposition, so the orthopaedic positions carry specific, examinable injuries that are a shared surgeon–anaesthetist responsibility:
- Peripheral nerves: the ulnar nerve at the elbow is the commonest perioperative neuropathy (tucked, pronated arms); the common peroneal nerve at the fibular head (lateral decubitus, lithotomy); and the brachial plexus with arm abduction beyond 90 degrees or a missing axillary roll in the lateral position.
- Beach-chair position (shoulder surgery): risk of cerebral hypoperfusion / watershed stroke because an arm blood-pressure cuff overestimates brain perfusion (a hydrostatic gradient of roughly 2 mmHg per inch of height above the heart), plus venous air embolism.
- Prone position (spine): post-operative visual loss / ischaemic optic neuropathy (prolonged prone time, blood loss, hypotension, direct eye pressure), facial and airway oedema, and caval compression from abdominal pressure.
- Traction table (femoral nailing): pudendal nerve injury and perineal/genital pressure necrosis from the perineal post, and sciatic stretch from excessive traction.
- Lithotomy / hemilithotomy: well-leg compartment syndrome in the elevated leg, and common peroneal palsy.
- General measures: pad bony prominences, protect the eyes (corneal abrasion is the commonest eye injury), and limit traction time.
Orthopaedic-Specific Anaesthetic Emergencies
Three intraoperative crises are bound tightly to orthopaedic operations themselves rather than to anaesthesia in general. They are high-yield because the surgeon is at the table when they happen and is part of the response.
Bone cement implantation syndrome
BCIS is sudden cardiovascular collapse during cementation and prosthesis insertion, classically when the femoral component of a cemented hemiarthroplasty or total hip replacement is impacted. The picture is hypotension, hypoxia, arrhythmia, and in severe cases cardiac arrest, occurring within minutes of cementing and reaming. The mechanism is embolisation of marrow fat, cement monomer and air into the circulation as the pressurised cement and prosthesis are driven into the canal, causing pulmonary hypertension and right heart strain, with a possible direct effect of the monomer. The classic patient is the elderly, ASA III–IV hip-fracture patient — the same patient in the hemiarthroplasty viva. Risk reduction is a shared surgeon–anaesthetist task: warn the anaesthetist before cementing, lavage and dry the canal, use a cement restrictor and retrograde insertion with adequate but not excessive pressurisation, and ensure the patient is well filled and not hypovolaemic. Severe cases are treated as resuscitation (100 percent oxygen, fluids, vasopressors). In the highest-risk patients, uncemented (cementless) fixation is an alternative that avoids the cement entirely.
Fat embolism syndrome
Fat embolism — the release of marrow fat into the circulation — occurs after long-bone and pelvic fractures and during intramedullary reaming and nailing. Most fat embolism is subclinical, but a minority develop fat embolism syndrome: the classic triad is respiratory distress (hypoxia), neurological dysfunction (confusion, drowsiness), and a petechial rash (typically over the chest, axillae and conjunctivae), developing 24 to 72 hours after the injury or surgery. It overlaps with BCIS mechanistically (both embolise marrow fat) but fat embolism syndrome is usually a postoperative ward diagnosis over hours to days, whereas BCIS is an immediate intraoperative collapse. Management is supportive — oxygen and respiratory support, careful fluid balance — and the most important lever is prevention through early fracture stabilisation.
Local anaesthetic systemic toxicity
Because regional anaesthesia and peripheral nerve blocks are central to orthopaedic care, every theatre team must recognise local anaesthetic systemic toxicity (LAST) — a toxic plasma level of local anaesthetic from inadvertent intravascular injection or overdose. It progresses from perioral tingling, tinnitus and agitation to seizures, and then to cardiovascular collapse and arrhythmia (bupivacaine is the most cardiotoxic agent). Treatment is to stop injecting, call for help, manage the airway and seizures, and give intravenous lipid emulsion (intralipid) alongside standard resuscitation. Prevention is meticulous technique: aspirate before injection, use ultrasound guidance, give incremental doses, and respect the maximum safe dose for the agent and the patient's weight.
Distinguish the two "embolic" orthopaedic emergencies by timing: bone cement implantation syndrome is an immediate collapse at the moment of cementation on the table, while fat embolism syndrome is a delayed (24–72 hour) triad of hypoxia, confusion and a petechial rash. Both share the underlying marrow-fat embolisation. A third, LAST, is the price of our heavy reliance on regional blocks — and its antidote, intravenous lipid emulsion, is a classic viva answer.
This section deliberately stops short of tourniquet physiology (the metabolic, haemodynamic and reperfusion effects of limb exsanguination and inflation), which is covered in depth in the dedicated tourniquet use topic.
Clinical Relevance
General anaesthesia touches almost every orthopaedic operation and recurs throughout the exam. In trauma, you must understand the full-stomach patient, the rapid sequence induction, and the unstable cervical spine. In arthroplasty and major surgery, the questions are about positioning, blood loss, fat embolism, and the general-versus-regional choice. In the elderly, the dominant issues are cardiac risk, frailty and postoperative delirium. And in the basic-science viva, the mechanism of the agents, the airway plan, and the recognition of complications such as malignant hyperthermia and local anaesthetic systemic toxicity are classic asks.
Being a good orthopaedic surgeon means planning with the anaesthetist: optimising the patient before surgery, agreeing the anaesthetic technique, and sharing responsibility for a safe recovery.
General versus Regional Anaesthesia
The choice between general anaesthesia and regional anaesthesia (spinal, epidural or peripheral nerve block) is one of the most examined practical questions, especially for hip fracture in the elderly. The intuitive argument that regional must be safer - avoiding airway instrumentation and deep sedation - has not been borne out as a clear survival or cognitive advantage in good randomised trials.
- General anaesthesia
- Requires airway support or a secured tube
- Regional anaesthesia
- Airway not instrumented (patient breathes spontaneously)
- General anaesthesia
- Broadly similar in good trials
- Regional anaesthesia
- Broadly similar - no clear survival advantage
- General anaesthesia
- No consistent difference from regional
- Regional anaesthesia
- No consistent difference from general
- General anaesthesia
- Needs separate analgesia plan
- Regional anaesthesia
- Nerve blocks give excellent early pain relief and less opioid
- General anaesthesia
- Useful when blocks fail, for long or prone cases, or anticoagulation
- Regional anaesthesia
- Limited by anticoagulation, patient refusal or inability to position
The honest exam answer is that the two techniques give similar major outcomes, so the choice is individualised - guided by the patient's comorbidities, anticoagulation, the surgery planned, and patient preference - and that peripheral nerve blocks add value either way by improving early pain relief and reducing opioid use and confusion.
Arthroplasty, revision, spine and pelvic/acetabular surgery can lose substantial blood, so patient blood management is examinable and surgeon-relevant:
- Tranexamic acid (TXA) — an antifibrinolytic (a lysine analogue that blocks plasminogen activation) given intravenously and/or topically. It reduces blood loss and transfusion and is now routine in elective hip and knee arthroplasty, and increasingly in hip-fracture and spine surgery; large datasets show no clear increase in thromboembolism in standard use.
- Cell salvage — intraoperative collection, washing and re-infusion of the patient's own shed blood; used in high-loss cases (revision arthroplasty, spine, pelvis/acetabulum), and avoided where the field is infected or contains tumour.
- Controlled (deliberate) hypotension — lowering the mean arterial pressure to reduce surgical bleeding (e.g. in spine), balanced against organ perfusion; regional/neuraxial anaesthesia itself lowers venous pressure and bleeding, one of its genuine advantages.
- Pre-operative optimisation and a restrictive transfusion trigger — correct anaemia (iron, sometimes erythropoietin) before elective surgery and transfuse to a restrictive haemoglobin threshold (commonly around 70 to 80 g/L) rather than liberally.
Guidelines, Registries and Global Practice
- Difficult airway guidelines (for example the Difficult Airway Society in the UK and the American Society of Anesthesiologists difficult airway algorithm) share a common stepwise structure - optimise laryngoscopy and use video laryngoscopy, move to a supraglottic device, and proceed to front-of-neck access in a can't intubate, can't oxygenate emergency.
- Hip fracture pathways worldwide (for example NICE and the national hip fracture audit in the UK, and orthogeriatric co-management models internationally) emphasise early surgery, multidisciplinary care, peripheral nerve blocks for analgesia, and delirium prevention rather than mandating a single anaesthetic technique.
- The general-versus-regional question is answered consistently across major randomised trials and meta-analyses: comparable major outcomes, so the choice is individualised to the patient, the surgery and contraindications such as anticoagulation.
- Malignant hyperthermia registries and reference centres exist in many countries to support diagnosis, family screening and the supply of dantrolene, reflecting how a rare but lethal complication is managed at a system level.
- Fasting guidance is broadly harmonised (clear fluids until shortly before surgery, longer for solids), with the rapid sequence induction reserved for patients who are not safely fasted.
Memory aids
HARMThe Goals of General Anaesthesia
Hook:A general anaesthetic must do no HARM - Hypnosis, Analgesia, Relaxation, Memory loss - the four goals delivered by a balanced technique.
LEMONPredicting the Difficult Airway
Hook:Squeeze the airway with LEMON - Look, Evaluate 3-3-2, Mallampati, Obstruction, Neck mobility - to predict who will be hard to intubate.
ORIENTPreventing Postoperative Delirium
Hook:Keep the patient ORIENTed to prevent delirium - Optimise analgesia, Reorient, Investigate, Early mobilise, No tethers, Trim risky drugs.

Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 84-year-old woman with a displaced intracapsular hip fracture is listed for hemiarthroplasty. She has mild dementia and takes an anticoagulant for atrial fibrillation. The examiner asks how the anaesthetic technique is chosen and what you would contribute as the surgeon.”
“A 30-year-old man with a high-energy injury needs an urgent general anaesthetic for an open femoral fracture. He ate two hours ago, is in severe pain, has a hard cervical collar on, and has facial bruising. What are the anaesthetic concerns and how is the airway managed?”
The Essentials
- Reversible drug-induced state: hypnosis, analgesia, amnesia, relaxation (HARM)
- Balanced technique - several drugs, each at a safer dose
- Four phases: induction, airway and maintenance, emergence, recovery
- Induction and emergence are the highest-risk phases
Airway
- Support with a laryngeal mask or secure with a cuffed tracheal tube
- Tracheal tube protects against aspiration - use for major or at-risk cases
- Predict the difficult airway (LEMON: Look, Evaluate 3-3-2, Mallampati, Obstruction, Neck)
- Can't intubate, can't oxygenate ends in a surgical front-of-neck airway
Orthopaedic-Specific
- Full stomach (trauma, pain, opioids) needs a rapid sequence induction
- Unstable cervical spine - manual in-line stabilisation during intubation
- GA versus regional for hip fracture: similar outcomes, individualise
- Add a peripheral nerve block - less pain, less opioid, less delirium
- ASA grade frames perioperative risk - many hip-fracture patients are ASA III+
Red Flags
- Rising end-tidal CO2, rigidity and fever - malignant hyperthermia (dantrolene)
- Hypotension, bronchospasm, rash - anaphylaxis (adrenaline)
- Collapse at cementation of a cemented hip - bone cement implantation syndrome
- Delayed hypoxia, confusion and petechiae - fat embolism syndrome
- Tingling, seizures, arrhythmia after a block - LAST (give intravenous lipid emulsion)
- New confusion after surgery - postoperative delirium (prevent with ORIENT)
Evidence
The strongest message here is a negative one and it is exam gold: across a meta-analysis (Bhushan) the long-debated general-versus-regional question has no winner for mortality or neurocognition in hip fracture — so never claim regional is "safer" in a viva; say the choice is individualised. The positive, actionable evidence is about adjuncts and depth: a high-certainty Cochrane review (Guay & Kopp) shows a peripheral nerve block reduces pain, delirium and chest infection regardless of anaesthetic technique, and the STRIDE RCT (Sieber) shows lighter sedation halves delirium in the otherwise-fit older patient. The Donaldson review anchors bone cement implantation syndrome as a real, recognised cause of intraoperative death that you mitigate by surgical selection (uncemented fixation) and team communication. Note the evidence grades: meta-analyses and a Cochrane review (Level 1) for the anaesthetic question, but a narrative review (Level 5) for BCIS — reflecting that BCIS is studied observationally, not by RCT.
Regional versus General Anaesthesia and Neurocognitive Outcomes in Hip Fracture
- Systematic review and meta-analysis of 8 randomised trials, 3555 patients over 65 undergoing hip fracture surgery
- No significant difference in postoperative delirium or cognitive dysfunction between regional and general anaesthesia at 24 hours, 3 days or 7 days
- No significant difference in other adverse events between the two techniques
- Authors conclude the anaesthetic choice should be based on individual patient characteristics, not on an expected outcome difference
Peripheral Nerve Blocks for Hip Fracture (Cochrane Review)
- 49 randomised trials, 3061 participants, comparing peripheral nerve blocks with no block (or sham)
- Nerve blocks reduce pain on movement within 30 minutes (high-certainty evidence)
- Nerve blocks reduce the risk of acute confusional state (delirium), number needed to treat about 12 (high-certainty evidence)
- Nerve blocks probably reduce chest infection and time to first mobilisation; permanent injury from blocks is rare
Depth of Sedation and Postoperative Delirium (STRIDE Randomised Trial)
- Double-blind RCT of 200 older patients having hip fracture repair under spinal anaesthesia with propofol sedation
- Lighter versus heavier sedation did not reduce overall delirium (34 versus 39 percent, not significant)
- In patients with no comorbidity, heavier sedation doubled the delirium risk (hazard ratio 2.3)
- Suggests sedation depth matters most in otherwise well patients, not those with multiple comorbidities
Bone cement implantation syndrome
- Narrative review establishing bone cement implantation syndrome (BCIS) as an important cause of intraoperative mortality and morbidity in cemented hip arthroplasty
- Describes a milder postoperative form causing hypoxia and confusion, not only the dramatic intraoperative collapse
- Older patients with co-existing pathology are at higher risk, and high-risk groups can be identified pre-operatively
- Recommends selecting uncemented arthroplasty for the highest-risk patients and considering invasive anaesthetic monitoring during cemented arthroplasty