Pneumatic cuff for a bloodless field | Set pressure from limb occlusion pressure | Mind the safe inflation time | Watch for nerve injury and post-tourniquet syndrome
- Purpose: a pneumatic tourniquet creates a bloodless field to improve visibility, speed surgery, and reduce blood loss - it does NOT make the operation sterile or stop hidden (postoperative) blood loss
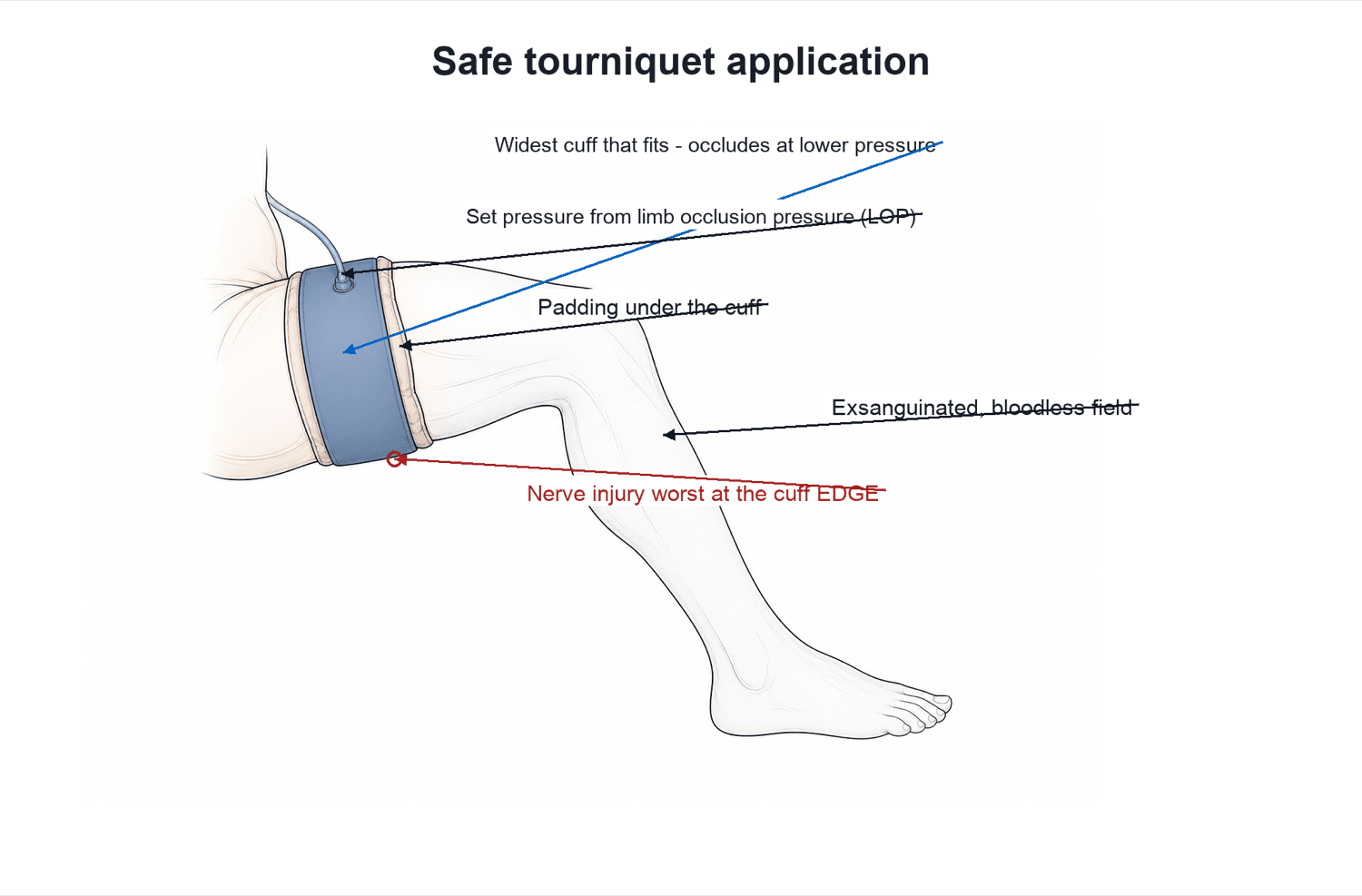
- Set the pressure to the limb, not the textbook: limb occlusion pressure (LOP) plus a safety margin gives the lowest effective pressure - lower pressure means less soft-tissue and nerve injury
- Apply correctly: widest cuff that fits, padding underneath, over the proximal limb, exsanguinate first (elevate then Esmarch/limb roll), then inflate - and protect the skin from prep fluid pooling under the cuff
- Time matters: keep inflation as short as possible; many units plan deflation by about 2 hours and a reperfusion break before re-inflating - the longer the time, the higher the complication risk
- The headline harms: nerve injury (commonest serious problem), post-tourniquet syndrome (swollen, stiff, weak limb), skin injury, and the systemic ischaemia-reperfusion response on deflation
- “Use the WIDEST cuff that fits - a wider cuff occludes arterial flow at a LOWER pressure, reducing nerve and muscle injury
- “Document inflation pressure and total tourniquet time in the operation note every time
- “Warn the anaesthetist before deflation - reperfusion causes a transient fall in blood pressure and a rise in end-tidal CO2 and serum potassium
- “Avoid or think very carefully before using a tourniquet in severe peripheral arterial disease, sickle cell disease, or a limb with infection or tumour
The modern standard is limb occlusion pressure (LOP) plus a safety margin, giving the lowest effective cuff pressure. A wider cuff occludes flow at a lower pressure. Lower pressure means less nerve and muscle injury - quoting a single fixed number for every patient is the dated answer.
The commonest serious complication. Caused by direct mechanical compression under the cuff (more than by ischaemia), so it is worst at the cuff edge. Risk rises with high pressure, long time, narrow cuff, and a thin limb. The radial nerve (arm) and sciatic/peroneal nerve (thigh) are vulnerable.
Deflation washes ischaemic metabolites into the circulation: expect a transient drop in blood pressure, a rise in end-tidal CO2, and a rise in serum potassium and lactate. In a frail patient or after a long inflation this can be significant - always warn before you let the cuff down.
Think hard before a tourniquet in severe peripheral arterial disease, sickle cell disease/trait (sickling in a hypoxic, acidotic, stagnant limb), active limb infection, limb tumour (theoretical tumour spread), previous vascular bypass, and significant venous thromboembolism risk.
Overview
The pneumatic tourniquet is one of the most common pieces of equipment in orthopaedic theatres. It is an inflatable cuff placed around the proximal part of a limb and pumped up above arterial pressure to stop blood flow, giving the surgeon a clean, bloodless field to operate in. It is used routinely for limb surgery such as knee replacement, foot and ankle work, hand surgery, and many trauma cases.
The benefit is better visibility and usually a faster operation with less blood in the wound. The cost is that the limb beyond the cuff is ischaemic for the duration, and the tissue under the cuff is squeezed hard. Almost every problem with tourniquets comes back to two things the examiner will test: how much pressure and how long. Get those right, apply the cuff properly, and the device is very safe; get them wrong and you can injure nerves, muscle, and skin.
For the exam, three threads recur throughout this topic: how to set it up safely (cuff choice, limb occlusion pressure, exsanguination, time), what the evidence shows (especially in total knee replacement), and what can go wrong (nerve injury, post-tourniquet syndrome, and the reperfusion response on deflation).
Principles: How a Tourniquet Works
A pneumatic tourniquet is an inflatable cuff connected to a console that pumps it to a set pressure and holds it there. When the cuff pressure rises above the pressure in the limb's arteries, arterial inflow stops; the cuff also compresses the veins so blood cannot drain in or out. The limb beyond the cuff becomes pale and bloodless.
The key idea: occlude at the lowest safe pressure. You only need enough pressure to stop arterial flow in that particular limb. Two factors decide how much that is:
- The patient's arterial pressure - a hypertensive patient needs more; this is why pressure is linked to systolic blood pressure or to a measured occlusion pressure.
- The cuff and the limb - a wider cuff transmits pressure more efficiently and occludes flow at a lower set pressure. A large, conical, or muscular limb needs more pressure than a thin one.
Limb occlusion pressure (LOP) is the minimum cuff pressure that stops arterial flow in that specific limb at that moment (detected by loss of a distal pulse or Doppler/plethysmography signal). Setting the cuff to LOP plus a safety margin gives a personalised, lower pressure than the old fixed numbers, and lower pressure is safer for nerves and muscle.
- How it is set
- Measure LOP for that limb, then add a margin (often 40 to 100mmHg depending on the LOP)
- Comment
- Preferred modern method - lowest effective pressure, personalised
- How it is set
- Systolic BP plus about 100mmHg (upper limb) or 150mmHg (lower limb)
- Comment
- Common, simple rule of thumb - reasonable when LOP is not measured
- How it is set
- About 250mmHg arm, 300mmHg leg for everyone
- Comment
- Outdated - often higher than the limb actually needs
If asked for a number, lead with the principle: "I set the lowest effective pressure using limb occlusion pressure plus a safety margin, and I use the widest cuff that fits." Then you can quote the systolic-plus-margin rule as a practical fallback. Leading with a single fixed number for all patients is the dated answer.
Applying the Tourniquet Safely
A safe tourniquet is as much about technique as about the machine. The steps below are a reliable viva structure.
Use the widest cuff that fits the limb and place it on the proximal limb (upper arm or proximal thigh) where there is muscle bulk to cushion the nerves. A contoured cuff fits a conical thigh better than a straight one.
Apply padding or a limb-protection sleeve under the cuff, with no wrinkles. Keep skin-prep fluid from pooling under the cuff - trapped alcoholic prep causes chemical burns. Some teams seal the cuff edge.
Empty the limb of blood first: elevate for a few minutes, then apply an Esmarch bandage or limb roller from distal to proximal (or just elevate if you must avoid squeezing - for example suspected infection or tumour). Then inflate to the set pressure and start the clock.
Document the inflation pressure and start time. Watch total tourniquet time, keep the team aware, and warn the anaesthetist before deflation. Deflate and let the limb reperfuse before closing if needed.
Alcoholic skin-prep fluid that runs under the cuff and is then trapped against the skin under pressure for the whole case is a classic cause of chemical burns and pressure blisters. Prevent it: pad the cuff, prevent pooling, and consider a waterproof seal at the cuff edge.
Inflation Time and the Ischaemic Limb
While the cuff is up, the limb beyond it has no blood supply. Tissue tolerates this for a while because muscle and nerve can survive a period of ischaemia, but the margin shrinks with time. There is no single universally agreed maximum, but a widely used practical approach is to keep inflation as short as possible and to plan a deflation by about 2 hours. If more time is needed, the cuff is let down for a reperfusion break (commonly around 10 to 15 minutes) before re-inflating.
- The limb becomes ischaemic, acidotic, and cold; anaerobic metabolites (lactate, potassium, carbon dioxide) build up.
- Nerve and muscle function progressively fail - this underlies the temporary "tourniquet palsy" seen after long inflations.
- Pooled metabolites wash into the central circulation, causing a transient fall in blood pressure, a rise in end-tidal CO2, and rises in serum potassium and lactate.
- There is a surge of blood into the dilated limb, so a brief drop in central volume and pressure.
- This is usually well tolerated in a fit patient but can be significant after a long inflation or in a frail or cardiac patient - which is exactly why you warn the anaesthetist first.
"Tourniquet time" is the total time the cuff is inflated, and it belongs in the operation note. The reperfusion changes on deflation (lower BP, higher CO2 and potassium) are a favourite physiology link - tie them to the build-up of metabolites in the ischaemic limb.
Contraindications and Cautions
There are few absolute contraindications, but several situations where you should think hard, choose elevation-only exsanguination, or avoid the tourniquet altogether:
A tourniquet can damage diseased, calcified vessels and worsen distal ischaemia. A previous vascular bypass graft in the limb is a strong reason to avoid the cuff.
The stagnant, hypoxic, acidotic limb beyond the cuff promotes sickling. Many avoid tourniquets here; if used, careful exsanguination, oxygenation, and minimal time are advised.
Exsanguinating an infected limb risks pushing organisms into the circulation; elevation-only exsanguination is preferred if a tourniquet is needed at all.
There is a theoretical risk of squeezing tumour cells into the circulation during exsanguination - avoid the Esmarch and use gentle elevation, or avoid the tourniquet.
Other cautions include significant venous thromboembolism risk, severe crush or vascular injury in the same limb, and very poor skin condition under the cuff.
Tourniquet for Intravenous Regional Anaesthesia (Bier Block)
Beyond the bloodless field, the tourniquet is the safety device in a Bier block (intravenous regional anaesthesia, IVRA) — a technique for short distal-limb procedures (typically under about an hour, for example hand or forearm surgery and fracture manipulation).
- Technique: insert a cannula in the operative limb distally, exsanguinate (elevate then Esmarch), inflate a double-cuff tourniquet (proximal cuff first), then inject dilute local anaesthetic into the distal vein so it fills the venous system and anaesthetises the limb. When the proximal cuff becomes painful, inflate the distal cuff over now-anaesthetised skin and release the proximal one.
- Drug: prilocaine is preferred for its low cardiotoxicity; bupivacaine is contraindicated (too cardiotoxic for this technique).
- The danger is the cuff: the tourniquet is the only thing keeping the local anaesthetic in the limb. Premature deflation or cuff failure releases a bolus of local anaesthetic into the systemic circulation, causing local anaesthetic systemic toxicity (LAST) — seizures and cardiovascular collapse.
Keep the cuff inflated for a minimum time (commonly around 20 to 30 minutes) even if the procedure finishes sooner, so the local anaesthetic becomes tissue-bound, and then deflate slowly or in cycles while watching for toxicity. Respect the maximum safe dose, use prilocaine rather than bupivacaine, and have lipid emulsion and resuscitation available.
The Emergency Haemorrhage-Control Tourniquet
Distinct from the theatre pneumatic cuff is the pre-hospital / trauma haemorrhage-control tourniquet, used for life-threatening external limb bleeding — the catastrophic haemorrhage ("C") that is addressed before the airway in the trauma primary survey.
- Device and application: a windlass tourniquet (for example a Combat Application Tourniquet, CAT) or a pneumatic/improvised one, applied proximal to the wound and tightened until external bleeding stops and the distal pulse is abolished; apply a second tourniquet side by side if one does not control the bleeding.
- Principles: apply early for exsanguinating limb haemorrhage, record the time of application, and do NOT periodically release it in the field (this rebleeds and disrupts the clot); the limb tolerates ischaemia for up to about 2 hours, after which the same reperfusion/metabolic load applies on release.
- Conversion: in hospital the tourniquet is converted to definitive haemostasis (direct repair or a haemostatic dressing) once the patient is resuscitated and bleeding is controlled.
Modern military and civilian evidence shows that, used correctly, an emergency tourniquet is life-saving with an acceptable complication rate — the old fear that "a tourniquet costs the limb" should not delay control of catastrophic limb haemorrhage. Mark the application time clearly and hand it over explicitly.
Complications
- Mechanism / who
- Mechanical compression at the cuff edge, made worse by high pressure, long time, narrow cuff, thin limb
- Key point
- Commonest serious harm - usually neurapraxia and recovers, but can be permanent
- Mechanism / who
- Reperfusion oedema and ischaemic injury after deflation
- Key point
- Swollen, stiff, pale, weak, numb limb for days to weeks; supportive treatment
- Mechanism / who
- Prep fluid pooling under the cuff, or pressure on skin
- Key point
- Prevent with padding, no pooling, seal the cuff edge
- Mechanism / who
- Washout of ischaemic metabolites at deflation
- Key point
- Transient BP drop, rise in end-tidal CO2, potassium and lactate - warn the anaesthetist
- Mechanism / who
- Venous stasis distal to the cuff
- Key point
- Higher DVT signal with tourniquet use in knee replacement
- Mechanism / who
- Crush plus ischaemia, very prolonged or high-pressure use
- Key point
- Rare - relates to excessive pressure and time
Nerve injury
This is the complication examiners chase, and the crucial concept is that it is mainly mechanical, not ischaemic - the nerve is crushed under the cuff, so injury is worst at the edge of the cuff. Risk climbs with high pressure, long inflation time, a narrow cuff, and a thin limb. The vulnerable nerves are the radial nerve in the arm and the sciatic and common peroneal nerves in the lower limb. Most are a neurapraxia that recovers over weeks to months, but severe or prolonged compression can cause lasting deficit. The prevention is the same theme throughout: lowest effective pressure, widest cuff, shortest time.
Post-tourniquet syndrome
After deflation the limb can become swollen, stiff, pale, weak, and numb without an actual nerve transection. It reflects reperfusion oedema and ischaemic soft-tissue injury, is usually self-limiting over days to weeks, and is managed supportively with elevation and time. It is more likely after long or high-pressure inflations.
If a patient wakes with a wrist drop after upper-limb surgery under tourniquet, think tourniquet-related radial nerve neurapraxia from cuff compression. Document the deficit, reassure that most recover, and follow up - but always exclude a surgical cause for the nerve injury too.
Clinical Relevance
The tourniquet appears across every limb operation and is a favourite of basic-science and operative vivas because it links anatomy, physiology, and safe practice in one device. In knee replacement the decision to use it, for how long, and at what pressure is an active debate you should be able to argue. In hand, foot, and trauma surgery correct cuff choice, exsanguination, and time-keeping are everyday skills. In anaesthesia and physiology the reperfusion changes on deflation are a classic teaching point. Knowing how to set safe pressure, how to apply the cuff, when to avoid it, and what can go wrong is the practical core examiners probe - and it all reduces to the same idea: the lowest effective pressure, the widest cuff, for the shortest time.
Guidelines, Registries and Global Practice
- Lowest effective pressure is the consistent message across modern guidance (for example AORN perioperative recommendations and AAOS/specialty education): set cuff pressure from limb occlusion pressure plus a margin and use the widest cuff that fits, rather than a fixed high pressure for everyone.
- Documentation of cuff pressure and total tourniquet time in the operative record is standard safe-surgery practice worldwide.
- Knee replacement practice varies globally: some surgeons use a tourniquet for the whole case, some only for cementation, and some omit it entirely. The trend, supported by meta-analyses, is toward shorter and lower-pressure use because of the early pain, slower recovery, and higher deep vein thrombosis signal seen with full-length high-pressure inflation.
- Special populations (sickle cell disease, severe peripheral arterial disease, previous vascular bypass, limb infection or tumour) are handled cautiously everywhere, with elevation-only exsanguination or avoidance of the tourniquet depending on the situation.
Memory aids
PRESSURETourniquet Complications
Hook:Too much PRESSURE for too long is what harms the limb - that is the whole story of tourniquet complications.
WIDESafe Application Steps
Hook:Go WIDE - the widest cuff, padded, on an exsanguinated limb, at a documented pressure and time.
VASTThink Twice (Contraindications)
Hook:A VAST list of red flags - Vascular disease, Abnormal red cells, Sepsis, Tumour - means think twice about a tourniquet.



Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are about to perform a foot operation under tourniquet on a 55-year-old man. The examiner asks how you choose the cuff and pressure and how you apply it safely.”
“A 60-year-old woman has had a 90-minute forearm operation under an upper-arm tourniquet. In recovery she cannot extend her wrist or fingers. How do you approach this?”
Purpose and Principle
- Pneumatic cuff above arterial pressure - bloodless field
- Set the LOWEST effective pressure for that limb
- Wider cuff occludes flow at a lower pressure
- Does not stop hidden (postoperative) blood loss
Setting Pressure
- Best: limb occlusion pressure (LOP) plus a safety margin
- Rule of thumb: systolic + about 100mmHg arm, 150mmHg leg
- Avoid quoting one fixed number for everyone
- Document pressure and start time every case
Safe Application
- Widest cuff on the proximal limb, padded
- Protect skin from prep-fluid pooling (chemical burn)
- Exsanguinate: elevate then Esmarch (or elevation only if infection/tumour)
- Keep time short; plan deflation by about 2 hours, reperfuse before re-inflating
Red Flags / Harms
- Nerve injury - mechanical, at the cuff edge, commonest serious harm
- Post-tourniquet syndrome - swollen, stiff, weak limb
- Warn anaesthetist before deflation (BP down, CO2, potassium, lactate up)
- Think twice: severe PAD, sickle cell, limb infection, limb tumour
Evidence: Tourniquet in Knee Replacement
Total knee arthroplasty is where tourniquet use has been studied most, because surgeons disagree about whether the bloodless field is worth the soft-tissue cost.
Tourniquet Worsens Early Pain and Function in Knee Replacement (Meta-Analysis)
- Systematic review and meta-analysis of 18 studies, 1279 total knee arthroplasties (646 with tourniquet, 633 without)
- Significantly LOWER early pain without a tourniquet, both in the first 5 days and at 1 to 3 months
- Range of motion at 2 to 3 days was significantly better without a tourniquet
- Deep vein thrombosis occurred significantly more often WITH a tourniquet; no difference in Knee Society Score, pulmonary embolism, or surgical site infection
Personalised (Limb Occlusion) Pressure Beats Uniform Pressure (Meta-Analysis of RCTs)
- Meta-analysis of 13 randomised controlled trials, 1204 total knee arthroplasties
- Personalised pressure (based on systolic BP and limb occlusion pressure) gave the same bloodless field as a uniform high pressure
- Personalised pressure produced LESS postoperative pain, less thigh swelling, and less thigh bruising (ecchymosis)
- Personalised pressure gave a higher early function score and better early knee range of motion
Limited Tourniquet Time Is Safe in Knee Replacement (RCT)
- Randomised controlled trial of 62 patients having primary unilateral total knee arthroplasty
- Compared a tourniquet used only during cementation versus full-time inflation throughout
- No significant difference in total or hidden blood loss, or in transfusion and perioperative complication rates
- Full-time use gave a clearer field and slightly lower measured intraoperative blood loss, but limited use was safe