Genetics & Modes of Inheritance in Orthopaedics
- Male-to-male (father-to-son) transmission EXCLUDES X-linkage — a father gives his sons a Y, not his X. Calling an obvious M→M pedigree "X-linked" is the classic trip-up. It is the single most decisive clue and points to autosomal dominant.
- A negative family history does NOT exclude an autosomal dominant disorder — many high-yield AD conditions are commonly de novo (achondroplasia ~80%, a large share of NF1 and OI). Do not reassure a family that a sporadic case "isn't genetic."
- X-linked recessive vs mitochondrial both seem to spare father-to-son, but only mitochondrial is strictly maternal to ALL children of an affected mother; an affected father passes a mitochondrial disorder to none.
- Reduced penetrance and variable expressivity can make an AD trait appear to skip a generation or look mild in a known carrier — never declare an at-risk relative "unaffected, therefore non-carrier" without testing.
- OPG/RANKL-style decoy logic does not apply here — keep the gene–disease pairs crisp: confusing COMP (MED/pseudoachondroplasia) with COL2A1 (SED/Stickler) or FBN1 (Marfan) with TGFBR1/2 (Loeys-Dietz) loses easy marks.
Overview & Introduction
Medical genetics is a recurring basic-science viva theme because so much of orthopaedic practice — skeletal dysplasias, connective-tissue disease, haemophilic arthropathy, hereditary tumour syndromes — is built on a handful of single-gene (Mendelian) disorders with predictable inheritance. The examiner is rarely testing molecular detail; they want to see that you can read a pedigree, name the pattern, attach the gene, and counsel recurrence risk in a few clean sentences.
This page works from the four classic patterns — autosomal dominant, autosomal recessive, X-linked (recessive and dominant) and mitochondrial — then layers on the modifying concepts (penetrance, expressivity, anticipation, mosaicism, de novo mutation) that make real pedigrees messy, and finishes with the gene–condition pairs examiners expect on demand. Throughout, the orthopaedic anchor conditions are kept front and centre so the genetics is never abstract: FGFR3/achondroplasia, COL1A1·2/osteogenesis imperfecta, FBN1/Marfan, EXT1·2/multiple hereditary exostoses, NF1, and PHEX/X-linked hypophosphataemic rickets.
For any pedigree, ask in order: (1) Is the trait in every generation (suggests dominant) or does it skip (suggests recessive)? (2) Are both sexes affected roughly equally (autosomal) or is there a strong male predominance (consider X-linked recessive)? (3) Is there male-to-male transmission (proves autosomal — excludes X-linkage)? (4) Is transmission exclusively maternal to all children (mitochondrial)? Four questions resolve almost every exam pedigree.
Autosomal dominant inheritance
In autosomal dominant (AD) inheritance a single mutant allele produces the phenotype. An affected heterozygote has a 50% chance of passing the allele to each child. The pedigree shows the trait in every generation, both sexes affected, and male-to-male transmission (which rules out X-linkage). Many AD conditions arise from new (de novo) mutations, so a negative family history does not exclude them. AD conditions often result from gain-of-function, dominant-negative (a faulty subunit poisoning a multimer, as in OI), or haploinsufficiency mechanisms.
- Gene
- FGFR3
- Mechanism / note
- Gain-of-function; suppresses growth-plate chondrocytes; ~80% de novo
- Gene
- COL1A1 / COL1A2
- Mechanism / note
- ~85% AD; dominant-negative effect on type I collagen
- Gene
- FBN1 (fibrillin-1)
- Mechanism / note
- Connective tissue; tall, arachnodactyly, scoliosis, aortic root
- Gene
- EXT1 / EXT2
- Mechanism / note
- Multiple osteochondromas; small malignant transformation risk
- Gene
- NF1 (neurofibromin)
- Mechanism / note
- Scoliosis, pseudarthrosis of tibia, café-au-lait spots
- Gene
- COMP and others
- Mechanism / note
- Epiphyseal dysplasia; early osteoarthritis
Autosomal recessive inheritance
In autosomal recessive (AR) inheritance both alleles must be mutated. Affected individuals usually have unaffected carrier parents, the trait commonly skips generations, and the risk rises with consanguinity. Two carrier parents have a 25% chance of an affected child, 50% carriers, 25% unaffected. Many inborn errors of metabolism and storage disorders with skeletal manifestations (e.g. mucopolysaccharidoses), some severe/lethal OI forms, and conditions such as diastrophic dysplasia follow AR inheritance.

X-linked & mitochondrial inheritance
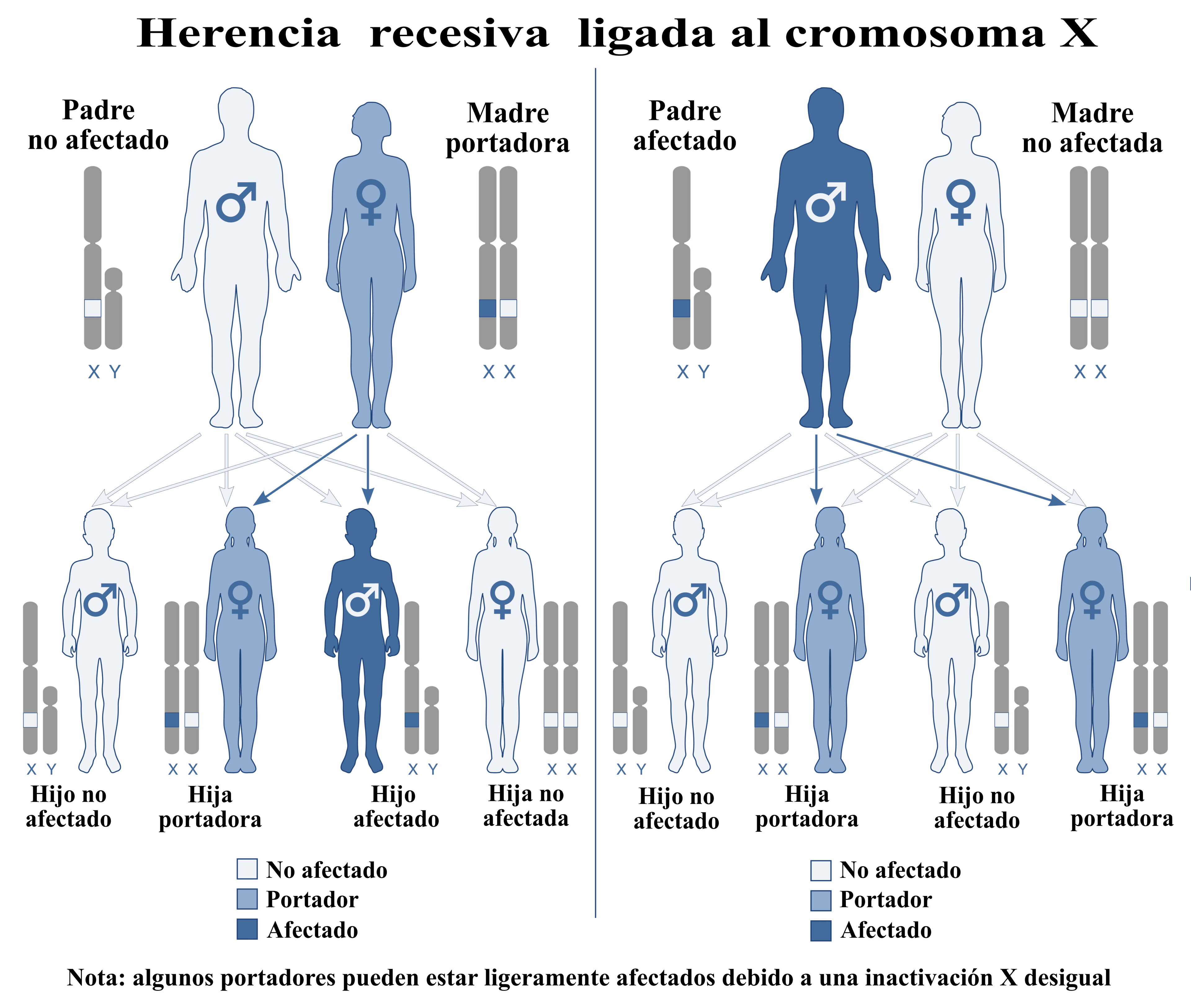
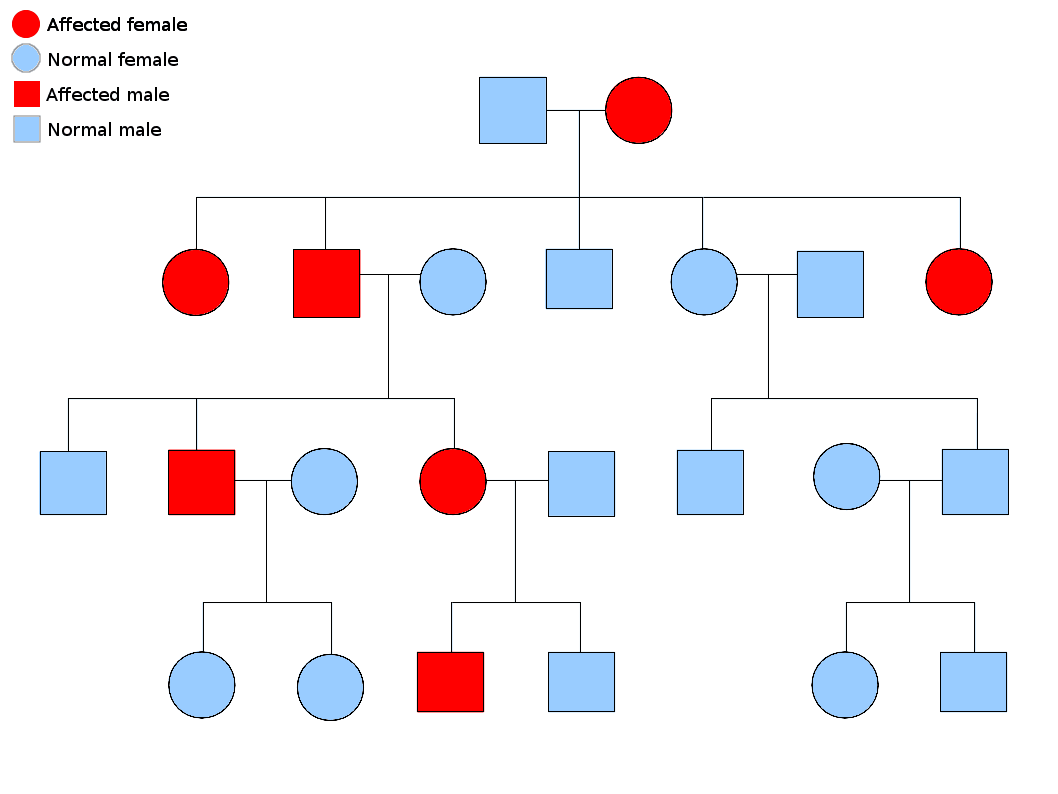
Males are hemizygous (one X), so a single mutant X-allele causes disease — hence X-linked recessive conditions predominantly affect males, transmitted through carrier females. There is no male-to-male transmission (a father gives his Y to sons), and an affected father's daughters are all carriers. Orthopaedic-relevant examples: Duchenne/Becker muscular dystrophy (dystrophin) and haemophilia A/B (factor VIII/IX — relevant to haemophilic arthropathy).

Concepts that modify the simple pattern
- Meaning
- Proportion of mutation carriers who show ANY phenotype
- Orthopaedic relevance
- Reduced penetrance can make AD conditions appear to skip a generation
- Meaning
- Severity/features vary between carriers of the same mutation
- Orthopaedic relevance
- e.g. wide severity range in NF1, Marfan
- Meaning
- New mutation absent in parents
- Orthopaedic relevance
- ~80% of achondroplasia; negative family history does not exclude AD
- Meaning
- Earlier onset / worse in successive generations
- Orthopaedic relevance
- Trinucleotide-repeat disorders (e.g. myotonic dystrophy)
- Meaning
- Mutation present in only some cells (somatic/germline)
- Orthopaedic relevance
- Explains some sporadic cases and recurrence risk despite unaffected parents
- Meaning
- One gene affecting multiple organ systems
- Orthopaedic relevance
- Marfan: skeletal + ocular + cardiovascular
These concepts drive counselling and recurrence-risk estimates. A patient with an apparently sporadic AD condition may have a de novo mutation (low sibling-recurrence risk but 50% for the patient's own offspring) or germline mosaicism in a parent (raising sibling-recurrence risk). Reduced penetrance and variable expressivity mean an "unaffected" relative may still carry the gene — important before reassuring a family.
Clinical Relevance: counselling & orthopaedic management
Knowing the inheritance pattern is not academic — it changes what you screen for, who you refer, and what you tell the family. The orthopaedic surgeon is often the first to recognise a heritable skeletal phenotype, so a structured response carries marks and changes care.
- Inheritance / counselling point
- AD, high penetrance; EXT1 disease tends more severe
- Orthopaedic surveillance & management implication
- Lifelong awareness of malignant transformation to secondary chondrosarcoma (~0.5-5% per the cited Bovee review); investigate a lesion that grows after skeletal maturity or becomes painful
- Inheritance / counselling point
- AD; pleiotropy means cardiac risk dominates prognosis
- Orthopaedic surveillance & management implication
- Mandatory cardiology referral for AORTIC ROOT surveillance before elective spinal/scoliosis or limb surgery; monitor scoliosis and protrusio acetabuli
- Inheritance / counselling point
- AD, ~50% de novo, near-complete penetrance, very variable expressivity
- Orthopaedic surveillance & management implication
- Watch dystrophic scoliosis (rapid, short-segment, kyphotic) and congenital tibial pseudarthrosis; low threshold for MRI
- Inheritance / counselling point
- Mostly AD dominant-negative; severe/recessive forms exist
- Orthopaedic surveillance & management implication
- Bisphosphonate therapy, fracture/deformity management, telescoping rods; consider non-accidental injury mimic
- Inheritance / counselling point
- AD, ~80% de novo; homozygous (two affected parents) is lethal
- Orthopaedic surveillance & management implication
- Foramen magnum/cervicomedullary and spinal stenosis surveillance; guarded limb-lengthening counselling; FGFR3-directed therapy (vosoritide) emerging
- Inheritance / counselling point
- X-linked dominant; affected father transmits to all daughters, no sons
- Orthopaedic surveillance & management implication
- Phosphate + active vitamin D (or burosumab); correct deformity only once medically optimised to avoid recurrence
When asked to counsel a family, structure it: (1) confirm the pattern and recurrence risk (50% for an AD heterozygote's offspring; 25% for two AR carriers); (2) flag that a de novo case has low sibling risk but 50% for the patient's own children, while germline mosaicism in a phenotypically normal parent can still raise sibling risk; (3) acknowledge reduced penetrance/variable expressivity so an "unaffected" relative may still carry the gene; (4) refer to clinical genetics for formal counselling, confirmatory testing and discussion of prenatal or preimplantation options. Surgeons recognise the phenotype and coordinate — they do not give definitive genetic counselling alone.
"Refer for confirmatory testing" means choosing the right molecular test for the question:
- Karyotype - whole-chromosome analysis for aneuploidy and balanced translocations.
- FISH - targeted detection of a specific locus or microdeletion.
- Chromosomal microarray (array-CGH / SNP array) - genome-wide copy-number; the first-tier test for unexplained developmental delay / multiple congenital anomalies.
- Targeted (Sanger) single-gene testing - when one gene/variant is expected (the recurrent FGFR3 mutation in achondroplasia, or a known familial variant).
- Multigene NGS panels - for a phenotype with locus heterogeneity (a skeletal-dysplasia or OI panel).
- Whole-exome / whole-genome sequencing - for the undiagnosed or atypical case.
Pick by scenario: a known familial pathogenic variant → targeted testing of that variant; a clinically obvious single-gene condition → that gene; a heterogeneous/unclear phenotype → a panel or exome.
Once the causative variant is identified, families can be offered, through clinical genetics:
- Prenatal diagnosis - chorionic villus sampling (CVS, ~11-14 weeks, placental tissue) or amniocentesis (from ~15-16 weeks, amniocytes) - both definitive for the known variant but invasive with a small miscarriage risk.
- Preimplantation genetic testing for monogenic disease (PGT-M) - IVF with embryo biopsy to transfer only unaffected embryos; requires a known familial mutation and avoids a termination decision.
- Non-invasive prenatal testing (cell-free DNA) is largely a screen (mainly for aneuploidy) and does not replace definitive testing for most monogenic skeletal disorders.
The orthopaedic surgeon's role is to recognise the phenotype and refer; clinical genetics delivers these options and the formal counselling.
Mnemonics & Memory Aids
- AD: every generation, both sexes, male-to-male transmission (excludes X-linkage), 50% offspring risk.
- AR: skips generations, carrier parents, consanguinity, 25% affected.
- X-linked recessive: mainly males via carrier females, no father-to-son; affected father → all daughters carriers.
- Mitochondrial: strictly maternal — an affected mother passes to all children, an affected father to none.
- Gene pairs: FGFR3-achondroplasia, COL1A1/2-OI (~85%), FBN1-Marfan, EXT1/2-MHE, NF1, PHEX-XLH.
- De novo + mosaicism + penetrance change recurrence risk — a negative family history doesn't exclude AD.
DOMINANTAutosomal dominant signature
Hook:DOMINANT: One allele, every generation, male-to-male - the AD signature.
X-LINKX-linked signature
Hook:X-LINK: affected males via carrier mothers, never father to son.
Evidence Base
Osteogenesis imperfecta
- About 85% of osteogenesis imperfecta is caused by DOMINANT autosomal mutations in the type I collagen genes COL1A1 and COL1A2, affecting collagen quantity or structure.
- Recessive, dominant and X-linked defects in many other genes (collagen processing, secretion, post-translational modification, osteoblast regulation) also cause OI, complicating classification.
- Manifestations extend beyond bone (cardiovascular, pulmonary, skin, hearing, dentinogenesis imperfecta) - an example of pleiotropy.
Achondroplasia: Development, pathogenesis, and therapy
- Autosomal dominant GAIN-OF-FUNCTION mutations in FGFR3 cause achondroplasia and related chondrodysplasias (hypochondroplasia, SADDAN, thanatophoric dysplasia).
- Increased FGFR3 signalling paradoxically SUPPRESSES growth-plate chondrocyte proliferation and maturation, reducing endochondral bone elongation.
- Illustrates how a single recurrent dominant mutation produces a defined skeletal phenotype and how therapies aim to counter excess FGFR3 signalling.
Multiple osteochondromas
- Multiple osteochondromas is an AUTOSOMAL DOMINANT disorder; germline mutations in the tumour-suppressor genes EXT1 or EXT2 are found in almost 90% of patients.
- Malignant transformation of an osteochondroma to secondary peripheral chondrosarcoma is estimated at 0.5-5% - the most important complication.
- Antenatal diagnosis is technically possible when the exact familial mutation is known; regular follow-up is justified for early detection of malignancy.
The OI inheritance and classification facts come from Marini et al. (Nat Rev Dis Primers 2017, DOI); the achondroplasia FGFR3 gain-of-function mechanism from Ornitz & Legeai-Mallet (Dev Dyn 2017, DOI); and the multiple-hereditary-exostoses EXT1/EXT2 genetics and chondrosarcoma risk from Bovée (Orphanet J Rare Dis 2008, DOI). All three are narrative reviews (Level V), appropriate for established genetic facts rather than comparative effectiveness. The remaining gene-condition pairings (Marfan-FBN1, NF1-neurofibromin, X-linked hypophosphataemic rickets-PHEX) are standard, well-established medical genetics.