Hip Abductor Tears | The Rotator Cuff of the Hip | Repair, Transfer, Reconstruction
- Rotator cuff of the hip - gluteus medius and minimus tears behave like supraspinatus tears, with footprint detachment, retraction and fatty infiltration driving outcome
- A tear is not the same as tendinopathy - this topic is the structural/surgical end of the spectrum; pure tendinopathy and bursitis are covered under greater trochanteric pain syndrome
- MRI is the reference standard - characterises tear thickness, retraction, and muscle fatty infiltration that determines reparability
- Fatty infiltration predicts failure - high-grade atrophy makes direct repair unreliable and pushes towards transfer or reconstruction
- Think abductor tear after THA - persistent limp, Trendelenburg gait or instability after hip replacement may be an iatrogenic or attritional abductor tear
- “Trendelenburg gait plus weak resisted abduction in a middle-aged woman with lateral hip pain points to a tear, not just bursitis
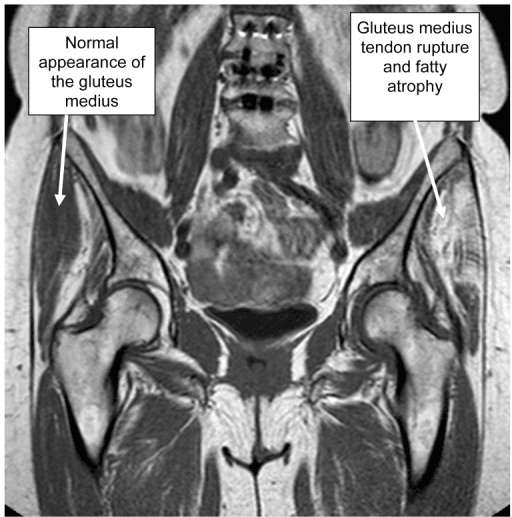
- “A focus of T2 hyperintensity superior to the greater trochanter is the single best MRI sign of an abductor tendon tear
- “Open and endoscopic repair give similar patient-reported outcomes; open techniques report higher complication rates
- “Gluteus maximus transfer is a salvage option for the chronically retracted, fatty, irreparable tendon
Do not blur the spectrum. Tendinopathy and bursitis sit under greater trochanteric pain syndrome and are managed non-operatively. A structural tear of the gluteus medius or minimus is the surgical entity examined here - graded by thickness, retraction and fatty infiltration.
MRI is the reference standard. Report tear thickness (partial vs full), retraction, and muscle fatty infiltration / atrophy. High-grade fatty change is the single most important predictor of irreparability and a poor repair outcome.
A persistent limp, positive Trendelenburg or recurrent instability after total hip arthroplasty should make you think of an abductor tendon tear or detachment, especially after a lateral or transgluteal approach. This is a recognised cause of failed THA and may need repair, transfer or reconstruction.
For chronic, retracted, fatty, irreparable tears, direct repair fails. Know the salvage options: graft augmentation, gluteus maximus tendon transfer, and combined gluteus maximus / tensor fascia lata transfers in revision arthroplasty.
Overview and Epidemiology
Gluteal tendon tears are tears of the gluteus medius and/or minimus tendons at their insertion on the greater trochanter. They are increasingly recognised as a discrete cause of chronic lateral hip pain and abductor weakness, distinct from simple bursitis. Because the gluteus medius and minimus stabilise the pelvis during single-leg stance in the same way the rotator cuff stabilises the glenohumeral joint, abductor tendon tears are widely described as the "rotator cuff of the hip" and follow a similar natural history of tendinopathy progressing to partial then full-thickness tearing with retraction and fatty muscle change. [1,2]
- Strong female predominance - most surgical series are heavily weighted towards women, frequently around or above a 4:1 ratio.
- Typical age at presentation is 50 to 70 years; tears are usually degenerative and insidious rather than acute traumatic events.
- Peritrochanteric tendon pathology is common on hip MRI. In a large consecutive imaging series, peritrochanteric lesions (including partial and full-thickness gluteus medius and minimus tears) were found in roughly one in five hips, and were detected significantly more often on 3.0-Tesla than 1.5-Tesla MRI. [3]
- Isolated trochanteric bursitis without tendon pathology is uncommon (well under 10% of patients with lateral hip pain), reinforcing that structural tendon disease drives most refractory symptoms.
distinguishing a structural tear from tendinopathy or bursitis changes management. Tendinopathy responds to loading rehabilitation; a full-thickness tear with weakness and fatty change is a surgical problem where the timing of intervention and the reparability of the tendon determine the outcome.
Anatomy and Pathophysiology
Functional anatomy
The hip abductor mechanism is formed by the gluteus medius and gluteus minimus, with the iliotibial band and tensor fascia lata contributing to lateral pelvic stability.
- Gluteus medius inserts on two facets of the greater trochanter: the lateral facet (the main, broad insertion) and the superoposterior facet. It is the principal hip abductor and the key pelvic stabiliser in single-leg stance.
- Gluteus minimus inserts more anteriorly on the anterior facet of the greater trochanter and on the hip capsule, acting as an abductor and a fine-tuner of femoral head position.
- The tendons lie deep to the iliotibial band; the overlying ITB applies a compressive load against the trochanter, particularly in hip adduction.
- The superior gluteal nerve supplies both muscles and the tensor fascia lata; it runs between gluteus medius and minimus and is at risk during lateral approaches and during surgical mobilisation of the tendons.
Pathophysiology
Mechanism and pathophysiology
Most tears are degenerative. Repetitive tensile load during abduction combines with compressive load from the ITB against the trochanter, producing a zone of tendinopathy near the insertion - directly analogous to the "critical zone" of the supraspinatus. Over time this degenerate tendon undergoes:
- Tendinopathy - intratendinous degeneration without a discrete tear.
- Partial-thickness tear - undersurface (deep) or interstitial fibre failure with the footprint partly intact.
- Full-thickness tear - complete detachment from the facet, with progressive retraction.
- Muscle change - chronic tears develop fatty infiltration and atrophy of the muscle belly, which is largely irreversible and is the strongest predictor of poor repair.
Tensor fascia lata hypertrophy is a recognised compensatory finding: as the gluteus medius fails, the TFL enlarges to maintain abduction, and this hypertrophy on imaging is a useful indirect clue to a significant abductor tear.
The post-arthroplasty abductor
After total hip arthroplasty - especially via a lateral (transgluteal) approach - the abductors can fail by iatrogenic detachment, suture pull-out, attritional wear, or denervation from superior gluteal nerve injury. The result is abductor deficiency, a Trendelenburg gait, and in severe cases recurrent dislocation, because the abductors also contribute to dynamic hip stability. [4]
The superior gluteal nerve runs between gluteus medius and minimus, roughly 3 to 5 cm above the tip of the greater trochanter. Both the original lateral approach and any surgical mobilisation or transfer of the abductors can injure it. Iatrogenic superior gluteal nerve palsy produces an abductor lurch that mimics a tendon tear - assess both tendon integrity and nerve function when a patient limps after hip surgery.
Classification and Grading
There is no single universally adopted classification for gluteal tendon tears; the most useful framework for the exam is to describe tears by tear thickness, retraction, and muscle fatty infiltration, because these are what guide treatment. Several descriptive schemes exist.
- Basis
- Footprint involvement on MRI / at surgery
- Categories
- Partial (undersurface or interstitial) vs full-thickness
- Why it matters
- Partial tears may respond to loading; full-thickness usually needs repair
- Basis
- Pattern of insertional involvement
- Categories
- Non-transfixing partial-extension, transfixing partial-extension, transfixing full-extension
- Why it matters
- Transfixing tears are high-grade and carry more fatty infiltration
- Basis
- Distance of tendon from footprint
- Categories
- Minimal vs significant retraction (often around 2 to 2.5 cm threshold)
- Why it matters
- Greater retraction = harder, less reliable repair
- Basis
- Muscle quality on T1 MRI
- Categories
- Low grade vs high grade fat / atrophy
- Why it matters
- High grade predicts irreparability - favour transfer or graft
Grading Muscle Fatty Infiltration: the Goutallier Scale
The topic repeatedly says fatty infiltration is graded "in a Goutallier-type fashion," and it is the single variable that most changes management - yet the scale itself is worth stating explicitly, because examiners ask candidates to name and apply it to the abductor muscle.
The Goutallier classification was originally described for the rotator-cuff muscles on CT and later adapted to MRI (the Fuchs modification), and the same five grades are applied to the gluteus medius and minimus:
- Grade 0 - normal muscle, no fat.
- Grade 1 - some fatty streaks within the muscle.
- Grade 2 - fatty infiltration present, but muscle bulk still exceeds fat.
- Grade 3 - fat and muscle in roughly equal amounts.
- Grade 4 - fat exceeds muscle.
Why it decides the operation: low-grade change (grades 0 to 2) behaves like a repairable tendon with viable muscle, so suture-anchor repair to the footprint is reasonable. High-grade change (grades 3 to 4) signals a muscle that has been largely replaced by fat - the change is essentially irreversible, the tendon is functionally irreparable, and direct repair is unreliable; this is where graft augmentation or gluteus maximus transfer is preferred. Fatty infiltration is best judged on T1-weighted images, where fat is bright, and it should always be paired with the structural description (thickness, retraction) to reach a decision. The scale is ordinal and shows only moderate inter-observer agreement, so it guides rather than dictates - a point worth conceding in a viva.
When an examiner asks which muscle grading system you would apply to the abductors, answer the Goutallier classification (grades 0 to 4) on T1 MRI, and immediately link it to the decision: grades 0 to 2 favour repair, while grades 3 to 4 (fat equal to or exceeding muscle) mark an irreparable tendon that pushes you towards transfer or graft. Muscle quality, not tear size alone, is the dominant predictor of repair success.
Clinical Presentation and Examination
History
- Chronic lateral hip pain over the greater trochanter, often present for months to years, worse with side-lying, stairs and prolonged single-leg loading.
- Abductor weakness - difficulty climbing stairs, getting out of a car, or a sense of the leg "giving way" laterally.
- A limp is common; patients may describe a waddling or lurching gait.
- In post-arthroplasty patients, a persistent limp, weakness or recurrent dislocation after hip replacement should raise suspicion of an abductor tear.
Examination
- Gait: Trendelenburg gait (pelvis drops on the contralateral swing side) or a compensatory abductor lurch (trunk shifts over the affected hip).
- Trendelenburg test: single-leg stance on the affected side - the contralateral hemipelvis drops, indicating abductor failure.
- Resisted abduction: weak and often painful; weakness (not just pain) suggests a structural tear rather than pure tendinopathy.
- Palpation: point tenderness over the greater trochanter.
- Hip lag sign / abduction lag: inability to hold the leg in passively positioned abduction is described as a clinical predictor of significant abductor damage.
- Hip range of motion: typically preserved (helps distinguish from hip osteoarthritis, which gives groin pain and restricted internal rotation).
Weakness of resisted abduction and a frank Trendelenburg gait push you towards a structural tear. Pure tendinopathy is painful but usually retains reasonable strength.
Gluteal tears give lateral pain with preserved hip ROM; hip OA gives groin pain (C-sign) with restricted, painful internal rotation. The two can coexist.
Radicular pain follows a dermatome below the knee with neurological signs; gluteal tears localise to the trochanter with a mechanical pattern and abductor weakness.
A new or persistent limp, weakness or instability after hip replacement is an abductor tear until proven otherwise - examine gait, abductor power and stability deliberately.
Investigations
Plain films are usually normal but are still worth obtaining to:
- Exclude hip osteoarthritis, fracture and other bony pathology as alternative causes of pain.
- Look for calcific deposits at the trochanter (calcific tendinopathy) and for cortical irregularity or enthesophytes at the insertion.
- Assess implant position in the post-arthroplasty patient.
A normal radiograph does not exclude a tendon tear - the tendon itself is not seen on plain films.
Management
Management is staged: structured rehabilitation first for most partial tears, with surgery reserved for refractory partial tears and for full-thickness tears, and salvage transfer or reconstruction for chronic irreparable disease.
Non-operative management
For partial tears and tendinopathy, non-operative care is first-line and overlaps heavily with greater trochanteric pain syndrome:
- Education and load management - reduce compressive ITB loading (avoid sustained adduction such as crossing legs and side-lying on the affected hip).
- Progressive abductor loading - isometric then isotonic strengthening, sparing aggressive ITB stretching that can increase trochanteric compression.
- Adjuncts - simple analgesia, image-guided corticosteroid injection for short-term pain relief, and platelet-rich plasma in tendinopathy without a full-thickness tear (more durable than corticosteroid in tendinopathy, but not for established full-thickness tears).
Gluteus Maximus Tendon Transfer: How the Salvage Works
The topic names gluteus maximus transfer as the workhorse salvage for the chronic, retracted, fatty, irreparable abductor - but an examiner will ask you to actually describe it and to counsel the patient, so the technique is worth developing.
Principle
When the gluteus medius and minimus are functionally lost (high-grade fatty infiltration and retraction) but the gluteus maximus is intact and innervated by the inferior gluteal nerve, part of gluteus maximus is transferred to reconstruct an active abductor pull across the greater trochanter. It is a dynamic, muscle-based reconstruction rather than a repair of the native tendon.
Technique in outline
- Through a lateral approach, the diseased abductor tendon is debrided and the greater trochanter is prepared to a bleeding bony bed.
- The anterior portion (flap) of gluteus maximus is mobilised on its neurovascular pedicle, preserving the inferior gluteal nerve supply, and advanced anterolaterally over the trochanter. In the classic Whiteside description a gluteus maximus flap alone is used; combined constructs add the posterior part of the tensor fascia lata, and the two flaps are wrapped to recreate an abductor sleeve (the technique described for severe deficiency in revision arthroplasty).
- The flap is secured to the trochanter or to the vastus lateralis / residual abductor stump and tensioned with the hip held in abduction, so that resting tone helps hold the pelvis level.
- Rehabilitation is protected and prolonged, mirroring an abductor repair: restricted weight-bearing with the limb supported in slight abduction and limited active abduction, then graded strengthening, because early loading pulls the transfer out.
What to warn the patient
Transfer reliably improves pain and stability, but it does not restore normal power: residual abductor weakness, a persistent Trendelenburg gait or lurch, and continued reliance on a walking aid are common, and the reconstruction can still fail. This honest counselling - a more comfortable, more stable hip, but not a normal gait - is exactly what examiners want to hear, and it matches the outcomes reported for salvage transfer.
Gluteus maximus transfer is indicated when the medius/minimus are irreparable (high-grade Goutallier fat, retraction) but the maximus is functioning. Say it plainly: mobilise the anterior gluteus maximus flap (with or without the posterior TFL), fix it to the trochanter / vastus lateralis under abduction tension, then protect it for weeks. Counsel that it treats pain and instability more reliably than it restores strength - residual weakness and some limp are the rule, not the exception.
Complications and Outcomes
The main concern, especially in chronic tears with high-grade fatty infiltration, large retraction, obesity, and non-compliance with protected rehabilitation. Muscle quality is the dominant predictor.
Even after successful repair or transfer, residual weakness and a degree of Trendelenburg gait can persist - especially after salvage gluteus maximus transfer for irreparable tears.
Iatrogenic injury during exposure or mobilisation produces denervation weakness that mimics a tendon tear; meticulous technique and respecting the safe zone above the trochanter reduce risk.
Infection, haematoma, prominent or irritating hardware, and the higher overall complication rate reported for open versus endoscopic repair.
Prognosis: appropriately selected partial and full-thickness tears with reasonable muscle quality do well with repair, achieving meaningful pain relief and strength gains by open or endoscopic technique. Chronic, retracted, fatty, irreparable tears do less well and rely on salvage transfer or reconstruction, where pain relief is more reliable than full restoration of strength.
Guidelines, Registries & Global Practice
Global Epidemiology
- Peritrochanteric tendon pathology, including partial and full-thickness gluteus medius/minimus tears, is found in roughly one in five hips on MRI in unselected imaging populations, and is detected more reliably on 3.0-Tesla scanners. [3]
- A strong female predominance and a peak in the sixth and seventh decades are consistent across surgical series worldwide; most tears are degenerative rather than acute.
- Abductor deficiency is a recognised cause of pain, limp and instability after total hip arthroplasty, particularly following lateral (transgluteal) approaches. [4]
Society Guidance Compared
- Diagnosis
- Clinical plus US/MRI for surgical planning
- Repairable tears
- Endoscopic or open suture-anchor repair
- Irreparable / revision
- Graft augmentation or tendon transfer
- Diagnosis
- MRI to grade thickness, retraction, fatty infiltration
- Repairable tears
- Open or endoscopic repair (single/double row)
- Irreparable / revision
- Gluteus maximus transfer, dermal allograft reconstruction
- Diagnosis
- Tendinopathy-to-tear spectrum framing
- Repairable tears
- Repair for full-thickness and refractory partial tears
- Irreparable / revision
- Transfer / reconstruction for chronic retracted tears
- Diagnosis
- MARS MRI / US around implants; exclude nerve injury
- Repairable tears
- Direct abductor repair if early and good tissue
- Irreparable / revision
- Soft-tissue augmentation and tendon transfers
There is broad international agreement that MRI guides surgical decision-making, that repairable tears are treated by open or endoscopic suture-anchor repair with comparable outcomes, and that chronic retracted irreparable tears require salvage transfer or reconstruction. No body endorses a single proven fixation construct.
Registry & Outcome Notes
There is no dedicated gluteal tendon tear registry. Surgical-outcome evidence comes from systematic reviews and case series: open and endoscopic abductor repair give comparable patient-reported outcomes with more complications reported after open surgery [6], and salvage reconstruction with dermal allograft shows promising early results in massive irreparable tears [7]. In the arthroplasty setting, abductor deficiency is an important but under-captured cause of an unhappy hip in registry follow-up, often presenting as persistent limp or instability rather than a discrete revision diagnosis. [4]
High- vs Limited-Resource Practice Variation
- Well-resourced settings: 3.0-T MRI, ultrasound-guided injection, endoscopic and open repair, dermal allograft reconstruction, and tendon-transfer salvage are all available.
- Limited-resource settings: diagnosis leans on clinical assessment (Trendelenburg gait, weak resisted abduction, abduction lag sign) and ultrasound; management emphasises structured abductor loading rehabilitation, with open repair where surgery is available and endoscopic equipment or graft is not. The global priority remains accurate identification of a structural tear so that rehabilitation and surgery are directed appropriately.
Controversies and Areas of Uncertainty
Both achieve similar outcomes, with open surgery carrying higher reported complications. There is no randomised comparison, so technique selection remains surgeon- and tear-dependent.
The optimal fixation construct and the role of graft augmentation (dermal allograft, synthetic mesh) are not defined by high-quality evidence; practice is extrapolated from rotator cuff surgery.
There is no agreed threshold of fatty infiltration or retraction at which to abandon repair for transfer. Decision-making is individualised on muscle quality and patient demand.
Multiple transfer and reconstruction techniques exist for post-arthroplasty abductor deficiency, but comparative evidence is sparse and persistent limp is common whichever is chosen.
Further uncertainty surrounds the prevalence of asymptomatic abductor tears, the prognostic value of MRI grading for predicting repair success, and the place of biologics in established full-thickness tears.
MCQ Practice Points
Q: What is the single best MRI sign of a hip abductor tendon tear?
A: A focus of T2 hyperintensity superior to the greater trochanter. Secondary signs include tendon elongation and discontinuity. 3.0-Tesla MRI detects more tears than 1.5-Tesla.
Q: Which factor most strongly predicts an irreparable tear or failed repair?
A: High-grade muscle fatty infiltration / atrophy (graded in a Goutallier-type fashion). With high-grade fat, direct repair is unreliable and salvage with transfer or graft is preferred.
Q: How do open and endoscopic gluteal repairs compare?
A: Similar patient-reported outcomes, pain and strength, but open repair has a higher reported complication rate. There is no randomised comparison proving one superior (Chandrasekaran systematic review).
Q: What is the workhorse salvage procedure for a chronic, retracted, fatty, irreparable abductor tear with a functioning gluteus maximus?
A: Gluteus maximus tendon transfer. It improves pain but residual abduction weakness and gait abnormality are common. Dermal allograft superior gluteal reconstruction is an alternative.
Q: What should a persistent limp with recurrent dislocation after a lateral-approach THA make you consider?
A: Abductor deficiency from an iatrogenic or attritional abductor tendon tear (or superior gluteal nerve injury). Options include direct repair, dermal allograft augmentation, and tendon transfers.
At a Glance
Gluteal tendon tears are structural tears of the gluteus medius and minimus tendons at their insertion on the greater trochanter - often called the rotator cuff of the hip because they mirror supraspinatus pathology. They typically affect women aged 50 to 70 and present as chronic lateral hip pain with abductor weakness, a Trendelenburg gait and difficulty single-leg standing. They are the structural, surgical end of a spectrum whose milder forms (tendinopathy and bursitis) are covered under greater trochanteric pain syndrome. MRI is the reference standard, characterising tear thickness, retraction and - most importantly - muscle fatty infiltration, which predicts reparability. Partial tears are managed with loading rehabilitation and repaired (open or endoscopic) if they fail; full-thickness tears are repaired with suture anchors; massive irreparable tears with high-grade fatty change are salvaged with graft augmentation or gluteus maximus tendon transfer. A distinct and high-yield setting is abductor deficiency after total hip arthroplasty, where attritional or iatrogenic tears cause limp and instability and may need repair, transfer or reconstruction.
WOMANWho Tears - WOMAN
Hook:A WOMAN with a Trendelenburg gait - think abductor tendon tear, not bursitis
GRADEReparability Factors - GRADE
Hook:GRADE the tear before you promise a repair - fatty infiltration is the dealbreaker
GRAFTSalvage Ladder - GRAFT
Hook:When you cannot repair, climb the GRAFT ladder - transfer and augmentation over heroic direct repair
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Classic chronic gluteal tendon tear presentation. The examiner wants a structured work-up that distinguishes a structural tear from tendinopathy and uses imaging to drive management.”
“The examiner is testing conceptual understanding linking shoulder and hip tendon pathology.”
“High-yield post-arthroplasty scenario testing recognition and management of abductor deficiency, including transfer and reconstruction options.”
“Tests knowledge of the comparative evidence and how to apply it.”
KEY CONCEPT
- Rotator cuff of the hip - gluteus medius/minimus tendon tears
- Structural/surgical end of the spectrum (vs tendinopathy/bursitis in GTPS)
- Female predominance, age 50-70, usually degenerative
- Fatty infiltration is the key predictor of reparability
ANATOMY
- Gluteus medius to lateral and superoposterior facets of GT
- Gluteus minimus to anterior facet
- Tendons lie deep to the ITB (compressive load)
- Superior gluteal nerve runs between medius and minimus - at risk
CLINICAL FEATURES
- Chronic lateral hip pain plus abductor WEAKNESS
- Trendelenburg gait and positive Trendelenburg test
- Weak resisted abduction; abduction lag sign
- Preserved hip ROM (helps exclude hip OA)
- Suspect after lateral-approach THA with limp/instability
INVESTIGATIONS
- Radiographs usually normal - exclude OA, calcific deposits, check implant
- MRI is reference standard - grade thickness, retraction, fatty infiltration
- Best MRI sign: T2 hyperintensity superior to greater trochanter
- 3.0-T MRI detects more tears than 1.5-T
- Ultrasound for dynamic assessment and around implants
MANAGEMENT
- Partial tears: load management + progressive abductor rehab first
- Full-thickness / refractory partial: suture-anchor repair
- Open and endoscopic repair give SIMILAR outcomes
- Open repair has higher reported complication rate
- Protected, prolonged rehabilitation after repair
SALVAGE / IRREPARABLE
- Irreparable = high-grade fatty infiltration + retraction
- Dermal allograft superior gluteal reconstruction
- Gluteus maximus tendon transfer (functioning maximus)
- Combined Gmax + TFL transfer in revision THA
- Counsel about residual weakness / limp
Evidence Base
- Open and endoscopic repair give similar patient-reported outcomes and strength
- Open repair carries a higher reported complication rate
- No randomised comparison exists to declare one technique superior
- Repair (open or endoscopic) is first-line surgery for repairable tears
- Gluteus maximus transfer is a salvage option for irreparable tears
- Evidence is still insufficient to mandate a specific fixation construct or graft
- About one in five hips show peritrochanteric tendon pathology on MRI
- 3.0-T MRI detects significantly more tears than 1.5-T
- Abductor pathology associates with muscle atrophy and osteoarthritis
- Dermal allograft reconstruction is an option for massive irreparable tears
- Promising short-term outcomes including in revision cases
- Small series and short follow-up limit strength of conclusions
Suggested Reading
- Harrasser N, Banke I, Gollwitzer H, et al. Gluteal insufficiency: pathogenesis, diagnosis and therapy. Z Orthop Unfall. 2016;154(2):140-147. doi:10.1055/s-0041-110812
- Morgan A, Moore M, Derry K, et al. Surgical treatment and outcomes for gluteal tendon tears. Curr Rev Musculoskelet Med. 2024;17(6):157-170. doi:10.1007/s12178-024-09896-w
- Oehler N, Ruby JK, Strahl A, et al. Hip abductor tendon pathology visualized by 1.5 versus 3.0 Tesla MRIs. Arch Orthop Trauma Surg. 2020;140(2):145-153. doi:10.1007/s00402-019-03228-1
- Elbuluk AM, Coxe FR, Schimizzi GV, et al. Abductor deficiency-induced recurrent instability after total hip arthroplasty. JBJS Rev. 2020;8(1):e0164. doi:10.2106/JBJS.RVW.18.00164
- Bitar AC, Guimaraes JB, Marques R, et al. Clinical and radiological results after endoscopic treatment for gluteal tendon injuries with a minimum follow-up of 12 months. Arch Bone Jt Surg. 2023;11(10):641-648. doi:10.22038/ABJS.2023.70495.3304
- Chandrasekaran S, Lodhia P, Gui C, et al. Outcomes of open versus endoscopic repair of abductor muscle tears of the hip: a systematic review. Arthroscopy. 2015;31(10):2057-2067. doi:10.1016/j.arthro.2015.03.042
- Browning RB, Clapp IM, Alter TD, et al. Superior gluteal reconstruction results in promising outcomes for massive abductor tendon tears. Arthrosc Sports Med Rehabil. 2021;3(5):e1321-e1327. doi:10.1016/j.asmr.2021.05.013
- Burns DM, Bornes TD, Al Khalifa A, et al. Surgical technique: abductor reconstruction with gluteus maximus and tensor fascia lata in revision total hip arthroplasty. J Arthroplasty. 2022;37(7S):S628-S635. doi:10.1016/j.arth.2022.03.006
- Lindner D, Shohat N, Botser I, et al. Clinical presentation and imaging results of patients with symptomatic gluteus medius tears. J Hip Preserv Surg. 2015;2(4):310-315. doi:10.1093/jhps/hnv035
- Caviglia H, Cambiaggi G, Vattani N, et al. Lesion of the hip abductor mechanism. SICOT J. 2016;2:29. doi:10.1051/sicotj/2016020