Iron Overload | Hook Osteophytes | 2nd & 3rd MCP Joints | HFE C282Y
- Iron overload (usually HFE C282Y homozygosity) drives a degenerative arthropathy that mimics osteoarthritis in unusual joints
- 2nd and 3rd MCP joints are the classic site - OA here in a middle-aged person should prompt iron studies
- Hook-shaped osteophytes on the radial side of the metacarpal heads are near-pathognomonic
- Strong overlap with chondrocalcinosis / CPPD - both can coexist
- Venesection treats the systemic disease but does NOT reverse established arthropathy - joint damage progresses
- “Squared metacarpal heads with hook osteophytes at 2nd/3rd MCP = think haemochromatosis
- “Screen with transferrin saturation (best initial test) and ferritin, then HFE genotyping
- “Arthropathy is often the presenting and most disabling feature - and the least reversible
- “Joint replacement works well; iron overload is not a contraindication to arthroplasty
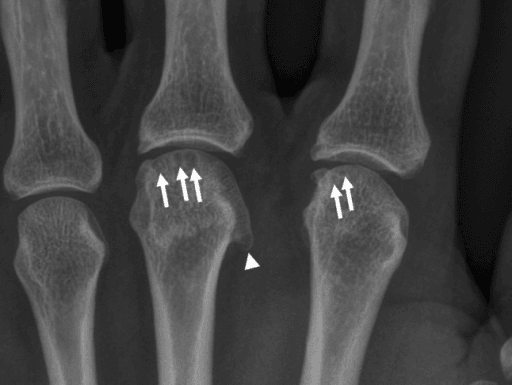
Squared metacarpal heads with hook-shaped osteophytes on the radial side of the 2nd and 3rd MCP heads, joint space narrowing and subchondral cysts. This pattern of "OA" in the MCP joints of a middle-aged person is a classic exam trigger - the answer is usually haemochromatosis.
Order transferrin saturation (best initial screen) and ferritin in anyone with MCP osteoarthritis, unexplained chondrocalcinosis, or premature large-joint OA, then confirm with HFE genotyping. Arthralgia often precedes the diagnosis by many years.
Venesection prevents and can reverse liver, cardiac and endocrine damage, but does NOT halt or reverse established arthropathy. This dissociation is a favourite viva point - manage joints on their own merits.
Haemochromatosis is one of the recognised metabolic causes of calcium pyrophosphate deposition (CPPD). Patients can present with acute pseudogout, and chondrocalcinosis is common. The two arthropathies share bone-centred pathogenic pathways.
IRONHaemochromatosis Arthropathy Features
Hook:IRON in the joints leaves a permanent mark!
BRONZESystemic Features of Haemochromatosis
Hook:A BRONZE patient with stiff knuckles - hunt for iron!
Overview and Epidemiology
Haemochromatosis arthropathy is the joint disease caused by hereditary (primary) haemochromatosis, an inherited disorder of iron metabolism in which excessive intestinal iron absorption leads to progressive tissue iron overload. Iron accumulates in many organs - liver, pancreas, heart, pituitary, skin - and also in synovium and cartilage, where it produces a distinctive degenerative arthropathy. The arthropathy is clinically important to orthopaedic surgeons because it is frequently the presenting feature, mimics osteoarthritis in unusual joints, and is largely irreversible even when the underlying iron overload is treated.
- Most cases are due to homozygosity for the C282Y mutation in the HFE gene (chromosome 6); compound heterozygosity (C282Y/H63D) is a less penetrant cause
- HFE dysfunction reduces hepcidin, the master iron-regulatory hormone, leading to unrestrained ferroportin-mediated iron export and absorption
- Autosomal recessive inheritance; clinical penetrance is incomplete and modified by sex, blood loss and alcohol
- One of the commonest inherited disorders in people of Northern European ancestry; C282Y homozygosity occurs in roughly 1 in 200 to 1 in 400 of this population
- Much rarer in South American, African and East Asian populations, where the HFE C282Y mutation is uncommon - the diagnostic algorithm differs there
- Joint pain is reported by around 70-75% of patients with iron overload and often precedes the diagnosis by years
- Men present earlier and more severely than women, who are partially protected by menstrual and pregnancy blood loss
In a large cohort, joint pain was present in 72% of haemochromatosis patients and preceded the diagnosis of haemochromatosis by an average of about 9 years. The orthopaedic surgeon or rheumatologist is therefore well placed to make the diagnosis early - look for MCP osteoarthritis and chondrocalcinosis and order iron studies.
Primary versus Secondary Iron Overload
The disease discussed here is hereditary (primary) haemochromatosis, but iron-overload arthropathy can also arise from secondary (acquired) iron loading, and the distinction changes the genetics, the systemic context and, importantly, the treatment.
- Mechanism / examples
- Autosomal recessive; C282Y homozygosity (commonest) or compound C282Y/H63D
- Iron-removal treatment
- Venesection (phlebotomy)
- Mechanism / examples
- Juvenile haemochromatosis (hemojuvelin HJV, hepcidin HAMP) - young, severe cardiac and gonadal failure; transferrin-receptor-2 (TFR2); ferroportin disease (SLC40A1, autosomal dominant)
- Iron-removal treatment
- Venesection (chelation if not tolerated)
- Mechanism / examples
- Repeated transfusion for thalassaemia major, sickle cell disease, myelodysplasia or aplastic anaemia
- Iron-removal treatment
- Iron chelation - an anaemic patient cannot be venesected
- Mechanism / examples
- Ineffective erythropoiesis (e.g. thalassaemia intermedia) increases gut iron absorption
- Iron-removal treatment
- Chelation, with selective venesection only if tolerated
- Mechanism / examples
- Chronic liver disease, excess parenteral or dietary iron, porphyria cutanea tarda
- Iron-removal treatment
- Treat the cause; venesection if not anaemic
Primary (hereditary) iron overload is treated by venesection. In secondary transfusional overload the patient is anaemic, so venesection is impossible and iron chelation is used instead. Juvenile (non-HFE) haemochromatosis presents young with severe cardiac and endocrine disease. All forms can produce an iron arthropathy and chondrocalcinosis.
Pathophysiology
The arthropathy results from chronic iron deposition in joint tissues. Unlike gout or CPPD, the dominant mechanism appears to be iron-driven damage to bone and cartilage cells rather than a single crystal trigger, although crystal disease frequently coexists.
Iron handling and the joint
Systemic iron loading:
- Loss of HFE function lowers hepcidin, so enterocytes and macrophages export iron unchecked via ferroportin
- Transferrin becomes saturated and non-transferrin-bound iron circulates, depositing in parenchymal tissues including synovium and cartilage
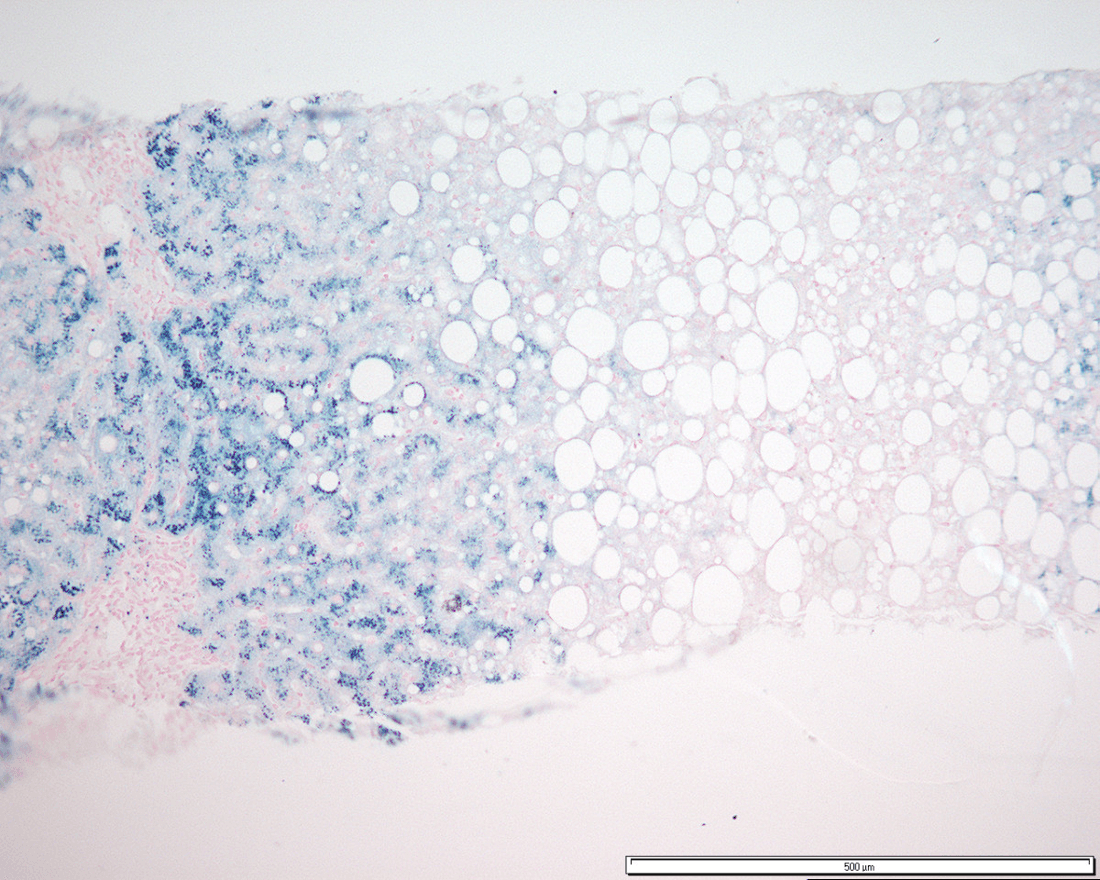
- Iron is visible histologically as haemosiderin in synovial lining cells and chondrocytes, and as low-signal "blooming" foci on T2*-weighted MRI
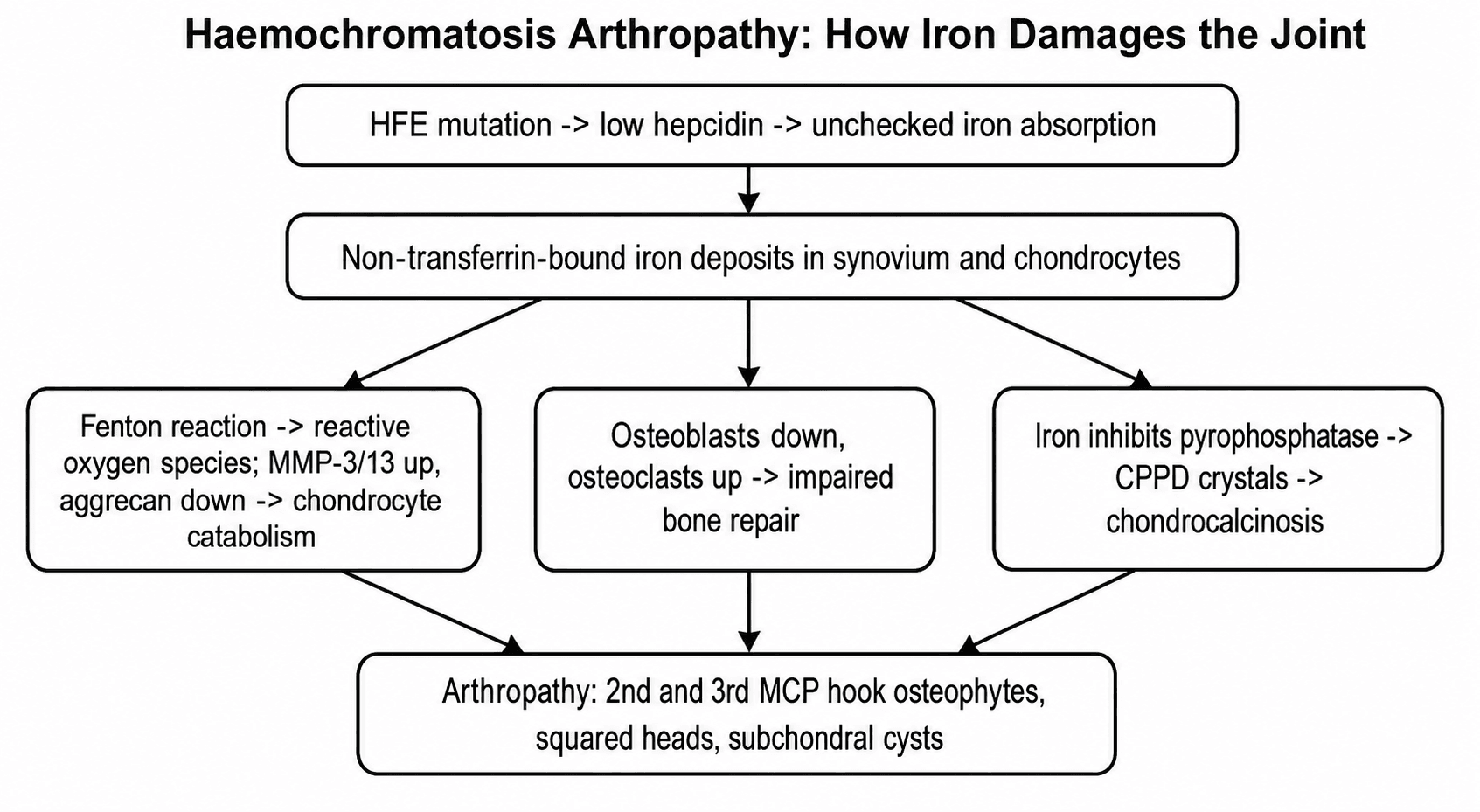
How iron damages the joint
- Excess intracellular iron catalyses reactive oxygen species (Fenton chemistry), causing oxidative stress
- In chondrocytes, iron exposure increases catabolic enzymes (matrix metalloproteinases such as MMP3 and MMP13), reduces extracellular matrix and aggrecan production, and pushes cells toward a hypertrophic, osteoarthritis-like phenotype
- Iron-loaded synovium becomes inflamed and contributes to cartilage breakdown
- Iron overload reduces osteoblast alkaline phosphatase activity and increases osteoclastogenesis, producing generalised bone loss and impaired joint repair
- These abnormalities in bone turnover and damage/repair are strikingly similar to those seen in CPPD, which may explain why the two diseases overlap and why haemochromatosis arthropathy can occur even without demonstrable CPP crystals
Link with calcium pyrophosphate deposition
- Haemochromatosis is one of the classic metabolic associations of CPPD
- Iron may inhibit pyrophosphatases or otherwise favour calcium pyrophosphate crystal formation, and shared effects on bone cells link the two
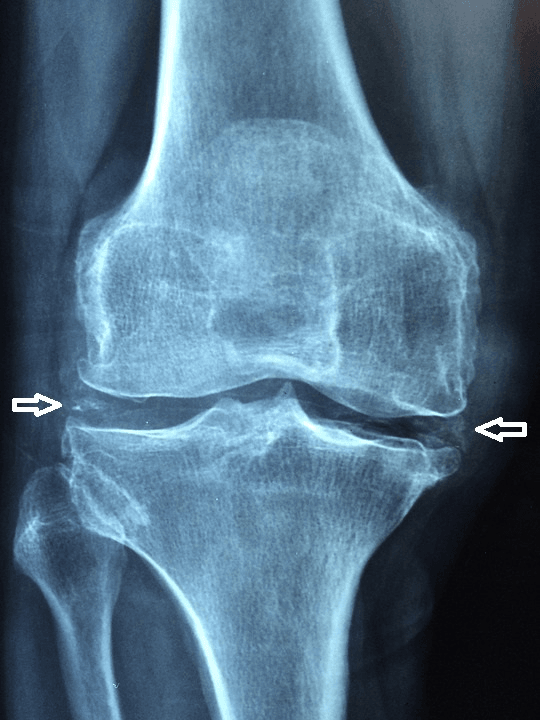
- Chondrocalcinosis is a common radiographic finding, and acute pseudogout attacks can occur
By the time arthropathy is clinically apparent, iron has already triggered chondrocyte catabolism, matrix loss and disordered bone remodelling. Removing circulating iron by venesection halts ongoing systemic damage but cannot reverse established cartilage and bone destruction - so the arthropathy characteristically progresses despite adequate iron-depletion therapy.
Metabolic Causes of CPPD (Chondrocalcinosis)
Because haemochromatosis is one of the metabolic causes of calcium pyrophosphate deposition, finding chondrocalcinosis - especially in a younger patient (under about 55), when it is florid or polyarticular, or in atypical joints - should prompt a screen for the secondary metabolic causes, not just haemochromatosis.
- Screening test
- Transferrin saturation, ferritin, HFE genotype
- Clue
- 2nd/3rd MCP hook osteophytes, systemic iron features
- Screening test
- Calcium and parathyroid hormone (PTH)
- Clue
- Hypercalcaemia, subperiosteal resorption, 'stones, bones, groans'
- Screening test
- Serum magnesium
- Clue
- Malabsorption, diuretics, Gitelman syndrome
- Screening test
- Alkaline phosphatase (characteristically low)
- Clue
- Low alkaline phosphatase, premature dental loss, fractures
- Screening test
- Thyroid-stimulating hormone (TSH)
- Clue
- A recognised but weaker association
Ageing and osteoarthritis are by far the commonest setting for CPPD overall, and familial forms (ANKH gene mutations) exist; but it is the metabolic causes above - haemochromatosis being the surgically important one - that must not be missed in a young or atypical presentation.
Chondrocalcinosis in a patient under about 55, or that is florid, polyarticular or in atypical joints, warrants a metabolic screen: haemochromatosis (iron studies), hyperparathyroidism (calcium and PTH), hypomagnesaemia (magnesium), hypophosphatasia (alkaline phosphatase) and hypothyroidism (TSH). Haemochromatosis is the one with surgical consequences.
HHHHMetabolic Screen for the Stiff Middle-Aged Joint
Hook:The 4 H's behind unexplained chondrocalcinosis - Haemochromatosis is the surgical one!
Clinical Presentation
Small-joint disease (the classic pattern)
- Insidious pain, stiffness and bony swelling of the 2nd and 3rd metacarpophalangeal joints
- Often bilateral and symmetrical; reduced grip and difficulty making a fist
- Wrists are also commonly involved
- The pattern resembles osteoarthritis but in joints that primary OA usually spares
Large-joint disease
- Hips, knees, ankles and shoulders may develop a destructive OA-like arthropathy
- Ankle involvement is increasingly recognised and can be a major source of disability
- Large-joint disease is a frequent reason for joint replacement, sometimes at a relatively young age
Acute presentations
- Acute pseudogout (acute CPP crystal arthritis) from coexisting chondrocalcinosis - a hot, swollen joint (often knee or wrist)
- Acute monoarthritis must always be distinguished from septic arthritis
Associated systemic features (the diagnostic context)
- Liver: hepatomegaly, deranged liver function, cirrhosis, hepatocellular carcinoma
- Pancreas: diabetes mellitus ("bronze diabetes")
- Skin: bronze or slate-grey pigmentation
- Heart: cardiomyopathy, arrhythmia
- Endocrine/gonadal: hypogonadism, impotence, fatigue
- Haematology: a high-normal or raised mean corpuscular volume (MCV) is associated with the presence of arthritis in haemochromatosis
Physical examination
- Bony enlargement of the 2nd/3rd MCP joints; squared knuckles
- Effusions in larger joints during acute crystal attacks
- Look for skin pigmentation and stigmata of chronic liver disease
- Hard, bony swelling rather than boggy synovitis (synovitis is the minority)
- Reduced range and grip; crepitus in established large-joint OA
Investigations
Biochemical screening for iron overload
- Transferrin saturation - the most useful initial screening test; a fasting value above approximately 45% in women or 50% in men is suggestive
- Serum ferritin - reflects iron stores but is an acute-phase reactant, so interpret with transferrin saturation
- HFE genotyping - C282Y homozygosity (or compound C282Y/H63D heterozygosity) confirms hereditary haemochromatosis in a patient with biochemical iron overload
- In populations where C282Y is rare, or with non-HFE genotypes, MRI quantification of hepatic iron or liver biopsy is used to demonstrate iron overload
- Assess end-organ damage: liver function, fasting glucose/HbA1c, and fibrosis staging
Synovial fluid (if acute hot joint)
- Send for crystals and culture - to identify coexisting CPP crystals (rhomboid, positively birefringent) and to exclude sepsis
- Crystals never exclude infection; treat as septic if in doubt
Imaging
- Squared metacarpal heads with hook-shaped osteophytes on the radial aspect of the 2nd and 3rd metacarpal heads (near-pathognomonic)
- Subchondral cysts and uniform joint space narrowing
- Chondrocalcinosis in wrists, knees, symphysis pubis and other fibrocartilage
- Large joints: OA-like changes (sometimes severe, sometimes at unusually young age)
- T2*-weighted ("gradient-echo") sequences show low-signal blooming from iron/haemosiderin in synovium
- Demonstrates associated cartilage loss, meniscal and ligamentous changes
Differential diagnosis of the small-joint arthropathy
The exam test is to recognise that "osteoarthritis" of the MCP joints is not ordinary OA.
- Key Pointers
- 2nd/3rd MCP, hook osteophytes, chondrocalcinosis, systemic iron features
- Decisive Test
- Transferrin saturation and ferritin, then HFE genotyping
- Key Pointers
- DIP and PIP joints (Heberden/Bouchard nodes), spares MCP
- Decisive Test
- Clinical distribution and radiographs
- Key Pointers
- Symmetrical MCP/wrist synovitis, erosions, soft-tissue swelling
- Decisive Test
- Rheumatoid factor, anti-CCP, ESR/CRP
- Key Pointers
- Chondrocalcinosis, pseudogout attacks, knee/wrist
- Decisive Test
- Synovial fluid CPP crystals; consider it a marker - screen for haemochromatosis
- Key Pointers
- 1st MTP podagra, tophi, hyperuricaemia, punched-out erosions
- Decisive Test
- Synovial fluid urate crystals
Management
Treating the Iron Overload
- First-line treatment for hereditary haemochromatosis
- Induction phlebotomy until iron stores are depleted (target ferritin low, e.g. below approximately 50 micrograms/L during induction), then maintenance
- Prevents and can reverse liver, cardiac and endocrine damage and improves survival when started before cirrhosis
- Iron-chelation therapy (e.g. deferasirox) is an alternative, mainly when anaemia precludes venesection
- Erythrocytapheresis is used in some centres
Counsel patients explicitly: venesection protects the liver, heart and pancreas but the arthropathy commonly progresses regardless. Joint symptoms must be managed in their own right, and persistent or worsening joint pain is not a sign of failed iron control.
This section covers control of the underlying iron overload.
Surgical Management
Indications for Surgery
- End-stage large-joint OA (hip, knee, ankle, shoulder) with pain and functional loss refractory to conservative care
- Disabling MCP/hand disease - selected cases may benefit from hand surgery, though small-joint reconstruction is less commonly required
- Mechanical derangement - e.g. meniscal pathology or loose bodies
Joint Replacement in Haemochromatosis
- Iron overload is not a contraindication to arthroplasty; outcomes are generally good
- Joint replacement is common in this population - in cohort data around 16% of patients underwent total joint replacement for severe OA, at a mean age in the late 50s
- Female sex, MCP joint involvement and chondrocalcinosis predict earlier joint failure and the need for replacement
- Optimise iron control and assess hepatic, cardiac and endocrine status before elective surgery (liver disease affects anaesthetic and bleeding risk)
- Screen for and plan for diabetes and cardiomyopathy
- Exclude active crystal arthritis or infection before implanting a prosthesis
This section covers arthroplasty in haemochromatosis.
Complications
Disease Complications
- Progressive joint destruction despite iron-depletion therapy
- Acute pseudogout flares from coexisting CPPD
- Generalised bone loss / osteoporosis related to iron effects on bone cells and hypogonadism
- Systemic morbidity: cirrhosis, hepatocellular carcinoma, diabetes, cardiomyopathy, hypogonadism - all relevant to perioperative risk
Surgical Complications
- Increased anaesthetic and bleeding risk in patients with significant liver disease
- Impaired glycaemic control and infection risk in those with diabetes
- Standard arthroplasty risks; crystal flare can occur perioperatively
- Continued symptoms in other joints as the systemic arthropathy progresses
Guidelines, Registries and Global Practice
Haemochromatosis arthropathy is a global disease wherever iron overload occurs, but the genetic background and diagnostic algorithm differ by population. International guidance agrees on two principles: detect and treat iron overload early to protect the liver and heart, and manage the joints on their own merits because the arthropathy is largely irreversible.
Global epidemiology
- HFE C282Y homozygosity is common in people of Northern European ancestry (roughly 1 in 200 to 1 in 400) and is the dominant cause there.
- In South American, African and East Asian populations the C282Y mutation is rare, so diagnosis relies more on biochemical iron overload plus MRI-quantified hepatic iron or biopsy and consideration of non-HFE genotypes.
- Joint pain affects around 70-75% of patients with iron overload and frequently precedes diagnosis by years.
Side-by-side guidance
- Region
- Europe
- Emphasis
- C282Y homozygosity plus raised transferrin saturation/ferritin diagnoses HH; non-C282Y needs hepatic iron on MRI/biopsy; early phlebotomy prevents complications including arthropathy
- Region
- International
- Emphasis
- Transferrin saturation is the best initial screen; screen patients with MCP OA or unexplained chondrocalcinosis
- Region
- International
- Emphasis
- Iron overload is not a contraindication to arthroplasty; optimise liver, cardiac and diabetic status and exclude infection/crystal flare first
Registry and arthroplasty evidence
- Large arthroplasty registries (NJR, AOANJRR, AJRR, Swedish/Norwegian) do not list haemochromatosis as a distinct indication, but cohort data show joint replacement is common (about 16% of patients) with generally good results, driven by severe large-joint OA.
- Implication: standard implant and bearing selection applies; haemochromatosis changes perioperative medical optimisation, not prosthesis choice.
High- vs limited-resource practice variation
- Well-resourced settings: HFE genotyping, MRI iron quantification and structured venesection programmes are readily available; T2*-weighted MRI can demonstrate joint iron.
- Limited-resource settings: diagnosis often rests on transferrin saturation, ferritin and plain radiographs (the hook-osteophyte pattern); venesection remains low-cost and effective, while chelation is reserved for those who cannot be venesected.
- Everywhere: recognise the MCP/chondrocalcinosis pattern, screen for iron overload, treat systemic disease early, and screen first-degree relatives.
Controversies and Areas of Uncertainty
Haemochromatosis arthropathy remains incompletely understood, which makes it good higher-order viva material.
- Exact mechanism of joint damage: whether iron acts mainly through direct chondrocyte toxicity, through disordered bone remodelling, or via promotion of CPP crystals is still debated; animal models do not always reproduce direct cartilage damage.
- Relationship with CPPD: the two diseases overlap clinically and share bone-centred pathways, but it is unclear how much of the arthropathy is "iron arthropathy" versus secondary CPPD.
- No joint-specific therapy: nothing reliably removes iron from cartilage or reverses the arthropathy; iron chelation has not been shown to treat the established joint disease.
- Whom and when to screen: the yield of iron studies in isolated hand OA versus the value of early detection (to protect the liver and heart) influences screening thresholds, which vary between guidelines.
- Optimal timing of large-joint surgery in patients who may also have liver disease and diabetes is individualised, with limited high-level evidence.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old man is referred with painful, stiff index and middle finger knuckles. Hand radiographs show squared metacarpal heads with hook-shaped osteophytes at the 2nd and 3rd MCP joints, joint space narrowing and subchondral cysts. He also mentions fatigue and reduced libido.”
“A 60-year-old woman with known haemochromatosis presents with an acutely painful, swollen, warm right knee. Radiographs show chondrocalcinosis of the menisci. She is afebrile.”
“A 56-year-old man with hereditary haemochromatosis has end-stage osteoarthritis of the hip and is listed for total hip arthroplasty. How do you approach his perioperative care?”
“You are shown a hand radiograph with squared metacarpal heads, hook-shaped osteophytes on the radial side of the 2nd and 3rd metacarpal heads, subchondral cysts and chondrocalcinosis. What is the diagnosis and what would you do?”
Signature Radiograph
- Squared metacarpal heads, 2nd and 3rd MCP joints
- Hook-shaped osteophytes on the radial metacarpal heads (near-pathognomonic)
- Subchondral cysts and joint space narrowing
- Chondrocalcinosis (wrist, knee, symphysis pubis)
Genetics and Cause
- Hereditary haemochromatosis, autosomal recessive
- Most cases: HFE C282Y homozygosity
- Low hepcidin leads to iron overload
- Iron deposits in synovium and cartilage
Screening Tests
- Transferrin saturation - best initial screen
- Serum ferritin (acute-phase reactant)
- HFE genotyping to confirm
- MRI hepatic iron or biopsy if non-C282Y
Key Associations
- CPPD / chondrocalcinosis overlap and pseudogout
- Liver (cirrhosis, HCC), diabetes, cardiomyopathy
- Hypogonadism, fatigue, bronze skin
- Raised MCV associated with arthritis
Management
- Venesection for iron overload (does NOT reverse joints)
- Symptomatic joint care: analgesia, hand therapy, NSAIDs
- Arthroplasty for end-stage large-joint OA
- Screen first-degree relatives
Exam Traps
- Do not call MCP OA 'ordinary osteoarthritis'
- Venesection treats organs, not the arthropathy
- Exclude sepsis in any acute hot joint
- Iron overload is not a contraindication to arthroplasty
Evidence Base
Musculoskeletal Disease Burden of Hereditary Haemochromatosis
- Joint pain reported by 72.4% of patients; mean age at first joint symptoms 45.8 years
- Joint pain preceded the diagnosis of haemochromatosis by a mean of about 9 years
- Joint replacement was common: 16.1% underwent total joint replacement for severe OA (mean age 58.3 years)
- Female sex, MCP joint involvement and chondrocalcinosis were associated with higher risk of early joint failure
HFE H63D Variant Predisposes to Arthralgia, Chondrocalcinosis and Osteoarthritis
- H63D homozygotes had more arthralgia, oligoarthralgia and Heberden's nodes than non-carriers
- In those aged 65 or younger, H63D homozygotes had more chondrocalcinosis in hip/knee and more hand osteophytes and OA
- Compound heterozygotes showed more arthralgia and hip chondrocalcinosis at older ages
- HFE variants may partly explain population-level arthralgia, chondrocalcinosis and hand OA
Common Pathogenic Pathways in Haemochromatosis Arthritis and CPPD
- Haemochromatosis arthritis and CPPD share joint distribution, low-grade synovial inflammation and generalised bone loss
- Excess iron damages chondrocytes and bone cells in vitro
- Iron reduces osteoblast alkaline phosphatase activity and increases osteoclastogenesis - changes also seen in CPPD
- Shared pathways relate more to bone and damage/repair than to direct cartilage damage
Effects of Iron Overload in Human Joint Tissue Explants and Animal Models
- Iron exposure increased catabolic gene expression (MMP13) in cartilage with stable chondrocyte viability
- Synovium showed increased GAG content and inflammation markers with iron
- Hfe, Tfr2 and diet-induced iron-overload mice developed spontaneous OA with proteoglycan loss and higher Mankin scores
- Supports iron modulation as a potential therapeutic strategy for OA
Hfe-KO Chondrocytes Show Increased Iron Uptake and an OA-Related Phenotype
- Iron exposure increased metalloprotease expression and reduced matrix and aggrecan production
- Hfe-KO chondrocytes showed greater iron accumulation and higher MMP3 (more catabolism)
- Iron pushed chondrocytes toward a hypertrophic phenotype with increased collagen I and reduced Sox9
- High iron, especially with HFE loss of function, favours an osteoarthritis-related phenotype
EASL Clinical Practice Guidelines on Haemochromatosis
- C282Y homozygosity with raised transferrin saturation and ferritin is sufficient to diagnose haemochromatosis
- Non-C282Y genotypes require demonstration of hepatic iron overload on MRI or biopsy
- Early phlebotomy can prevent cirrhosis, hepatocellular carcinoma, diabetes and arthropathy
- Phlebotomy targets: ferritin below 50 micrograms/L (induction) and below 100 micrograms/L (maintenance)
Overview of Ankle Arthropathy in Hereditary Haemochromatosis
- Arthropathy mainly involves MCP and ankle joints, less often hip and knee
- Ankle radiographic signs often do not differ from primary osteoarthritis
- Surgery (arthrodesis or total ankle arthroplasty) is the mainstay for end-stage ankle disease
- Iron-homeostasis therapy may help prevent arthropathy but conclusive data are lacking
Arthropathy in Haemochromatosis Segregates with Elevated Mean Corpuscular Volume
- MCV was higher in haemochromatosis patients with arthritis than those without (95 vs 92.75 fL)
- Haemochromatosis patients had higher MCV than non-haemochromatosis OA and RA controls
- An MCV of 97.85 fL or above gave a likelihood ratio of 2.2 for arthritis in haemochromatosis
- Suggests a relationship between erythrocyte parameters and arthropathy in incident haemochromatosis