The Other Side of Instability
- HAGL stands for Humeral Avulsion of the Glenohumeral Ligament.
- It is a cause of recurrent instability often missed on standard MRI.
- The 'J Sign' on coronal oblique MRI is pathognomonic.
- It is frequently associated with subscapularis tears (Open repair addresses both).
- Failure to recognize HAGL leads to failed Bankart repairs.
- “In a patient with instability but NO Bankart lesion, look for the HAGL.
- “Arthroscopic repair is technically demanding (70-degree scope helps).
- “Open repair is the historical gold standard.
"Bankart Negative Instability" A patient presents with recurrent anterior instability. MRI report says "No labral tear". DO NOT dismiss as "functional" or "MDI". Review the MRI specifically for the J Sign. The IGHL may be stripped from the humerus.
Failed Stabilization. Performing a Bankart repair on a HAGL patient will FAIL. You are tightening the wrong side of the hammock. The instability persists.
- Bankart Lesion
- Glenoid (Labrum)
- HAGL Lesion
- Humerus (Neck)
- Bankart Lesion
- Labral detachment
- HAGL Lesion
- Ligament avulsion
- Bankart Lesion
- 80-90%
- HAGL Lesion
- 2-9%
- Bankart Lesion
- Anterior Scope
- HAGL Lesion
- Anterior Open / 5 O'clock Scope
JUMPMRI Signs
Hook:JUMP to the diagnosis.
SHAGAssociations
Hook:SHAG lesions (Shoulder HAGL).
Overview
A HAGL lesion (Humeral Avulsion of the Glenohumeral Ligament) is a traumatic detachment of the inferior glenohumeral ligament (IGHL) complex from its insertion on the anatomical neck of the humerus.
This lesion was once considered rare or a "lesion of exclusion," but modern MRI techniques and arthroscopic vigilance have revealed it to be a significant contributor to recurrent instability, particularly in contact athletes. It represents the "humeral side" of the capsular failure spectrum.
While the classic Bankart lesion involves the glenoid side of the IGHL complex, the HAGL lesion represents failure at the humeral insertion. It is a potent cause of anterior instability because the "hammock" of the IGHL is disabled.
Glenohumeral stability is a balance the exam loves to test, because it explains why a HAGL matters yet mid-range stability can be normal:
- Static (passive) stabilisers: the bony glenoid (shallow, so it contributes little alone), the labrum (deepens the socket by roughly 50 percent and forms a chock-block and suction seal), the negative intra-articular pressure and adhesion-cohesion of the synovial fluid, and the capsuloligamentous complex (SGHL, MGHL, IGHL) acting mainly as end-range check-reins.
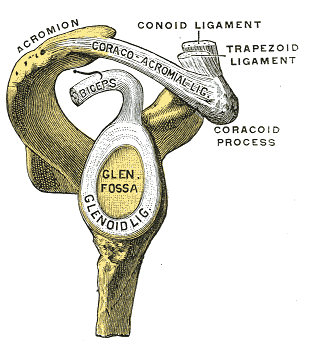
- Dynamic (active) stabilisers: the rotator cuff producing concavity-compression (pressing the convex head into the concave glenoid), the long head of biceps, and scapular positioning by the periscapular muscles keeping the glenoid under the head.
In the mid range the dynamic cuff centres the head; at end range (ABER) the static IGHL takes over. A HAGL is a failure of that end-range static restraint - so the shoulder feels stable in mid-range but apprehensive in abduction-external rotation.
Pathophysiology and Mechanisms
IGHL Complex
- Anterior Band: The primary restraint to anterior translation in abduction and external rotation (ABER). Requires restoration.
- Posterior Band: Restraint to posterior translation in flexion/internal rotation.
- Axillary Pouch: The hammock between the bands.
The IGHL inserts onto the humeral neck, just below the articular surface.
This insertion is the "weak link" in HAGL lesions.
Humeral Insertion Anatomy
- Location: Anatomical neck, approximately 1-2 cm from articular margin.
- Width: The IGHL insertion spans 2-3 cm along the humeral neck.
- Blood Supply: Branches of anterior circumflex humeral artery.
- Surgical Relevance: Anchors must be placed at the anatomical footprint for restoration.
Understanding this anatomy is critical for proper anchor placement during repair.
The IGHL that avulses in a HAGL is one of three discrete capsular thickenings - examiners expect you to place it in the complete complex and say what each restrains, because the dominant restraint changes with arm position:
- Superior glenohumeral ligament (SGHL): primary restraint to inferior translation in adduction (arm by the side) and a contributor to anterior stability; part of the rotator interval with the coracohumeral ligament.
- Middle glenohumeral ligament (MGHL): main restraint to anterior translation in the mid range (around 45 degrees of abduction) with external rotation; the most anatomically variable ligament (the Buford complex is a cord-like MGHL with an absent antero-superior labrum - a normal variant not to be repaired).
- Inferior glenohumeral ligament (IGHL): the anterior band is the primary restraint to anterior translation at 90 degrees of abduction and external rotation (ABER) - the position of instability - with a posterior band and the axillary pouch between them forming the hammock.
This positional hierarchy is why a HAGL (failure of the IGHL at its humeral end) presents specifically with ABER apprehension: the end-range anterior check-rein has been lost.
Classification Systems
West Point Classification (Bui-Mansfield)
- Type A: Anterior HAGL (93%) - Avulsion of anterior band from humeral neck.
- Type B: Posterior HAGL (7%) - Avulsion of posterior band (rare).
- Type C: Floating AIGHL (Bipolar - Glenoid and Humeral) - Both ends detached.
- Bony HAGL (BHAGL): Any of the above with a bone fragment from the humerus (20%).
BHAGL is often easier to heal (bone-to-bone) if fixed.
The floating type represents a devastating loss of all inferior restraints.
APEWest Point Classification
Hook:The APE hung from the humerus.
Clinical Presentation
History
- Event: Traumatic dislocation, classically high-energy (contact sport, fall, motor accident). Bokor's series found 94% had a violent first dislocation.
- Demographics: Tends to occur in slightly older patients than isolated Bankart instability, but is also seen in adolescents as an "atypical" lesion.
- Recurrence: Instability or apprehension with overhead/ABER activity.
- Pop: Patient may report a pop or tearing sensation deep in the axilla.
- Failed Surgery: Persistent instability after a "successful" Bankart repair that "never felt tight".
Always question the diagnosis in failed instability repairs and in any traumatic dislocation without a labral tear.
Examination
Physical Exam
- Apprehension: Positive in ABER.
- Relocation: Positive (Pain/Apprehension relief).
- Subscapularis: Check Lift-off / Belly-press (often associated tear).
- Axillary Nerve: ALWAYS verify sensation/deltoid function.
Clinically indistinguishable from Bankart instability without imaging.
The Apprehension test is sensitive but not specific for the type of lesion.
Imaging: MRI
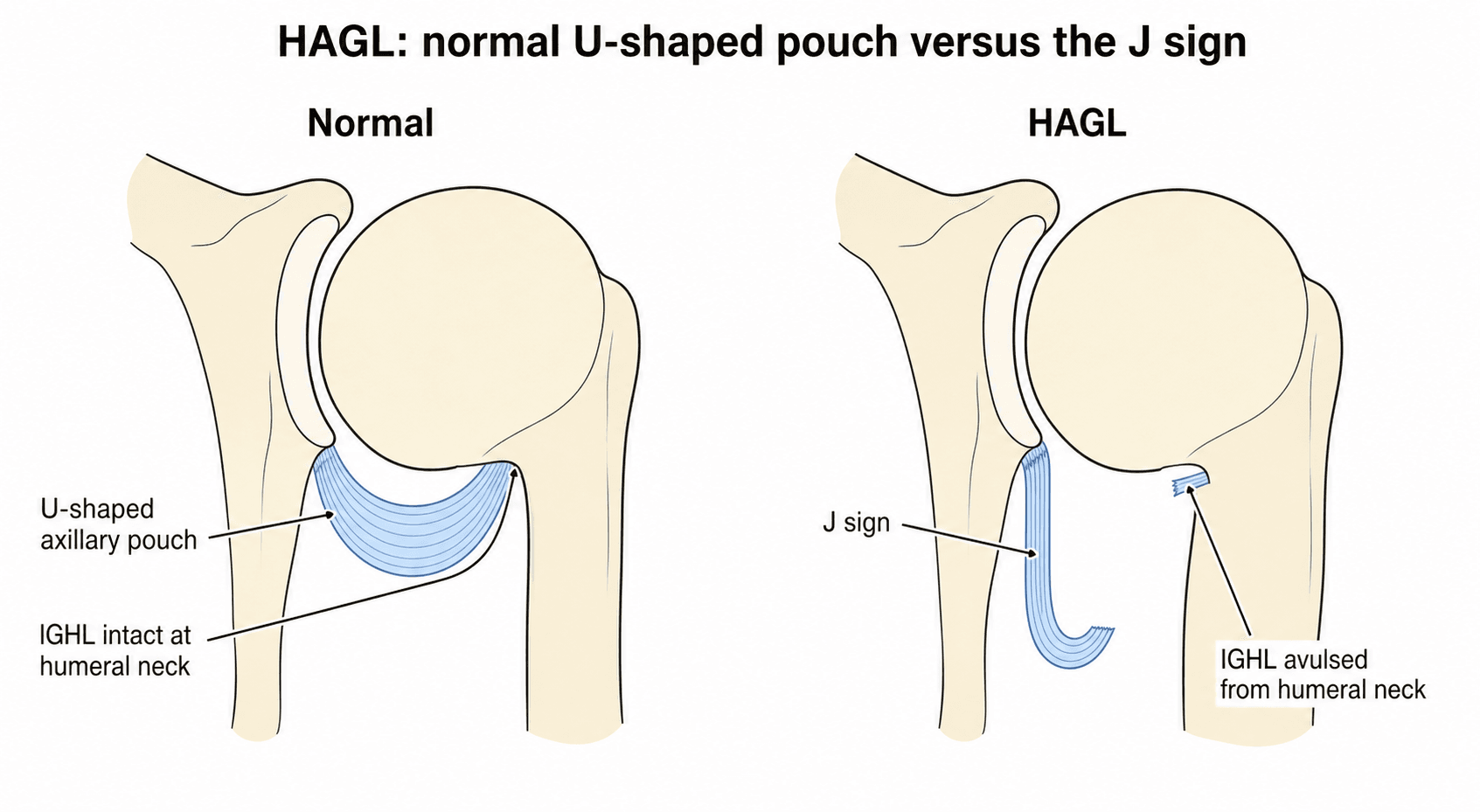
Coronal Oblique T2. Normally, the axillary pouch forms a "U" shape under the humeral head. In a HAGL, the lateral attachment is gone. The IGHL falls inferiorly against the chest wall/glenoid, forming a deep "J" shape.
MRI Signs
- J Sign: The normally U-shaped axillary pouch loses its lateral (humeral) attachment and droops inferiorly, taking on a J configuration on coronal oblique images.
- Double Axillary Pouch: Fluid can collect both within the joint and in the disrupted capsule, creating the appearance of two pouches.
- Extravasation: On MR arthrography, contrast escapes through the humeral-side capsular defect and tracks inferiorly along the humeral neck and shaft (in contrast to the glenoid-side leak typical of a capsular Bankart variant).
- Edema: Bone marrow oedema at the humeral neck in acute lesions.
Always evaluate the integrity of the capsule on the humeral side, not just the labrum.
Differential Diagnosis
The clinical picture of "traumatic anterior instability" is shared by several lesions. The discriminator is almost always imaging and arthroscopy, not the bedside exam. Knowing how each entity differs determines where you place your anchors.
- Site of Failure
- Antero-inferior labrum / glenoid
- Key Discriminator
- Labral detachment with intact periosteum
- Implication
- Standard anterior arthroscopic Bankart repair
- Site of Failure
- Glenoid side, medialised
- Key Discriminator
- Labrum healed medially on the scapular neck
- Implication
- Mobilise and re-tension labrum back to glenoid rim
- Site of Failure
- Glenoid side, non-displaced
- Key Discriminator
- Labrum detached but held by intact periosteum, lies anatomically (often MRI-occult; ABER view helps)
- Implication
- Mobilise the labroperiosteal sleeve and re-fix to the rim
- Site of Failure
- Humeral insertion of IGHL
- Key Discriminator
- J sign on MRI, capsule stripped off humeral neck
- Implication
- Repair to humeral neck (open or 5 o'clock scope)
- Site of Failure
- Antero-inferior glenoid bone
- Key Discriminator
- Glenoid fragment, bone loss on CT
- Implication
- Address bone loss (fragment fixation or Latarjet)
- Site of Failure
- Global capsular redundancy
- Key Discriminator
- Sulcus sign, bilateral, atraumatic, no discrete lesion
- Implication
- Rehabilitation first; capsular plication if it fails
A patient with a genuinely traumatic, unidirectional dislocation but a "normal" MRI labrum is not MDI. Reclassify the imaging as inadequate and look specifically at the humeral capsular insertion for a HAGL before labelling the shoulder "functional".
Management Strategy
Decision Making
- Non-Operative: Reserved for low-demand or elderly patients. Bracing has little role because the avulsed capsule retracts and the synovial environment limits spontaneous healing.
- Operative: Young patients, athletes, and recurrent instability.
- Choice of Approach:
- Open: Gold Standard. Associated Subscap tear. Easier to find and fix.
- Arthroscopic: Technically difficult. Needs 70-degree scope and accessory portals (5 o'clock).
The choice depends largely on surgeon experience and presence of subscapularis pathology.
The 5 O'Clock Portal For arthroscopic repair, a standard anterior portal is too high. Establish a low anterior portal (5 o'clock) to access the inferior pouch. Use localized cutaneous nerve protection.
Surgical Considerations
Open Repair (L-shaped Incision)
- Approach: Deltopectoral.
- Subscapularis: L-shaped tenotomy or Takedown (lower half) to access the deep capsule.
- Identification: Humerus is externally rotated to reveal the avulsed ligament.
- Fixation: Suture anchors (double loaded) placed in the humeral neck.
- Closure: Repair Subscapularis robustly.
- Pros: Visualization, protect Axillary nerve.
- Cons: Subscapularis morbidity.
The L-shaped tenotomy provides excellent exposure of the inferior pouch.
The Axillary Nerve During both open and arthroscopic repair, the axillary nerve is at risk. It runs approx 1-2cm inferior to the glenoid at the 6 o'clock position. In open surgery, bluntly dissect and visualize it if unsure. In scopy, keep portals high (above equator) or use safe zones (5 o'clock needs care).
Complications
Intraoperative Complications
- Axillary Nerve Injury: The most feared complication. The nerve runs approximately 1-2 cm inferior to the capsule at the surgical neck. Both open and arthroscopic approaches place it at risk.
- Subscapularis Damage: During open approach, aggressive retraction or inadequate repair can lead to subscapularis insufficiency.
- Anchor Malposition: Anchors placed too high (cartilage) or too low (shaft) fail to restore anatomy.
- Inadequate Mobilization: Failure to release scarred tissue in chronic cases leads to insufficient repair.
Early Postoperative Complications
- Recurrent Instability: If repair fails or associated Bankart/bone loss missed.
- Stiffness: Specifically loss of External Rotation (capsular tightening).
- Infection: Standard surgical risk.
- Hematoma: Risk increased with subscapularis dissection.
Late Complications
- Chronic Instability: Often due to missed pathology or inadequate repair.
- Subscapularis Failure: Weakness in internal rotation and lift-off tests.
- Glenohumeral Arthritis: Long-term sequela of recurrent instability.
- Anchor Migration: Bioabsorbable anchor osteolysis or metal anchor loosening.
Axillary Nerve Protection:
- In open surgery, identify and protect the nerve before capsular repair.
- In arthroscopy, keep instruments above the equator when possible.
- The 5 o'clock portal should be established with care using blunt trocar.
- Never pass needles blindly in the inferior pouch.
Rehabilitation
-
Phase 1 (0-6 weeks):
- Sling immobilization.
- Limit External Rotation (to protect Subscap and HAGL repair) - usually less than 30 degrees.
- Pendulums.
-
Phase 2 (6-12 weeks):
- Active Range of Motion.
- Progress ER.
-
Phase 3 (3-6 months):
- Strengthening.
- Return to sport at 6 months.
Note: Rehabilitation is often slower than Bankart due to Subscapularis precautions (if open).
Prognosis
Outcomes by Repair Type
- Open Repair Success Rate: Greater than 90% stability restoration.
- Arthroscopic Repair: Variable (75-90%), highly surgeon and case dependent.
- BHAGL Repair: Excellent outcomes due to bone-to-bone healing.
- Floating IGHL Repair: Most challenging; may require combined open approach.
Functional Outcomes
- Return to Sport: 85-95% return to pre-injury level activity.
- Time to Return: Typically 6-9 months (longer than isolated Bankart).
- Range of Motion: External rotation may be slightly reduced (5-10 degrees).
- Strength: Full recovery expected if subscapularis healed properly.
Prognostic Factors
- Positive
- Acute (less than 3 weeks)
- Negative
- Chronic (greater than 6 months)
- Positive
- BHAGL
- Negative
- Floating IGHL
- Positive
- Isolated
- Negative
- Combined Bankart/Bone loss
- Positive
- Younger patient
- Negative
- Older with tissue degeneration
Long-Term Considerations
- Missed HAGL: 100% failure rate of Bankart repair when HAGL is present.
- Arthritis Risk: Ongoing instability leads to accelerated osteoarthritis.
- Re-dislocation: Low (less than 5%) if properly repaired and rehabilitated.
Guidelines, Registries & Global Practice
Global Epidemiology
- HAGL accounts for roughly 2-9% of operatively treated anterior instability depending on the population studied (≈2.3% in the multicentre MOON cohort, ≈9% in early arthroscopic series).
- In the selected subgroup of a violent first dislocation without a Bankart lesion and no multidirectional laxity, incidence rises to ~39% (Bokor series).
- Predominantly affects young to middle-aged males injured in high-energy contact sport (rugby codes, football, wrestling) or trauma; also described as an "atypical" lesion in adolescents.
Society Guidance (side by side)
There is no dedicated international guideline for HAGL specifically; recommendations are extrapolated from anterior instability guidance and expert consensus.
- Relevant Position
- Anterior instability guidance emphasises identifying all capsulolabral pathology and bone loss before stabilisation; no HAGL-specific recommendation
- Relevant Position
- Shoulder instability pathways stress thorough MRI/MRA assessment and surgeon experience for non-Bankart lesions
- Relevant Position
- Recognise HAGL as a distinct cause of failure; recommend dedicated imaging review and repair to the humeral footprint
- Relevant Position
- Highlights axillary nerve protection during anterior-inferior capsular surgery
Registry Notes
- Joint registries (NJR, AJRR, AOANJRR, Swedish, Norwegian) capture arthroplasty, not soft-tissue instability repair, so there is no large-scale registry survivorship data for HAGL repair. Evidence remains limited to case series and multicentre cohorts such as MOON.
High- vs Limited-Resource Practice Variation
- Well-resourced centres: ready access to MR arthrography, ABER-positioned MRI, 70-degree arthroscopes and accessory portals enables attempted arthroscopic repair.
- Limited-resource settings: reliance on plain radiographs and standard MRI increases the miss rate; open deltopectoral repair is often the pragmatic, reliable default and addresses any associated subscapularis tear in the same exposure.
Controversies and Areas of Uncertainty
The evidence base for HAGL is built almost entirely on small case series, cadaveric work, and a handful of multicentre cohorts. There is no randomised trial, so several questions remain genuinely open.
- Open vs arthroscopic repair: There is no high-level comparative trial. Open deltopectoral repair remains the historical reference standard and is favoured when a subscapularis tear coexists or when the lesion is chronic and retracted. Arthroscopic repair is increasingly reported with good results in expert hands but is technically demanding. The MOON cohort showed HAGL is strongly associated with open surgery in current practice.
- Anchor position: Cadaveric data support placing anchors in the humeral neck rather than juxtachondrally to restore the anterior restraint, but the clinical magnitude of this difference is small and unproven in vivo.
- True incidence: Reported figures range from ~2% (MOON multicentre) to ~9% (early arthroscopic series) and up to 39% in the highly selected subgroup of violent first dislocation without a Bankart. The denominator drives the number; quote the population, not a single figure.
- MRI vs MR arthrography: HAGL is missed on roughly one-third of preoperative MRIs even in specialist centres. Whether routine MR arthrography or ABER positioning meaningfully closes that gap is not settled.
- Posterior (reverse) HAGL: A rare entity, usually linked to posterior instability, but recent data show it can accompany recurrent anterior dislocation and respond to arthroscopic repair. Its optimal management is still being defined.
- Role of non-operative treatment: Because the avulsed capsule retracts and the synovial environment limits healing, conservative management is generally reserved for low-demand patients, but the threshold is opinion-based rather than evidence-based.
MCQ Practice Points
Q: The 'J Sign' on coronal oblique MRI indicates: A: HAGL Lesion (Humeral Avulsion of Glenohumeral Ligament).
Q: What percentage of anterior instability cases involve a HAGL lesion? A: Approximately 9%.
Q: Which tendon tear is most commonly associated with an anterior HAGL? A: Subscapularis.
Q: A floating glenohumeral ligament (bipolar avulsion) corresponds to which West Point type? A: Type C.
Q: What is the most likely cause of a failed Bankart repair in a patient with persistent instability and no evidence of bone loss? A: Missed HAGL lesion - performing a glenoid-side repair when the lesion is on the humeral side leads to 100% failure.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old rugby player returns 1 year after 'successful' Bankart repair with recurrent instability. He says it never felt tight. What are your thoughts?”
“A 30-year-old male dislocates his shoulder. Reduced in ED. Post-reduction X-ray shows a small fleck of bone lateral to the humeral head. What is this?”
“You perform an open Latarjet. During exposure, you notice the subscapularis tendon is partially torn inferiorly. What should you look for?”
Diagnosis
- History: Traumatic Dislocation
- Sign: Apprehension Positive
- MRI: J Sign (Inferior droop)
- MRI: Double Axillary Pouch
- X-ray: BHAGL Fleck
Classification (West Point)
- Type A: Anterior (93%)
- Type B: Posterior (7%)
- Type C: Floating (Bipolar)
- BHAGL: Bony Avulsion
Management
- Non-op: Elderly/Low demand
- Open: Gold Standard (Subscap approach)
- Scope: Technically demanding (5 o'clock portal)
- Rehab: Protect ER for 6 weeks
Evidence Base
The Original HAGL Description
- Prospective arthroscopic evaluation of 64 shoulders with anterior instability
- 6 shoulders (9.3%) had a HAGL lesion; 73.5% had a Bankart lesion
- Coined the term HAGL and described its pathological anatomy
- In instability without a primary Bankart lesion, HAGL must be ruled out
West Point Nomenclature
- Systematic review combining 6 institutional cases with a MEDLINE search
- Developed the West Point nomenclature for HAGL variants and associated injuries
- Standardised terminology because different variants require different surgical approaches
Imaging Features of HAGL
- Retrospective review of 6 HAGL lesions with radiographic and MR correlation
- Only 50% were detected on imaging (radiograph or MRI) prior to arthroscopy
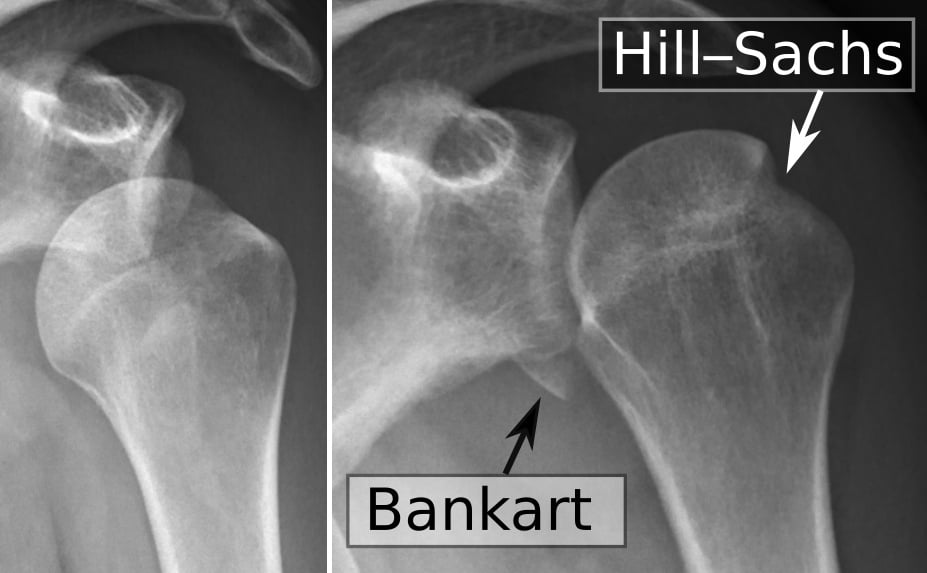
- 68% had associated injuries (rotator cuff, Bankart, Hill-Sachs, osteochondral)
- Cited incidence of 7.5-9.4% across two large series