First MTP Joint Arthritis | Carp Classification | Grading-Based Treatment Algorithm
Carp Classification (Most Common)
Critical Must-Knows
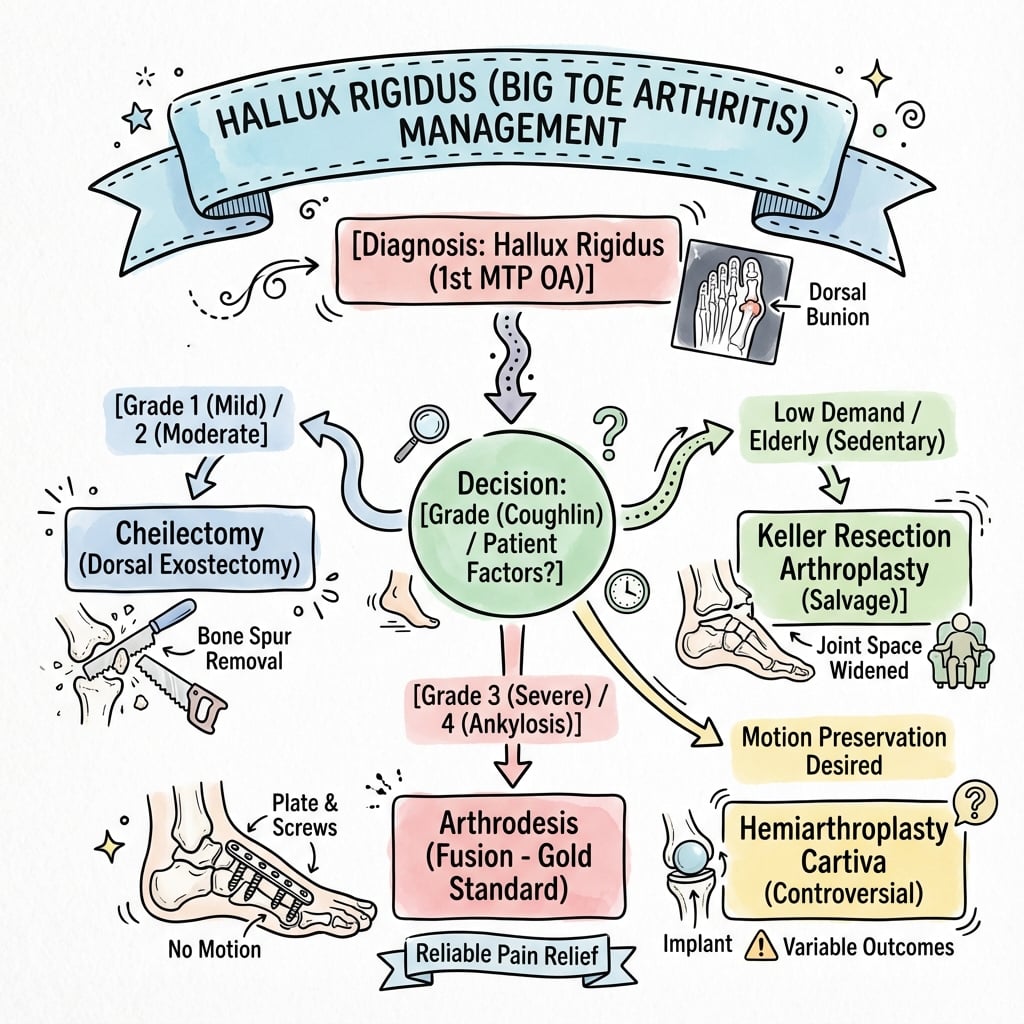
- Grading (Carp) determines treatment: Grade 1-2 = cheilectomy, Grade 3-4 = arthrodesis
- Cheilectomy requires at least 30 degrees dorsiflexion to be effective
- Arthrodesis fusion position: 10-15 degrees valgus, 15-20 degrees dorsiflexion, neutral rotation
- Cheilectomy contraindicated if cartilage loss extends beyond dorsal third of joint
- First MTP arthrodesis has 90-95% fusion rate with high satisfaction
Clinical Pearls
- "Distinguish from hallux valgus (lateral deviation vs stiffness/pain on dorsiflexion)
- "Grind test (compression + rotation) reproduces pain from joint arthritis
- "Dorsal osteophyte causes impingement in toe-off phase of gait
- "Failed cheilectomy can proceed to arthrodesis without major compromise
Clinical Imaging
Imaging Gallery



Critical Hallux Rigidus Exam Points
Key Pathophysiology
Degenerative arthritis of first MTP joint. Primary (70%) or secondary to trauma, gout, inflammatory arthropathy. Dorsal osteophyte blocks dorsiflexion needed for toe-off.
Classification Drives Treatment
Carp grading (0-4) based on radiographic changes and ROM. Grade 1-2 = cheilectomy, Grade 3-4 = arthrodesis. Hattrup-Johnson simpler (3 grades) but less granular.
Treatment Algorithm
Conservative first for all grades. Surgical: cheilectomy if dorsal disease only, arthrodesis for advanced disease, arthroplasty controversial due to high failure.
Critical Surgical Decision
Cheilectomy requires adequate cartilage on plantar surface. If cartilage loss extends beyond dorsal third, proceed directly to arthrodesis. Check intraoperatively.
Quick Decision Guide
| Patient Scenario | Carp Grade | First-Line Surgical | Key Pearl |
|---|---|---|---|
| Early, active patient, minimal symptoms | Grade 0-1: Dorsal spurring, mild JSN | Cheilectomy (30% dorsal head + osteophyte) | 80-90% good results, preserves joint |
| Moderate disease, preserved plantar cartilage | Grade 2: 50-75% JSN, moderate ROM loss | Cheilectomy vs Interposition arthroplasty | Intraop assessment crucial - check cartilage |
| Advanced arthritis, circumferential cartilage loss | Grade 3: Over 75% JSN, severe stiffness | First MTP arthrodesis (gold standard) | 90-95% fusion, 85-90% satisfaction |
| Grade 3 plus hallux valgus or varus deformity | Grade 4: Advanced disease plus deformity | First MTP arthrodesis | Correct alignment: 10-15° valgus, 15-20° dorsiflexion |
CARPHallux Rigidus Classification Systems
| C | Carp grading Grades 0-4, most commonly used, based on JSN and ROM |
| A | Assessment radiographic Dorsal osteophyte, joint space narrowing, subchondral sclerosis |
| R | ROM measurement Normal 65-75° dorsiflexion, hallux rigidus typically under 30° |
| P | Pain on grind test Compression plus rotation reproduces arthritic pain |
| C | Carp grading Grades 0-4, most commonly used, based on JSN and ROM | R | ROM measurement Normal 65-75° dorsiflexion, hallux rigidus typically under 30° |
| A | Assessment radiographic Dorsal osteophyte, joint space narrowing, subchondral sclerosis | P | Pain on grind test Compression plus rotation reproduces arthritic pain |
Hook:CARP - like a fish mouth that can't open (rigid joint)!
DORSALCheilectomy Indications
| D | Dorsal disease only Cartilage loss limited to dorsal third of joint |
| O | Osteophyte prominent Dorsal spurring causing impingement |
| R | ROM at least 30 degrees Minimum dorsiflexion needed for success |
| S | Stage 1-2 Carp Early to moderate disease |
| A | Active patient desires Wants to preserve joint motion |
| L | Limited plantar involvement Plantar cartilage must be preserved |
| D | Dorsal disease only Cartilage loss limited to dorsal third of joint | R | ROM at least 30 degrees Minimum dorsiflexion needed for success | A | Active patient desires Wants to preserve joint motion |
| O | Osteophyte prominent Dorsal spurring causing impingement | S | Stage 1-2 Carp Early to moderate disease | L | Limited plantar involvement Plantar cartilage must be preserved |
Hook:DORSAL disease = cheilectomy removes the DORSAL bump!
VDNFirst MTP Arthrodesis Fusion Position
| V | Valgus 10-15 degrees Relative to first metatarsal axis |
| D | Dorsiflexion 15-20 degrees Relative to ground with foot plantigrade |
| N | Neutral rotation Avoid internal or external rotation |
| V | Valgus 10-15 degrees Relative to first metatarsal axis |
| D | Dorsiflexion 15-20 degrees Relative to ground with foot plantigrade |
| N | Neutral rotation Avoid internal or external rotation |
Hook:VDN - Very Deliberate Numbers for fusion position!
Overview and Epidemiology
Why Hallux Rigidus Matters
Hallux rigidus is the most common arthritic condition of the foot, second only to hallux valgus as a disorder of the first MTP joint. Unlike hallux valgus (deformity-driven), hallux rigidus is pain and stiffness-driven, significantly affecting gait and quality of life. Treatment is grading-based with predictable outcomes.
Demographics
- Age: Bimodal - adolescent (osteochondritis) and 40-60 years (degenerative)
- Gender: Males twice as common as females
- Bilateral: 50-80% of cases
- Occupation: Higher in athletes, dancers, manual laborers
Etiology and Impact
- Primary (70%): Idiopathic, likely multifactorial (genetics, mechanics, anatomy)
- Secondary (30%): Trauma, inflammatory arthritis (gout, RA), osteochondritis dissecans
- Gait impact: Painful toe-off, compensatory external foot progression angle
- Function loss: Unable to squat, difficulty with stairs, impaired running
Pathophysiology and Mechanisms
First MTP Joint Biomechanics
The first MTP joint undergoes 2-3 times body weight during normal gait, increasing to 8 times body weight with running. Normal dorsiflexion of 65-75 degrees is required for toe-off. Hallux rigidus reduces this to typically under 30 degrees, forcing compensatory mechanisms that alter gait mechanics.
| Structure | Normal Anatomy | Hallux Rigidus Changes | Clinical Significance |
|---|---|---|---|
| Articular cartilage | Smooth, covers entire joint surface | Erosion starts dorsal, progresses plantar | Dorsal-only disease amenable to cheilectomy |
| Dorsal capsule | Allows 65-75° dorsiflexion | Contracted, fibrotic, thickened | Capsular release improves ROM post-cheilectomy |
| Sesamoid complex | Glides smoothly under metatarsal head | Arthritic changes in advanced disease | Consider sesamoid debridement if involved |
| Dorsal osteophyte | Absent | Progressive spurring blocking extension | Primary cause of impingement pain |
Normal Gait Mechanics
- Heel strike: Foot plantigrade
- Mid-stance: First MTP joint neutral
- Toe-off: Requires 65-75° dorsiflexion
- Push-off: 60% body weight through hallux
Hallux Rigidus Compensation
- Toe-off altered: Cannot achieve normal dorsiflexion
- External rotation: Foot turns out to avoid MTP dorsiflexion
- Lateral weight shift: Loads lesser toes abnormally
- Pain cycle: Dorsal impingement reinforces stiffness
Classification Systems
Carp Classification (Most Commonly Used)
| Grade | Radiographic Findings | Clinical ROM | Treatment |
|---|---|---|---|
| 0 | Dorsal osteophyte, no JSN | 10-20% loss, over 60° dorsiflexion | Conservative, consider cheilectomy if symptomatic |
| 1 | Mild spurring, 20-50% JSN, minimal sclerosis | 20-50% loss, 40-60° dorsiflexion | Cheilectomy first-line, excellent results |
| 2 | Moderate spurring, 50-75% JSN, subchondral sclerosis | 50-75% loss, 20-40° dorsiflexion | Cheilectomy if plantar cartilage OK, or interposition |
| 3 | Severe spurring, over 75% JSN, cysts, loose bodies | Over 75% loss, under 20° dorsiflexion | Arthrodesis gold standard |
| 4 | Grade 3 changes plus hallux valgus or varus | Severe stiffness plus deformity | Arthrodesis with deformity correction |
Carp Grading Key Distinction
The critical decision point is Grade 2: if intraoperative assessment shows cartilage preservation on the plantar surface, cheilectomy can succeed. If cartilage loss is circumferential, proceed directly to arthrodesis. Do not compromise with inadequate debridement.
This classification system correlates well with treatment outcomes and provides clear decision-making framework.
Clinical Assessment
History
- Pain: Dorsal MTP, worse with toe-off, stairs, squatting
- Stiffness: Progressive loss of dorsiflexion
- Gait: External foot progression angle to avoid dorsiflexion
- Footwear: Difficulty with heels, dress shoes, athletic shoes
- Activities: Reduced running, dancing, sports participation
- Previous treatments: Orthotics, injections, activity modification
Examination
- Look: Dorsal prominence, skin irritation over osteophyte
- Feel: Tenderness over dorsal MTP, osteophyte palpable
- Move: Measure dorsiflexion (normal 65-75°), grind test positive
- Deformity: Assess for hallux valgus/varus component (Carp Grade 4)
- Gait: Observe toe-off phase, external rotation compensation
- Neurovascular: Ensure intact (dorsalis pedis, sensation)
Grind Test - Key Diagnostic Maneuver
Compress the first MTP joint while rotating the hallux. Pain reproduction indicates intra-articular pathology (arthritis). Compare with dorsal impingement pain (pain only at end-range dorsiflexion). Grind test specificity distinguishes arthritis from isolated dorsal impingement.
| Finding | Hallux Rigidus | Hallux Valgus | Turf Toe |
|---|---|---|---|
| Primary complaint | Pain and stiffness | Deformity and bunion pain | Acute traumatic pain |
| Deformity | Dorsal osteophyte, usually straight alignment | Lateral deviation, medial eminence | Swelling, ecchymosis |
| ROM | Restricted dorsiflexion, painful | Variable, often normal early | All motion painful acutely |
| Radiographs | Dorsal osteophyte, JSN, sclerosis | Hallux valgus angle, 1-2 IM angle | Often normal, may show avulsion |
Investigations
Imaging Protocol
Essential views for grading and planning. AP shows joint space narrowing, medial/lateral osteophytes. Lateral shows dorsal osteophyte (key for cheilectomy planning), assess dorsal 30% of metatarsal head.
Sesamoid assessment. Evaluates sesamoid arthritis which may require debridement at surgery. More sensitive than AP for lateral osteophytes.
CT: Preoperative planning for complex deformity or failed surgery. MRI: If concern for osteochondritis dissecans (young patient) or to assess cartilage (not routine).
Radiographic Features (Progressive)
- Early (Grade 1): Dorsal osteophyte, maintained joint space
- Moderate (Grade 2): Flattening of metatarsal head, 50% JSN
- Advanced (Grade 3): Severe JSN, subchondral sclerosis, cysts
- Late (Grade 4): Near ankylosis, loose bodies, deformity
Pre-Operative Planning
- Measure dorsal osteophyte: Extent of resection for cheilectomy
- Assess joint space: Plantar cartilage preservation?
- Check sesamoids: Arthritic changes requiring debridement?
- Measure alignment: Hallux valgus/varus for fusion correction

Non-Operative Management
Conservative Management Role
All patients should trial non-operative management before surgery, unless severe pain or functional limitation. Success rates vary: 20-30% achieve satisfactory symptom control with conservative measures. Duration of trial: 3-6 months.
Conservative Treatment Algorithm
Wide toe box, stiff sole. Rigid sole reduces MTP dorsiflexion demand. Rocker-bottom sole shifts toe-off proximal. Avoid high heels (increase dorsiflexion demand).
Morton's extension orthotic (carbon fiber plate extending to hallux tip) prevents MTP dorsiflexion. Turf toe plate similar effect. Padding over dorsal osteophyte for shoe pressure.
Avoid high-impact activities, running, jumping. Low-impact alternatives: cycling, swimming. Occupational modifications for prolonged standing/walking.
NSAIDs for pain and inflammation. Oral or topical. Caution in elderly, renal disease. Not disease-modifying, symptom control only.
Corticosteroid (+ local anesthetic). Diagnostic: confirms intra-articular source. Therapeutic: 3-6 months relief common. Maximum 2-3 injections. Consider hyaluronic acid (less evidence).
When to Abandon Conservative Management
Indications for surgical referral: Failure of 3-6 months conservative treatment, severe pain limiting daily activities, progressive deformity (Grade 4), significant gait disturbance affecting work/recreation. Emphasize to patients that surgery is elective but highly effective.
Management Algorithm
Cheilectomy - Joint-Preserving Procedure
Indications:
- Carp Grade 1-2 (mild to moderate arthritis)
- Dorsal osteophyte causing impingement
- Preserved plantar cartilage (critical!)
- At least 30 degrees dorsiflexion remaining
- Failed conservative management
Contraindications:
- Circumferential cartilage loss (intraop finding)
- Severe stiffness (under 20 degrees dorsiflexion)
- Grade 3-4 disease
- Sesamoid arthritis
Cheilectomy Technique
Dorsal longitudinal incision over first MTP joint, 3-4 cm. Protect dorsal sensory nerves (medial and lateral cutaneous branches). Incise capsule longitudinally, preserve for repair.
Intraoperative cartilage evaluation. Plantarflex hallux to expose dorsal metatarsal head. Assess cartilage: if intact on plantar two-thirds, proceed with cheilectomy. If circumferential loss, convert to arthrodesis.
Remove dorsal 25-30% of metatarsal head. Use oscillating saw or osteotome. Resect from medial to lateral, ensuring complete removal of dorsal ridge. Smooth with rongeur. Remove phalangeal osteophytes.
Release dorsal capsular adhesions to improve dorsiflexion. Gentle manipulation to achieve at least 60-70 degrees dorsiflexion. Avoid forced manipulation (fracture risk).
Repair capsule loosely (over-tightening limits dorsiflexion). Subcuticular skin closure. Soft dressing, wooden shoe or post-op shoe for 2 weeks.
Pearls
- 30% rule: Remove dorsal 30% to decompress joint
- Check motion: Aim for 60-70° intraoperative dorsiflexion
- Preserve plantar cortex: Critical for stability
- Early mobilization: Start ROM at 2 weeks
Pitfalls
- Under-resection: Inadequate decompression, recurrent impingement
- Over-resection: Metatarsal fracture, instability, transfer metatarsalgia
- Missed plantar disease: Poor outcome, consider conversion
- Forced manipulation: Fracture, damage plantar cartilage
Cheilectomy Outcomes
Grade 1-2 disease: 80-90% good-excellent results at 5 years. Pain relief predictable, ROM improvement variable (average 20-30 degree gain). Satisfaction high. Durability: 70-80% avoid further surgery at 10 years. Failed cheilectomy can proceed to arthrodesis without compromise.
These outcomes make cheilectomy an excellent first-line option for appropriate candidates.


Surgical Technique
Patient Positioning
Setup Checklist
Supine on standard operating table. Ankle bump to internally rotate leg, expose medial aspect of first MTP joint. Contralateral limb: flat on table or frog-leg position.
Thigh or ankle tourniquet. Ankle preferred for better access. Exsanguinate with Esmarch or elevation. Inflate to 250-300 mmHg (ankle) or 100 mmHg above systolic (thigh).
Foot and ankle free-draped. Expose from toes to mid-calf. Ensure C-arm access for lateral and AP views of first MTP joint.
Standard positioning allows both cheilectomy and arthrodesis through same approach.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Recurrent stiffness/pain post-cheilectomy | 15-20% at 5-10 years | Under-resection, progression of arthritis, Grade 3-4 disease | Revision cheilectomy if residual osteophyte, or convert to arthrodesis |
| Malunion (arthrodesis) | 10-15% (most common complication) | Technical error, inadequate fluoroscopy, poor positioning technique | If symptomatic: revision arthrodesis with osteotomy |
| Nonunion (arthrodesis) | 5-10% | Smoking, diabetes, inadequate fixation, poor bone quality | Revision arthrodesis with bone graft, biologics, rigid fixation |
| Hardware irritation (arthrodesis) | 10-15% | Prominent plate, low-profile skin, patient factors | Hardware removal after union (typically 6-12 months) |
| Transfer metatarsalgia | 5-10% | Over-resection (cheilectomy), malunion (arthrodesis) | Orthotics, metatarsal pads, rarely osteotomy |
| Infection | 1-3% | Diabetes, smoking, immunosuppression | Antibiotics, wound care, rarely debridement or hardware removal |
| Nerve injury (sensory) | 5-10% temporary, 1-2% permanent | Dorsal medial/lateral cutaneous nerves | Usually resolves, neuropathic pain management if persistent |
Preventing Malunion - Most Common Arthrodesis Complication
Malunion is the most common significant complication of first MTP arthrodesis. Prevention requires meticulous intraoperative technique: use sterile block to simulate weight-bearing, check hallux alignment (should point between 2nd-3rd toes), ensure 15-20 degrees dorsiflexion (1-2 cm ground clearance), confirm 10-15 degrees valgus. Fluoroscopy in multiple planes before final fixation. Do not accept suboptimal position - reposition and re-fix if needed.
Postoperative Care and Rehabilitation
Cheilectomy Rehabilitation
Dressing and footwear: Soft dressing, wooden shoe or post-op shoe. Weight-bearing: Immediate weight-bearing as tolerated in protective shoe. Activity: Elevate foot, ice, minimal walking. Pain control: Oral analgesics, NSAIDs after 48 hours.
ROM exercises: Start gentle dorsiflexion exercises at 2 weeks (critical!). Manual stretching, active ROM. Goal: regain 60-70 degrees. Footwear: Transition to stiff-soled athletic shoe. Weight-bearing: Full weight-bearing. Activity: Walking, avoid running/jumping.
Strengthening: Toe curls, marble pick-up, resistance band dorsiflexion. Proprioception: Balance exercises. Activity: Gradual return to sports, impact activities. Footwear: Normal shoes, avoid high heels initially.
Return to sport: Running, jumping, cutting at 3 months if ROM adequate. Long-term: Expect 90% recovery by 6 months. Maintain ROM with daily stretching. Avoid excessive high heels long-term.
Critical Cheilectomy Rehab Point
Early ROM exercises are critical to cheilectomy success. Start at 2 weeks - capsular adhesions form quickly. Goal: 60-70 degrees dorsiflexion. Aggressive physiotherapy improves outcomes. Stiffness post-cheilectomy often reflects inadequate rehabilitation, not surgical failure.
Early mobilization maximizes the motion-preservation benefit of cheilectomy.
Outcomes and Prognosis
| Procedure | Best For | Success Rate | Advantages | Disadvantages |
|---|---|---|---|---|
| Cheilectomy | Grade 1-2, dorsal disease | 80-90% satisfaction at 5 years | Motion preserved, simple procedure, low morbidity | May fail (15-20% at 10 years), arthritis progression |
| Interposition Arthroplasty | Grade 2, young patient | 60-80% satisfaction at 5 years | Motion preserved, no implant | Higher failure than cheilectomy or arthrodesis, limited evidence |
| Arthrodesis | Grade 3-4, failed cheilectomy | 85-90% satisfaction long-term | Predictable pain relief, durable, low revision rate | Loss of motion, malunion risk, longer recovery |
| Arthroplasty | Limited role (elderly, low demand) | 60-80% at 5 years, 60% at 10 years | Motion preserved (theoretically) | High failure, loosening, revision difficult, not recommended |
Predictors of Poor Outcome
Cheilectomy: Grade 3-4 disease (wrong procedure), circumferential cartilage loss, inadequate debridement. Arthrodesis: Malunion (affects function, satisfaction), nonunion (5-10%), smoking. General: Inflammatory arthropathy, worker's compensation, unrealistic patient expectations. Patient selection and meticulous technique are critical to optimal outcomes.
Evidence Base and Key Trials
Coughlin & Shurnas - The Landmark Grading and Long-Term Outcome Study
- Single-surgeon series of 110 patients (114 joints) followed over a 19-year period; mean follow-up 9.6 years (cheilectomy) and 6.7 years (arthrodesis)
- Introduced the now widely used 5-grade (0-4) clinical-radiographic classification combining ROM, pain and radiographic change
- 80 patients (93 feet) had cheilectomy, 30 patients (34 feet) had arthrodesis
- 92% (86/93) of cheilectomies were successful for pain and function; cheilectomy reliable for Grade 1-2 and SELECTED Grade 3
- Grade 4, or Grade 3 with less than 50% of metatarsal head cartilage remaining at surgery, should be treated with arthrodesis
- No association found between hallux rigidus and first-ray hypermobility or metatarsus primus elevatus
Cheilectomy vs Interpositional Arthroplasty - Procedure-Specific Outcomes
- Retrospective comparison: 19 patients (24 feet) Grade 2 disease treated with cheilectomy vs 11 patients (11 feet) Grade 3 disease treated with interpositional arthroplasty
- Cheilectomy satisfaction 87.5% vs interpositional arthroplasty 72.7%; mean AOFAS 77.3 vs 71.6
- Great-toe weakness reported in 72.7% of interposition patients vs only 16.7% of cheilectomy patients
- Pedobarography showed reduced great-toe load and weight transfer to lesser metatarsals in all patients, greatest after interposition
- Authors conclude interposition is a salvage procedure with less reliable results than cheilectomy
Arthrodesis vs Total Joint Replacement - Randomised Controlled Trial
- RCT of 63 patients (77 toes): 38 toes arthrodesis vs 39 toes total replacement arthroplasty, single surgeon, 24-month follow-up
- Pain improved in both groups but significantly more after arthrodesis (p = 0.01)
- All 38 arthrodeses united (mean dorsiflexion 26 degrees) with few complications
- 6 of 39 arthroplasty implants required removal for phalangeal component loosening; remaining implants gained poor motion
- Cost ratio 2:1 in favour of arthrodesis; arthrodesis preferred even when implant failures were excluded
Synthetic Cartilage Implant vs Arthrodesis - Multicentre Non-inferiority RCT
- Prospective randomised (2:1) non-inferiority trial across 12 centres in Canada and the UK; 152 hydrogel synthetic cartilage implants vs 50 arthrodeses, advanced-stage disease
- VAS pain and FAAM sport/ADL scores improved significantly in both groups at 12 and 24 months with statistical equivalence on the composite outcome
- Implant gained 6.2 degrees (27.3%) active dorsiflexion, maintained at 24 months
- Secondary surgery: 11.2% implant vs 12.0% arthrodesis; under 10% of implants required conversion to arthrodesis at 2 years
- No cases of implant fragmentation, wear or bone loss
Crossed Screws vs Plate-and-Screw Fixation - Meta-Analysis
- Systematic review and meta-analysis: 9 comparative studies, 976 patients (1,035 toes)
- NO significant difference in union rates between crossed screws and plate-plus-interfragmentary-screw (OR 0.75, p = 0.29)
- No significant difference in overall complications, revision, hardware removal or malunion
- Plate-and-screw construct gave a significantly shorter time to fusion (mean difference 0.51 weeks, p = 0.02)
- Choice should also weigh indication, bone quality and cost
Interposition Arthroplasty - Contemporary Systematic Review
- Systematic review of 20 studies, 498 patients (539 feet), mean follow-up 4.5 years
- Autogenous first MTP capsular tissue was the commonest interposition material (60% of studies)
- Mean improvements in standardised scores exceeded the minimal clinically important difference in most studies
- Progression to further surgery in only 3.8% of toes
- Transfer metatarsalgia was the commonest complication (up to 57.9% in one series)
- 85% of included studies were Level IV evidence
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classification and Initial Management (2-3 min)
"A 55-year-old male accountant presents with 2 years of progressive pain and stiffness in his right great toe. Pain is worse with walking, particularly when pushing off. He has tried wider shoes and ibuprofen with minimal relief. On examination, there is a dorsal prominence at the first MTP joint, tenderness on palpation, and dorsiflexion limited to 25 degrees (plantarflexion full). Grind test is positive. Weight-bearing radiographs show a dorsal osteophyte, 60% joint space narrowing, and mild subchondral sclerosis. What is your assessment and management?"
Scenario 2: Surgical Technique - Arthrodesis (3-4 min)
"A 62-year-old female with severe hallux rigidus (Carp Grade 3, over 75% joint space loss, dorsiflexion 10 degrees) has failed conservative management and wants definitive treatment. You plan a first MTP arthrodesis. Walk me through your surgical technique, focusing on achieving optimal fusion position."
Scenario 3: Complication Management (2-3 min)
"A 48-year-old male underwent cheilectomy for Grade 2 hallux rigidus 18 months ago. He returns with recurrent pain and stiffness. Dorsiflexion is now only 20 degrees. Radiographs show progression to Grade 3 disease with near-complete joint space loss and a small residual dorsal osteophyte. How do you manage this patient?"
MCQ Practice Points
Anatomy Question
Q: What is the normal dorsiflexion range of the first MTP joint required for normal gait? A: 65-75 degrees. This range is required for toe-off phase of gait. Hallux rigidus typically reduces this to under 30 degrees, causing compensatory gait alterations (external foot progression angle, lateral weight shift).
Classification Question
Q: What are the key features distinguishing Carp Grade 2 from Grade 3 hallux rigidus? A: Grade 2: 50-75% joint space narrowing, moderate dorsal/lateral osteophytes, 20-50% ROM loss. Treatment: cheilectomy if plantar cartilage OK. Grade 3: Over 75% joint space narrowing, severe osteophytes, subchondral cysts, over 75% ROM loss (under 20 degrees dorsiflexion). Treatment: arthrodesis. The distinction guides surgical decision-making.
Treatment Algorithm Question
Q: What is the critical intraoperative decision point during cheilectomy for Grade 2 hallux rigidus? A: Assessment of plantar cartilage status. If cartilage is preserved on the plantar two-thirds of the joint, proceed with cheilectomy (30% dorsal head resection). If cartilage loss is circumferential, convert to arthrodesis. Do not compromise with inadequate debridement - this leads to poor outcomes.
Surgical Technique Question
Q: What is the optimal fusion position for first MTP arthrodesis? A: VDN mnemonic: Valgus 10-15 degrees (relative to first metatarsal axis), Dorsiflexion 15-20 degrees (relative to ground with foot plantigrade), Neutral rotation. Check alignment with foot on sterile block - hallux should clear ground by 1-2 cm and point between 2nd-3rd toes. Malunion is the most common complication and is position-dependent.
Outcomes Question
Q: What are the evidence-based success rates for cheilectomy vs arthrodesis in hallux rigidus? A: Cheilectomy (Grade 1-2): 80-90% satisfaction at 5 years, 70-80% avoid further surgery at 10 years. Arthrodesis: 90-95% fusion rate, 85-90% patient satisfaction long-term. Arthrodesis has slightly higher satisfaction but sacrifices motion. Both are evidence-based, appropriate procedures when used for correct indications.
Complication Question
Q: What is the most common significant complication of first MTP arthrodesis and how is it prevented? A: Malunion (10-15%) is the most common complication. Prevention requires meticulous intraoperative technique: use sterile block to simulate weight-bearing, check hallux alignment (between 2nd-3rd toes), ensure 15-20 degrees dorsiflexion (1-2 cm ground clearance), confirm 10-15 degrees valgus, fluoroscopy in multiple planes before final fixation. Do not accept suboptimal position.
Guidelines, Registries & Global Practice
Global Epidemiology
Hallux rigidus is the most common arthritic condition of the foot and the second most common disorder of the first MTP joint after hallux valgus. Population studies estimate symptomatic disease in roughly 2.5% of adults over 50 years, with bilateral involvement in 50-80%. Peak incidence is in the fifth and sixth decades, with a bimodal pattern (adolescent osteochondral and adult degenerative). These figures are broadly consistent across high-income populations; data from low- and middle-income settings are sparse.
Side-by-Side Guideline and Society Positions
| Source / Region | Stance on Grading | Joint-Preserving Surgery | End-Stage Disease |
|---|---|---|---|
| AOFAS / US foot-ankle literature | Coughlin-Shurnas 5-grade system most widely cited | Cheilectomy for Grade 1-2 and selected Grade 3; synthetic cartilage implant an accepted alternative (FDA-approved) | Arthrodesis is gold standard for advanced disease |
| BOFAS / UK (British Orthopaedic Foot & Ankle Society) | Grading guides management; emphasis on shared decision-making | Cheilectomy first-line for early disease; cautious adoption of synthetic implants pending long-term data | Arthrodesis preferred for end-stage; replacement reserved for selected low-demand patients |
| AO Foundation / technique guidance | Focus on fixation principles rather than grading | Joint preparation to bleeding bone; congruent surfaces | Rigid compression (lag screw plus dorsal plate or crossed screws) targeting 10-15 deg valgus, 10-15 deg dorsiflexion |
| EFORT / European consensus | Supports validated grading and patient-reported outcomes | Motion-sparing options offered to younger, higher-demand patients after counselling | Arthrodesis remains the most durable, cost-effective end-stage option |
Registry & Evidence Notes
- No dedicated joint registry captures first MTP implants the way hip/knee registries do, so durability data rely on RCTs and case series
- Cartiva synthetic implant: equivalent to fusion at 2 years (Baumhauer RCT) but post-market series report higher early revision and subsidence
- Constrained total joint replacements: historically poor (Gibson RCT - loosening), largely abandoned
- Fusion union rates consistently 90-100% across series with rigid compression fixation
High- vs Limited-Resource Practice
- High-resource: ready access to weight-bearing radiographs, locking plates, synthetic implants, formal physiotherapy and rocker-sole footwear
- Limited-resource: greater reliance on conservative care (stiff-soled footwear, activity modification); fusion favoured over implants given cost and lack of revision infrastructure
- Universal principles: grade-directed treatment, conservative trial first, fusion as the reliable end-stage solution regardless of setting
- Implant selection should reflect availability of revision capability, not novelty
Documentation and Consent (Globally Applicable)
Key documentation requirements:
- Conservative management trial documented (footwear, orthotics, injections, duration)
- Informed consent: procedure options (cheilectomy vs arthrodesis vs motion-sparing implant), fusion position (permanent loss of motion), outcomes (satisfaction and revision rates), complications (malunion, nonunion, infection, nerve injury)
- Realistic expectations: cheilectomy may fail (15-20% at 10 years); arthrodesis sacrifices motion but gives reliable pain relief
- Intra-operative decision-making: if converting from cheilectomy to arthrodesis based on cartilage status, document the finding and rationale
- Malunion prevention: document intra-operative checks (sterile block, fluoroscopy, alignment confirmation)
Common litigation themes: malunion (position not verified intra-operatively), deep infection, sensory nerve injury (medial dorsal cutaneous nerve), and unrealistic expectations of retained motion after arthrodesis.
Controversies and Areas of Uncertainty
Motion-Sparing vs Fusion in Younger Patients
The central debate is whether synthetic cartilage implants or interposition arthroplasty justify their higher revision risk to preserve motion in active patients. RCT data (Baumhauer) show 2-year non-inferiority for the hydrogel implant, but durability beyond 5 years and real-world revision rates remain contested. Fusion remains the most predictable, lowest-cost option.
Cheilectomy in Grade 3 Disease
Coughlin-Shurnas showed cheilectomy can succeed in SELECTED Grade 3 joints with greater than 50% cartilage remaining, blurring the simple "Grade 3 equals fusion" rule. The decision is ultimately intra-operative, based on cartilage assessment, not radiographs alone.
Fixation Construct for Arthrodesis
Earlier teaching favoured dorsal plate-plus-lag-screw over crossed screws, but the 2025 meta-analysis (Lim) found no difference in union or complications, only marginally faster fusion with plating. Construct choice is now driven by bone quality, cost and surgeon preference.
Optimal Fusion Dorsiflexion Angle
Texts quote 15-20 degrees of dorsiflexion relative to the ground, but AO and several series favour 10-15 degrees; excessive dorsiflexion causes interphalangeal joint overload and shoe-wear difficulty, while insufficient dorsiflexion causes pulp pressure. The functional reference (foot plantigrade on a block) matters more than an absolute number.
Role of the Moberg Osteotomy
A dorsal closing-wedge phalangeal (Moberg) osteotomy is increasingly added to cheilectomy to augment effective dorsiflexion, but its independent contribution to outcome versus cheilectomy alone is not firmly established.
Imaging and Cartilage Assessment
Radiographic grade correlates poorly with symptoms and with intra-operative cartilage status (Coughlin-Shurnas). Whether advanced imaging (MRI/CT cartilage mapping) should refine pre-operative decision-making, rather than intra-operative inspection, remains unresolved.
HALLUX RIGIDUS
Clinical summary
Key Anatomy
- •First MTP joint: 2-3x body weight in gait, 8x with running
- •Normal dorsiflexion: 65-75 degrees (required for toe-off)
- •Hallux rigidus: Typically under 30 degrees dorsiflexion
- •Dorsal osteophyte: Blocks dorsiflexion, causes impingement pain
Carp Classification
- •Grade 0: Dorsal osteophyte, no JSN = Conservative
- •Grade 1: 20-50% JSN, mild spurring = Cheilectomy
- •Grade 2: 50-75% JSN, moderate spurring = Cheilectomy or Interposition
- •Grade 3: Over 75% JSN, severe changes = Arthrodesis
- •Grade 4: Grade 3 plus hallux valgus/varus = Arthrodesis
Treatment Algorithm
- •Conservative first (all grades): Stiff shoes, orthotics, NSAIDs, injections
- •Cheilectomy: Grade 1-2, plantar cartilage preserved, 80-90% satisfaction
- •Arthrodesis: Grade 3-4, failed cheilectomy, 90-95% fusion rate
- •Arthroplasty: Limited role, high failure rates (20-40% at 10 years)
Surgical Pearls
- •Cheilectomy: Remove dorsal 30% metatarsal head, achieve 60-70° intraop dorsiflexion
- •Arthrodesis position (VDN): 10-15° Valgus, 15-20° Dorsiflexion, Neutral rotation
- •Use sterile block to simulate weight-bearing when checking fusion position
- •Plate fixation: 95% union vs screws 88% (meta-analysis)
- •Intraop cartilage assessment determines cheilectomy vs arthrodesis
Complications
- •Malunion (arthrodesis): 10-15%, most common, position-dependent
- •Nonunion (arthrodesis): 5-10%, smoking major risk factor
- •Recurrent pain (cheilectomy): 15-20% at 10 years, disease progression
- •Hardware irritation: 10-15%, may require removal after union
- •Transfer metatarsalgia: Over-resection or malunion