Find the structure, level and urgency
- A hand examination is a localisation exercise, not a list of tests.
- Compare active and passive motion before diagnosing tendon rupture.
- Test median, ulnar and radial motor function with one reliable muscle each, then add sensory testing.
- FDP, FDS, EPL, central slip and terminal extensor must be tested separately because combined finger motion can hide a rupture.
- Document preoperative sensation and motor function before any hand trauma procedure.
- “If active motion is absent but passive motion is full, think tendon rupture, nerve palsy or pain inhibition.
- “If passive motion is restricted, the problem is at least partly joint, capsule, skin, tendon adhesions or swelling.
- “AIN palsy has motor findings without sensory loss.
- “A high ulnar nerve lesion can have less obvious clawing than a low ulnar lesion because FDP to ring and little may also be weak.
Hand Examination and Clinical Localisation
Pain, swelling, tendon rupture, joint dislocation, compartment syndrome, infection and poor cooperation can all look like weakness. Localisation requires pattern recognition plus active-passive comparison.
Overview/Epidemiology
Hand examination is common in trauma clinics, emergency departments, fracture clinics, rheumatology, nerve clinics and elective hand practice. It is high-value because a careful clinical examination often identifies the injured structure before imaging or electrodiagnostic testing.
The common settings are:
- laceration with possible tendon, nerve or vessel injury
- finger deformity after trauma
- post-fracture stiffness or tendon rupture
- carpal tunnel, cubital tunnel or peripheral nerve compression
- ulnar or radial nerve palsy
- rheumatoid or inflammatory hand deformity
- Dupuytren disease, trigger finger and tendon imbalance
- infection, compartment syndrome or complex regional pain
The hand has many structures in a small space. A vague statement such as "weak grip" is not enough. The aim is to localise the weakness to a tendon, muscle, nerve level, joint, pain generator or vascular problem.
Anatomy/Biomechanics
Hand movement comes from three linked systems:
- Extrinsic tendons: flexors and extensors cross the wrist and fingers from the forearm.
- Intrinsic muscles: thenar, hypothenar, lumbricals and interossei control pinch, MCP flexion, IP extension and fine balance.
- Nerves: median, ulnar and radial nerve branches provide motor control and sensory feedback.
The same visible problem can arise from different levels. Thumb weakness can be APB weakness from median nerve compression, FPL weakness from AIN palsy, EPL rupture after distal radius fracture, pain inhibition from CMC arthritis or stiffness after immobilisation.
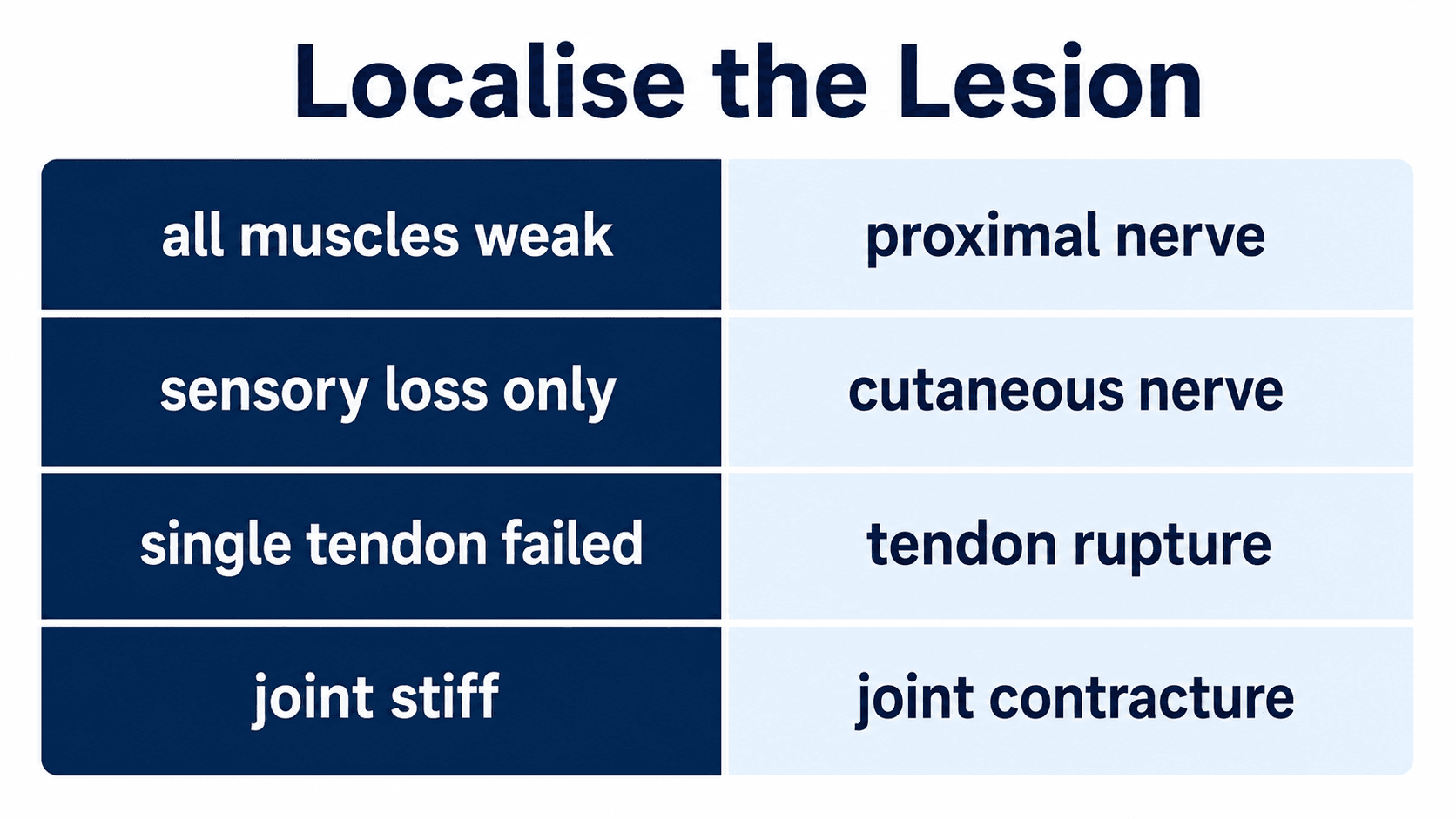
- Interpretation
- Tendon rupture, nerve palsy, pain inhibition or poor effort
- Next test
- Isolate tendon and test nerve pattern
- Interpretation
- Joint stiffness, contracture, swelling, adhesions or mechanical block
- Next test
- Assess end feel, imaging and inflammatory/infective signs
- Interpretation
- Pain inhibition, infection, fracture, instability or CRPS
- Next test
- Do not force; investigate urgent causes
- Interpretation
- Peripheral nerve lesion above sensory branch
- Next test
- Map motor and sensory territories
- Interpretation
- AIN or PIN, tendon rupture, central cause or muscle injury
- Next test
- Use nerve-specific motor tests and tendon isolation
Pathophysiology
Clinical signs in the hand arise from predictable failure patterns. Understanding the mechanism prevents misdiagnosis.
- Clinical effect
- Loss of active movement across one joint while passive motion is preserved
- Example
- FDP laceration causing absent DIP flexion
- How to prove it
- Isolate that tendon and check wound level
- Clinical effect
- Weakness follows a nerve distribution, often with sensory or autonomic change
- Example
- Ulnar palsy causing FDI wasting and pinch weakness
- How to prove it
- Map motor and sensory pattern, then localise level
- Clinical effect
- Active and passive motion are both limited
- Example
- PIP contracture after injury
- How to prove it
- Assess passive end feel and radiographs
- Clinical effect
- Apparent weakness without a consistent anatomical pattern
- Example
- Acute fracture, infection or CRPS
- How to prove it
- Control pain, identify driver and repeat focused testing
- Clinical effect
- Characteristic deformity from tendon, ligament or intrinsic imbalance
- Example
- Boutonniere, swan neck or ulnar claw
- How to prove it
- Match posture to the disrupted stabiliser
Important consequences:
- Tendon rupture is a mechanical failure and will not recover with nerve observation.
- Nerve palsy can recover, need decompression, need repair or need tendon transfer depending level, cause and time course.
- Joint stiffness becomes harder to reverse with time, especially in the PIP joint.
- Pain-limited motion can hide a tendon or nerve injury; reassess once pain is controlled but do not delay urgent referral.
Clinical Assessment
Position and exposure
Sit opposite the patient with both hands and forearms exposed. The hands should rest on a table so the cascade, resting posture, sweat pattern, scars, wasting and deformity can be compared side to side.
History
Ask questions that help localisation:
- Mechanism: sharp laceration, crush, fall, bite, closed rupture, gradual compression or inflammatory disease.
- Timing: acute tendon/nerve injury, delayed rupture, chronic compression or progressive deformity.
- Wound: location, depth, contamination, glass, bite, machinery, farm or water exposure.
- Symptoms: pain, numbness, paraesthesia, weakness, triggering, locking, cold intolerance, colour change.
- Function: writing, buttons, pinch, grip, tools, keyboard, sport, musical instrument and work demands.
- Previous pathology: distal radius fracture, rheumatoid disease, diabetes, cervical radiculopathy, previous tendon repair, carpal tunnel release or nerve injury.
Inspection
Look before touching:
- resting finger cascade
- rotational deformity or scissoring
- wounds in relation to tendon and nerve zones
- swelling, bruising, erythema, drainage or bite marks
- thenar, hypothenar and first dorsal interosseous wasting
- trophic skin changes, sweating asymmetry or dry skin
- nail-bed injury, mallet posture, boutonniere posture or swan-neck posture
- Dupuytren nodules, cords and contracture
- rheumatoid MCP ulnar drift, Z-thumb and tendon imbalance
An abnormal finger cascade may reveal tendon rupture, rotational malalignment, intrinsic imbalance or pain guarding before formal testing begins.
Tendon Examination
Flexor tendons
- How to test
- Hold PIP extended and ask for DIP flexion
- Positive finding
- No active DIP flexion
- Clinical meaning
- FDP rupture or laceration; zone depends on wound and level
- How to test
- Hold other fingers extended and ask tested finger to flex PIP
- Positive finding
- No isolated PIP flexion
- Clinical meaning
- FDS rupture, laceration or normal variant, especially little finger
- How to test
- Stabilise thumb MCP and ask for thumb IP flexion
- Positive finding
- No active IP flexion
- Clinical meaning
- FPL rupture/laceration or AIN palsy depending pattern
- How to test
- Palpate A1 pulley while flexing and extending
- Positive finding
- Clicking, locking or painful nodule
- Clinical meaning
- Stenosing tenosynovitis
Important interpretation:
- A clean volar laceration over the finger with loss of isolated tendon function is a tendon injury until proven otherwise.
- Flexor tendon injury should be assessed before local anaesthetic blocks eliminate useful motor testing.
- The finger may still flex weakly through adjacent tendons, lumbricals or tenodesis, so isolated testing is essential.
- In an open flexor injury, document digital nerve and artery status before dressing and referral.
Because the lumbricals originate from the FDP tendons and insert into the extensor (lateral band) mechanism, two classic phenomena confuse the unwary:
- Lumbrical-plus finger - paradoxical PIP extension on attempted flexion. When the FDP is functionally lengthened (a distal FDP laceration or avulsion, an over-long flexor graft, or amputation distal to the FDS), pulling on FDP no longer flexes the fingertip and instead tensions the lumbrical, which extends the PIP and DIP through the lateral bands - the harder the patient tries to make a fist, the more that finger straightens. Treatment addresses the slack FDP (lumbrical release or graft revision).
- Quadriga - because the FDP to the middle, ring and little fingers shares a common muscle belly, over-advancing or over-tightening one FDP (or an FDP tethered by a tight repair or amputation stump) limits active flexion of the other fingers, producing a weak, incomplete grip and an extension lag in the neighbouring digits. Avoid over-shortening the FDP at repair or amputation closure.
Both are mechanical, not neurological - the giveaway is the shared FDP linkage, not a nerve territory.
Extensor tendons
- Test
- Ask for active DIP extension
- Positive finding
- DIP extensor lag
- Meaning
- Mallet injury or terminal tendon rupture
- Test
- Elson test with PIP flexed over table edge
- Positive finding
- Weak PIP extension with rigid DIP extension
- Meaning
- Central slip rupture; boutonniere risk
- Test
- Ask for thumb IP extension or thumb retropulsion
- Positive finding
- Loss of thumb IP extension
- Meaning
- EPL rupture or radial/PIN lesion
- Test
- Ask for MCP extension of fingers
- Positive finding
- Loss of MCP extension
- Meaning
- Extensor tendon rupture, radial/PIN lesion or sagittal band problem
- Test
- Observe tendon tracking during MCP flexion/extension
- Positive finding
- Extensor tendon subluxation
- Meaning
- Boxer's knuckle or inflammatory sagittal band rupture
The decision is not simply "tendon cut". Record wound level, tendon function, digital nerve sensation, perfusion, contamination, tetanus status and timing before definitive management.
Nerve Examination
Core motor tests
- Motor test
- Abductor pollicis brevis
- What it tests
- Thenar motor branch
- Pattern clue
- Weak palmar thumb abduction with radial digit sensory symptoms
- Motor test
- OK sign: FPL and FDP index
- What it tests
- Pure motor branch
- Pattern clue
- Weak thumb IP and index DIP flexion with no sensory loss
- Motor test
- First dorsal interosseous finger abduction
- What it tests
- Deep motor branch and interossei
- Pattern clue
- FDI wasting, Froment sign, clawing pattern
- Motor test
- Wrist, finger and thumb extension
- What it tests
- Radial/PIN motor
- Pattern clue
- High radial lesion has wrist drop; PIN lesion has motor loss without sensory loss
Core sensory tests
- Useful point
- Index finger pulp
- Why it helps
- Reliable radial digital sensory territory
- Pitfall
- Palmar cutaneous branch may be spared in carpal tunnel syndrome
- Useful point
- Little finger pulp
- Why it helps
- Useful ulnar digital sensory territory
- Pitfall
- Dorsal ulnar sensation helps separate wrist from more proximal lesions
- Useful point
- Dorsal first web space
- Why it helps
- Superficial radial sensory territory
- Pitfall
- PIN palsy has no sensory loss
- Useful point
- Radial and ulnar sides of each digit
- Why it helps
- Localises finger-level laceration
- Pitfall
- Compare with adjacent digit and opposite hand
High-yield localisation patterns
Carpal tunnel causes thenar weakness and radial digit symptoms. AIN palsy causes FPL and FDP index weakness without sensory loss. A proximal median lesion adds forearm pronation and flexor involvement.
Low ulnar lesions affect intrinsics more than FDP. High ulnar lesions add FCU and FDP ring/little weakness. Dorsal ulnar sensory sparing suggests a lesion distal to the dorsal cutaneous branch.
High radial nerve palsy affects wrist, finger and thumb extension and may have sensory loss. PIN palsy is motor only and commonly affects finger/thumb extension more than wrist extension.
Test both sides of each digit after laceration. Two-point discrimination and light touch should be documented before repair or exploration.
Motor deficit without sensory loss should make you consider AIN palsy, PIN palsy or tendon rupture. The pattern of individual tendons then separates nerve from tendon.
Joint and Deformity Assessment
Joint assessment explains stiffness, deformity and instability.
Range and end feel
- Measure MCP, PIP and DIP active and passive range.
- Look for extension lag versus fixed flexion contracture.
- Check whether motion improves when adjacent joints are positioned differently.
- Compare soft end feel, hard bony block and pain-limited movement.
Deformity localisation
- Appearance
- DIP flexion posture
- Mechanism
- Terminal extensor disruption or bony avulsion
- Clinical implication
- Assess open injury, subluxation and extensor lag
- Appearance
- PIP flexion with DIP hyperextension
- Mechanism
- Central slip failure and lateral band migration
- Clinical implication
- Early Elson test matters
- Appearance
- PIP hyperextension with DIP flexion
- Mechanism
- Volar plate laxity, intrinsic imbalance or inflammatory disease
- Clinical implication
- Treat underlying cause, not the shape alone
- Appearance
- MCP hyperextension with IP flexion, worse ring/little
- Mechanism
- Ulnar intrinsic weakness
- Clinical implication
- Low ulnar lesions claw more than high lesions
- Appearance
- Finger overlap on flexion
- Mechanism
- Metacarpal or phalangeal malrotation
- Clinical implication
- Radiographs may underestimate clinically important rotation
When PIP flexion is limited, decide whether the block is intrinsic muscle tightness, extrinsic (extensor/capsular) tightness or PIP joint contracture - the Bunnell-Littler test does this. With the MCP held in extension (which tightens the intrinsics) assess passive PIP flexion, then flex the MCP (relaxing the intrinsics) and reassess. If PIP flexion improves with the MCP flexed, the limitation is intrinsic tightness; if PIP flexion stays equally limited in both positions, the problem is PIP joint or capsular contracture; if it is worse with the MCP flexed, suspect extrinsic extensor tightness. The analogous DIP test is the Haines-Zancolli (oblique retinacular ligament) test: passive DIP flexion that is limited with the PIP extended but free with the PIP flexed indicates a tight oblique retinacular ligament (Landsmeer) rather than a DIP joint contracture. These tests separate therapy from intrinsic release from capsulotomy.
Function
Assess real tasks:
- key pinch
- pulp pinch
- tripod pinch
- power grip
- hook grip
- writing grip
- opening jar or using tools if relevant
- occupation-specific or sport-specific function
Vascular and Sensory Testing
The hand is intolerant of missed vascular injury. A pink finger can still have a single digital artery injury; urgency depends on perfusion, contamination, nerve injury and associated structural damage.
Vascular assessment
- Capillary refill and colour.
- Temperature compared with adjacent digits.
- Radial and ulnar pulses.
- Digital Allen testing when digital artery injury is suspected.
- Doppler signal when clinical perfusion is uncertain.
- Pulse oximetry waveform on injured digit if available.
Sensory assessment
- Light touch and pinprick for screening.
- Static two-point discrimination for digital nerve injury.
- Semmes-Weinstein monofilament testing when quantifying sensory threshold.
- Compare with the opposite hand and adjacent digits.
- Document before local anaesthetic, exploration or repair.
If sensory loss follows a digital nerve distribution after a sharp wound, the default assumption should be digital nerve injury. Document it and refer or explore appropriately.
Investigations
Clinical examination decides what imaging or tests are needed.
- Investigation
- Plain radiographs with appropriate views
- What it adds
- Bone injury, alignment, joint congruity and radio-opaque foreign body
- Investigation
- CT
- What it adds
- Bone detail, articular fragments and surgical planning
- Investigation
- MRI
- What it adds
- Soft-tissue detail and marrow oedema
- Investigation
- Ultrasound
- What it adds
- Dynamic tendon motion, neuroma, ganglion or compressive lesion
- Investigation
- Nerve conduction study and EMG
- What it adds
- Level, severity, denervation and recovery over time
A normal radiograph does not exclude tendon laceration, digital nerve injury, early infection, ligament injury or pain-limited instability.
Differential Diagnosis
The single most useful skill in hand examination is separating causes that produce the same surface appearance. Loss of active movement, weak grip and an abnormal posture each have several explanations, and the differentials carry very different urgencies.
- Differential to consider
- Tendon laceration, high median or ulnar lesion, pain inhibition, tendon adhesion, lumbrical-plus, locked trigger finger
- Discriminating feature
- Isolated tendon test, passive range, wound level and nerve pattern
- Why it matters
- Tendon rupture needs repair; pain inhibition resolves; nerve lesion needs level localisation
- Differential to consider
- EPL rupture, posterior interosseous nerve palsy, high radial palsy, sagittal band or extensor subluxation
- Discriminating feature
- Test other radial-innervated muscles and dorsal first web sensation
- Why it matters
- EPL rupture needs transfer; PIN palsy may recover or need decompression
- Differential to consider
- Carpal tunnel syndrome, C8/T1 radiculopathy, thoracic outlet, proximal median lesion, motor neurone disease
- Discriminating feature
- Sensory territory, neck and limb screen, electrodiagnostics
- Why it matters
- Avoids missing a proximal or systemic cause behind apparent carpal tunnel syndrome
- Differential to consider
- Low ulnar lesion, high ulnar lesion, C8/T1 lesion, intrinsic contracture, established Volkmann
- Discriminating feature
- Dorsal ulnar sensation, FDP ring/little power, FCU, claw severity
- Why it matters
- High versus low ulnar lesions and central causes differ in prognosis and treatment
- Differential to consider
- Infection, acute fracture, complex regional pain syndrome, gout/inflammatory flare, missed dislocation
- Discriminating feature
- Wound, systemic signs, radiographs, allodynia and disproportionate pain
- Why it matters
- Infection and compartment problems are time-critical and must not be labelled stiffness
- Differential to consider
- Digital nerve injury, partial laceration with neurapraxia, referred symptoms, pre-existing neuropathy
- Discriminating feature
- Sensory mapping on both sides of the digit and comparison with adjacent digits
- Why it matters
- A digital nerve laceration is a surgical problem until excluded
Examiners reward candidates who say what else the finding could be and how they would separate the options, rather than committing instantly to one diagnosis.
Management Decisions
The examination should lead to a decision, not just a diagnosis.
- Why it matters
- Ischaemia can become irreversible
- Immediate action
- Urgent hand/vascular assessment and perfusion protection
- Why it matters
- Deep contamination and instability
- Immediate action
- Sterile dressing, antibiotics when indicated, splint and urgent referral
- Why it matters
- Delayed diagnosis worsens repair and rehabilitation
- Immediate action
- Document tendon, nerve and vessel status, splint and refer
- Why it matters
- Repair decision depends on timing and wound status
- Immediate action
- Document sensory deficit before anaesthetic and refer
- Why it matters
- Rapid spread in closed compartments
- Immediate action
- Antibiotics, elevation, urgent surgical assessment
- Why it matters
- Tissue toxicity and compartment necrosis
- Immediate action
- Emergency referral even if skin wound looks small
Complications
Complications often come from missed localisation rather than from the examination itself.
- Possible consequence
- Persistent numbness, painful neuroma, poor pinch and delayed repair
- Prevention
- Test both sides of each digit before anaesthetic
- Possible consequence
- Delayed repair, adhesions, rupture, stiffness and poor function
- Prevention
- Isolate FDP and FDS in every suspicious volar wound
- Possible consequence
- Delayed boutonniere deformity
- Prevention
- Perform Elson test when PIP injury suggests extensor mechanism damage
- Possible consequence
- Ischaemia, cold intolerance or tissue loss
- Prevention
- Check colour, capillary refill, temperature, Doppler and digital perfusion
- Possible consequence
- Stiffness, scissoring and functional grip loss
- Prevention
- Assess passive range, cascade and radiographs
- Possible consequence
- Deep-space infection, tendon sheath infection, stiffness or amputation risk
- Prevention
- Recognise pain pattern, swelling, wounds and systemic signs early
Guidelines, Registries and Global Practice
Hand and wrist trauma is one of the highest-volume presentations in any emergency or orthopaedic service worldwide, and the clinical examination is the universal first step regardless of resource setting.
Global epidemiology
- Hand and wrist injuries account for a large share of all emergency department trauma presentations across high-, middle- and low-income settings, with lacerations, fractures and tendon injuries predominating in working-age adults.
- Occupational and machinery-related mechanisms are over-represented in industrial and agricultural economies, while falls and sport dominate in many high-income settings.
- Flexor and extensor tendon, digital nerve and vascular injuries cluster in young working adults, making accurate first-contact examination economically as well as clinically important.
Side-by-side guidance
- Emphasis
- Standards for open hand injury and timely specialist referral
- Practical point for examination
- Document tendon, nerve and vascular status of each digit before block or exploration
- Emphasis
- Structured upper limb and nerve examination, evidence appraisal of clinical tests
- Practical point for examination
- Combine provocative tests with sensorimotor examination; do not rely on single signs
- Emphasis
- Injury pattern, soft-tissue assessment and timing of management
- Practical point for examination
- Assess the soft-tissue envelope and neurovascular status before planning fixation
- Emphasis
- Harmonised hand surgery training and examination competencies
- Practical point for examination
- A reproducible, structured hand examination is a core trainee competency
Registry and practice variation
- Distal radius fracture fixation is tracked in arthroplasty and trauma registries and large series; flexor and extensor tendon rupture (especially FPL and EPL) is a recognised complication of volar plating, which is why specific thumb-tendon testing belongs in every post-fixation review.
- In well-resourced settings, ultrasound, MRI and electrodiagnostics are readily available adjuncts after the clinical examination.
- In limited-resource settings, the structured clinical examination carries even greater weight because imaging and electrodiagnostics may be delayed or unavailable; the same look-feel-move-test-function sequence still localises the lesion and triages urgency.
References
- 1Bulut T, Akgun U, Ozcan C, Unver B, Sener M. "Inter- and intra-tester reliability of sensibility testing in digital nerve repair". Journal of Hand Surgery (European Volume). 2015PubMed
- 2Herman ZJ, Ilyas AM. "Sensory Outcomes in Digital Nerve Repair Techniques: An Updated Meta-analysis and Systematic Review". Hand (New York). 2019PubMed
- 3Dabbagh A, MacDermid JC, Yong J, Packham TL, Grewal R, Boutsikari EC. "Diagnostic Test Accuracy of Provocative Maneuvers for the Diagnosis of Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis". Physical Therapy. 2023PubMed
- 4Rubin J, Bozentka DJ, Bora FW. "Diagnosis of closed central slip injuries. A cadaveric analysis of non-invasive tests". Journal of Hand Surgery (British Volume). 1996PubMed
- 5Arvind V, Hong DY, Strauch RJ. "Extensor Tendon Repair". JBJS Essential Surgical Techniques. 2024PubMed
- 6Peters SE, Jha B, Ross M. "Rehabilitation following surgery for flexor tendon injuries of the hand". Cochrane Database of Systematic Reviews. 2021PubMed
- 7Monaco NA, Dwyer CL, Ferikes AJ, Lubahn JD. "Hand Surgeon Reporting of Tendon Rupture Following Distal Radius Volar Plating". Hand (New York). 2016PubMed
- 8Alvarez DA, Ballard DH, Carroll T, Frilot C, Simoncini AA. "Ultrasound localization of lacerated flexor tendon ends in the hand: a cadaveric study". Skeletal Radiology. 2019PubMed
- 9Casaletto JA, Machin D, Leung R, Brown DJ. "Flexor pollicis longus tendon ruptures after palmar plate fixation of fractures of the distal radius". Journal of Hand Surgery (European Volume). 2009PubMed
Controversies and Areas of Uncertainty
Hand examination feels objective, but several widely taught manoeuvres are weaker than candidates assume. Knowing the limits is a hallmark of consultant-level reasoning.
- Common teaching
- Treated as confirmatory tests
- What the evidence shows
- Pooled Phalen sensitivity around 0.57 and Tinel sensitivity around 0.45; neither is accurate alone
- Practical position
- Combine clinical tests with sensorimotor findings, hand diagrams and electrodiagnostics
- Common teaching
- A 2PD value defines recovery
- What the evidence shows
- Static 2PD and monofilament reproducibility are poor; monofilament is the more reliable of the two
- Practical position
- Use a consistent method and interpret with motor and functional findings
- Common teaching
- Imaging confirms the cut
- What the evidence shows
- Ultrasound is highly accurate for complete laceration but operator dependent and adjunctive
- Practical position
- Use selectively when the examination is equivocal, not as a substitute
- Common teaching
- One protocol is clearly best
- What the evidence shows
- Cochrane evidence across protocols is very low certainty
- Practical position
- Refer for a structured supervised regimen; do not over-claim superiority of one method
- Common teaching
- Always repair or always observe
- What the evidence shows
- Thresholds for repair versus observation remain debated, especially around 60% division and triggering risk
- Practical position
- Document the percentage, discuss with a hand surgeon, and watch for triggering or rupture
At a Glance Table
- Most likely structure
- FDP
- How to confirm
- Hold PIP extended and ask for DIP flexion
- Important trap
- Pain or poor effort can mimic rupture
- Most likely structure
- FDS
- How to confirm
- Hold other fingers extended and ask tested finger to flex PIP
- Important trap
- Little finger FDS may be absent or weak normally
- Most likely structure
- EPL or radial/PIN
- How to confirm
- Check isolated thumb IP extension and other radial-nerve muscles
- Important trap
- EPL rupture after distal radius fracture can be missed
- Most likely structure
- Median nerve
- How to confirm
- APB strength and radial digit sensation
- Important trap
- AIN palsy has no sensory loss
- Most likely structure
- Ulnar nerve
- How to confirm
- Finger abduction/adduction and ulnar digit sensation
- Important trap
- High versus low ulnar lesions behave differently
- Most likely structure
- Radial nerve above PIN branch
- How to confirm
- EPL, wrist extension and first dorsal web sensation
- Important trap
- PIN palsy has no sensory loss
- Most likely structure
- Joint, capsule, adhesions or swelling
- How to confirm
- Compare passive motion and end feel
- Important trap
- Do not diagnose isolated tendon rupture without passive range
MAPHand Localisation
Hook:Map the problem before naming the diagnosis.
VINHand Trauma Red Flags
Hook:Vascular, infection and nerve findings change urgency.
ACTActive-Passive Interpretation
Hook:Active loss must be compared with passive range.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a clean volar laceration over the middle finger and says they cannot bend the fingertip.”
“A patient recovering after distal radius fracture treatment reports inability to extend the thumb IP joint.”
“A patient has hand intrinsic wasting, weak pinch and numbness in the little finger.”
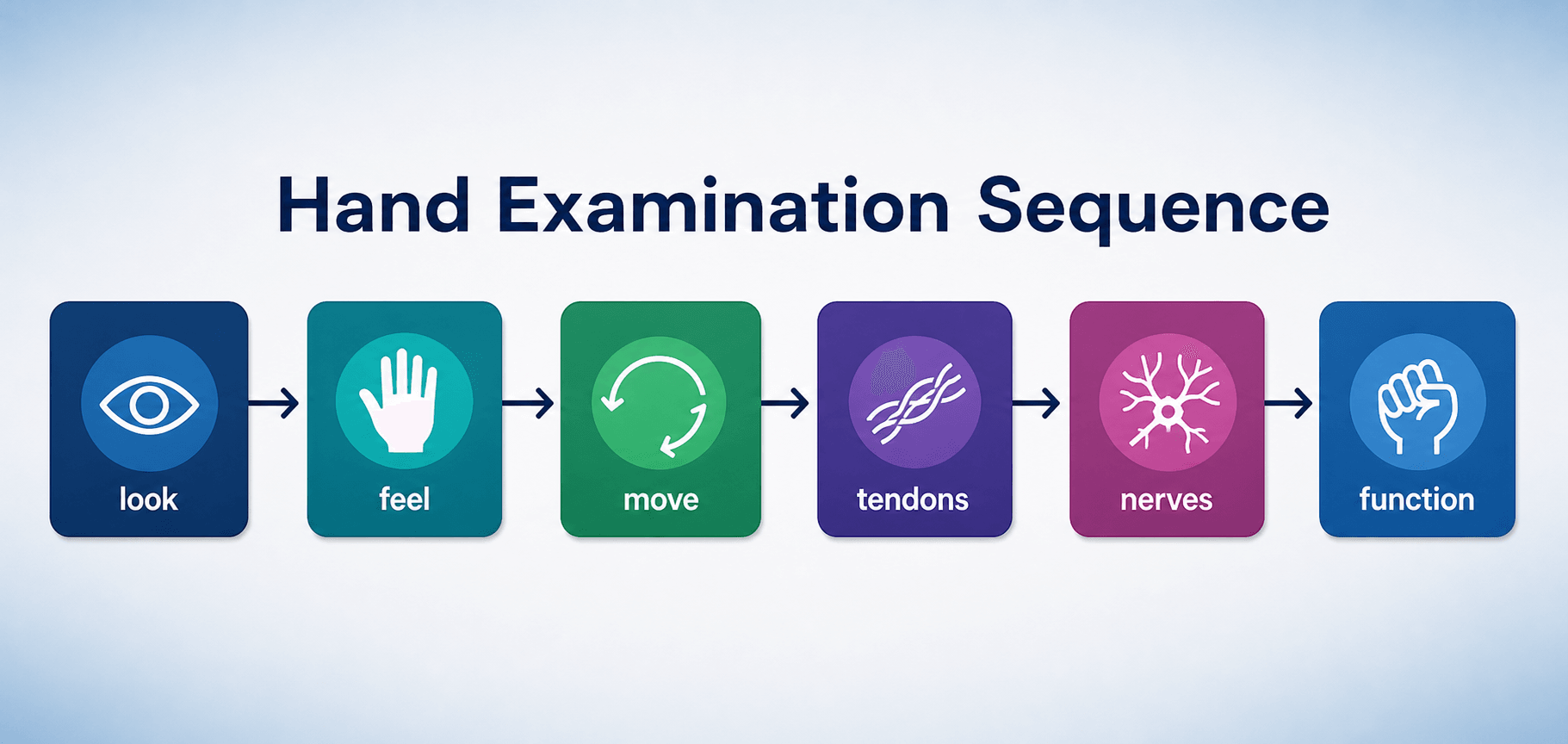
Sequence
- Look: cascade, wounds, wasting, deformity.
- Feel: tenderness, swelling, temperature, tendons.
- Move: active then passive range.
- Test: tendons, nerves, sensation, vessels.
- Function: pinch, grip and task-specific use.
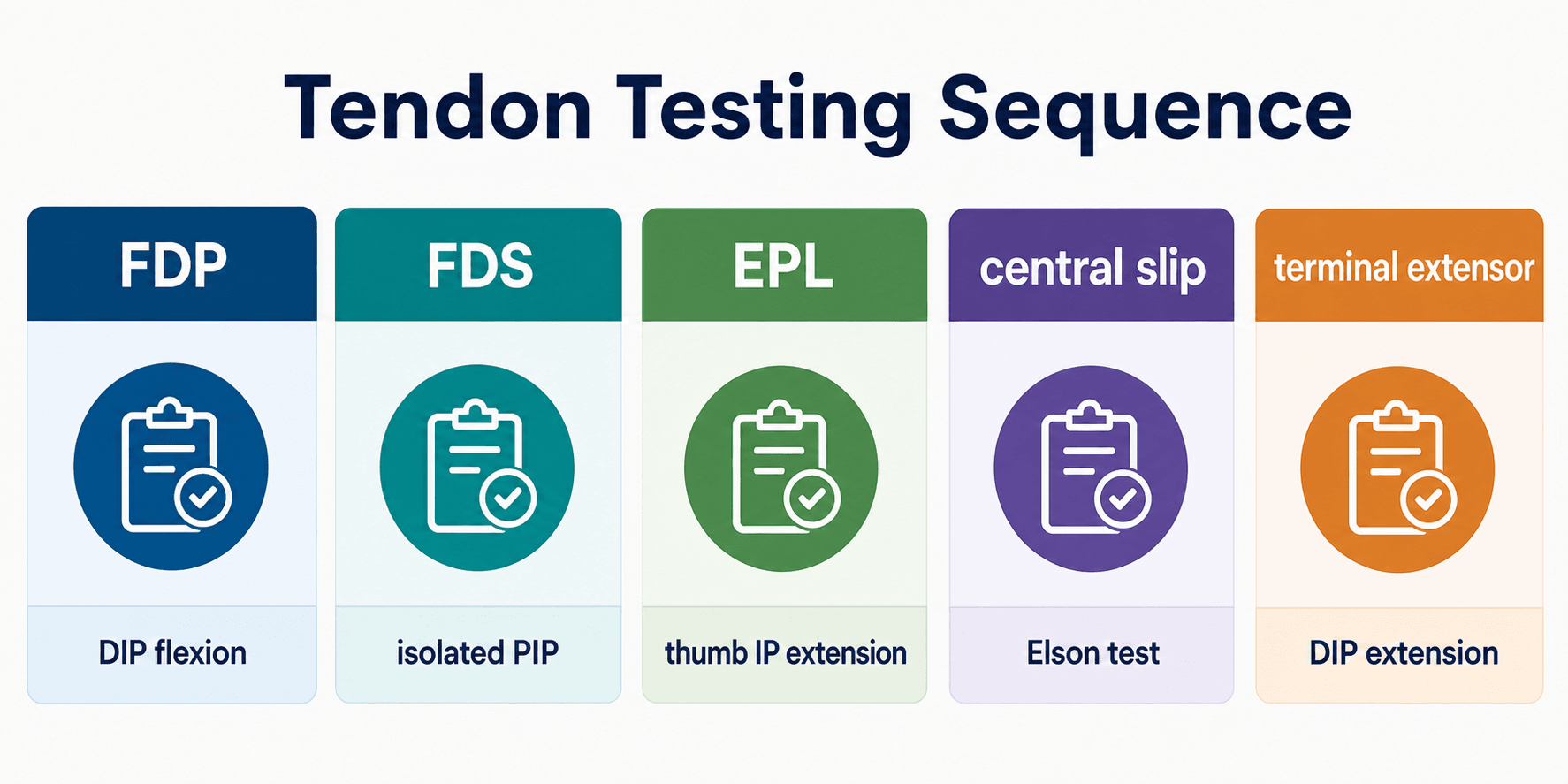
Tendons
- FDP: isolated DIP flexion.
- FDS: isolated PIP flexion with other fingers held extended.
- EPL: thumb IP extension and retropulsion.
- Central slip: Elson test.
- Terminal extensor: DIP extension.
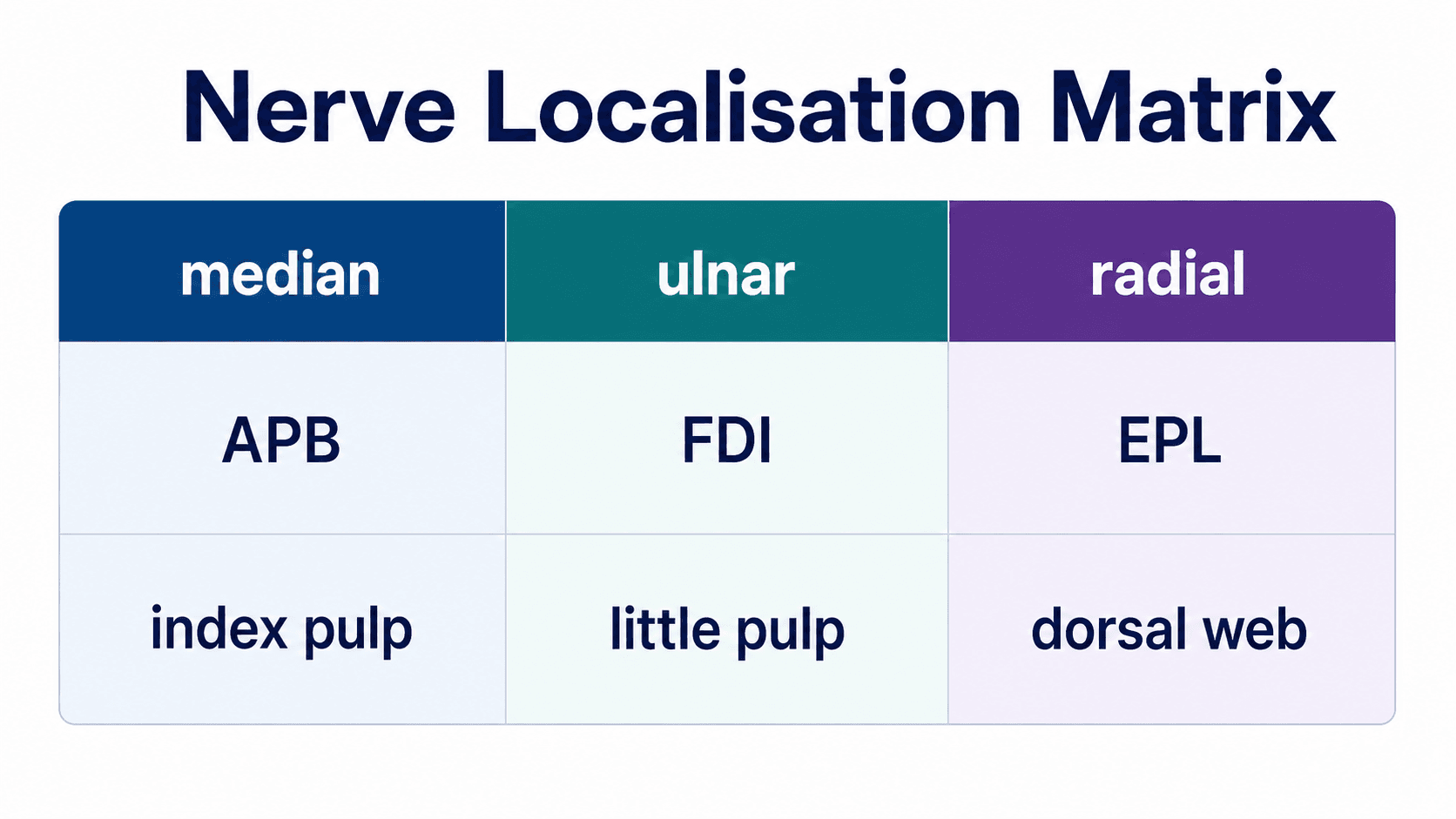
Nerves
- Median: APB and index pulp.
- AIN: OK sign, no sensory loss.
- Ulnar: FDI and little finger pulp.
- Radial/PIN: wrist, finger and thumb extension.
- PIN: motor only.
Urgent
- Vascular compromise.
- Open joint, open fracture or tendon laceration.
- Digital nerve injury with open wound.
- Bite, flexor sheath infection or deep-space infection.
- Compartment syndrome or high-pressure injection injury.
“A good hand examination identifies the failed structure, localises the level and decides urgency. Active-passive comparison and isolated tendon/nerve testing prevent most errors.”
Evidence Base
Reliability of sensibility testing in digital nerve repair
- 100 digital nerves in 67 patients assessed for static two-point discrimination and Semmes-Weinstein monofilament reproducibility.
- Reproducibility was poor for both tests, but the monofilament test was more reliable than static two-point discrimination.
- Sensibility test scores should not be used in isolation to monitor sensory recovery.
Sensory outcomes after digital nerve repair: updated meta-analysis
- 15 studies and 625 digital nerve repairs pooled across neurorrhaphy, autograft, allograft and conduit techniques.
- For static two-point discrimination, autograft repair was statistically superior to all other techniques.
- When a nerve gap exists, autograft and allograft performed comparably and both outperformed conduit repair.