Benign Subungual Neuromyoarterial Hamartoma | Classic Pain Triad | Marginal Excision
- Classic triad: paroxysmal pain + pinpoint tenderness + cold sensitivity
- Love test: pinhead pressure on the tender spot causes disproportionate pain
- Hildreth test: tourniquet exsanguination abolishes the pain (highly specific)
- MRI is the imaging gold standard - well-defined T2 hyperintense lesion
- Treatment is marginal surgical excision - cure rate greater than 90 percent
- “Glomus body = arteriovenous anastomosis (Sucquet-Hoyer canal) for thermoregulation
- “Tumour arises from modified smooth muscle cells of the glomus body
- “Subungual lesions may show a faint blue-red spot beneath the nail plate
- “Plain X-ray can show scalloped erosion of the distal phalanx dorsal cortex
- “Always send the specimen for histology - exclude subungual melanoma
Glomus body = neuromyoarterial structure in reticular dermis. Regulates skin blood flow and temperature. Most concentrated in the fingertips and subungual region. The tumour arises from modified smooth muscle cells of the Sucquet-Hoyer canal, an arteriovenous anastomosis.
Paroxysmal pain + pinpoint tenderness + cold sensitivity. Triad is pathognomonic when all three features are present. Mean diagnostic delay is around 7 years - high index of suspicion is essential in any unexplained fingertip pain.
Love test: pinhead pressure (tip of a pencil or paper clip) on the tender spot causes severe disproportionate pain. Hildreth test: exsanguination with a finger tourniquet abolishes the pain - the test is positive when the patient cannot localise the pain once exsanguinated.
Marginal surgical excision is curative. Cure rate greater than 90 percent with complete excision. Recurrence (10-20 percent) usually reflects incomplete excision, a satellite lesion, or a second glomus tumour. Histology is mandatory to exclude subungual melanoma.
- Diagnosis
- Love positive + Hildreth positive + MRI T2 hyperintense lesion
- Treatment
- Marginal excision with nail bed repair
- Key Pearl
- Cure rate greater than 90 percent with complete excision
- Diagnosis
- MRI confirms subungual lesion; X-ray for cortical erosion
- Treatment
- Transungual approach with partial nail avulsion
- Key Pearl
- Preserve nail matrix to prevent permanent nail dystrophy
- Diagnosis
- MRI to localise residual or satellite lesion
- Treatment
- Re-excision with wider margin ± two-stage repair
- Key Pearl
- Always consider a missed satellite or a second glomus
TRIADClassic Triad of Glomus Tumour
Hook:A glomus tumour TRIAD: Triggered pain, Reproduction on pressure, Intolerance to cold, Accurate spot, and Disappears with Hildreth - the pathognomonic set the examiner expects.
LATERALSurgical Excision Approach
Hook:LATERAL approach: Localise, Approach by site, Tourniquet, Excise, Repair, Allow regrowth, Look for recurrence.
GLOMUSDifferential Diagnosis of a Subungual Lesion
Hook:GLOMUS differential: do not miss Glomus, Lentigo/melanoma, Onychomycosis, Mucoid cyst, Underlying exostosis, or SCC - pigmented or painful subungual lesions must be biopsied.
Overview and Epidemiology
Glomus tumours of the hand are uncommon but cause disproportionately severe symptoms. The classic triad of paroxysmal pain, pinpoint tenderness and cold sensitivity is so specific that, when recognised, the diagnosis is essentially clinical. Yet the average diagnostic delay is around 7 years, because clinicians do not examine the nail bed carefully and do not perform Love and Hildreth tests. A missed glomus tumour means years of unnecessary pain, multiple specialist visits, and often incorrect diagnoses of Raynaud disease, neuropathy, psychiatric pain or chronic regional pain syndrome.
- Frequency: 1 to 5 percent of all hand tumours
- Age: peak in the third to fifth decades, but reported at any age
- Sex: female predominance (approximately 2-3 to 1)
- Location: 75 to 80 percent subungual; remainder in pulp, volar finger, palm
- Multiple lesions: approximately 10 percent, often familial (glomuvenous malformation)
- Disabling pain: paroxysmal, triggered by cold and pressure
- Diagnostic delay: average 7 years from symptom onset
- Functional loss: avoidance of typing, writing, tool use, cold weather
- Psychological impact: chronic undiagnosed pain, anxiety, sleep disturbance
- Cost: multiple GP and specialist visits, unnecessary imaging and treatment
Pathophysiology
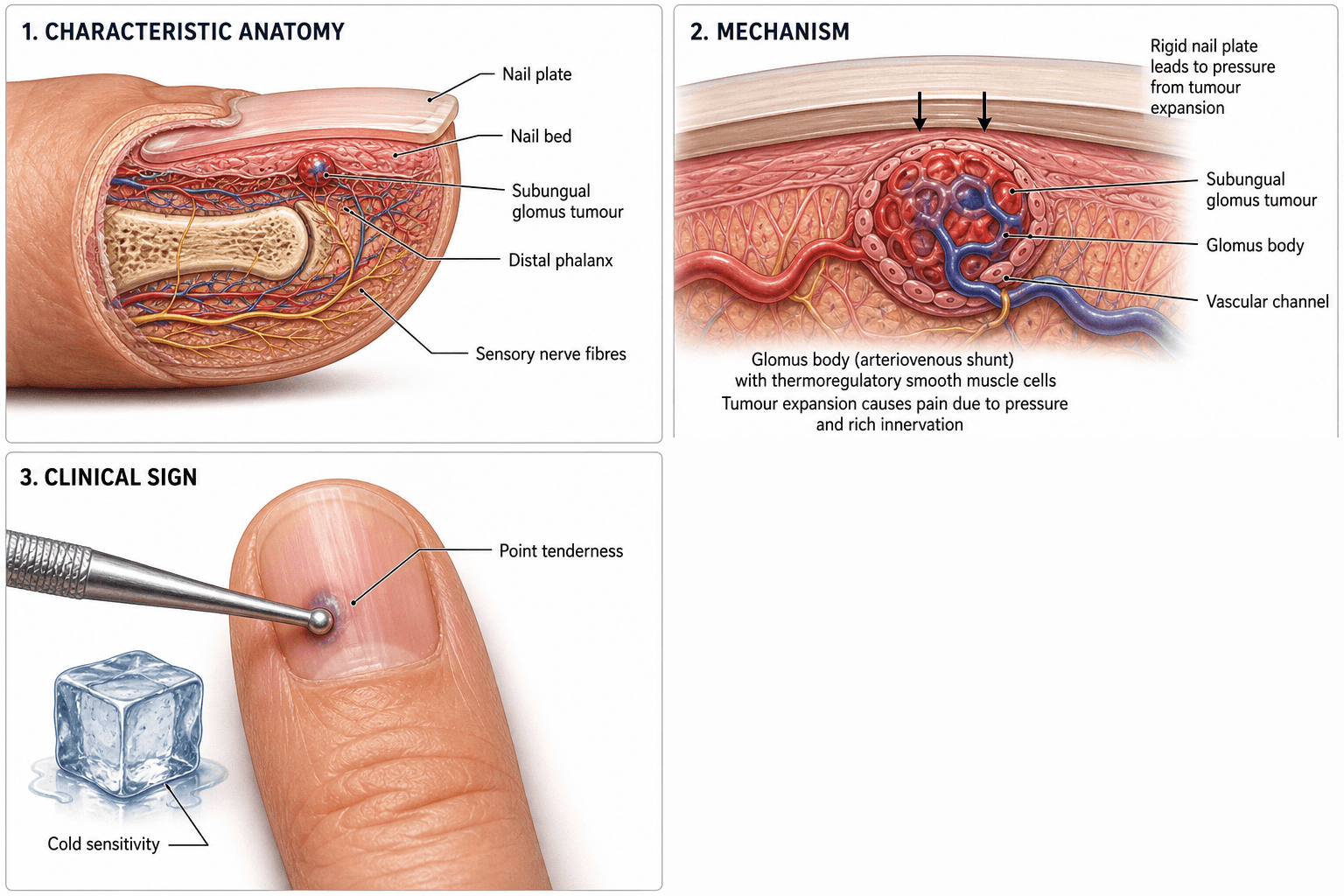
The normal glomus body is a specialised arteriovenous anastomosis (Sucquet-Hoyer canal) located in the reticular dermis. It is composed of an afferent arteriole, the Sucquet-Hoyer canal, an efferent venule, and an intraglomerular reticulum of modified smooth muscle cells. Its function is thermoregulation: it shunts blood flow in the skin in response to temperature, particularly in the fingertips, toes and subungual regions. A glomus tumour is a benign hamartomatous proliferation of these modified smooth muscle cells, producing a small, well-circumscribed, purple-red nodule that is rich in nerve fibres - hence the exquisite pain.
- Description
- Spindle or epithelioid glomus cells around vascular spaces
- Contribution to Symptoms
- Cause of bulk of tumour; positive for SMA and vimentin
- Description
- Small, endothelium-lined channels within the lesion
- Contribution to Symptoms
- Cold-induced vasoconstriction triggers paroxysmal pain
- Description
- Abundant unmyelinated C fibres within and around the tumour
- Contribution to Symptoms
- Pinpoint tenderness, hyperalgesia, Love and Hildreth positivity
Pain: dense unmyelinated C-fibre innervation of the lesion
Cold sensitivity: thermoregulatory origin of the parent cell; vascular channels constrict in cold
Pinpoint tenderness: small (1-5 mm) discrete, encapsulated, superficial nodule
Hildreth relief: exsanguination empties the vascular channels and removes pressure on nerve fibres
Tumour is tiny (1-5 mm) and often invisible on inspection
Plain X-ray is frequently normal in early disease
Symptoms are episodic - patients are well between attacks
Misdiagnosis is common: neuroma, Raynaud, arthritis, CRPS, psychiatric pain
Average 7 years from first symptom to correct diagnosis in published series
Histologically, glomus tumours are well-circumscribed nodules composed of uniform, round, epithelioid glomus cells arranged in nests around small vascular channels. The cells are positive for smooth muscle actin (SMA), vimentin and h-caldesmon, and negative for S100, CD31 and cytokeratins - useful in distinguishing them from melanoma, neurofibroma and adnexal tumours. A fibrous pseudocapsule is typical, supporting the concept of marginal (rather than wide) excision.
Classification and Types
Classification by Anatomic Location
- Frequency
- 75-80 percent
- Typical Sign
- Blue-red spot, nail ridging, possible cortical erosion
- Surgical Approach
- Transungual with partial or total nail avulsion
- Frequency
- 10-15 percent
- Typical Sign
- Small palpable nodule, localised tenderness
- Surgical Approach
- Direct volar marginal excision
- Frequency
- Less than 5 percent
- Typical Sign
- Small bluish nodule visible or palpable
- Surgical Approach
- Direct excision over lesion
- Frequency
- Approximately 10 percent
- Typical Sign
- Several painful bluish nodules; AD inheritance (glomulin gene)
- Surgical Approach
- Selective excision of symptomatic lesions
Location dictates approach; subungual lesions are the most common and technically the most demanding.
Although the overwhelming majority of glomus tumours are benign, a malignant variant - the glomangiosarcoma (malignant glomus tumour) - is rare but real, so "benign" is the rule rather than a guarantee. The Folpe criteria stratify malignancy on histology: a glomus tumour is malignant if it shows either (a) marked nuclear atypia with any mitotic activity, or (b) atypical (abnormal) mitotic figures. Lesions that are large (over 2 cm) and/or deep (subfascial/visceral) but lack these features are classed as uncertain malignant potential, and those with a single worrying feature such as large size alone are termed symplastic/atypical.
Practical points: malignant glomus tumours are far more common in deep or extradigital sites than in the typical superficial subungual location, they can metastasise (lungs), and this is a second reason - beyond excluding melanoma - that every excised specimen must go to histology. A genuinely malignant or uncertain-potential lesion warrants wide excision and oncological follow-up, not simple marginal excision.
Clinical Assessment
- Pain pattern: episodic, paroxysmal, sharp or burning
- Triggers: cold exposure, light pressure, dependency
- Localisation: patient points to a single fingertip or subungual spot
- Duration: average 7 years from symptom onset to diagnosis
- Prior diagnoses: neuroma, Raynaud, arthritis, CRPS, psychiatric pain
- Inspect: subungual blue-red spot, nail ridging, onycholysis
- Palpate: small, well-defined, exquisitely tender nodule
- Love test: tip of a paper clip or pencil - disproportionate pain
- Hildreth test: tourniquet exsanguination - pain abolished
- Cold test: ice cube on the digit reproduces pain (less specific)
Love test: With the patient seated and the hand rested, apply the tip of a paper clip, ballpoint pen or cotton-tipped applicator to the suspected spot. A positive test is disproportionate, sharp pain with minimal pressure. The patient typically withdraws the hand.
Hildreth test (ischaemic test): Apply a digital tourniquet (Penrose drain or finger of a glove) at the base of the affected digit. Exsanguinate the digit by wrapping or milking blood proximally, then inflate or tighten the tourniquet. A positive test is complete abolition of the pain (and often of the ability to localise it) while the digit is exsanguinated. Release of the tourniquet causes immediate return of pain.
A positive Hildreth test is highly specific for glomus tumour and helps differentiate it from other causes of fingertip pain, including neuroma and small nerve entrapment.
- Technique
- Pinhead pressure on tender spot
- Positive Finding
- Sharp, disproportionate pain
- Notes
- Easy to perform at the bedside; high sensitivity
- Technique
- Exsanguination with finger tourniquet
- Positive Finding
- Pain abolished while exsanguinated
- Notes
- Highly specific for glomus tumour
- Technique
- Ice cube or cold water on digit
- Positive Finding
- Reproduction of pain
- Notes
- Helpful but less specific; positive in Raynaud too
- Technique
- Penlight through distal phalanx
- Positive Finding
- Small reddish mass visible under nail
- Notes
- Useful adjunct for subungual lesions
- Discriminating Feature
- Classic triad; small bluish spot; positive Love and Hildreth
- Key Test
- Love and Hildreth
- Imaging
- MRI T2 hyperintense lesion; possible cortical erosion on X-ray
- Discriminating Feature
- Slow-growing firm nodule lifting the nail
- Key Test
- Inspection and X-ray
- Imaging
- X-ray diagnostic: bony outgrowth from distal phalanx
- Discriminating Feature
- Pigmented streak (Hutchinson sign if proximal fold), irregular border
- Key Test
- Biopsy (excisional)
- Imaging
- Dermoscopy; MRI for staging if confirmed
- Discriminating Feature
- Dorsal DIP, ganglion-like, often with degenerative joint
- Key Test
- Inspection and aspiration
- Imaging
- X-ray shows DIP osteophytes; MRI shows cyst
- Discriminating Feature
- Burning pain along nerve distribution, Tinel positive
- Key Test
- Tinel and nerve block
- Imaging
- MRI may show small nerve lesion
- Discriminating Feature
- Bilateral, colour change, cold-induced
- Key Test
- Cold challenge, nailfold capillaroscopy
- Imaging
- Not a focal lesion; X-ray and MRI normal
- Discriminating Feature
- Diffuse hand pain, swelling, vasomotor changes
- Key Test
- Budapest criteria
- Imaging
- Three-phase bone scan (old); clinical diagnosis
Hildreth's ischaemic test is the most specific bedside test for glomus tumour. When the finger is exsanguinated, the patient who previously could localise the pain to a single point can no longer find the spot. This near-pathognomonic sign, combined with the classic triad, should be sufficient to justify surgery without further imaging - though MRI is still obtained for surgical planning.
The familial, multiple "glomus tumours" are a genuinely different entity - glomuvenous malformations (GVM) - and the distinction matters for both the exam and management:
- Solitary glomus tumour: single, tiny, exquisitely painful (classic triad), usually subungual, sporadic, cured by marginal excision.
- Glomuvenous malformation (GVM): multiple, often plaque-like or nodular bluish, partially compressible lesions that are frequently non-tender or only mildly tender (NOT the paroxysmal triad), inherited autosomal dominant via the GLMN (glomulin) gene with a paradominant / "second-hit" mechanism (hence the patchy distribution and variable penetrance).
GVMs are venous-predominant histologically (the glomangioma pattern) and respond poorly to simple excision; symptomatic or cosmetically troublesome lesions may be treated with sclerotherapy or laser as well as selective excision. The take-home: a painful solitary subungual lesion is a classic glomus tumour, whereas multiple compressible, non-tender bluish lesions with a family history are a glomuvenous malformation - so examine the skin and ask about affected relatives.
Investigations
Imaging and Diagnostic Protocol
Views: PA and true lateral of the affected digit
Look for: Scalloped erosion of the dorsal cortex of the distal phalanx (pathognomonic when present)
Limitation: Normal in many cases - tumour is soft tissue only
Always obtain before MRI to exclude exostosis, bone tumour or significant deformity
Indication: Quick, cheap screen in clinic; operator dependent
Findings: Small, well-defined, hypoechoic, hypervascular nodule
Limit: Deeply subungual lesions may be obscured by nail plate
Indication: All suspected glomus tumours before surgery
Sequences: T1, T2 fat-sat or STIR, post-gadolinium T1 fat-sat
Findings: Well-circumscribed, T2 hyperintense, strongly enhancing nodule beneath nail
Advantage: Localises occult or satellite lesions; guides surgical approach
Indication: Always send excised specimen
Findings: Nests of uniform glomus cells around vascular channels; SMA positive, S100 negative
Purpose: Confirms diagnosis and excludes melanoma or other lesion
A scalloped erosion of the dorsal cortex of the distal phalanx on plain X-ray is highly suggestive of a long-standing subungual glomus tumour - the slow-growing lesion has remodelled the bone. When present, it is a useful pre-operative confirmatory sign. However, a normal X-ray does NOT exclude a glomus tumour. MRI is the imaging gold standard, and modern high-resolution sequences (3 T with a dedicated surface coil) can identify lesions as small as 1 to 2 mm.
- Best For
- First-line screen, exclude exostosis
- Findings
- Scalloped dorsal cortical erosion of distal phalanx
- Limitations
- Normal in many cases; cannot see soft-tissue tumour
- Best For
- Quick screen in clinic
- Findings
- Hypoechoic, hypervascular subungual nodule
- Limitations
- Operator dependent; obscured by nail plate
- Best For
- Localise lesion and any satellite
- Findings
- T2 hyperintense, enhancing nodule on T1 fat-sat post-gad
- Limitations
- Cost; not always available urgently
- Best For
- Definitive diagnosis
- Findings
- Glomus cells, SMA positive, S100 negative
- Limitations
- Post-excision only
Management Algorithm
Subungual Glomus Tumour
Goal: Complete marginal excision of the lesion with preservation of the nail matrix and minimum nail dystrophy
Surgical Protocol
Imaging: MRI to localise the lesion, identify satellites, and plan approach
Marking: Use Love test to mark the spot immediately before surgery (regional block can be done first, but the mark should be made before distortion)
Consent: Recurrence (10-20 percent), nail dystrophy, persistent pain
Anaesthesia: Digital block; confirm positive Hildreth test under block if feasible
Tourniquet: Finger tourniquet for bloodless field
Technique A - Transungual: Partial or total nail plate avulsion, then longitudinal incision of nail bed directly over the lesion
Technique B - Subungual (Littler): Lateral subungual incision, raising a nail bed flap, preserving the nail plate
Excision: Sharp dissection around the well-defined, blue-red nodule; take a 1-2 mm cuff of normal tissue
Nail bed repair: 6-0 or 7-0 absorbable (e.g. polyglactin) interrupted sutures under loupe magnification
Replace nail plate: Acts as a physiological splint for the repaired nail bed and prevents synechiae
Dressing: Non-adherent, soft, with the fingertip exposed
Splint: Light protective dressing for 10-14 days
Healing: Nail bed heals in 2-3 weeks; new nail grows at approximately 0.1 mm per day
Follow-up: 2 weeks for wound review, 6 weeks, 3, 6 and 12 months for recurrence check
The Littler (lateral subungual) approach preserves the nail plate and offers excellent exposure for radial or ulnar subungual lesions, with less post-operative nail dystrophy. The transungual approach with partial nail avulsion gives direct midline access and is preferred for centrally placed lesions, but carries a higher risk of nail ridging. Choose the approach that gives the best exposure for the lesion's location, rather than a one-size-fits-all incision.
Complications
- Incidence
- 10-20 percent
- Risk Factors
- Incomplete excision, missed satellite, multifocal disease
- Management
- MRI and re-excision; histology to confirm
- Incidence
- Up to 20 percent of subungual excisions
- Risk Factors
- Transungual approach, matrix injury, scar contracture
- Management
- Nail bed revision; long-term observation
- Incidence
- Less than 5 percent
- Risk Factors
- Wrong diagnosis, neuroma, CRPS
- Management
- MDT review; targeted nerve block; consider capsaicin
- Incidence
- 5-10 percent
- Risk Factors
- Volar approach in pulp, neuroma
- Management
- Desensitisation therapy; neuroma excision if needed
- Incidence
- Less than 2 percent
- Risk Factors
- Diabetes, poor hygiene, distal location
- Management
- Oral antibiotics; rare surgical drainage
When a patient returns with recurrent pain after a technically sound glomus excision, the two most likely explanations are a missed satellite lesion (multifocal disease) or an incomplete first excision. Before re-operating, obtain an MRI to localise the residual or second lesion and re-discuss the case at a hand surgery MDT. A third possibility is a wrong primary diagnosis (e.g. digital neuroma, subungual melanoma, or CRPS) - review the original histology and consider a second opinion.
Outcomes and Prognosis
- Treatment
- Marginal excision with nail bed repair
- Expected Outcome
- Greater than 90 percent immediate pain relief
- Long-term Function
- Excellent return to function, minimal nail dystrophy
- Treatment
- Direct volar marginal excision
- Expected Outcome
- Greater than 90 percent pain relief; small scar
- Long-term Function
- Good function; minor pulp dysaesthesia in some
- Treatment
- Re-excision with wider margin after MRI
- Expected Outcome
- 70-85 percent relief after re-excision
- Long-term Function
- Good function if no further recurrence
- Treatment
- Selective excision of symptomatic lesions
- Expected Outcome
- Variable; depends on number and location
- Long-term Function
- Genetic counselling; long-term surveillance
Best prognosis: a single, well-localised subungual lesion treated by an experienced hand surgeon with intra-operative localisation and complete marginal excision.
Poorer prognosis: multifocal disease, incomplete first excision, misdiagnosis (e.g. neuroma, CRPS), or a transungual approach that injures the nail matrix.
Key message: most patients are cured with one well-planned operation. The single biggest predictor of a good outcome is accurate pre-operative localisation - which is why Love testing and MRI before surgery are not optional.
Guidelines, Registries & Global Practice
- Hand tumours: glomus tumours account for 1 to 5 percent of all hand tumours worldwide
- Subungual predilection: 75-80 percent of glomus tumours in the hand are subungual, with a female predominance
- Diagnostic delay: average 7 years from symptom onset to correct diagnosis, regardless of healthcare system
- Familial forms: autosomal dominant inheritance with mutations in the glomulin gene; more common in some populations
- High-resource: MRI with dedicated finger coil is the standard pre-operative localiser; Littler approach or transungual with nail bed repair under loupe magnification
- Limited-resource: clinical diagnosis (triad plus Love and Hildreth tests) with or without plain X-ray is acceptable; transungual excision is inexpensive and effective
- Universal principle: accurate pre-operative localisation (clinical, MRI or both) and complete marginal excision are the keys to cure
- Histology: essential in all healthcare settings - melanoma must be excluded
- Diagnosis emphasis
- Triad plus Love and Hildreth; MRI before surgery
- Treatment emphasis
- Marginal excision with nail bed repair; Littler approach when feasible
- Special notes
- Always send for histology to exclude melanoma
- Diagnosis emphasis
- Clinical diagnosis; MRI for surgical planning
- Treatment emphasis
- Day-case local anaesthetic excision is standard
- Special notes
- Nail bed repair with fine absorbable sutures
- Diagnosis emphasis
- Triad plus imaging (X-ray and MRI)
- Treatment emphasis
- Transungual or subungual approach depending on location
- Special notes
- Wide excision discouraged - marginal is curative
- Diagnosis emphasis
- Triad, bedside tests and ultrasound in resource-limited settings
- Treatment emphasis
- Transungual excision with nail bed repair
- Special notes
- Emphasis on high index of suspicion to reduce delay
There is no dedicated registry for glomus tumours (unlike arthroplasty registries) because the lesion is benign, treated by a small day-case operation, and typically cured. The evidence base is dominated by retrospective surgical series and operative-technique descriptions rather than randomised trials, so guidance is principle-based: recognise the classic triad, perform Love and Hildreth tests, obtain MRI for surgical planning, and excise the lesion completely with a marginal cuff.
Record in every suspected subungual lesion:
- Triad features (paroxysmal pain, pinpoint tenderness, cold sensitivity) - present or absent
- Love test result and Hildreth test result
- Pre-operative MRI findings (location, size, satellites)
- Surgical approach and margin taken
- Histology result and confirmation of complete excision
A missed glomus tumour - particularly one misdiagnosed as CRPS, neuroma or psychiatric pain - is a recurring source of patient dissatisfaction and medico-legal complaint. Always perform and document Love and Hildreth tests on any focal subungual or pulp pain.
Controversies & Areas of Uncertainty
The transungual approach (with partial or total nail avulsion) gives direct midline access but carries a higher risk of nail dystrophy. The Littler lateral subungual approach preserves the nail plate and is associated with less dystrophy, but offers more limited exposure. There is no high-quality comparative trial; choice is dictated by lesion location and surgeon preference.
The classic triad plus positive Love and Hildreth tests is highly specific, and some surgeons proceed to surgery without MRI. However, MRI detects occult satellite lesions and guides the approach. In recurrent cases, MRI is mandatory. The balance between cost and added value remains debated.
Multifocal disease carries a higher risk of recurrence. There is no consensus on the timing of excision of asymptomatic lesions, the value of genetic testing, or surveillance protocols. Selective excision of symptomatic lesions, with genetic counselling, is the current pragmatic approach.
A small number of patients have persistent pain despite complete excision and benign histology. Causes include digital nerve neuroma, scar neuroma, complex regional pain syndrome, or a missed satellite. MDT discussion, diagnostic nerve block, and pain-clinic input are useful; further surgery without a clear target is rarely helpful.
MCQ Practice Points
Q: From which structure does a glomus tumour arise? A: The modified smooth muscle cells of the Sucquet-Hoyer canal, a specialised arteriovenous anastomosis in the reticular dermis. The glomus body is concentrated in the subungual region and fingertip pulp, where it functions in thermoregulation. Tumour cells are positive for smooth muscle actin and negative for S100, which helps distinguish glomus tumour from melanoma and neurofibroma.
Q: What is the classic triad of a glomus tumour? A: Paroxysmal pain + pinpoint tenderness + cold sensitivity. The Love test (pinhead pressure) reproduces the pain, and the Hildreth test (tourniquet exsanguination) abolishes it. When all three features of the triad are present, the diagnosis is essentially clinical, although MRI is used to localise the lesion before surgery.
Q: What is the most useful imaging modality for a suspected glomus tumour? A: MRI with a dedicated surface finger coil and gadolinium enhancement. The lesion appears as a well-circumscribed, T2 hyperintense, strongly enhancing nodule. Plain X-ray may show scalloped erosion of the dorsal cortex of the distal phalanx, but is frequently normal. High-resolution ultrasound can also identify the lesion but is operator dependent.
Q: What is the appropriate surgical margin for a glomus tumour? A: Marginal excision with a 1-2 mm cuff of normal tissue. Wide excision is unnecessary for this benign lesion and risks unnecessary damage to the nail bed and matrix. Histology is mandatory to confirm the diagnosis and exclude melanoma.
Q: A patient has recurrent pain at the same site 12 months after glomus excision. What is the most likely cause? A: Incomplete primary excision or a missed satellite lesion. Obtain an MRI to localise residual disease, re-review the original histology, and offer re-excision with a wider margin. A small number of patients will have a wrong primary diagnosis (e.g. neuroma, CRPS) - re-review of histology and targeted nerve block can clarify.
Q: What is the most important diagnosis not to miss in a subungual lesion? A: Subungual melanoma. Any pigmented streak, non-healing ulcer or atypical subungual lesion must be biopsied and sent for histology. Glomus tumour and melanoma can occasionally coexist, and the absence of pain does not exclude melanoma. When in doubt, biopsy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old woman presents with a 4-year history of severe episodic pain in the right little fingertip. The pain is sharp, paroxysmal, triggered by cold weather and by bumping the fingertip. She has seen two hand surgeons, a neurologist and a pain specialist. She has been trialled on gabapentin, amitriptyline and a stellate ganglion block without benefit. On examination, the nail plate of the little finger shows a faint blue-red spot under the lateral edge, with a subtle longitudinal ridge. Plain X-ray is reported as normal. How would you proceed?”
“A 46-year-old man had a subungual glomus tumour of the right ring finger excised 18 months ago through a transungual approach. The histology confirmed a glomus tumour and he was pain-free for about 9 months. He now returns with identical pain at the same site. The previous surgeon told him the excision was complete. Examination shows a healed nail bed scar with a small bluish spot at its radial edge, and Love test is strongly positive at that spot. How would you manage this?”
Key Anatomy
- Glomus body = specialised arteriovenous anastomosis (Sucquet-Hoyer canal) for thermoregulation
- Tumour arises from modified smooth muscle cells of the glomus body
- Tumour cells are SMA positive and S100 negative (distinguishes from melanoma and neurofibroma)
- Most concentrated in subungual region and fingertip pulp
Classic Triad and Clinical Features
- Classic triad: paroxysmal pain + pinpoint tenderness + cold sensitivity
- Average diagnostic delay of 7 years - high index of suspicion is essential
- Subungual blue-red spot and nail ridging are characteristic
- Female predominance, peak age 30-50 years, 75-80 percent subungual
Bedside Tests
- Love test: pinhead pressure with a paper clip or pencil reproduces the pain
- Hildreth test: exsanguination with a finger tourniquet abolishes the pain
- Cold test: ice cube on the digit reproduces the pain (less specific)
- Transillumination: small reddish nodule visible under the nail
Investigations
- Plain X-ray: PA and lateral - look for scalloped erosion of the distal phalanx dorsal cortex
- MRI with a dedicated finger coil and gadolinium: T2 hyperintense, enhancing nodule
- High-resolution ultrasound: hypoechoic, hypervascular subungual nodule (operator dependent)
- Histology: always send the specimen to confirm glomus tumour and exclude melanoma
Treatment Algorithm
- Marginal (not wide) excision with a 1-2 mm cuff of normal tissue
- Transungual approach for central subungual lesions; Littler lateral subungual approach for eccentric lesions
- Pulp lesions: direct volar marginal excision with nerve preservation
- Nail bed repair with 6-0 or 7-0 absorbable sutures under loupe magnification; replace nail plate as a physiological splint
Outcomes and Complications
- Cure rate greater than 90 percent with complete marginal excision
- Recurrence 10-20 percent - usually incomplete excision or missed satellite
- Nail dystrophy in up to 20 percent of subungual excisions
- Re-excision with wider margin after MRI for recurrent disease
Differential Diagnosis
- Subungual melanoma: pigmented streak, Hutchinson sign, biopsy mandatory
- Subungual exostosis: bony outgrowth, X-ray diagnostic
- Mucoid (myxoid) cyst: dorsal DIP, ganglion-like, often with osteophyte
- Digital neuroma, Raynaud, CRPS: ruled out by bedside tests and MRI
Evidence Base and Key Trials
Glomus tumors of the hand: review of the literature and report of 28 cases
- Classic surgical-pathology series defining the clinical features of glomus tumours of the hand
- Confirms the triad of paroxysmal pain, pinpoint tenderness and cold sensitivity
- Subungual location in the majority of cases; subungual lesions often show bony erosion of the distal phalanx on X-ray
- Marginal surgical excision is curative in the great majority of cases
The ischaemic test for glomus tumour: a new diagnostic test
- Describes the ischaemic (Hildreth) test: a digital tourniquet is applied after exsanguination of the digit
- Positive test is abolition of the pain and of the ability to localise the lesion while the digit is exsanguinated
- Reports high specificity in differentiating glomus tumour from other causes of fingertip pain
Outcomes of the Transungual Approach in 56 Consecutive Digital Subungual Glomus Tumours
- Large consecutive series of 56 subungual glomus tumours treated by transungual excision with excellent pain relief and low recurrence
The 'shark mouth' flap approach for digital glomus tumours in 24 patients: technique and clinical outcomes
- Describes a novel shark mouth flap approach for digital glomus tumours with good clinical outcomes in 24 patients