Growth disturbance of the volar-ulnar distal radial physis | Tethered by Vickers ligament | Linked to Leri-Weill dyschondrosteosis and SHOX defects | Bilateral, female, adolescent
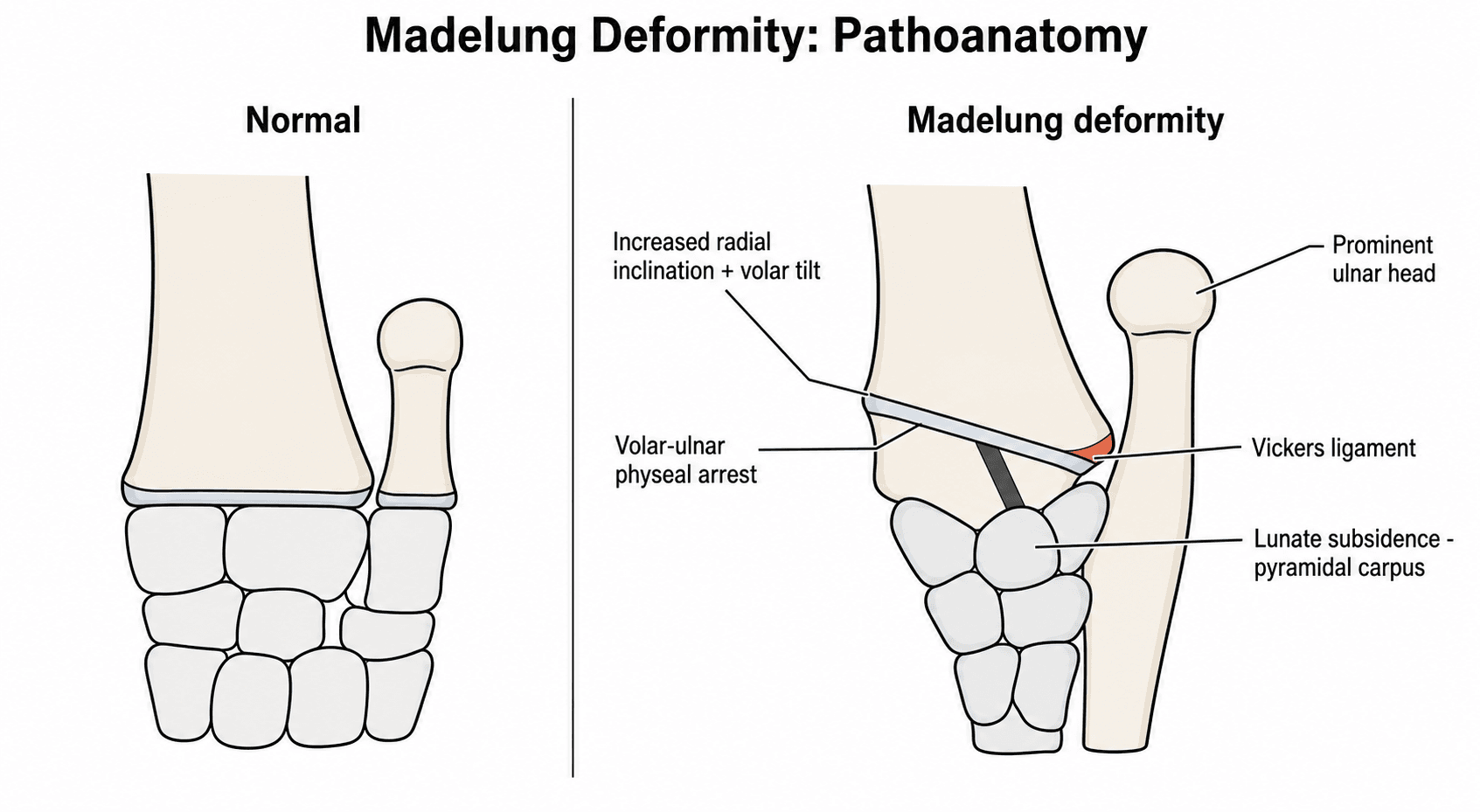
- Core lesion: a partial growth arrest of the volar and ulnar corner of the distal radial physis, so the radius keeps growing on its dorsal-radial side but not its volar-ulnar side - this twists the joint surface and lets the carpus slide volar and ulnar
- Vickers ligament: an abnormal thick band running from the volar distal radius to the lunate. It tethers the volar physis and is the structure released at surgery
- Who gets it: typically an adolescent girl with bilateral wrists, presenting with deformity, a prominent ulnar head, pain, and loss of forearm rotation and wrist extension
- The big association: Leri-Weill dyschondrosteosis (a mesomelic short-stature dwarfism) caused by SHOX gene defects - but many cases are idiopathic, post-traumatic, post-infective, or part of other dysplasias
- Treatment depends on skeletal maturity: in the growing child, release Vickers ligament and free the radial physis (physiolysis) to slow progression; in the mature, symptomatic wrist, a dome osteotomy of the radius corrects the deformity, and severe joint damage may need a salvage procedure
- “Madelung deformity is the classic exam wrist that is bilateral, female, adolescent and associated with short stature - say all four
- “The deforming tether is Vickers ligament running from the volar radius to the lunate; releasing it is the key growth-modulating step in children
- “Think SHOX and Leri-Weill dyschondrosteosis, but remember Madelung-like deformity can also follow trauma, infection, or other skeletal dysplasias (the reverse Madelung points the other way)
- “Match the operation to the skeleton: physiolysis and ligament release while growing; osteotomy once mature
A partial growth arrest of the volar-ulnar distal radial physis, tethered by an abnormal Vickers ligament (volar radius to lunate). The radius tilts in the coronal and sagittal planes, the carpus slides volar and ulnar, and the ulna looks relatively long and prominent. Classic patient: adolescent girl, bilateral wrists, short stature.
The headline association is Leri-Weill dyschondrosteosis, a mesomelic short-stature dwarfism caused by SHOX gene defects. But do not say all Madelung deformity is genetic - it can also be idiopathic, post-traumatic, post-infective, or part of other dysplasias (for example multiple hereditary exostoses, Turner syndrome).
In the growing child: release the Vickers ligament and free the radial physis (physiolysis), sometimes with an ulnar epiphysiodesis, to slow progression. In the skeletally mature, symptomatic wrist: a dome osteotomy of the distal radius corrects all three planes; severe joint destruction may need a salvage procedure (for example ulnar shortening, distal-radioulnar-joint reconstruction, or arthrodesis).
Madelung deformity is the wrist condition. Madelung disease (benign symmetric lipomatosis) is a completely different fatty-neck condition - same surname, unrelated. A reverse Madelung deformity tilts the radius the opposite way (dorsal, not volar).
Overview
Madelung deformity is a developmental abnormality of the wrist in which the distal radius grows in the wrong shape because part of its growth plate stops working. It is named after Otto Madelung, who described it in the 19th century. The typical patient is an adolescent girl who develops a bent-looking wrist with a prominent bump on the little-finger side (the ulnar head), often in both wrists, with pain and reduced movement.
The simplest way to understand it is to think of the distal radius growth plate as having a corner that fails. The volar (palmar) and ulnar corner of the physis stops growing, while the rest of the radius carries on. The result is a joint surface that tilts towards the ulna and towards the palm, a carpus that slides into the gap that forms, and an ulna that ends up looking too long because the radius has shortened on that side. Running across the front of the failing physis is an abnormal thick band, the Vickers ligament, which tethers the lunate to the volar radius and is central to both the pathology and the surgery.
For the exam, Madelung deformity is a favourite because it links genetics (the SHOX gene and Leri-Weill dyschondrosteosis), growth-plate biology, three-dimensional deformity, and a maturity-dependent treatment decision. Get the classic picture, the Vickers ligament, and the growing-versus-mature treatment split, and you have answered most of what an examiner will ask.
Anatomy and Pathophysiology
The distal radius normally grows from a physis (growth plate) that contributes most of the length of the radius. In Madelung deformity, the volar-ulnar part of this physis is abnormal and arrests early, while the dorsal-radial part keeps growing. This asymmetric growth twists the distal radius:
- In the coronal plane, the joint surface tilts so its ulnar side is lower - this is increased radial inclination, and it points the carpus towards the ulna.
- In the sagittal plane, the joint surface tilts towards the palm - increased volar (palmar) tilt - so the carpus and lunate are carried forwards (palmar carpal displacement).
- Because the radius shortens on the affected side while the ulna grows normally, the ulna becomes relatively long and its head sits prominent and often dorsal at the wrist.
The carpus adapts to this distorted radius. The lunate sinks into the notch that forms between the tilted radius and the ulna (lunate subsidence), and the proximal carpal row takes on a wedge or pyramid/triangle shape pointing proximally - a classic descriptive sign on the X-ray.
The Vickers ligament is the abnormal structure at the centre of it all. According to PubMed, histopathological study of patients with Leri-Weill dyschondrosteosis and a confirmed SHOX abnormality showed widespread disorganisation of the radial growth plate - the normally neat parallel columns of cartilage cells are disrupted - and confirmed that the Vickers ligament blends with the triangular fibrocartilage complex (TFCC) (Munns et al., Hand Surg 2001, DOI). This abnormal volar tether is thought to bowstring across the volar physis, both reflecting and reinforcing the local growth disturbance.
The core sentence to memorise: "Madelung deformity is a partial arrest of the volar-ulnar distal radial physis, tethered by an abnormal Vickers ligament running from the volar radius to the lunate, producing increased radial inclination, increased volar tilt, lunate subsidence, and a relatively prominent ulna."
Aetiology and Genetics
Not all Madelung deformity has the same cause. It is useful to split it into a genetic/dysplastic group, where the physis is intrinsically abnormal, and an acquired group, where something damages a previously normal physis.
- Examples
- SHOX gene defect (deletion or mutation), mesomelic short stature
- Key point
- The classic association; bilateral, female predominant, true Vickers ligament
- Examples
- Turner syndrome, multiple hereditary exostoses, other skeletal dysplasias
- Key point
- Madelung-like deformity as part of a wider skeletal picture
- Examples
- Physeal injury to the volar-ulnar distal radius
- Key point
- Post-traumatic arrest mimics the genetic shape
- Examples
- Osteomyelitis affecting the physis, prior radiation
- Key point
- Damaged physis behaves like an arrest
- Examples
- No identifiable cause or syndrome
- Key point
- Common - do not assume every case is genetic
The SHOX gene (short-stature homeobox gene) sits in the pseudoautosomal region at the tip of the X and Y chromosomes. Losing one working copy (haploinsufficiency) causes Leri-Weill dyschondrosteosis, a mesomelic (middle-segment) short-stature dwarfism in which Madelung deformity is the most characteristic limb feature. According to PubMed, SHOX haploinsufficiency accounts for around 80% of genetic causes of Leri-Weill dyschondrosteosis, and SHOX-deficient bone shows a disrupted columnar growth plate with an expanded hypertrophic layer and altered programmed cell death of the cartilage cells - the cellular basis of the deformity (Seki et al., Clin Pediatr Endocrinol 2014, DOI).
If the examiner shows a short adolescent girl with bilateral Madelung wrists, link it to SHOX and Leri-Weill dyschondrosteosis and mention that you would consider endocrine/genetic referral. But add the caveat that Madelung-like deformity can also be acquired (trauma, infection) or part of other dysplasias - this shows you are not pattern-matching blindly.
SHOX Genetics: Inheritance and the Disease Spectrum
The SHOX association is worth understanding in more depth than just "SHOX causes Leri-Weill," because examiners like the gene-dose spectrum and the inheritance pattern.
Where the gene sits and how it behaves:
- SHOX (short-stature homeobox) lies in the pseudoautosomal region (PAR1) at the tips of the X and Y chromosomes, so it escapes X-inactivation and is normally present as two active copies in everyone.
- Because both copies are normally active, it behaves in a pseudoautosomal dominant fashion - losing one working copy (haploinsufficiency) is enough to cause disease, with variable penetrance and a tendency for Madelung deformity to be more frequent and more marked in females.
The gene-dose spectrum (high-yield):
- Condition
- Leri-Weill dyschondrosteosis
- Phenotype
- Mesomelic short stature plus Madelung deformity - the classic association
- Condition
- Langer mesomelic dysplasia
- Phenotype
- Severe mesomelic AND rhizomelic dwarfism - the most severe end of the spectrum
- Condition
- Turner syndrome
- Phenotype
- Short stature and an increased incidence of Madelung deformity, among the other features
- Condition
- Isolated / idiopathic short stature
- Phenotype
- Short stature with little or no Madelung change
Why it matters clinically:
- Bilateral Madelung deformity in a short child should prompt genetic testing (SHOX deletion/duplication analysis such as MLPA, plus sequencing) and endocrine referral.
- Growth hormone is an approved treatment for the short stature of SHOX deficiency / Leri-Weill dyschondrosteosis, so an early diagnosis has a non-orthopaedic payoff.
Frame SHOX as a dose-response gene: one copy lost gives Leri-Weill dyschondrosteosis (mesomelic short stature plus Madelung), both copies lost gives Langer mesomelic dysplasia (severe dwarfism), and 45,X (Turner) loses a copy too, which is why those girls are short and prone to Madelung. It is pseudoautosomal dominant with variable, female-predominant penetrance.
Classification
There is no single universally used classification, but examiners expect you to be able to categorise by cause and to describe the deformity in a structured way. A practical scheme groups Madelung deformity by aetiology, direction, severity, and radiographic measurement:
Dysplastic / genetic (Leri-Weill dyschondrosteosis and SHOX, other dysplasias), post-traumatic, post-infective, and idiopathic. Naming the group guides whether you look for short stature, a family history, or a previous injury.
Clinical Presentation
The classic story is an adolescent girl (commonly early teens) who notices that her wrists look bent and that there is a bump on the ulnar side (the prominent ulnar head). It is frequently bilateral, and there may be a family history and short stature if there is underlying Leri-Weill dyschondrosteosis.
- Deformity and cosmetic concern - often the main reason for presenting, especially the prominent dorsal ulnar head.
- Pain - typically ulnar-sided wrist pain, worse with loading and activity, often emerging in adolescence as the deformity matures.
- Stiffness - loss of wrist extension and especially loss of forearm rotation (supination), and loss of radial deviation.
- Weakness of grip in symptomatic wrists.
- A characteristic wrist contour with the hand looking displaced towards the palm and the ulnar head prominent dorsally (the "bayonet" or step look).
- Reduced range of movement, particularly forearm rotation and wrist extension.
- The forearm may look mesomelically short (shortened middle segment) if there is dyschondrosteosis; check the other wrist and the patient's height.
Madelung deformity is a leading congenital cause of ulnar-sided wrist pain and loss of supination in an adolescent. If you are given that triad with a prominent ulnar head and bilateral involvement, Madelung deformity should be at the top of your list.
How to examine the wrist (OSCE sequence)
- Look - inspect both wrists from the front, side and above. Note the volar-tilted "bayonet" contour, the dorsally prominent ulnar head, any forearm shortening (mesomelia), and surgical scars. Always expose and compare both sides and look at the patient's overall stature.
- Feel - palpate the prominent ulnar head and the distal radioulnar joint (DRUJ) for tenderness; assess DRUJ stability (ballottement) and ulnar-sided tenderness over the TFCC.
- Move - measure active and passive wrist flexion/extension and especially forearm pronation/supination and radial deviation, which are characteristically reduced; compare with the other side. Check grip strength.
- Special tests / complete the exam - examine the DRUJ (piano-key sign), do a focused neurovascular check, then examine the rest of the child (height, limb proportions, the contralateral wrist) because bilateral disease with short stature points to Leri-Weill dyschondrosteosis.
Investigations
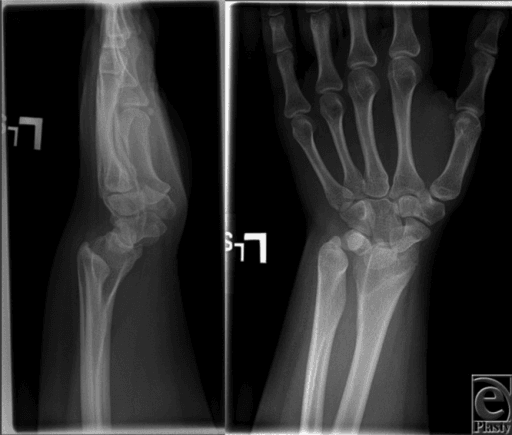
Posteroanterior and lateral wrist X-rays are the cornerstone and usually diagnostic. Look for:
- Increased radial inclination (the joint surface tilting towards the ulna).
- Increased volar tilt and palmar carpal displacement on the lateral view.
- Lunate subsidence into a V-shaped notch between radius and ulna, with the proximal carpal row taking a pyramid/triangle shape.
- A relatively long, dorsally prominent ulna and changes in the sigmoid notch.
- Bowing of the radial shaft and shortening.
Measurements such as ulnar (radial) tilt, lunate subsidence, lunate fossa angle, and palmar carpal displacement quantify the deformity and let you follow progression and judge surgical correction.
How each is measured (what an examiner may ask you to demonstrate on the film):
- Ulnar tilt (radial inclination) - on the PA view, the angle between the distal radial articular surface and a line perpendicular to the long axis of the radius. It is increased in Madelung (the joint surface slopes towards the ulna).
- Lunate subsidence - on the PA view, how far the proximal pole of the lunate has sunk proximally between the radius and ulna (it sits in the V-shaped notch), measured against the distal ulna/radius as a reference.
- Lunate fossa angle - the angulation of the lunate fossa of the distal radius, reflecting the abnormal slope of the articular surface that the carpus sits on.
- Palmar carpal displacement - on the lateral view, how far the carpus (lunate) lies volar to the long axis of the radius - the radiographic counterpart of the clinical palmar carpal shift.
There is no single agreed "abnormal" cut-off; each value is interpreted against the normal/contralateral wrist and, more usefully, tracked over time and before/after surgery to judge progression and the adequacy of correction. These same four measurements are the ones reported in the surgical literature (for example the dome-osteotomy and growth-modulation series cited below).
A bilateral Madelung deformity in a short adolescent is a clue to an underlying skeletal dysplasia. Examine the whole child (height, limb proportions, the other limbs) and have a low threshold for genetic/endocrine referral - the wrist may be the presenting sign of Leri-Weill dyschondrosteosis.
Differential Diagnosis
Madelung deformity is the classic congenital cause of a bent, ulnar-prominent adolescent wrist, but several conditions mimic it. The discriminators are laterality, sex, the presence of bony lesions, systemic features, and a trauma history.
- Discriminating feature
- Bilateral, female, short stature; volar-ulnar physeal arrest with a Vickers ligament
- Best test
- PA and lateral radiographs; MRI for the tether; SHOX testing
- Discriminating feature
- Visible osteochondromas tethering the distal ulna/radius (Masada forearm deformity); often male; lesions elsewhere; family history
- Best test
- Radiographs of the whole forearm / skeletal survey showing exostoses
- Discriminating feature
- History of distal radius trauma; usually unilateral; no systemic features
- Best test
- Radiographs; CT or MRI for a physeal bar
- Discriminating feature
- Wider skeletal or syndromic stigmata; short stature with other features
- Best test
- Skeletal survey; karyotype / genetics
- Discriminating feature
- History of distal radius osteomyelitis or sepsis; often unilateral
- Best test
- Radiographs; history and inflammatory markers
- Discriminating feature
- Radius tilts dorsally with a dorsally subluxed ulna - the opposite tilt
- Best test
- Lateral radiograph showing dorsal rather than volar carpal displacement
The single most useful discriminator is the whole-forearm radiograph: osteochondromas point to multiple hereditary exostoses (a Masada forearm deformity, not Madelung), a unilateral deformity with a physeal bar points to old trauma or infection, and a symmetric bilateral volar-ulnar physeal arrest in a short girl points to true (often SHOX-related) Madelung deformity.
Management
The single most important decision is skeletal maturity: a growing physis can be modulated, whereas an established deformity in a mature wrist can only be corrected by cutting and realigning bone. Severity and symptoms then refine the plan.
Many patients - especially those with mild, painless deformity - never need surgery. The natural history is unpredictable, so a reasonable approach is observation with serial radiographs, activity modification, analgesia, and splinting for symptom control. According to PubMed, mild asymptomatic deformity warrants a period of non-surgical management with serial X-rays because the natural history is uncertain and many patients never require surgery (Kozin and Zlotolow, J Hand Surg Am 2015, DOI).
- Typical approach
- Observation, serial X-rays, splint/analgesia
- Aim
- Avoid unnecessary surgery; many never progress
- Typical approach
- Vickers ligament release + radial physiolysis (+/- ulnar epiphysiodesis)
- Aim
- Slow progression and let remaining physis grow
- Typical approach
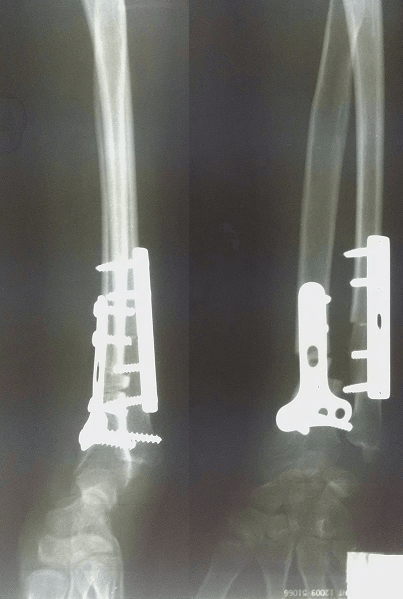
- Dome osteotomy of distal radius (+/- ulnar shortening)
- Aim
- Correct deformity, offload the ulnar wrist, restore rotation
- Typical approach
- Salvage: ulnar procedure, partial arthrodesis, DRUJ reconstruction
- Aim
- Reliable pain relief when reconstruction is not possible
The examiner wants to hear the maturity split out loud: "If she is still growing I would release the Vickers ligament and free the radial physis to modulate growth; if she is skeletally mature with a symptomatic deformity I would correct it with a dome osteotomy of the distal radius, addressing the ulna as needed." That single sentence carries most of the marks.
Complications
- Why it happens
- Ongoing asymmetric physeal growth and tethering
- Key point
- Natural history is unpredictable; serial X-rays in mild cases
- Why it happens
- Abnormal radioulnar mechanics, TFCC and DRUJ loading
- Key point
- Common indication for surgery; main complaint in adolescents
- Why it happens
- Distorted distal radioulnar joint and sigmoid notch
- Key point
- Supination and wrist extension are typically most affected
- Why it happens
- Joint incongruity and chronic abnormal loading
- Key point
- May ultimately need salvage (arthrodesis, DRUJ reconstruction)
- Why it happens
- Growth modulation does not fully normalise the physis
- Key point
- Long-term studies show further surgery may be needed after growth
- Why it happens
- Nonunion, malunion, hardware irritation, neurovascular risk
- Key point
- Standard risks of distal radius corrective osteotomy
Clinical Relevance
Madelung deformity sits at the crossroads of paediatric hand surgery, genetics, and growth-plate biology, which is exactly why it is a recurring exam topic. It teaches the principle that a physeal growth disturbance produces a predictable three-dimensional bony deformity, and that timing surgery to skeletal maturity changes the whole strategy - growth modulation while the physis is open, correction once it is closed. It also rewards the candidate who looks beyond the wrist: recognising the link with SHOX and Leri-Weill dyschondrosteosis turns an isolated wrist problem into a diagnosis that may need genetic and endocrine input. In practice, the everyday skills it tests - reading the deformity on plain films, deciding who needs surgery, and choosing between ligament release, physiolysis, osteotomy, and salvage - are the same judgements that come up across deformity correction in the upper limb.
Guidelines, Registries and Global Practice
- No high-level guideline or registry governs Madelung deformity - it is rare, so the evidence base is case series (level IV) and a systematic review of them, and practice is guided by paediatric hand surgery experience rather than randomised trials.
- Consistent global principle: treat symptoms and progression, not the X-ray alone. Mild, painless deformity is observed with serial radiographs everywhere; surgery is reserved for pain, functional loss, or progressive deformity.
- Maturity-based strategy is universal: growth modulation (Vickers ligament release with radial physiolysis, sometimes ulnar epiphysiodesis) in the skeletally immature wrist, and corrective osteotomy (commonly a distal radial dome osteotomy, with ulnar-sided procedures as needed) once mature. Salvage arthrodesis is reserved for severely damaged joints.
- Multidisciplinary input: because of the strong link with SHOX-related Leri-Weill dyschondrosteosis, bilateral disease in a short child prompts genetic and endocrine assessment in addition to orthopaedic care - a point valued internationally.
Memory aids
MADELUNGThe Classic Patient and Lesion
Hook:Spell MADELUNG and you have the whole clinical picture: a short adolescent girl with a tethered, arrested distal radius and a prominent ulna in both wrists.
RIVThree Planes of Deformity
Hook:RIV - Radial inclination up, Inclined volar, Vickers tether - the three things every Madelung X-ray and viva answer needs.
GROWChoosing the Operation
Hook:GROW: while the child can still GROW you modulate growth; once growth is over you osteotomise; if the joint is wrecked you salvage.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old girl is referred with deformity of both wrists and a prominent bump on the little-finger side. She is short for her age. The examiner asks for your diagnosis and assessment.”
“Two patients have symptomatic Madelung deformity: a 10-year-old with open physes and a 19-year-old who is skeletally mature. The examiner asks how your surgical plan differs and why.”
The Core Lesion
- Partial arrest of the volar-ulnar distal radial physis
- Abnormal Vickers ligament tethers volar radius to lunate
- Increased radial inclination + volar tilt + palmar carpal displacement
- Lunate subsidence, pyramid carpus, relatively long prominent ulna
Classic Patient and Association
- Adolescent girl, bilateral wrists, short stature
- Leri-Weill dyschondrosteosis from SHOX gene defects
- But also post-traumatic, post-infective, idiopathic, other dysplasias
- Presents with ulnar-sided pain and loss of supination/extension
Investigations
- PA + lateral wrist X-rays - usually diagnostic
- Measure radial tilt, lunate subsidence, palmar carpal displacement
- MRI to show Vickers ligament and plan; CT/3D for osteotomy planning
- Genetic/endocrine referral if syndromic (SHOX testing)
Treatment by Maturity
- Mild/painless: observe with serial X-rays, splint, analgesia
- Growing child: Vickers release + physiolysis (+/- ulnar epiphysiodesis)
- Mature wrist: dome osteotomy of distal radius (+/- ulnar shortening)
- Destroyed joint: salvage (partial arthrodesis, DRUJ reconstruction)
Evidence
According to PubMed, the following studies support the modern, maturity-dependent approach to Madelung deformity.
Surgical Management of Madelung Deformity: A Systematic Review
- Systematic review of 25 studies (all case series, level IV evidence) describing surgery for Madelung deformity
- The main indication for surgery was wrist pain, not deformity alone
- Procedures fall into radial lengthening/correction, ulnar shortening, or a combination of both
- All studies reported postoperative pain reduction and most reported improved range of motion, but inconsistent outcome reporting prevented pooling of results
Long-Term Outcomes After Vickers Ligament Release and Growth Modulation
- Six skeletally immature patients (8 wrists) with symptomatic Madelung deformity treated by Vickers ligament release and distal radial physiolysis, median follow-up 10.6 years
- Pain relief was durable - 6 of 8 wrists were completely pain-free at final follow-up
- Range of motion was preserved compared with before surgery
- Lunate subsidence still progressed over time and 2 of 6 patients needed a later procedure (one radial dome osteotomy, one ulnar shortening osteotomy)
Dome Osteotomy with Vickers Ligament Section in Children: Esthetic and Functional Outcomes
- Retrospective series of 6 wrists treated with distal radial dome osteotomy plus Vickers ligament section
- Radiographic correction achieved across ulnar tilt, lunate subsidence, lunate fossa angle, and palmar carpal displacement
- Good postoperative motion preserved in flexion, extension, pronation, and supination
- Low residual pain and disability (median DASH 0), with high patient satisfaction
Radioscapholunate Arthrodesis with a Neo-DRUJ as a Salvage Option
- Six wrists with a severely abnormal sigmoid notch treated by radioscapholunate arthrodesis with construction of a neo-distal radioulnar joint, compared with 7 reverse wedge osteotomies
- No difference in postoperative pain, grip strength, or most range of motion between the two salvage approaches
- Quality of life and Michigan Hand Outcomes Questionnaire scores were similar between groups
- Extension was reduced after the arthrodesis-with-neo-DRUJ procedure