Ligament | alignment | reducibility | cartilage | demand
- Pain is not instability. Link symptoms to ligament injury, carpal alignment, reducibility and cartilage status.
- Scapholunate injury tends to DISI. The scaphoid flexes; the lunate follows the triquetrum into extension.
- Lunotriquetral injury may produce VISI, but isolated LT instability is less common than combined ulnar-sided or midcarpal pathology.
- Neutral radiographs can be normal. Stress views, dynamic fluoroscopy, MRI arthrogram and arthroscopy may be needed.
- A chronic arthritic wrist is not a repair problem. It is a salvage procedure discussion.
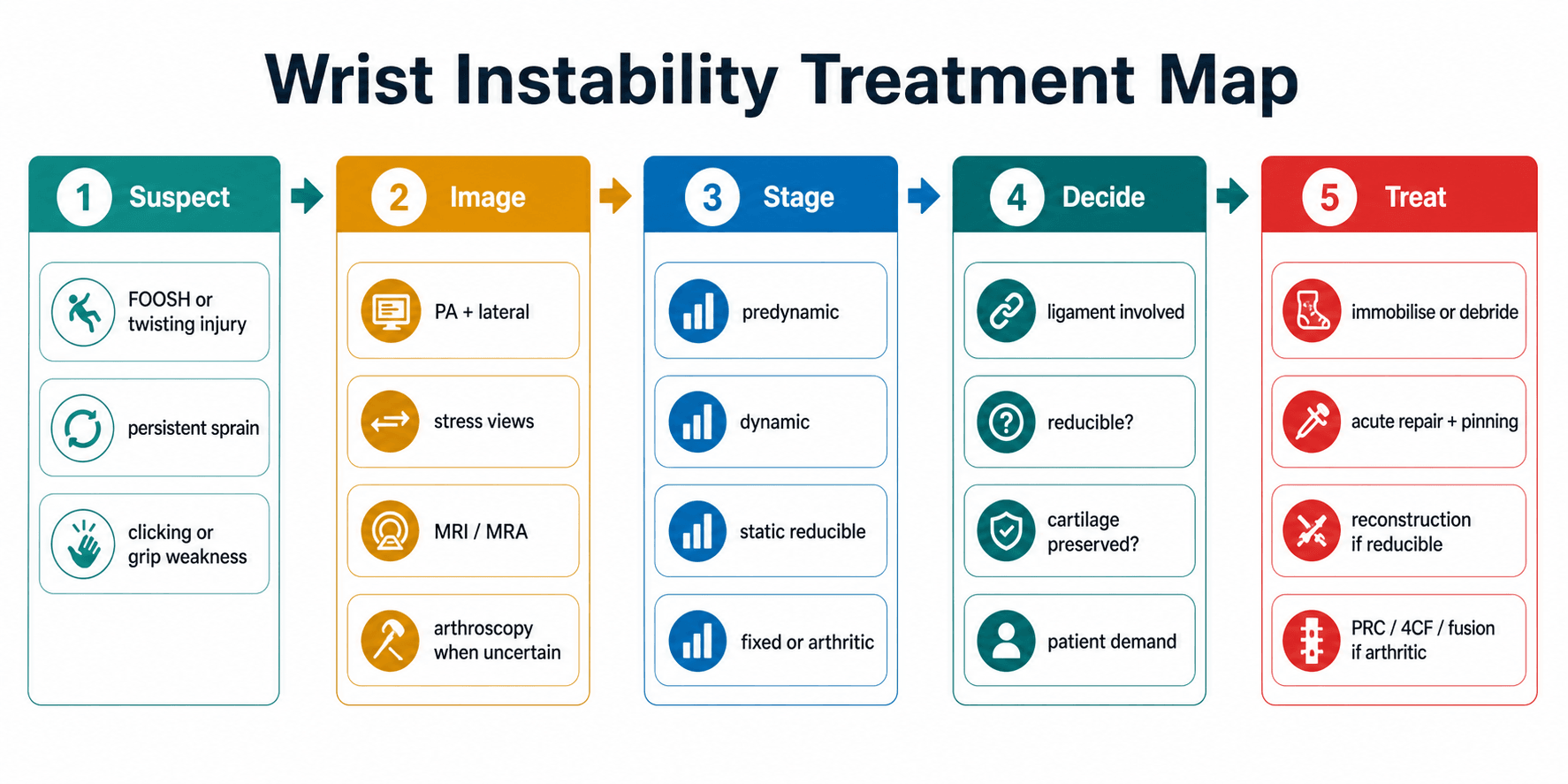
- “The safe answer starts with stage: predynamic, dynamic, static reducible, static irreducible or arthritic.
- “Every management plan must state timing, reducibility, cartilage and patient demand.
- “Watson and LT ballottement tests are screening tests; they do not replace imaging and arthroscopy.
- “SLAC progression is the late consequence of untreated chronic scapholunate dissociation.
A widened scapholunate interval, painful Watson test or VISI posture is not enough to choose an operation. Treatment depends on the ligament injured, timing, reducibility, cartilage status, associated fracture, ulnar-sided pathology and patient demand.
- What You Need To Know
- SL, LT, extrinsic ligament, TFCC, midcarpal or combined injury.
- Why It Changes Treatment
- Determines whether the main pattern is DISI, VISI, ulnar-sided instability or mixed instability.
- What You Need To Know
- Normal neutral films versus stress gap or fixed malalignment.
- Why It Changes Treatment
- Dynamic injury can be missed; static injury needs reducibility and cartilage assessment.
- What You Need To Know
- Repairable ligament tissue versus attenuated scar.
- Why It Changes Treatment
- Acute repair differs from chronic reconstruction or salvage.
- What You Need To Know
- Alignment corrects under fluoroscopy, traction or arthroscopy.
- Why It Changes Treatment
- Reducible deformity can be reconstructed; irreducible deformity often needs salvage.
- What You Need To Know
- Radioscaphoid, capitolunate, radiolunate and midcarpal cartilage.
- Why It Changes Treatment
- Cartilage loss makes ligament reconstruction inappropriate.
GATEAssessment | FLEXScapholunate | RACETreatment Choice |
|---|---|---|
G Gap Measure SL or LT interval on neutral and stress views. | F Flexed scaphoid Scaphoid flexion gives ring sign and SL gap. | R Reducible Can carpal alignment be restored? |
A Alignment Assess DISI, VISI, carpal height and capitolunate axis. | L Lunate extends DISI posture develops with dorsal lunate tilt. | A Arthritis Is there SLAC, SNAC or radiocarpal cartilage loss? |
T Timing Acute, subacute, chronic or arthritic. | E Early repair Best before chronic attenuation and arthritis. | C Chronicity Acute repair differs from chronic reconstruction. |
E End-stage Irreducible or arthritic wrists need salvage logic. | X X-ray stress Dynamic injury may need clenched-fist or stress views. | E Expectation Age, demand and occupation change the operation. |
GATE decides whether the wrist is reconstructable. | Scaphoid flexion plus lunate extension creates DISI. | Race through stage before choosing treatment. |
Overview and Epidemiology
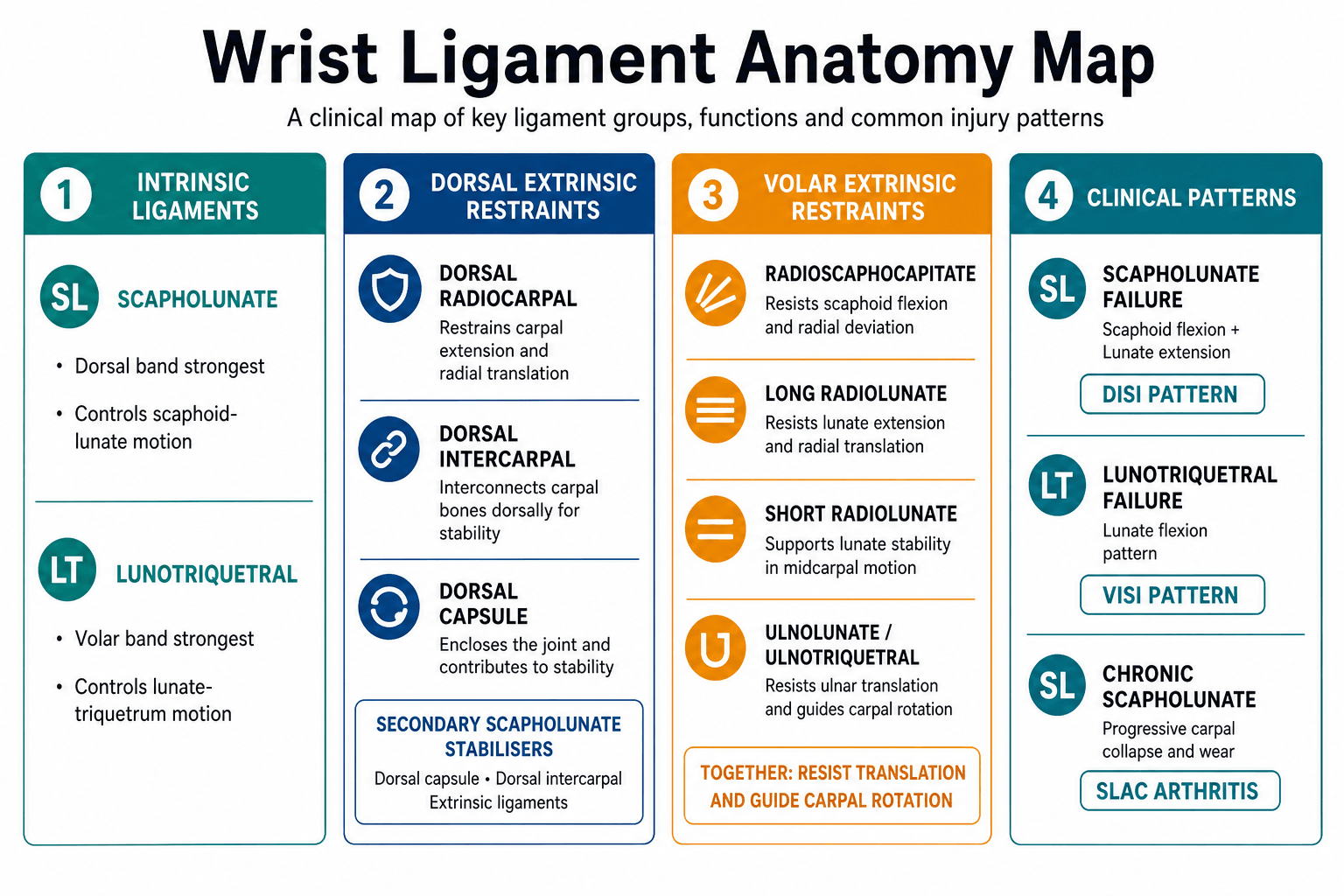
Wrist ligament instability is failure of the soft-tissue stabilisers that keep the carpal bones aligned during load and motion. The most important intrinsic ligament injuries are scapholunate and lunotriquetral injuries, but a competent assessment must also consider the dorsal intercarpal ligament, dorsal radiocarpal ligament, volar radiocarpal ligaments, TFCC, distal radius alignment, scaphoid fracture or nonunion, distal radioulnar joint pathology and midcarpal instability.
The typical patient presents after a fall on the outstretched hand, a twisting injury, high-energy trauma, sports injury, or persistent symptoms after a wrist sprain. Symptoms may be dorsal wrist pain, ulnar-sided pain, clicking, clunking, grip weakness, push-up pain, reduced load tolerance, or late degenerative collapse. The injury is commonly missed because early radiographs may be normal and because symptoms can be attributed to a nonspecific sprain.
The core management question is not "is there a tear?" The surgeon must decide whether the wrist is stable, dynamically unstable, statically malaligned, reducible, irreducible or arthritic. That staging determines whether the answer is observation, immobilisation, arthroscopic debridement, direct repair, pinning, capsulodesis, ligament reconstruction, limited fusion, proximal row carpectomy or wrist fusion.
Pathophysiology
The proximal carpal row has no direct tendon insertions. It behaves as an intercalated segment between the radius and distal carpal row. Stability depends on carpal bone geometry, intrinsic ligaments, extrinsic ligaments, capsule and coordinated load transfer.
Causes and injury mechanisms
- Typical Injury Pattern
- Hyperextension, ulnar deviation and intercarpal supination load can tear the SL ligament or progress into a perilunate spectrum injury.
- Clinical Consequence
- Dorsal radial wrist pain, SL tenderness, dynamic widening or acute static dissociation.
- Typical Injury Pattern
- Perilunate fracture-dislocation, trans-scaphoid pattern, capitate fracture, distal radius fracture or combined intrinsic ligament injury.
- Clinical Consequence
- Do not stop at the ligament label; search for fracture, median nerve symptoms and carpal malalignment.
- Typical Injury Pattern
- Partial SL, LT, TFCC or midcarpal injury, often with normal initial radiographs.
- Clinical Consequence
- Persistent pain, clunking and load intolerance need stress views or arthroscopic staging.
- Typical Injury Pattern
- Distal radius malunion, scaphoid nonunion or carpal collapse changes load transfer.
- Clinical Consequence
- Instability may be secondary; treatment may require correction or salvage rather than isolated ligament repair.
- Typical Injury Pattern
- Capsuloligamentous attenuation and cartilage loss.
- Clinical Consequence
- Pain may come from arthritis rather than repairable instability.
Surgically relevant ligament anatomy
- Main Role
- Strongest SL component; resists abnormal scaphoid-lunate separation and rotation.
- Why It Matters
- Repair target in acute SL injuries; poor tissue quality pushes treatment toward reconstruction.
- Main Role
- Contribute to restraint but are weaker than the dorsal band.
- Why It Matters
- MRI signal in these regions must be correlated with instability, not treated in isolation.
- Main Role
- Secondary stabiliser that helps restrain scaphoid flexion and links the dorsal carpus.
- Why It Matters
- Used or tensioned in capsulodesis and tenodesis concepts for chronic reducible SL instability.
- Main Role
- Dorsal extrinsic restraint to proximal-row malrotation and carpal translation.
- Why It Matters
- Secondary stabiliser; injury or attenuation worsens chronic instability.
- Main Role
- Volar restraint and sling supporting the scaphoid waist region.
- Why It Matters
- Preserve volar ligaments during salvage such as PRC; disruption can destabilise the remaining wrist.
- Main Role
- Volar restraints stabilising the lunate against translation and excessive rotation.
- Why It Matters
- Radiolunate cartilage and stability decide whether motion-preserving salvage is possible.
- Main Role
- Volar band is usually the strongest LT component; controls lunate-triquetrum motion.
- Why It Matters
- Complete LT failure may produce VISI or painful ulnar-sided instability, but isolated LT disease is uncommon.
- Main Role
- Stabilise the ulnar wrist and distal radioulnar joint.
- Why It Matters
- LT symptoms overlap with TFCC, ECU and ulnar impaction; missing these leads to wrong surgery.
Scapholunate instability
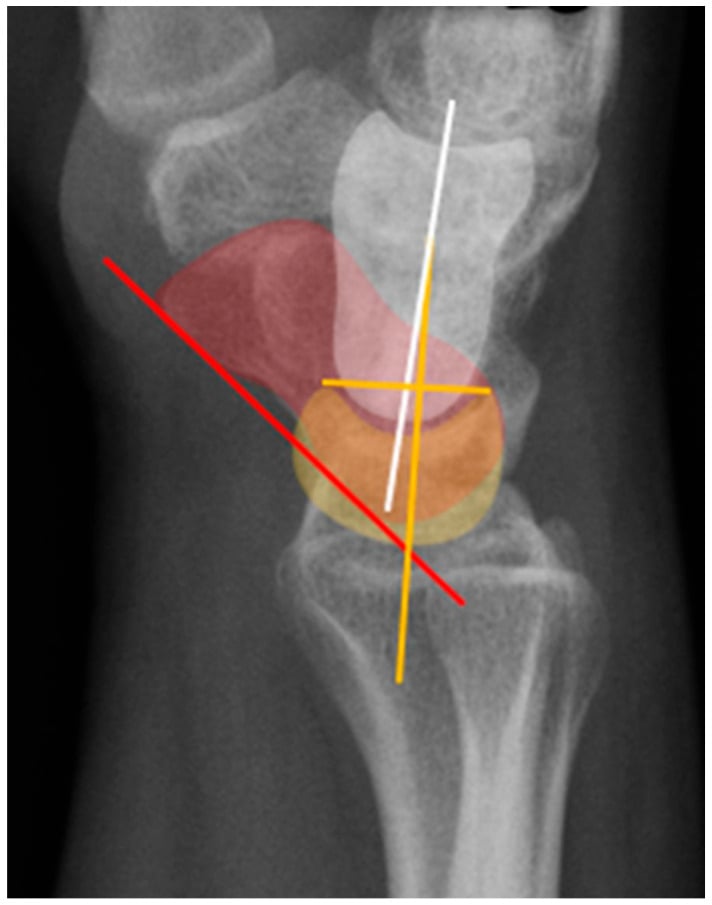
The scapholunate interosseous ligament has dorsal, proximal membranous and volar portions. The dorsal portion is the strongest and most important restraint to abnormal scaphoid-lunate motion. When the scapholunate ligament fails, the scaphoid tends to flex and pronate, while the lunate remains linked to the triquetrum and extends. The result may be a dorsal intercalated segment instability pattern.
Important associated stabilisers include the dorsal intercarpal ligament, dorsal radiocarpal ligament, radioscaphocapitate ligament and scaphotrapeziotrapezoid stabilisers. Chronic instability is therefore not simply a torn SL ligament; it is progressive failure of a stabilising complex.
Lunotriquetral instability
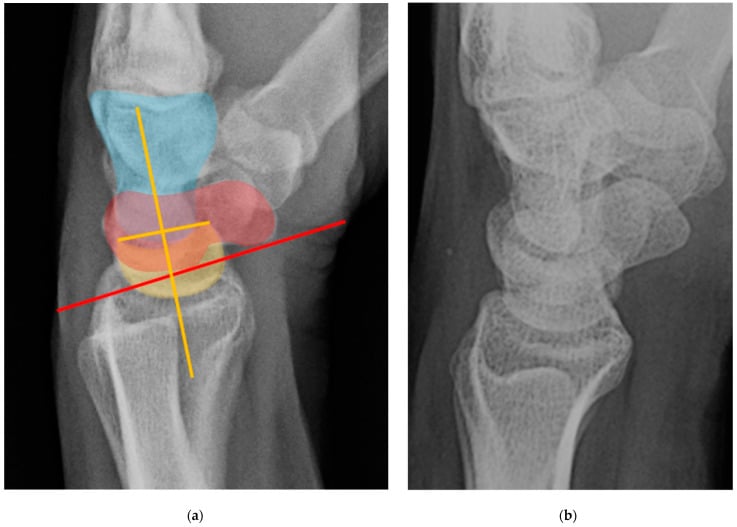
The lunotriquetral interosseous ligament has dorsal, proximal and volar components. The volar portion is usually the strongest. LT instability can produce ulnar-sided pain, painful clicking and sometimes volar intercalated segment instability. Isolated LT instability is less common than scapholunate instability and must be separated from TFCC injury, ulnar impaction, ECU pathology and midcarpal instability.
Degenerative collapse
Chronic scapholunate dissociation changes carpal load. The usual late pattern is scapholunate advanced collapse: radioscaphoid arthritis begins first, then scaphocapitate and capitolunate degeneration may follow while the radiolunate joint is often preserved until late. Once cartilage is lost, ligament reconstruction cannot restore a durable painless wrist.
SL and LT ligaments connect proximal-row bones. They control the immediate relationship between scaphoid, lunate and triquetrum.
Dorsal and volar extrinsic ligaments become increasingly important in chronic instability and reconstruction planning.
Chronic malalignment overloads cartilage. Once arthritis develops, treatment shifts from ligament reconstruction to salvage.
Classification
- Definition
- Partial or complete ligament injury without radiographic instability.
- Typical Findings
- Pain, tenderness, normal PA/lateral and stress views; arthroscopy may show tear.
- Treatment Direction
- Immobilisation, therapy, arthroscopic debridement or pinning in selected symptomatic tears.
- Definition
- Instability appears only under load or stress.
- Typical Findings
- Clenched-fist SL widening, dynamic fluoroscopy abnormality, normal resting alignment.
- Treatment Direction
- Repair or reconstruction if symptomatic, high-demand and repairable.
- Definition
- Gap or malalignment visible on resting films but correctable.
- Typical Findings
- SL gap, DISI or VISI on neutral films; alignment reduces with fluoroscopy or traction.
- Treatment Direction
- Acute repair if early; chronic reconstruction or capsulodesis if cartilage preserved.
- Definition
- Fixed malalignment without reliable reduction.
- Typical Findings
- Fixed DISI/VISI, adaptive contracture, chronic deformity.
- Treatment Direction
- Limited fusion or salvage depending pain and cartilage.
- Definition
- Degenerative collapse.
- Typical Findings
- SLAC, SNAC or radiocarpal/midcarpal cartilage loss.
- Treatment Direction
- PRC, four-corner fusion, limited fusion, total wrist fusion or selected arthroplasty.
Beyond staging a single ligament, examiners expect the overarching Mayo (Larsen/Dobyns) classification of carpal instability, which sorts every pattern into four groups by where the instability sits. CID — Carpal Instability Dissociative: failure within a carpal row, between bones of the same row — the scapholunate and lunotriquetral dissociations that dominate this topic. CIND — Carpal Instability Non-Dissociative: failure between the rows with the intrinsic ligaments intact — classically midcarpal instability (the proximal and distal rows move abnormally as units). CIC — Carpal Instability Complex (Combined): features of both dissociative and non-dissociative patterns — the perilunate dislocation spectrum is the prototype. CIA — Carpal Instability Adaptive: the carpus is malaligned secondary to a problem outside the intrinsic ligaments — most often a distal radius malunion (a dorsally-tilted radius forces a compensatory carpal DISI). The exam value: it forces the question "dissociative, non-dissociative, complex or adaptive?", which immediately separates an SL/LT repair problem from a midcarpal-rehabilitation problem, a perilunate emergency, or a malunion that needs corrective osteotomy rather than ligament surgery.
Clinical Presentation
History
Ask for the mechanism and the functional problem, not just the pain site.
- Why It Matters
- SL injury and perilunate spectrum injuries may follow extension and ulnar deviation loading.
- Decision Consequence
- Triggers careful PA, lateral, stress and fracture assessment.
- Why It Matters
- Tissue repairability decreases with chronic attenuation and capsular contracture.
- Decision Consequence
- Acute repair, chronic reconstruction and salvage are different decisions.
- Why It Matters
- Dorsal central pain suggests SL; ulnar-sided pain suggests LT, TFCC, ECU or ulnar impaction.
- Decision Consequence
- Directs examination and imaging.
- Why It Matters
- Mechanical symptoms suggest instability rather than isolated inflammation.
- Decision Consequence
- Raises threshold for stress imaging or arthroscopy.
- Why It Matters
- Manual work, sport, cane use and transfers increase load demands.
- Decision Consequence
- Influences operative threshold and salvage choice.
Examination technique
Examine both wrists because laxity, contralateral widening and old malunion can mislead interpretation. The sequence should be practical: look, feel, move, load, then stress specific ligament intervals.
- How To Do It
- Seat the patient facing you with forearms supported on a table. Expose both wrists and hands. Compare side-to-side throughout.
- What You Are Looking For
- Guarding, swelling, asymmetry, old scars, deformity, generalised laxity and functional confidence.
- How To Do It
- Inspect dorsally, radially and ulnarly. Ask the patient to make a fist, extend the wrist, load through the palm if tolerated and demonstrate the painful activity.
- What You Are Looking For
- Dorsal swelling around the SL interval, ulnar-sided fullness, ECU subluxation, apprehension with loading, clunking or inability to push up.
- How To Do It
- Palpate Lister's tubercle, SL interval just distal to it, scaphoid tubercle, anatomic snuffbox, LT interval, fovea, ECU sheath and DRUJ.
- What You Are Looking For
- Localised SL tenderness, LT tenderness, foveal pain, ECU pain or DRUJ tenderness. Pain location guides the next stress tests.
- How To Do It
- Assess active and passive flexion, extension, radial deviation, ulnar deviation, pronation, supination and grip. Compare strength and painful arcs.
- What You Are Looking For
- Loss of extension after dorsal capsular injury, painful midcarpal clunk, grip weakness, load-related pain or motion loss from arthritis.
- How To Do It
- Only after localisation, perform Watson shift, LT ballottement, midcarpal shift, TFCC foveal/compression tests, ECU synergy and DRUJ stability.
- What You Are Looking For
- The aim is to reproduce the patient's pain and demonstrate abnormal motion compared with the other side.
- Exact Technique
- Stabilise the distal radius with one hand. Put the thumb of the other hand firmly on the palmar scaphoid tubercle and fingers around the distal carpus. Start in ulnar deviation and slight extension, then move the wrist into radial deviation and flexion while keeping dorsal pressure through the scaphoid tubercle. Release pressure at the end to feel reduction.
- Positive Finding
- Dorsal radial pain, apprehension, a clunk, or a subluxation-reduction sensation compared with the other wrist.
- Interpretation Limits
- Pain alone is non-specific. False positives occur with laxity and painful sprains. It is a screening test; imaging and arthroscopy stage the injury.
- Exact Technique
- Find Lister's tubercle, then palpate just distal and slightly ulnar over the dorsal SL interval with the wrist flexed slightly.
- Positive Finding
- Point tenderness matching the patient's dorsal pain.
- Interpretation Limits
- Useful localisation, but it does not prove mechanical instability.
- Exact Technique
- Stabilise the lunate between thumb and index finger of one hand. Grasp the triquetrum and pisiform with the other hand and translate the triquetrum dorsally and volarly relative to the lunate.
- Positive Finding
- Pain, excessive translation, crepitus or clunk compared with the other side.
- Interpretation Limits
- Overlap with TFCC injury, ECU pathology, ulnar impaction and midcarpal instability is common.
- Exact Technique
- Palpate between the ulnar styloid and FCU tendon for foveal tenderness. Add ulnar deviation and axial compression with rotation if tolerated.
- Positive Finding
- Deep ulnar pain suggests TFCC or ulnocarpal pathology.
- Interpretation Limits
- A positive ulnar-sided test should make isolated LT surgery less likely until TFCC and ulnar variance are assessed.
- Exact Technique
- Resist thumb abduction or wrist extension/ulnar deviation while palpating ECU. Supinate/pronate and look for tendon snapping.
- Positive Finding
- ECU pain, bowstringing or subluxation.
- Interpretation Limits
- ECU pathology can mimic LT or TFCC pain and changes the operative plan.
- Exact Technique
- Apply axial load to the hand with the wrist slightly flexed and ulnarly deviated, then move from radial to ulnar deviation while feeling for sudden reduction or clunk.
- Positive Finding
- Painful clunk, catch or apprehension at the midcarpal joint.
- Interpretation Limits
- Can reflect constitutional laxity. Interpret with symptoms and imaging rather than as an isolated diagnosis.
Watson shift and LT ballottement are useful only when interpreted with symptoms, comparison examination, radiographs, stress imaging and cartilage status. A painful manoeuvre is not the same as surgically important instability.
Differential diagnosis
The single most examined error in this topic is anchoring on a ligament label before excluding the mimics. Dorsal-sided and ulnar-sided wrist pain each have a short, high-yield differential that changes the operation.
- Discriminating Features
- Dorsal-radial pain, positive Watson shift, SL gap and DISI on imaging.
- Key Test or Investigation
- PA, lateral and stress PA; arthroscopy when uncertain.
- Why It Changes Management
- True repairable or reconstructable instability if reducible and cartilage preserved.
- Discriminating Features
- Ulnar-sided pain, positive LT ballottement, possible VISI.
- Key Test or Investigation
- LT ballottement, MRA, arthroscopy.
- Why It Changes Management
- Often overlaps mimics; isolated surgery rarely indicated without confirmation.
- Discriminating Features
- Foveal tenderness, painful forearm rotation, pain with ulnar deviation and loading.
- Key Test or Investigation
- Fovea sign, ulnar variance, MRA, arthroscopy.
- Why It Changes Management
- Treated by TFCC repair or ulnar shortening, not carpal ligament surgery.
- Discriminating Features
- Ulnar-positive variance, chronic load-related ulnar pain, lunate/triquetral chondral change.
- Key Test or Investigation
- Neutral-rotation PA grip view for variance; MRI marrow oedema.
- Why It Changes Management
- Ulnar shortening osteotomy or wafer addresses the driver; ignoring it dooms LT surgery.
- Discriminating Features
- Ulnar pain, snapping with supination, positive ECU synergy test.
- Key Test or Investigation
- ECU synergy test, dynamic ultrasound.
- Why It Changes Management
- Tendon or subsheath problem; managed conservatively or by subsheath reconstruction.
- Discriminating Features
- Painful clunk on ulnar deviation, often constitutional laxity, frequently no discrete tear.
- Key Test or Investigation
- Midcarpal shift test, dynamic fluoroscopy.
- Why It Changes Management
- Reconstruction is unreliable; therapy and proprioceptive retraining come first.
- Discriminating Features
- High-energy injury, broken Gilula arcs, lunate or perilunate malalignment, median nerve signs.
- Key Test or Investigation
- True lateral radiograph, CT, urgent assessment.
- Why It Changes Management
- Surgical emergency-level reduction and stabilisation, not elective ligament work.
- Discriminating Features
- Snuffbox tenderness, scaphoid waist pain, humpback deformity.
- Key Test or Investigation
- Scaphoid views, CT.
- Why It Changes Management
- Fixation or salvage of the scaphoid drives treatment, with its own collapse pattern (SNAC).
- Discriminating Features
- Central dorsal pain, lunate sclerosis or collapse, possible ulnar-negative variance.
- Key Test or Investigation
- Radiographs (Lichtman stage), MRI.
- Why It Changes Management
- Lunate osteonecrosis needs unloading or salvage, not interosseous ligament repair.
Investigations
Plain radiographs
Write a specific imaging request. A useful request is: PA wrist, true lateral wrist, oblique wrist, clenched-fist or pencil-grip stress PA view, and contralateral comparison if subtle instability is suspected. Add scaphoid views if scaphoid fracture is possible and traction or dynamic fluoroscopy if a perilunate spectrum injury or reducibility question exists.
- Why You Request It
- Baseline carpal alignment.
- What To Check
- SL interval, LT interval, Gilula arcs, cortical ring sign, fractures, ulnar variance and arthritis.
- Why You Request It
- Intercalated segment alignment.
- What To Check
- SL angle, capitolunate angle, radiolunate angle, DISI, VISI and perilunate alignment.
- Why You Request It
- Occult carpal fracture and joint overlap clarification.
- What To Check
- Scaphoid, triquetrum, hamate, capitate and distal radius articular injury.
- Why You Request It
- Loads the carpus to reveal dynamic SL widening.
- What To Check
- Side-to-side SL gap difference and dynamic dissociation.
- Why You Request It
- Separates abnormal widening from constitutional laxity.
- What To Check
- Compare gap, angles and symptoms rather than treating an isolated number.
- Why You Request It
- Shows gap opening, clunk and reducibility in real time.
- What To Check
- Helpful when examination and static radiographs disagree.
- How To Assess
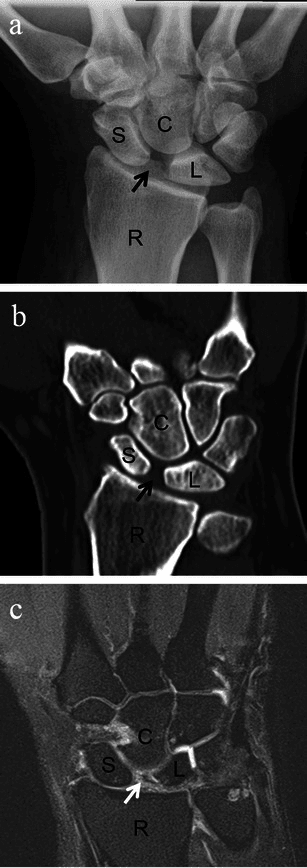
- Measure the interval between the scaphoid and lunate on PA and stress PA views. Greater than 3 mm is suspicious; around 5 mm or more is strongly abnormal when symptomatic.
- Meaning
- SL dissociation or dynamic SL instability.
- How To Assess
- Visible widening between scaphoid and lunate on neutral PA view.
- Meaning
- Static SL dissociation if present at rest.
- How To Assess
- Look for the distal scaphoid seen end-on because the scaphoid is flexed.
- Meaning
- Scaphoid flexion caused by loss of SL control.
- How To Assess
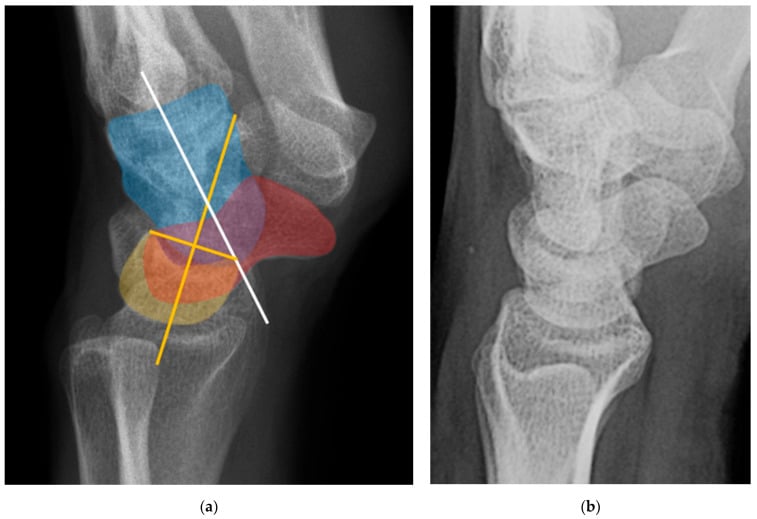
- On the true lateral, draw the scaphoid long axis and the lunate axis. Normal is roughly 30 to 60 degrees; greater than 70 degrees supports DISI.
- Meaning
- Dorsal lunate extension pattern after SL failure.
- How To Assess
- Draw the radial shaft axis and lunate axis on the lateral. The lunate should sit close to neutral relative to the radius.
- Meaning
- Dorsal or volar lunate tilt helps define DISI or VISI.
- How To Assess
- Draw the capitate axis and lunate axis. A small angle is expected; widening indicates carpal malalignment.
- Meaning
- Perilunate spectrum, DISI, VISI or midcarpal instability.
- How To Assess
- Smooth arcs across proximal and distal carpal rows on PA view.
- Meaning
- Broken arcs suggest carpal malalignment or fracture-dislocation.
- How To Assess
- Radioscaphoid narrowing, styloid arthritis, scaphocapitate/capitolunate involvement.
- Meaning
- Ligament reconstruction becomes inappropriate when cartilage is lost.
Advanced imaging
- Best Use
- Dynamic SL gap and comparison with the contralateral wrist.
- Limitations
- Can be normal in predynamic injury and can overcall laxity.
- Best Use
- Real-time clunk, gap opening and reducibility.
- Limitations
- Operator-dependent and requires clinical correlation.
- Best Use
- Ligament signal, occult fracture, cartilage, marrow oedema and associated pathology.
- Limitations
- May miss partial tears or overcall incidental signal change.
- Best Use
- Contrast passage through SL or LT interval and cartilage assessment.
- Limitations
- Invasive; still does not replace arthroscopy when treatment depends on exact grade.
- Best Use
- Fracture, scaphoid nonunion, carpal alignment, arthritis and surgical planning.
- Limitations
- Poor for ligament integrity unless arthrographic.
- Best Use
- Direct ligament, interval, reducibility and cartilage assessment.
- Limitations
- Invasive, but often the reference standard for uncertain symptomatic instability.
Management
Management is chosen by stage, timing, reducibility, cartilage, associated pathology and patient demand. A repairable acute SL tear, a chronic reducible SL dissociation and an arthritic SLAC wrist are different problems.
- Best Treatment Logic
- Immobilisation, analgesia, oedema control, hand therapy and reassessment. Arthroscopic debridement only for persistent symptomatic synovitis or partial tear.
- Do Not Do
- Do not reconstruct a stable wrist because MRI shows signal change.
- Best Treatment Logic
- Direct dorsal SL repair, temporary pinning and possible dorsal capsulodesis augmentation.
- Do Not Do
- Do not repair without correcting the SL gap and carpal angles first.
- Best Treatment Logic
- Stress-view or arthroscopy-confirmed instability: acute repair if early and repairable; reconstruction if chronic and symptomatic.
- Do Not Do
- Do not reassure solely because neutral radiographs look normal.
- Best Treatment Logic
- Capsulodesis, tenodesis or ligament reconstruction depending tissue, demand and surgeon technique.
- Do Not Do
- Do not promise normal wrist kinematics; counsel stiffness and recurrence risk.
- Best Treatment Logic
- Salvage based on cartilage: PRC, four-corner fusion, limited fusion or total wrist fusion.
- Do Not Do
- Do not offer ligament reconstruction when cartilage is already damaged.
- Best Treatment Logic
- Exclude TFCC, ECU, ulnar impaction and midcarpal instability before repair, pinning or fusion.
- Do Not Do
- Do not diagnose isolated LT instability from tenderness alone.
Non-operative management is appropriate only when the wrist is stable or when the patient's symptoms, demand, comorbidity or preference do not justify surgery.
- Treatment
- Short immobilisation, analgesia, oedema control, hand therapy and reassessment.
- Review Trigger
- Persistent dorsal or ulnar-sided pain, clicking or inability to load.
- Treatment
- Immobilisation, protected loading and therapy; arthroscopic debridement if persistent mechanical synovitis.
- Review Trigger
- Positive stress imaging or persistent mechanical symptoms.
- Treatment
- Splinting, activity modification, injections only as diagnostic or temporary tools, therapy.
- Review Trigger
- Progressive deformity, loss of function or degenerative change.
- Treatment
- Splint, analgesia, activity modification, corticosteroid injection and shared decision-making.
- Review Trigger
- Pain, function and radiographic progression.
Do not call non-operative care complete unless follow-up is planned. Dynamic instability can declare itself later.
Delayed diagnosis can convert a repairable ligament injury into a reconstruction or salvage problem. Persistent wrist pain after trauma needs reassessment, not reassurance alone.
Surgical Technique Details
Purpose: confirm ligament grade, dynamic instability, cartilage condition and associated TFCC or chondral injury.
Steps
- Supine position, arm table, traction tower or wrist traction setup.
- Mark Lister's tubercle, EPL, 3-4 portal, 4-5 portal, 6R/6U portals and midcarpal portals.
- Establish 3-4 portal for radiocarpal viewing.
- Inspect radius, scaphoid fossa, lunate fossa, proximal scaphoid, lunate, TFCC and SL interval.
- Probe SL and LT ligaments; assess step-off and whether a probe or scope passes through the interval.
- Use midcarpal portals to assess SL/LT interval from the opposite side, capitolunate joint and cartilage.
- Treat according to grade: debridement for stable partial tears, pinning/repair for unstable acute tears, reconstruction or salvage if chronic.
Hazards: superficial radial nerve, dorsal sensory branches, ECU subsheath, extensor tendons and iatrogenic chondral injury.
- Proximal Row Carpectomy
- Capitate head and lunate fossa must be usable.
- Four-Corner Fusion
- Radiolunate joint must be preserved.
- Proximal Row Carpectomy
- No fusion site; simpler rehabilitation when cartilage is suitable.
- Four-Corner Fusion
- Maintains carpal height better and may suit heavier demand in selected patients.
- Proximal Row Carpectomy
- Radiocapitate arthritis and reduced grip strength if cartilage selection is poor.
- Four-Corner Fusion
- Nonunion, hardware irritation and stiffness.
- Proximal Row Carpectomy
- Capitate head cartilage or lunate fossa is poor.
- Four-Corner Fusion
- Radiolunate arthritis is present or the patient cannot tolerate fusion protection.
Complications
- Cause
- Normal neutral films interpreted as normal wrist.
- Prevention or Response
- Use stress views, reassessment and arthroscopy when symptoms persist.
- Cause
- Immobilisation, capsular surgery, tendon tethering or pain.
- Prevention or Response
- Counsel preoperatively, protect tendons and use staged hand therapy.
- Cause
- Chronic tissue attenuation, failed reconstruction or inadequate reduction.
- Prevention or Response
- Stage properly, reduce before fixation and counsel limitations.
- Cause
- Persistent malalignment and cartilage overload.
- Prevention or Response
- Recognise when reconstruction is too late; shift to salvage.
- Cause
- Trauma, swelling, portals or surgical exposure.
- Prevention or Response
- Document pre/post-op nerve status; decompress if acute carpal tunnel syndrome is present.
- Cause
- K-wire migration, infection, irritation, broken implants.
- Prevention or Response
- Appropriate pin care, removal timing and follow-up.
- Cause
- Poor preparation, fixation, smoking, biology or early loading.
- Prevention or Response
- Meticulous joint preparation, grafting, stable fixation and protected rehabilitation.
- Cause
- Adjacent joint disease, nonunion, expectations or residual impingement.
- Prevention or Response
- Match procedure to cartilage pattern and patient goals.
Guidelines, Registries & Global Practice
Carpal instability is a low-volume, high-complexity problem with no single randomised gold-standard operation, so practice is driven by expert society consensus, surgeon experience and resource setting rather than by registry-mandated implants.
Global epidemiology
- Scapholunate injury is the most frequent carpal instability and a common occult injury after fall-on-the-outstretched-hand trauma (Kitay & Wolfe, J Hand Surg Am 2012).
- Up to two-thirds of displaced intra-articular distal radius fractures carry an associated intracarpal ligament or TFCC injury (Geissler, JBJS Am 1996), so instability is frequently a missed companion of a common fracture.
- SLAC is the most common pattern of wrist osteoarthritis, accounting for around 57% of degenerative wrists in the original radiographic series (Watson & Ballet 1984).
Side-by-side society positions
- Emphasis
- Evidence-based management of distal radius fractures highlights screening for associated carpal/TFCC injury; instability itself has no dedicated high-level guideline.
- Practical Take-Home
- Have a low threshold to look for SL/LT injury when treating wrist trauma.
- Emphasis
- Specialist hand-surgery referral pathways for suspected carpal instability and ulnar-sided wrist pain; emphasis on staged assessment and arthroscopy.
- Practical Take-Home
- Refer persistent post-traumatic wrist pain to a hand unit rather than repeatedly reassuring.
- Emphasis
- Standardised arthroscopic staging of SL and LT tears and arthroscopic-assisted treatment algorithms.
- Practical Take-Home
- Arthroscopy is the reference standard when clinical and radiographic findings disagree.
- Emphasis
- Reduction-first principles for the perilunate spectrum and articular distal radius; carpal alignment must be restored before soft-tissue work.
- Practical Take-Home
- Reduce and align the carpus before judging or repairing ligaments.
- Emphasis
- Recognition that no single reconstruction is superior and that staged, cartilage-led decision-making prevails across Europe.
- Practical Take-Home
- Tailor the operation to stage, reducibility and cartilage, not to a fixed protocol.
Registry note
Unlike hip and knee arthroplasty, wrist ligament reconstruction is not tracked by national joint registries because it uses no standardised implant. Total wrist arthroplasty — a salvage option in selected low-demand wrists — is captured in some national registries (for example the Norwegian and Australian arthroplasty registries report wrist implant survival), and these data consistently show inferior longevity compared with hip and knee implants, reinforcing caution in high-demand patients.
High- versus limited-resource practice variation
- Typical Pathway
- Stress imaging, MR arthrography, diagnostic and therapeutic wrist arthroscopy, full salvage menu including arthroplasty.
- Reason
- Access to arthroscopy and advanced imaging allows precise staging and motion-preserving options.
- Typical Pathway
- Plain radiographs with contralateral comparison, clinical staging, immobilisation, open repair and fusion-based salvage.
- Reason
- Reliance on robust low-cost techniques; arthrodesis is durable and forgiving where arthroscopy and implants are scarce.
- Typical Pathway
- Reduction of perilunate injuries, recognition of acute carpal tunnel syndrome and avoidance of reconstructing an arthritic wrist.
- Reason
- These principles are universal and do not depend on resources.
Common Pitfalls
Persistent wrist pain after trauma needs reassessment. Dynamic SL instability can have normal neutral radiographs.
MRI signal does not equal clinically important instability. Correlate with stress imaging, arthroscopy and symptoms.
SLAC or fixed arthritic collapse is a salvage problem, not a ligament repair problem.
LT pain overlaps with TFCC injury, ECU pathology, ulnar impaction and midcarpal instability.
Controversies and Areas of Uncertainty
This is a field with strong opinions and weak comparative evidence. Naming the honest controversies is a fast way to demonstrate maturity in a viva.
- The Debate
- Capsulodesis, three-ligament tenodesis, bone-ligament-bone graft and screw-based constructs (RASL/SLAM) all have advocates; comparative high-level data are lacking and recurrent radiographic gap is common with every technique.
- Pragmatic Position
- Match technique to tissue, demand and surgeon experience; counsel that no method reliably restores normal kinematics and that radiographic recurrence does not always mean clinical failure.
- The Debate
- The assumption that early stabilisation prevents degenerative collapse is biologically plausible but not proven by long-term controlled data.
- Pragmatic Position
- Treat symptomatic, repairable, reducible injury early, but avoid over-promising arthritis prevention.
- The Debate
- High-resolution MRI and arthroscopy detect partial SL/LT tears whose natural history in asymptomatic wrists is unknown; overtreatment is a real risk.
- Pragmatic Position
- Treat the patient, not the scan; reserve intervention for mechanical symptoms with corroborating examination and stress imaging.
- The Debate
- Meta-analysis now favours PRC for outcomes and complications, yet many surgeons still prefer fusion for younger, heavy-demand patients citing carpal-height preservation.
- Pragmatic Position
- Let cartilage pattern decide first (capitate head and lunate fossa for PRC; radiolunate for fusion); use demand and age as tie-breakers.
- The Debate
- Cadaver and clinical work suggests selective muscle retraining can dynamically stabilise ligament-deficient wrists, but robust trial evidence is limited.
- Pragmatic Position
- A reasonable adjunct for dynamic instability and low-demand patients; not a substitute for surgery in established static instability.
- The Debate
- Reported non-union rates up to 57% and persistent pain make LT fusion contentious.
- Pragmatic Position
- Use only after exhaustively excluding TFCC, ulnar impaction and midcarpal drivers, and counsel the high failure rate.
MCQ Practice Points
Q: What does a normal PA wrist radiograph exclude? A: It excludes obvious static dissociation, but it does not exclude predynamic or dynamic scapholunate instability.
Q: What radiographic pattern is classically associated with scapholunate dissociation? A: DISI, with scaphoid flexion and lunate extension.
Q: What is the key contraindication to ligament reconstruction? A: Fixed irreducible deformity or established arthritis where salvage is required.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A young manual worker has dorsal wrist pain three months after a fall. Neutral radiographs look normal.”
“A high-demand patient has an acute complete scapholunate ligament tear with reducible SL widening and no arthritis.”
“A patient has chronic scapholunate dissociation, DISI deformity and radioscaphoid arthritis.”
“A 35-year-old presents with chronic ulnar-sided wrist pain, a painful click and a positive lunotriquetral ballottement test. They want to know if they need a lunotriquetral fusion.”
Core diagnosis
- SL injury: dorsal pain, Watson shift, SL gap, DISI.
- LT injury: ulnar-sided pain, LT ballottement, possible VISI.
- Dynamic injury may need stress views or arthroscopy.
Measure
- SL gap on PA and stress views.
- Scapholunate angle and capitolunate angle on lateral.
- Gilula arcs, ring sign, DISI/VISI and arthritis pattern.
Stage
- Predynamic: symptoms, no radiographic instability.
- Dynamic: stress instability.
- Static reducible: visible malalignment that corrects.
- Irreducible or arthritic: salvage logic.
Treat
- Stable partial tear: immobilisation, therapy, selected arthroscopic debridement.
- Acute complete reducible SL: repair, pinning, possible capsulodesis.
- Chronic reducible SL: reconstruction or capsulodesis.
- Arthritic collapse: PRC, four-corner fusion, limited fusion or total wrist fusion.
Must not miss
- Perilunate spectrum injury in high-energy trauma.
- TFCC, ECU and ulnar impaction in LT-type symptoms.
- Cartilage loss before offering reconstruction.
- Median nerve symptoms after carpal trauma.
Evidence Base
The papers below are the ones most worth being able to cite by name in a viva. Each statistic has been checked against the original PubMed record. According to PubMed, the verified sources are as follows.
Watson & Ballet — the SLAC pattern (landmark natural history)
- Review of 4,000 wrist radiographs identified 210 cases of degenerative arthritis after excluding other arthritides; the scapholunate advanced collapse (SLAC) sequence was the single most common pattern at 57%, beginning at the radioscaphoid joint.
- A further 27% involved the scaphotrapezium-trapezoid joint and 15% combined both patterns; 18 of 19 operated patients had less pain postoperatively.
Geissler — arthroscopic classification of carpal ligament tears
- Prospective arthroscopic study of 60 displaced intra-articular distal radius fractures: 41 patients (68%) had associated intracarpal soft-tissue injury, including 26 TFCC tears, 19 scapholunate and 9 lunotriquetral interosseous ligament tears.
- Intracarpal injuries clustered with fractures involving the lunate facet; the paper introduced the arthroscopic grading of interosseous ligament tears now known as the Geissler classification.
Kitay & Wolfe — scapholunate instability current concepts
- Comprehensive review establishing scapholunate injury as the most frequent cause of carpal instability and proposing a widely used treatment algorithm based on stage of injury, secondary ligament damage and arthritic change.
- An isolated SLIL tear may show normal static radiographs yet progress to abnormal kinematics, cartilage wear and degenerative collapse.