Microsurgical Replantation | Sharp vs Crush vs Avulsion | Warm and Cold Ischaemia | BEFANV Sequence of Repair | Artery-Vein-Nerve-Vein | Survival and Functional Outcomes | Replant vs Revision Amputation
- Replantation means reattachment of a completely amputated part; revascularisation means restoration of flow to a critically ischaemic but still partially attached part - both are managed by the same microsurgical team using the same principles
- Ischaemia time is the single most important triage factor: digits tolerate up to 12 hours of cold ischaemia or 6 hours of warm ischaemia; the more proximal the amputation (hand, forearm, arm) the less the muscle tolerates ischaemia and the shorter the window
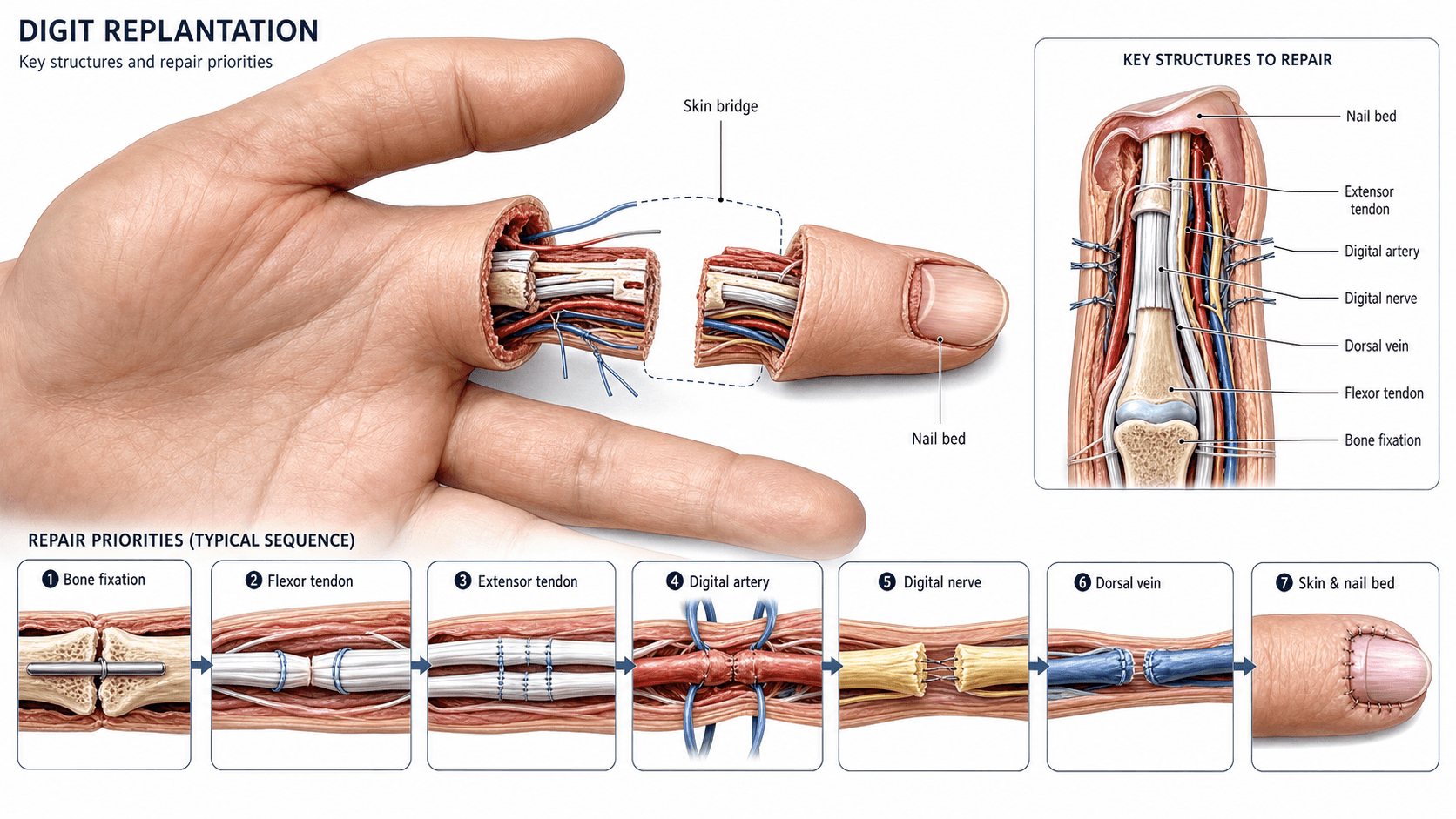
- The classical sequence of repair is BEFANV: Bone shortening and fixation, Extensor tendon repair, Flexor tendon repair, Artery anastomosis, Nerve coaptation, Vein anastomosis - always bone first to provide a stable platform and allow vessel repair under no tension
- Indications follow the BSSH/ASSH consensus: thumb (always), multiple digits, single digit in children, and any amputation at hand, wrist or more proximal level; single finger amputation in an adult is a relative indication and is judged case-by-case
- The avulsed thumb with prolonged ischaemia is often still worth replanting because the thumb is 40% of hand function; alternative procedures (pollicisation, toe transfer) are reserved for the failed or impossible replant
- Replantation is not always in the patient's best interest: a stiff, painful, cold-intolerant replanted finger may be functionally worse than a well-performed revision amputation with a prosthesis - the decision must be shared with the patient and family
- “Always start a viva on replantation with ischaemia time and the mechanism of injury - examiners want to see you triage the case before you start talking about microsurgery
- “A single, sharply amputated finger in a 50-year-old manual worker is a relative indication - discuss the realistic functional outcome honestly and offer revision amputation as an alternative
- “The 'red line' and 'ribbon sign' on the dorsal vein of an avulsed digit predict poor vessel quality and almost always need vein grafting
- “Bone shortening of 5-10 mm relaxes the vessel and nerve repairs and converts a high-tension anastomosis into a safe one - this is the first decision in the operating room, not the last
- “After arterial repair, allow the digit to perfuse for 10-15 minutes before repairing the veins - this identifies the bleeding dorsal veins, fills the venous bed, and reduces anastomotic tension
Digit and Hand Replantation
Replantation is a long, expensive, technically demanding operation with a meaningful failure rate and a significant burden of re-operation, stiffness and cold intolerance. The patient and family must understand that survival of the replant does not equal function, and that a single stiff finger in an extension contracture may impair the hand more than a clean amputation would. Examiners will mark you down for offering replantation to every patient, and equally for refusing it without a defensible reason. The decision is a calculation of mechanism, ischaemia time, level, patient age, vocation and patient choice - not an automatic response to a severed digit.
- Best option
- Replantation (or toe transfer if replant fails or is impossible)
- Reasoning
- Thumb is approximately 40% of hand function; loss cannot be compensated by the remaining digits; even a stiff, short thumb is better than no thumb
- Best option
- Replantation of at least one or two digits to restore pinch and grip
- Reasoning
- Even replantation of two of four amputated fingers gives a tripod pinch and acceptable grip; combination of replantation and completion amputation is often the best answer
- Best option
- Replantation
- Reasoning
- Children regain excellent function and sensate recovery; adults with a clear functional need (e.g. musician) warrant replantation despite zone II concerns
- Best option
- Revision amputation (and prosthesis)
- Reasoning
- Zone II replants are stiff; a clean amputation with early mobilisation gives faster, more reliable return to work; offer both options honestly
- Best option
- Replantation in a specialist centre
- Reasoning
- Proximal amputations affect multiple tissues including muscle; viability and function are both reasonable; muscle ischaemia is the limiting factor
- Best option
- Revision amputation
- Reasoning
- Survival is unlikely, function would be poor, and the patient is best served by a clean closure, dressing and early mobilisation
Overview and Indications
Replantation is the surgical reattachment of a body part that has been completely amputated. Revascularisation is the restoration of blood flow to a part that remains partially attached but is critically ischaemic. Both are managed by the same microsurgical team using the same principles of bone fixation, tendon repair, microvascular anastomosis and nerve coaptation.

The history of replantation began with the first successful thumb replantation by Komatsu and Tamai in 1968 in Japan, followed by the world's first arm replantation in 1962 (Malt and McKhann reported a 12-year-old boy with an arm replant). Modern digital replantation became clinically routine after the introduction of the operating microscope, fine monofilament nylon sutures (10-0, 11-0) and the development of structured post-operative monitoring and salvage protocols.
The decision to replant is not automatic. It is a calculated judgement based on:
- The mechanism of injury (sharp, crush, avulsion) - the most important predictor of success
- The ischaemia time (warm and cold) - dictates muscle viability and the risk of reperfusion injury
- The level of amputation (zone, digit, hand, more proximal)
- The patient (age, vocation, hand dominance, comorbidities, expectations)
- The resources (microsurgical team, theatre time, monitoring capability)
- Thumb amputation at any level - absolute indication; thumb is approximately 40% of hand function
- Multiple digit amputation - replant at least one or two to restore tripod pinch
- Single digit amputation in children - excellent functional recovery and nerve regeneration
- Single digit in selected adults - musicians, professionals with unique hand requirements
- Hand, wrist, forearm or arm amputation - survival and function are both reasonable in specialist units
- Bilateral digital or hand amputation - at least one side must be restored
- Amputated part that is destroyed, severely crushed or degloved beyond surgical reconstruction
- Multiple-level amputation in the same digit
- Prolonged warm ischaemia beyond muscle tolerance (greater than 6 hours for digits, greater than 4-6 hours for hand/forearm)
- Medically unfit patient unable to tolerate 6-12 hours of anaesthesia
- Self-inflicted amputation in a psychiatrically unstable patient
- Single finger amputation at zone II in an adult (the most debated indication)
- Avulsion injury with extensive vessel and nerve damage
- Severe contamination (farmyard, marine, sewerage)
- Prolonged ischaemia in a part containing significant muscle
- Patient unable or unwilling to commit to prolonged rehabilitation
- Surgeon or centre without microsurgical capability and no safe transfer pathway
Examiners frequently test whether you can defend offering revision amputation with prosthesis to an adult with a single zone II finger amputation. The argument: zone II replantation produces a stiff finger, often held in extension, with poor active flexion, painful neuroma, and 6-12 months off work. A clean amputation with dressing, early mobilisation and a tailored prosthesis gives faster return to function and less pain. The exceptions are children, musicians, patients with a clear unique functional need for that digit, and patients who have a strong informed preference for replantation after a balanced discussion.
The decision and conduct of proximal ("macro") replantation - hand, forearm, arm - differ fundamentally from a digit, because the part contains large muscle bulk and the systemic stakes are high:
- Muscle is the limiting tissue: warm ischaemia tolerance is only a few hours (roughly under 4-6 hours for the hand, under 4 hours for the forearm/arm), far shorter than the 6-12+ hours a muscle-free digit tolerates.
- Reperfusion is a systemic event: re-establishing flow washes out the potassium, lactate/acid, and myoglobin that accumulated in ischaemic muscle - risking hyperkalaemic cardiac arrest, metabolic acidosis, and myoglobinuric acute kidney injury (rhabdomyolysis). Anticipate it: liaise with anaesthesia, check/correct potassium, ensure aggressive hydration and urine output (+/- alkalinisation) before and during reperfusion, and consider flushing the part (and a brief controlled wash-out) before completing the venous anastomosis.
- No-reflow phenomenon: after prolonged ischaemia, microvascular thrombosis/endothelial swelling can prevent capillary perfusion even with a patent anastomosis - another reason proximal replants have a tighter time window and lower viability.
- Strategy: macroreplantation often uses early bony shortening, generous muscle debridement, temporary arterial shunting to restore perfusion fast, and a low threshold for fasciotomy; "life over limb" - revision amputation is correct if the systemic risk is prohibitive or the muscle is non-viable. Ectopic ("banking") implantation of a salvageable part onto a distant recipient vessel is an option when immediate definitive replant is not possible.
Exam point: proximal replantation is governed by muscle ischaemia and reperfusion - short time window, hyperkalaemia/acidosis/myoglobinuria on reperfusion, no-reflow, the need for fasciotomy/debridement, and a life-over-limb threshold that a single-digit replant never faces.
Relevant Anatomy and Biomechanical Principles
- Each digit is supplied by two proper digital arteries that run on the ulnar and radial sides of the volar surface, just deep to the volar skin and superficial to the flexor tendon sheath
- The radial digital artery is usually the dominant vessel in the index, middle and ring fingers; the ulnar digital artery is dominant in the thumb and little finger (the "all-ulnar" thumb is a well-recognised variant)
- The arteries give off dorsal branches at each phalanx that supply the dorsal skin, nail bed and distal phalanx
- Venous drainage is predominantly by dorsal veins that lie in the subcutaneous tissue on the dorsum of the digit; volar veins exist but are smaller and less reliable
- The dorsal veins are the target for venous anastomosis - they are larger, more numerous, and easier to work with under the microscope
- The proper digital nerves run alongside the proper digital arteries on the ulnar and radial sides of the volar digit
- They are pure sensory nerves supplying the pulp, volar skin, dorsal distal skin and nail bed
- The dorsal sensory branch of the radial or ulnar nerve supplies the dorsum of the proximal and middle phalanges
- Coaptation must restore both volar and dorsal sensibility to prevent painful neuroma and to allow fine touch discrimination
- Flexor digitorum profundus (FDP) inserts on the volar base of the distal phalanx; flexes the DIP joint
- Flexor digitorum superficialis (FDS) inserts on the volar shaft of the middle phalanx; flexes the PIP joint
- The flexor tendon sheath (zone II of Verdan's classification) overlies the tendons from the distal palmar crease to the middle of the middle phalanx
- Extensor tendon is a single extensor digitorum communis (EDC) tendon over the proximal phalanx, with a central slip inserting on the middle phalanx base and lateral bands joining to insert on the distal phalanx base
- The distal phalanx, middle phalanx and proximal phalanx are short tubular bones with good cortical purchase for K-wires
- The head of the phalanx flares slightly, making rigid plate fixation less common in digits; K-wire fixation (axial, crossed or longitudinal) is the workhorse
- In the hand (metacarpals) and forearm (radius, ulna), plate fixation is feasible and provides more rigid bone fixation, allowing early mobilisation
- Digits (no muscle): warm ischaemia tolerated up to 6 hours; cold ischaemia (wrapped in saline-soaked gauze, placed in a sealed bag, then in ice water) tolerated up to 12 hours; some series report success at 24-30 hours of cold ischaemia
- Hand (small muscles of the hand): warm ischaemia less than 4-6 hours; cold ischaemia less than 10-12 hours
- Forearm and arm (large muscle bulk): warm ischaemia less than 4 hours; cold ischaemia less than 8-10 hours - the muscle is the limiting factor because of reperfusion injury, myonecrosis, myoglobinuria and renal failure
- Shortening the bone by 5-10 mm converts a high-tension vessel, nerve and tendon repair into a low-tension repair
- This is the single most important technical decision: do not try to perform a primary repair under tension - shorten the bone, then repair everything else
- A digital replant with 5 mm of bone shortening is functionally indistinguishable from one with no shortening; a digital replant with a failed arterial anastomosis from tension is functionally a dead digit
Internervous Plane and Surgical Interval
The replantation approach is not a true internervous plane - the dissection follows the wound edges and exposes the cut structures serially, identifying and tagging vessels, nerves and tendons for later repair. The relevant surgical intervals depend on the level and the digit:
- Volar approach (preferred for vessel and nerve access): mid-lateral or Bruner-style zig-zag incisions on the volar aspect of the digit, identifying the flexor sheath, the proper digital neurovascular bundles, and the distal cut ends of the digital arteries and nerves
- Dorsal approach (preferred for venous access): a longitudinal or zig-zag incision on the dorsum of the digit and the hand, identifying the dorsal veins, extensor tendon and bone ends
- The two approaches (volar and dorsal) are used together - the volar for arteries and nerves, the dorsal for veins and bone fixation
- Extend the volar wound proximally into the palm using a Bruner or mid-lateral incision
- Identify the common digital arteries and nerves in the palm
- Identify the flexor tendons in the palm and tag them
- Expose the metacarpal fractures for fixation
- Use a separate dorsal incision over the metacarpals to identify the dorsal veins and extensor tendons
- Volar approach: extend the volar incision proximally to expose the median nerve, ulnar nerve, radial and ulnar arteries, and the flexor tendons
- Dorsal approach: separate dorsal incision to expose the extensor tendons, dorsal veins, and the radius/ulna for fixation
- The two approaches are linked by the circumferential skin at the level of injury, which is usually debrided and used to expose all structures
- Both proper digital arteries (or the common digital arteries in the palm)
- Both proper digital nerves
- The flexor digitorum profundus and (where present) superficialis tendons
- The extensor tendon
- The dorsal veins (usually 2-4 dorsal veins per digit)
- The bone ends
- The digital skin edges (for orientation and length)
The single commonest cause of replantation failure is a missed structure that is later needed and cannot be found in a blood-filled, retracted field. Tag every cut end of artery, nerve, tendon and vein with a fine suture or microclip as you identify it, and only then begin the repair sequence. Skipping this step is a recipe for theatre chaos.
Patient Positioning and Setup
- Position: supine on a radiolucent operating table. The arm is extended on a hand table. The patient must be positioned to allow two surgical teams to work simultaneously - one preparing the amputated part on a separate instrument table, and one preparing the stump
- Anaesthesia: general anaesthesia is the standard for adults. Regional anaesthesia (axillary brachial plexus block) is used by some centres and may provide intra-operative vasodilation, post-operative analgesia and sympathetic blockade
- Tourniquet: an upper-arm or forearm tourniquet is used for the initial wound debridement and vessel identification, then released. Avoid prolonged tourniquet use once the anastomosis is being performed
- Microscope: an operating microscope (10x to 25x magnification) is mandatory for all vessel and nerve work. Some surgeons use loupes (4x-6x) for vein harvesting and nerve preparation
- Instruments: microsurgical instrument set - micro-forceps, micro-scissors, micro-needle holder, jeweller's forceps, vessel dilators, single and double micro-clamps
- Suture: 9-0, 10-0 and 11-0 monofilament nylon (Ethilon or similar) on a fine taper needle; 9-0 for larger proximal vessels, 10-0 for digital vessels, 11-0 for supermicrosurgical distal vessels
- Irrigation: heparinised saline (1000 units heparin in 100 mL normal saline) for vessel irrigation and irrigation of the cut vessel ends
- Pre-operative preparation of the amputated part: as soon as the part arrives in theatre, it is inspected, photographed, radiographed if bony injury is suspected, and the vessels, nerves and tendons are identified under the microscope and tagged. The part is kept cool (wrapped in saline-soaked gauze, sealed in a plastic bag, placed in an ice-water bath) and is only removed from cooling when the team is ready for the anastomosis
- Anticoagulation: prophylactic systemic heparin (low-dose, 5000 unit subcut or 1000 units IV per hour) is used by many centres during the anastomosis, but practice varies. Aspirin and dextran are used by some units; topical heparin irrigation of the vessel ends is universal
Identify and tag the vessels, nerves and tendons in the amputated part on the back table while the second team is preparing the stump. This is the single biggest time-saver in replantation. A properly prepared amputated part can be reattached in 30-45 minutes once the stump is ready; a poorly prepared part adds hours.
Surgical Technique
The classical sequence of repair is BEFANV - Bone, Extensor, Flexor, Artery, Nerve, Vein. The principle is to provide a stable, low-tension platform for every subsequent repair.
Debride the bone ends with a rongeur, shorten by 5-10 mm (more in avulsion injuries), and fix with K-wires (axial, crossed, or longitudinal intramedullary) for digits, or a mini-plate for hand/forearm. The bone must be rigid before any soft tissue repair.
Repair the extensor tendon over the dorsum of the digit using a modified Kessler or figure-of-eight core suture (4-0 or 3-0 non-absorbable). The extensor is repaired before the flexor to avoid disrupting the flexor repair when suturing on the dorsum.
Repair the FDP and (where present) FDS using a modified Kessler or Strickland core suture (4-0 or 3-0 non-absorbable) with an epitendinous running suture. In zone II, the sheath is opened widely; A2 and A4 pulleys are preserved.
Anastomose at least one proper digital artery under the microscope. Use 10-0 or 11-0 nylon with interrupted sutures. Both ends are debrided to healthy intima; the lumen is irrigated with heparinised saline; the vessel is dilated gently; a single or double micro-clamp is applied. Typical anastomosis uses 6-10 interrupted sutures.
Coapt the proper digital nerves with 9-0 or 10-0 nylon epineurial sutures (typically 2-4 sutures per nerve). The nerve repair is performed while the digit is being perfused, so the field is clearer and the vessels are easier to identify.
After 10-15 minutes of arterial perfusion, the dorsal veins become engorged and identifiable. Anastomose at least two dorsal veins for every one artery repaired. Use 10-0 or 11-0 nylon with interrupted sutures. The skin is loosely approximated; do not close tightly to avoid venous congestion.
The window for salvage of a thrombosed replant is measured in hours, not days. A sudden change in colour, capillary refill, temperature or Doppler signal within the first 5-7 days mandates immediate return to theatre. Delay leads to irreversible ischaemia, no-reflow phenomenon and loss of the replant. Have a low threshold to re-explore - the worst that can happen is you find a patent anastomosis; the worst that can happen if you delay is a dead digit.
Structures at Risk and Complications
Replantation has a meaningful complication profile, both technical and functional. The overall survival rate in modern series is 80-90% for digits and 60-80% for hand/forearm amputations, but function and patient satisfaction are not guaranteed by survival.
- Arterial thrombosis - most common in the first 24-72 hours; presentation is sudden pallor, cool pulp, loss of Doppler signal. Managed by immediate re-exploration, thrombectomy, and revision of the anastomosis (often with a vein graft)
- Venous congestion - more common than arterial occlusion, particularly in fingertip replants; presentation is cyanosis, dark purple colour, brisk dark bleeding on pinprick. Managed by leech therapy (Hirudo medicinalis) for the first 24-48 hours, nail plate removal to allow bleeding, or re-exploration with revision venous anastomosis
- No-reflow phenomenon - despite a patent anastomosis, the microcirculation fails to reperfuse; the digit remains mottled and cool. Caused by prolonged ischaemia, reperfusion injury, and microthrombi. Difficult to manage; consider hyperbaric oxygen therapy, IV iloprost, or sympathectomy
- Compartment syndrome of the forearm/hand after prolonged ischaemia and reperfusion; managed by urgent fasciotomy
- Myoglobinuria and acute kidney injury after release of muscle ischaemia; managed by aggressive IV fluid resuscitation, urinary alkalinisation, and dialysis if needed
- Hyperkalaemia and acidosis on reperfusion; monitor and correct in real time
- Neuroma at the repair site, particularly if the nerve was repaired under tension; may require later neuroma excision and grafting
- Cold intolerance - very common, affecting 50-80% of replant patients; may persist for years; managed by warming, gloves, and reassurance
- Stiffness and dysaesthesia - particularly in zone II replants with poor flexor recovery
- Adhesions after zone II flexor tendon repair in the digital sheath; common cause of poor active flexion; managed by tenolysis at 3-6 months
- Rupture of the flexor or extensor repair; managed by re-repair or tendon grafting
- Lateral band migration and boutonniere deformity after central slip disruption
- Nonunion or malunion at the osteotomy site; rare with K-wire fixation
- Pin-track infection with externalised K-wires; managed by pin care, oral antibiotics, and early K-wire removal
- Joint stiffness secondary to prolonged immobilisation; managed by hand therapy and dynamic splinting
- Superficial wound infection - common; managed by oral antibiotics and wound care
- Deep infection / osteomyelitis - rare but devastating; may lead to loss of the replant
- VTE - uncommon in upper limb surgery, but reported
- Fat embolism - rare, but reported in major limb replants
- Drug reactions and transfusion complications - related to the long operation and blood loss
- Stiffness - the commonest long-term problem; zone II replants have the worst prognosis
- Cold intolerance - 50-80% of patients
- Chronic pain - in a minority
- Failure of intrinsic muscle function after prolonged ischaemia
- Delayed tendon rupture - flexor or extensor
Cold intolerance affects 50-80% of replant patients, often for years. It is the commonest reason patients are dissatisfied with a technically successful replant. Counsel patients pre-operatively; this is the most under-acknowledged complication in the consent process and the commonest long-term cause of disappointment.
Guidelines, Registries and Global Practice
There is no single universal guideline for replantation, but international consensus exists through the major hand surgery societies on the core indications, sequence of repair and post-operative care.
- American Society for Surgery of the Hand (ASSH) / American Academy of Orthopaedic Surgeons (AAOS): thumb, multiple digits, hand/wrist/forearm, and bilateral amputations are absolute indications. Single-finger amputation in an adult is a relative indication. The use of a structured hand therapy programme and routine clinical monitoring is recommended.
- British Society for Surgery of the Hand (BSSH): the BSSH endorses a similar list, with explicit emphasis on transfer of amputated parts and patients to a specialist replantation centre for any amputation that may be replantable. The standard is that the amputated part is wrapped in saline-soaked gauze, placed in a sealed bag, and the bag is placed in ice water - and the patient is transferred with the part.
- Japanese Society for Surgery of the Hand (JSSH): Japan has historically had the largest concentration of replantation expertise, with pioneering surgeons including Tamai, Komatsu, and Buncke. The Japanese experience underpins the modern understanding of the procedure.
- Federation of European Societies for Surgery of the Hand (FESSH) / EFORT: the European consensus mirrors the BSSH and ASSH, with the addition of structured outcome reporting using the Chen criteria (I-IV) and the Tamai criteria (I-IV) for functional assessment.
- International Federation of Societies for Surgery of the Hand (IFSSH): provides the global standard for training and credentialing in replantation, including the requirement for a microscope, micro-instruments, an experienced team and a post-operative monitoring protocol.
- There is no single global replantation registry comparable to the arthroplasty registries, but national audits in the UK (BSSH), US (ASSH), Japan (JSSH) and the Replantation Registry at the Kleinert-Kutz Hand Care Center (USA) have reported survival and functional outcome data.
- Large single-centre series (Tamai, Waikakul, Morrison) have shaped practice more than registries have.
- The Chen criteria classify functional outcome: I = excellent (return to work, normal range of motion, normal two-point discrimination), II = good (return to work, near-normal range of motion, slightly impaired two-point discrimination), III = fair (return to lighter work, limited range of motion, poor two-point discrimination), IV = poor (unable to return to work, severe stiffness, painful neuroma).
- East Asia (Japan, China, Korea, Taiwan): historically the highest volume of replantation in the world, with established regional and national centres of excellence. Replantation is offered more liberally than in the West; survival rates are consistently high.
- United States and Europe: the trend over the last 25 years has been more selective offering, particularly for single-finger zone II amputations in adults. Revision amputation with a tailored prosthesis is more commonly recommended than in East Asia.
- Low- and middle-income settings: replantation may be limited by the availability of a microscope, an experienced microvascular team, and the long operative and post-operative commitment. Transfer of the patient (with the part) to a regional centre is the standard.
- Distant and rural settings: the amputated part should be cooled, the patient stabilised, and transfer to a replantation centre should occur as soon as possible. Aeromedical retrieval with the part cooled in transit is well established.
- Chen criteria and Tamai criteria are the most widely used functional outcome scores
- The DASH (Disabilities of the Arm, Shoulder and Hand) and MHQ (Michigan Hand Outcomes Questionnaire) are validated patient-reported outcome measures
- Cold intolerance is measured by the CISS (Cold Intolerance Symptom Severity) score
- Survival alone is no longer considered an adequate outcome; modern series report survival AND function AND patient satisfaction
- Wrap the part in saline-moistened gauze
- Place in a sealed plastic bag
- Place the sealed bag in ice water (not dry ice - that freezes the tissue)
- Do not allow the part to soak in water or saline (causes maceration)
- Do not attempt to clean, debride or cannulate the part
- Transport with the patient; the part and the patient travel together
- Notify the receiving centre in advance so the team and theatre are ready
Memory Aids
THUMBIndications for Replantation - THUMB
Hook:THUMB - replant because no other digit can substitute for the thumb; without it, pinch and grip are lost
BEFANVSequence of Repair - BEFANV
Hook:BEFANV - bone first to give a stable platform, extensor before flexor, vessels before nerves before veins; bone shortening relaxes tension on every repair
AVOIDContraindications to Replantation - AVOID DISASTER
Hook:AVOID DISASTER - the relative and absolute contraindications are a hierarchy; absolute is fewer than trainees believe, but the relative list is the one that tests judgment
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old right-handed builder amputates his dominant right thumb cleanly with a circular saw at the level of the interphalangeal joint. The amputated part is wrapped in saline-soaked gauze and brought with him to the emergency department. He arrives 90 minutes after injury. He is haemodynamically stable, has no other injuries, and is asking urgently about replantation. Discuss your management.”
“A 28-year-old chef had a sharp amputation of his right index finger at the middle of the middle phalanx 4 days ago. The replant was performed at your centre with a K-wire, repair of FDP/FDS, anastomosis of the radial digital artery, both proper digital nerves and two dorsal veins. The digit was well-perfused for 72 hours. On day 4, the digit is suddenly cold, mottled purple, with no Doppler signal in the arterial pedicle, but brisk dark bleeding on pinprick. Discuss your management.”
One-liner
- Microsurgical reattachment of a completely amputated part using a structured sequence of bone fixation, tendon repair, microvascular anastomosis and nerve coaptation
- Replantation must be offered selectively - the decision balances mechanism, ischaemia time, level, patient factors and the realistic functional outcome
Indications (THUMB)
- Thumb at any level (absolute - 40% of hand function)
- Hand, wrist, forearm, arm amputation (muscle limits ischaemia window)
- Unique functional need (musician, surgeon, manual specialist)
- Multiple digits (replant one or two to restore tripod pinch)
- Bilateral amputation
Contraindications
- Absolute: destroyed part, prolonged warm ischaemia, medically unfit, self-inflicted in psychiatric instability
- Relative: single finger zone II in adult, avulsion, severe contamination, prolonged ischaemia with muscle, patient unable to commit to rehab
Ischaemia times
- Digits: warm less than 6 hours, cold less than 12 hours (no muscle)
- Hand: warm less than 4-6 hours, cold less than 10-12 hours
- Forearm/arm: warm less than 4 hours, cold less than 8-10 hours - muscle is the limit
- Transport: wrap in saline-soaked gauze, sealed bag, ice water - never dry ice, never soak
Sequence of repair (BEFANV)
- Bone: debride, shorten 5-10 mm (more in avulsion), fix with K-wires or plate
- Extensor: repair first to avoid disrupting flexor repair
- Flexor: FDP and FDS core suture plus epitendinous run
- Artery: at least one proper digital artery, 10-0 or 11-0 nylon
- Nerve: epineurial 9-0 or 10-0 nylon while the digit is perfusing
- Vein: at least two dorsal veins for every one artery; perfuse 10-15 minutes to identify veins
Vessel and nerve technique
- Debride vessel ends to healthy intima - watch for red line and ribbon signs
- Irrigate with heparinised saline; dilate gently to relieve spasm
- Vein graft from volar forearm or foot for tension-free repair
- Nerve coaptation with 9-0 or 10-0 epineurial; cable graft from MABCN or sural if gap
- Bone shortening is the single biggest technical decision - converts high-tension to low-tension repair
Post-op monitoring and salvage
- Nurse in warm room (24-26 degrees), elevate, hourly colour and Doppler checks
- Implantable Doppler (Cook-Swartz) for continuous venous monitoring is the gold standard
- Aspirin 75-150 mg daily for 2-4 weeks; broad-spectrum antibiotics 24-48 hours
- Sudden change = immediate return to theatre; leech therapy for venous congestion
- Take-back within 2-4 hours of vascular change; salvage rate 30-50%
Outcomes and complications
- Digit survival 80-90%; hand/forearm 60-80%; function always below normal
- Cold intolerance 50-80% - the commonest long-term complaint
- Stiffness (zone II worst), tenolysis at 3-6 months if no progress
- Chen and Tamai functional criteria (I-IV); DASH and MHQ for PROMs
- Single finger zone II adult - often better with revision amputation and prosthesis
Evidence Base
- First reported successful major limb (arm) replantation in a 12-year-old boy whose right arm was severed at the proximal humerus in a train accident; the limb was cooled, the patient transferred, and the arm was reattached with anastomosis of the brachial artery and veins, internal fixation of the humerus, and repair of the musculocutaneous, median, ulnar and radial nerves, with documented functional recovery at follow-up.
- In 100 consecutive digital replantations and revascularisations, overall digit survival was 78% with sharp cuts achieving the highest survival, crush injuries intermediate, and avulsion injuries the lowest. Long-term functional assessment showed useful range of motion in the majority of successful replants, with two-point discrimination averaging 10-12 mm in the best cases and cold intolerance as the commonest long-term complaint.
- In 65 single-finger replantations (excluding thumb) followed for an average of 4.5 years, 71% of replants survived but only 36% achieved a 'good' functional outcome, with zone II replants particularly poor. The authors concluded that single-finger replantation in adults is not always in the patient's best interest and emphasised the importance of careful patient selection.
- In 293 upper extremity replantations performed by the Tamai group over 20 years, overall survival was 82% for digits, 73% for hands, and 67% for more proximal amputations. Survival was highest for sharp cuts, intermediate for crush, and lowest for avulsion. Functional recovery, assessed by Chen's criteria, was good or excellent in 65% of cases overall, with cold intolerance and stiffness as the commonest long-term complaints.
- In 1018 digital replantations across 552 patients, overall digit survival was 92%. Survival was lower with avulsion injuries (76%), crush injuries (88%) and in zone II (87%) than with sharp cuts at other levels. Return to work averaged 3 months; the majority of patients reported satisfaction, but cold intolerance persisted in 64% at one year.