Hawkins Classification of Talar Neck Fractures
A displaced talar neck fracture with a dislocation is treated urgently — but be precise about WHY. Urgent reduction of the dislocated subtalar/ankle joint and of any open wound protects the skin and soft-tissue envelope and relieves pressure; however, high-level evidence (Vallier 2004; Rammelt 2009) shows that the AVN rate is determined by the initial injury severity (degree of displacement, comminution, open fracture) and is not reduced by emergent definitive fixation. So: reduce dislocations and open fractures now, but definitive rigid fixation can sensibly wait until soft-tissue swelling settles. Non-operative treatment is reserved for a truly undisplaced Type I; everything displaced needs anatomical reduction and stable fixation. Know the mechanism (forced dorsiflexion), the blood supply, and the Hawkins sign.
The Hawkins classification
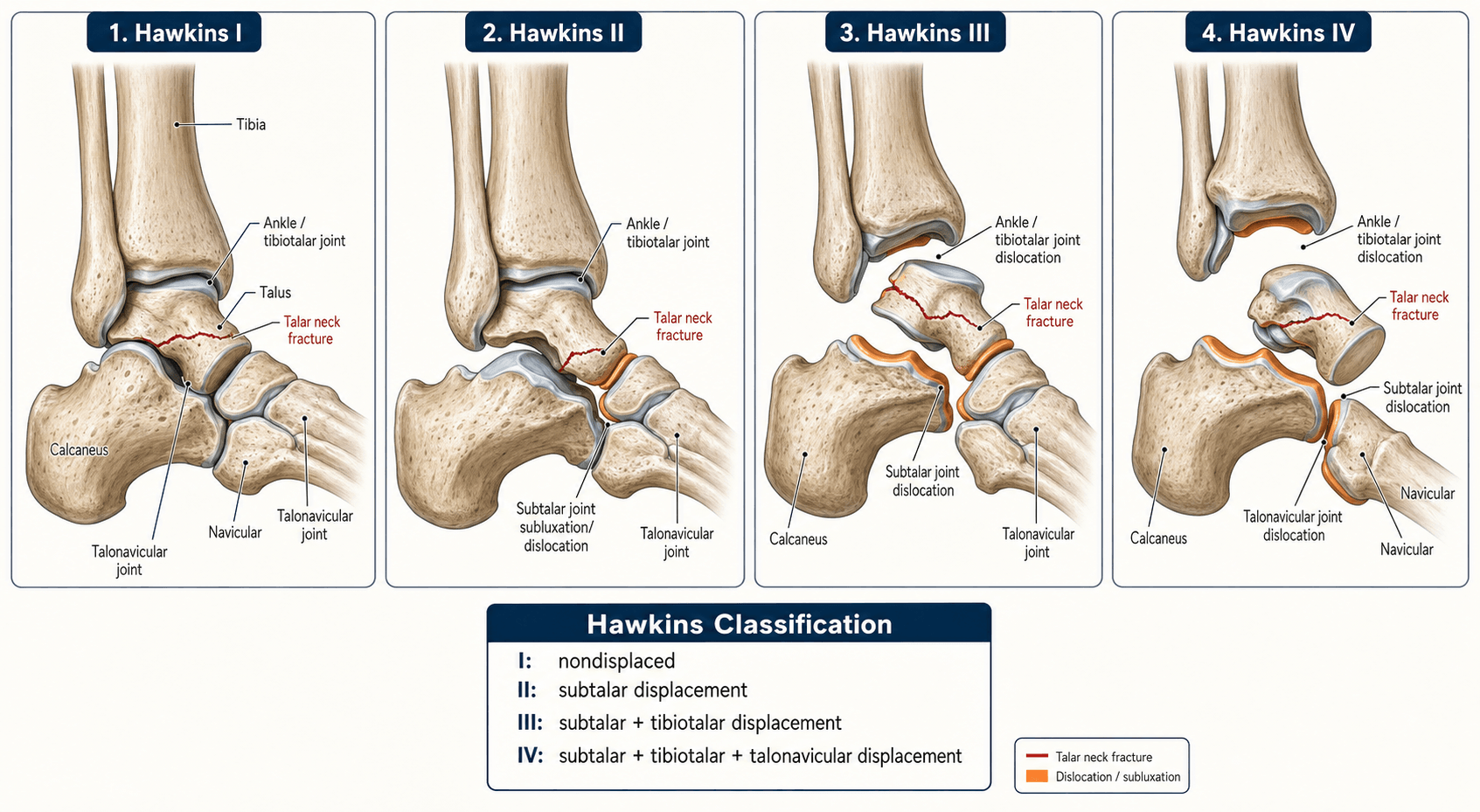
The Hawkins classification (1970), with the Type IV addition by Canale and Kelly (1978), stratifies talar neck fractures by displacement and the pattern of associated peri-talar dislocation. The talus has a precarious, largely retrograde blood supply through the neck, so each step up in grade represents further disruption of that supply and a higher likelihood of avascular necrosis.
- Displacement
- Undisplaced or minimally displaced
- Joint Involvement
- No dislocation
- AVN Rate (Dodd meta-analysis)
- ~10%
- Typical Treatment
- Non-operative (cast) or percutaneous screws in selected patients
- Displacement
- Displaced
- Joint Involvement
- Subtalar subluxation or dislocation
- AVN Rate (Dodd meta-analysis)
- ~27%
- Typical Treatment
- Urgent reduction of the dislocation; internal fixation (screws)
- Displacement
- Displaced
- Joint Involvement
- Subtalar and ankle (tibiotalar) dislocation
- AVN Rate (Dodd meta-analysis)
- ~53%
- Typical Treatment
- Urgent reduction; open reduction and internal fixation (often dual approach)
- Displacement
- Displaced
- Joint Involvement
- Subtalar, ankle, and talonavicular dislocation
- AVN Rate (Dodd meta-analysis)
- ~48%
- Typical Treatment
- Urgent reduction of all dislocated joints plus fixation; salvage planning
None · Sub · Sub+Ankle · Sub+Ankle+NavThe four grades and what they mean
Hook:Each step up adds a dislocated joint and strips more of the talar blood supply — hence the rising AVN risk.
Mechanism of injury is forced dorsiflexion — the talar neck impacts the anterior tibial margin (classically a road-traffic collision with the foot on the dashboard, or a fall from height onto a dorsiflexed foot). The fracture line is typically vertical through the neck, and the body of the talus displaces posteriorly.
A displaced talar neck fracture is a high-energy injury; the examiner wants the wider assessment, not just the grade:
- Open fracture — common in displaced fractures (overall roughly 15–25%, higher in Hawkins III/IV), usually a medial wound from the posteromedially-displaced body; it needs urgent debridement and antibiotics (open fracture and comminution are the factors most associated with AVN — Vallier).
- Talar body extrusion ("missing talus") — the body can be wholly extruded from the wound; current practice generally favours thorough debridement and re-implantation rather than discarding it.
- Skin tenting/necrosis — a posteromedially-displaced body tents the posteromedial skin; urgent reduction relieves the pressure and saves the skin — this, together with reducing the dislocated joints, is the real reason for emergent reduction (not AVN prevention).
- Foot compartment syndrome — high-energy hindfoot trauma can cause it; measure compartment pressures, because a missed compartment syndrome contracts the foot.
- Associated injuries — a medial malleolus fracture frequently accompanies a medial talar neck fracture (and a medial malleolar osteotomy may be used for body access); look also for calcaneal/other foot fractures and ipsilateral limb injuries from the dashboard/fall mechanism, and complete an ATLS survey.
Blood supply of the talus and why AVN happens
The talus has no muscular or tendinous attachments and depends entirely on capsular and ligamentous vessels. Understanding this anatomy explains why AVN rates climb with each Hawkins grade.
- Artery of the tarsal sinus (anastomosis of the lateral tarsal artery and a branch of the perforating peroneal artery): supplies the lateral talar neck and part of the body. Disrupted with subtalar dislocation (type II onwards).
- Deltoid branch of the posterior tibial artery: enters the medial talar body deep to the deltoid ligament. This is the single most important vessel for talar body perfusion and the last remaining supply in high-grade injuries.
- Artery of the tarsal canal (from the posterior tibial artery): the dominant supply to the central talar body, running in the canal between the talar neck and body.
- Superior neck vessels from the anterior tibial (dorsalis pedis) artery: supply the dorsal talar neck and are torn in any displaced neck fracture.
Canal · Deltoid · SinusThe arterial inputs to the talus
Hook:A displaced fracture tears the sinus and dorsal neck vessels; if the deltoid branch survives the body may revascularise — if it is also torn (III–IV), AVN is far more likely.

The talar body is the zone at risk for AVN because its blood supply arrives retrograde through the neck. A displaced talar neck fracture interrupts the primary route, and subtalar dislocation tears the remaining capsular vessels — hence the stepwise AVN risk with increasing Hawkins grade.
The Hawkins sign
The Hawkins sign is a radiographic indicator of revascularisation of the talar dome and, by implication, a reduced likelihood of AVN.
- Appearance: a subchondral radiolucent line in the talar dome, visible on an anteroposterior view of the ankle, typically at 6 to 8 weeks after injury.
- Mechanism: the lucency reflects subchondral resorption (disuse osteopenia) in the revascularised, living talar dome — bone that is dead cannot become osteopenic.
- Interpretation: the Hawkins sign indicates a living blood supply — AVN is unlikely if the sign is present (lucency = life).
- Limitation: absence of the Hawkins sign does not confirm AVN. MRI is the definitive investigation for AVN when clinically suspected, particularly after 8 to 12 weeks. The Hawkins sign is useful but not sufficient on its own.
Lucency = life, at 6–8 weeksRemember the sign
Hook:Present = reassuring; absent = inconclusive (not diagnostic of AVN). Don't reverse the inference.
Examiners frequently ask: "What does absence of the Hawkins sign mean?" The correct answer is that absence does not confirm AVN — it is a non-specific finding. If the Hawkins sign is present, AVN is unlikely; if absent, you need MRI to determine whether AVN has actually developed.
Radiographic assessment

- What It Shows
- Talar neck fracture line; Hawkins sign at 6–8 weeks
- Key Finding
- Medial clear-space widening suggests subtalar involvement
- What It Shows
- Displacement direction (dorsiflexion mechanism), talar body subluxation
- Key Finding
- Posterior displacement of the body
- What It Shows
- Talar neck alignment and comminution
- Key Finding
- The true neck-arch view — best for residual varus
- What It Shows
- Exact geometry, comminution, subtalar and ankle congruity
- Key Finding
- Mandatory pre-operative planning for types II–IV
- What It Shows
- Avascular necrosis and revascularisation patterns
- Key Finding
- Best for AVN at 8–12 weeks post-injury
A talar neck fracture is easily missed on a standard ankle series — the lateral view may show only subtle neck angulation. Obtain a Canale (oblique) view and a CT scan after any high-energy dorsiflexion injury. An undisplaced type I fracture missed on initial films can displace, converting a low-risk injury into a high-risk one.
Management

- 1Reduce dislocations / open wounds urgentlyA dislocated subtalar or ankle joint and any open fracture are reduced/debrided emergently to protect skin and soft tissues — not because emergent fixation lowers AVN.
- 2Image fullyCanale view + CT for geometry, comminution and joint congruity; CT is mandatory for types II–IV planning.
- 3Type I: cast or percutaneous screwsTruly undisplaced fractures: below-knee non-weight-bearing cast 6–8 weeks, or percutaneous screws if any doubt about stability.
- 4Displaced (II–IV): anatomical ORIFHeadless/cannulated screws (± mini-plate); dual anteromedial + posterolateral approach for III–IV. Definitive fixation can wait for soft-tissue swelling to settle.
- Reduction
- None required
- Fixation
- Non-operative cast, or percutaneous screws if any doubt
- Non-weight-bearing
- 6–8 weeks
- AVN monitoring
- Hawkins sign at 6–8 weeks; MRI if concern
- Reduction
- Urgent reduction of the subtalar dislocation
- Fixation
- Headless compression / cannulated lag screws
- Non-weight-bearing
- 8–12 weeks; CT at ~6 weeks to confirm union
- AVN monitoring
- Hawkins sign; MRI at 8–12 weeks
- Reduction
- Urgent reduction; open reduction usually needed
- Fixation
- Screw fixation; dual anteromedial + posterolateral approach; external fixator as a temporising bridge
- Non-weight-bearing
- 10–14 weeks
- AVN monitoring
- MRI at 8–12 weeks; anticipate AVN; discuss salvage early
- Reduction
- Urgent reduction of all dislocated joints
- Fixation
- Neck fixation plus talonavicular reduction/repair; plan for possible salvage
- Non-weight-bearing
- Prolonged; staged reconstruction
- AVN monitoring
- MRI at 8–12 weeks; expect AVN; early MDT planning
Open reduction is indicated whenever closed reduction fails to restore anatomical alignment — common in types III and IV. The anteromedial approach is standard, but a combined anteromedial plus posterolateral (dual) approach gives better visualisation and is recommended for types III and IV. The posterolateral incision sits in the safe interval between the sural nerve and the peroneal tendons.
The examiner pushes past "screws ± plate" to the technical detail and the classic pitfall:
- Screw direction / biomechanics — posterior-to-anterior screws (from the posterolateral talar process across the neck) give the biomechanically strongest construct; anteromedial-to-posterolateral screws are also used and more accessible. Use headless compression screws or countersink the heads to avoid talonavicular/subtalar joint impingement.
- The varus trap — the medial neck is often comminuted, and placing lag (compression) screws across a comminuted medial column shortens it into VARUS (producing forefoot adduction, lateral-column overload and subtalar stiffness). The key pearl: use position (non-lag) screws or a medial mini-fragment BRIDGE plate to span the comminution and maintain length and alignment.
- Mini-plates (medial and/or lateral) are increasingly used for comminuted necks to control alignment, supplemented by temporary K-wires when there is added ligamentous instability (Rammelt).
- Confirm the reduction on the Canale view — restore neck length and alignment rather than over-compressing the comminution.
Complications and salvage
The three major complications are AVN, post-traumatic arthritis, and malunion.
- Avascular necrosis of the talar body: the defining complication, rising with Hawkins grade (meta-analytic rates ~10% type I to ~53% type III). Importantly, partial AVN often revascularises without collapse — in Vallier's series, 37% of patients with radiographic osteonecrosis revascularised without collapse, so only a minority (~31%) developed collapse. If the body collapses, salvage options include tibiotalar arthrodesis (Blair fusion), tibiocalcaneal/tibiotalocalcaneal fusion, talar prosthesis, or (less successfully) talectomy.
- Post-traumatic arthritis: the subtalar joint is affected in most displaced fractures — subtalar arthritis is actually the commonest late sequela (up to ~80% at longer follow-up), often exceeding AVN. The ankle is additionally involved in types III–IV.
- Malunion: varus angulation of the talar neck causes anterior/medial impingement and altered biomechanics; corrected by osteotomy if symptomatic, but technically demanding.
The salvage pathway progresses from conservative (orthoses, activity modification) through isolated arthrodesis (subtalar or ankle) to combined fusion (tibiotalocalcaneal) and ultimately talar replacement or talectomy. Each step sacrifices motion and escalates functional limitation — which is why the index operation (anatomical reduction and stable fixation) matters so much, even though it does not abolish the AVN risk set at the time of injury.
Viva practice
- I undisplaced; II + subtalar; III + ankle; IV + talonavicular (Canale & Kelly).
- AVN rises with grade (~10/27/53/48% by meta-analysis) — Type IV is NOT higher than III; drop the 'approaching 100%' figure.
- AVN is set by the injury (displacement, comminution, open) — surgical timing does not change the AVN rate (Vallier, Rammelt); reduce dislocations/open fractures urgently for the soft tissues.
- Hawkins sign: subchondral lucency at 6–8 weeks = revascularisation; absence is non-specific (get MRI).
- Subtalar arthritis is the commonest late complication, often exceeding AVN.
- Dual approach (anteromedial + posterolateral) for types III–IV.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old motorcyclist presents with a swollen deformed right ankle after a high-speed collision. Radiographs show a displaced fracture through the talar neck with the talar body dislocated posteriorly out of the ankle joint. How would you classify this, what is the mechanism, and how would you manage it?”
“You review a 35-year-old patient 10 weeks after open reduction and internal fixation of a Hawkins type II talar neck fracture. The Hawkins sign is absent on radiographs. The patient has increasing ankle pain and stiffness. What is your differential diagnosis, how would you investigate, and what are the management options?”
Exam cheat sheet
The four types
- Type I: undisplaced talar neck fracture, no dislocation — AVN ~10%
- Type II: displaced neck + subtalar subluxation/dislocation — AVN ~27%
- Type III: displaced neck + subtalar and ankle (tibiotalar) dislocation — AVN ~53%
- Type IV (Canale & Kelly): all three joints dislocated (+ talonavicular) — AVN ~48%
Blood supply
- Artery of the tarsal canal (posterior tibial): dominant supply to the central body
- Deltoid branch of the posterior tibial artery: the medial lifeline — torn in type III/IV
- Artery of the tarsal sinus (lateral): torn with subtalar dislocation (type II onwards)
- Superior neck vessels (anterior tibial/dorsalis pedis): torn in any displaced fracture
Hawkins sign
- Subchondral lucency in the talar dome on AP radiograph at 6–8 weeks
- Lucency = revascularisation — AVN unlikely if present
- Absence does NOT confirm AVN — MRI is required for diagnosis
Management & timing
- Type I: non-operative cast or percutaneous screws
- Types II–IV: anatomical reduction + stable internal fixation; dual approach for III/IV
- Reduce dislocations/open fractures urgently (soft tissue) — but timing of DEFINITIVE fixation does not change AVN rate
- Subtalar arthritis is the commonest late complication, often exceeding AVN
Evidence
Fractures of the neck of the talus
- Proposed the original three-type classification based on displacement and associated dislocation.
- Showed that AVN risk correlates with the grade of displacement/dislocation.
- Described the subchondral radiolucent sign (later named the Hawkins sign) indicating revascularisation.
Fractures of the neck of the talus. Long-term evaluation of seventy-one cases
- 71 talar neck fractures, mean follow-up 12.7 years; good or excellent results in 59%. (This series is credited with adding Type IV.)
- Avascular necrosis occurred in 52% overall — 2 of 13 non-displaced, about half of those with subtalar subluxation/dislocation, and 16 of 19 with complete body dislocation.
- Recommended accurate anatomical reduction (by ORIF if necessary); many AVN cases treated conservatively still did satisfactorily.
Talar neck and body fractures
- Comprehensive review: AVN rates correlate with the degree of INITIAL dislocation, and outcome is determined by injury severity and quality of reduction/fixation.
- The timing of DEFINITIVE internal fixation does not appear to affect the final result (open fractures and dislocations are still emergencies for the soft tissues).
- Only total AVN with talar-body collapse leads to inferior results; prolonged offloading is not indicated for partial AVN.
According to PubMed, the classification and Hawkins sign are from Hawkins 1970 (J Bone Joint Surg Am 1970;52(5):991-1002; PMID 5479485), with Type IV and long-term AVN data (52% overall) from Canale & Kelly 1978 (PMID 417084). Grade-specific AVN rates (I 9.8%, II 27.4%, III 53.4%, IV 48.0%) are from Dodd & Lefaivre 2015 (DOI 10.1097/BOT.0000000000000297). That AVN is determined by injury severity rather than surgical timing comes from Vallier et al. 2004 (no correlation with delay; PMID 15292407) and Rammelt & Zwipp 2009 (DOI 10.1016/j.injury.2008.01.021).