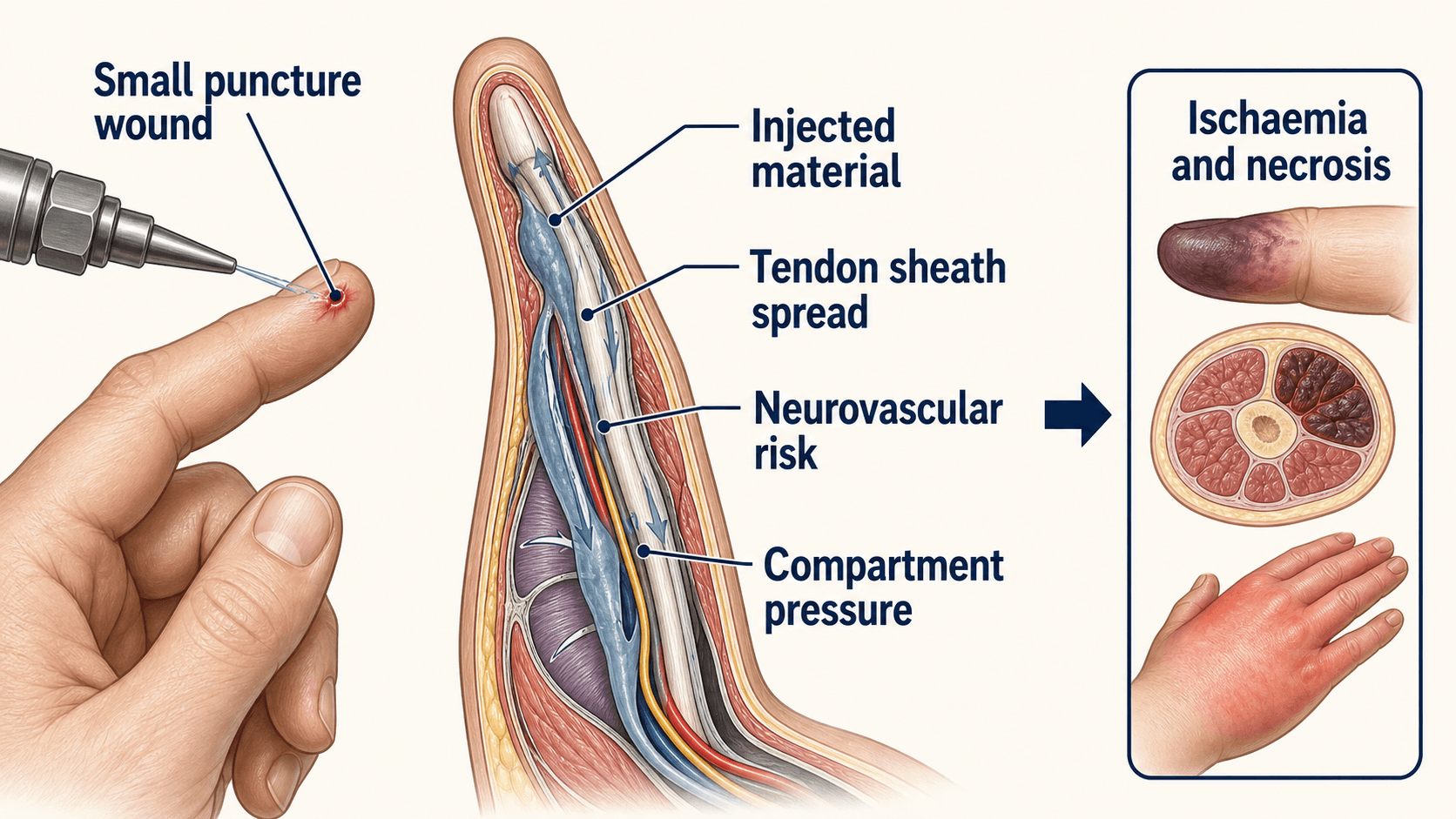
A tiny wound can hide deep contamination, chemical necrosis and compartment pressure
- The skin wound is misleading. The injected material can track far beyond the visible puncture.
- Ask exactly what was injected: paint, thinner, grease, oil, diesel, hydraulic fluid, water, air, gas, cement and adhesives behave differently.
- Pain, swelling, pallor, numbness, crepitus, reduced motion or vascular concern should trigger urgent hand-surgery involvement.
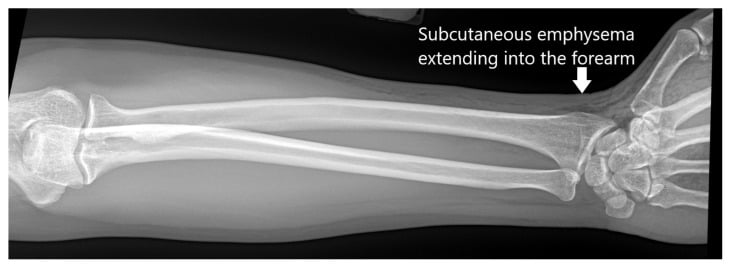
- X-rays are useful even when the wound is tiny: they may show air, radiopaque material, spread into the forearm or foreign-body distribution.
- Most liquid chemical or particulate injections need urgent decompression, wide debridement and removal of material, often with planned second look.
- Steroids remain controversial; they are not a substitute for decompression and debridement when surgical indications are present.
- “The key question is not how small the wound is; it is what was injected, where it went and whether the hand is deteriorating.
- “Paint and solvent injuries are higher risk than small-volume air injection because chemical toxicity drives tissue necrosis.
- “A normal-looking finger early after injury does not exclude deep tendon sheath or neurovascular involvement.
- “If the patient says a pressure washer, grease gun or paint gun injected the hand, treat it as a hand emergency until proven otherwise.
High-Pressure Injection Injury of the Hand
A high-pressure injection injury is not a simple puncture wound. Small entry wound plus pressure device exposure needs urgent assessment, imaging, antibiotics, tetanus review and early hand-surgery discussion.
- Low Concern
- Air or gas, small volume, clinically stable
- High Concern
- Paint, thinner, grease, oil, diesel, cement, adhesive, caustic chemical
- Management Effect
- High-risk materials usually need urgent exploration and debridement
- Low Concern
- Superficial dorsal soft tissue, no spread
- High Concern
- Digit pulp, flexor sheath, palm, web space or carpal tunnel region
- Management Effect
- Closed spaces raise pressure and neurovascular risk
- Low Concern
- Pain improving, normal perfusion, no sensory change
- High Concern
- Escalating pain, swelling, pallor, numbness, stiffness, crepitus
- Management Effect
- Deterioration overrides a small entry wound
- Low Concern
- No gas or foreign material and stable examination
- High Concern
- Air, radiopaque material, proximal tracking or extensive soft-tissue spread
- Management Effect
- Defines extent and supports urgent operative planning
- Low Concern
- Immediate presentation with reassuring serial exams
- High Concern
- Delayed recognition or delayed specialist review
- Management Effect
- Delay increases necrosis, infection, stiffness and amputation risk
WOUNDRecognition | MATERIALRisk | OPENTreatment |
|---|---|---|
W Weapon Identify the pressure device: paint gun, grease gun, pressure washer, air line or industrial injector. | M Mixed solvents Thinner and oil-based paint are highly toxic. | O Operate if high-risk Liquid toxic material, compartment signs or deterioration need urgent decompression and debridement. |
O Object injected Material toxicity drives prognosis more than the puncture size. | A Adhesives Sealants and cement can harden or adhere to tissue. | P Protect Analgesia, elevation, tetanus, broad antibiotics and neurovascular documentation. |
U Under the skin Material tracks through tendon sheaths, neurovascular planes and compartments. | T Tendon sheath Flexor sheath spread makes closed-space damage worse. | E Explore extent Incise along safe hand-surgery approaches to remove material and release pressure. |
N Nerve and vessel status Document sensation, perfusion and capillary refill early. | E Emphysema Gas or air may be visible on X-ray and still needs serial examination. | N Next look Plan second look, wound care, therapy and reconstruction when required. |
D Do not delay Early hand-surgery review is the safe default. | R Reoperation Serial debridement is common when material remains or necrosis declares. | |
The wound underestimates the injury. | Material matters. | Open the threatened hand. |
Overview and Epidemiology
High-pressure injection injury of the hand occurs when material from an industrial or domestic pressure device is forced through the skin into the deep soft tissues. The classic setting is a working-age person using a paint gun, grease gun, diesel or hydraulic system, pressure washer, air line, refrigerant line, concrete sealant or adhesive injector.
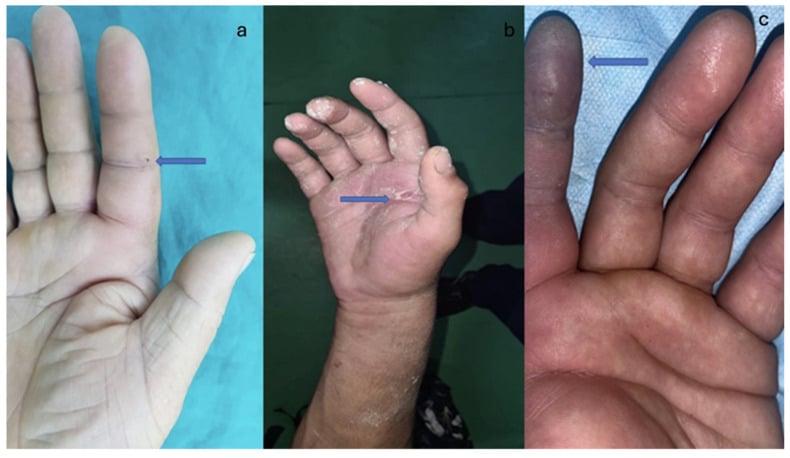
The entry wound may look harmless. That is the danger. Injected material spreads along low-resistance paths such as tendon sheaths, fascial planes and neurovascular bundles. Tissue injury then comes from a combination of mechanical pressure, vascular compression, chemical toxicity, inflammatory oedema, infection and delayed necrosis.
The most common teaching trap is calling it a puncture wound. The more accurate first sentence is: "This is a high-pressure injection injury until proven otherwise, and the hand can deteriorate even if the skin wound is small."
Pathophysiology and Anatomy
The injury has three simultaneous components:
- Mechanical injection: a narrow jet penetrates skin and drives material into tissue under pressure.
- Closed-space spread: injected material follows tendon sheaths, neurovascular bundles, palmar spaces and fascial compartments.
- Biological toxicity: solvents, paint, petroleum products, cement, adhesives and caustic materials cause inflammation, oedema, thrombosis and tissue necrosis.
The hand is vulnerable because it has multiple small compartments, tight tendon sheaths and important digital neurovascular structures. A digital injection can track proximally into the palm; a palmar injection can threaten intrinsic compartments, carpal tunnel structures and digital vessels. Air or gas may dissect widely into the forearm, producing impressive radiographs but sometimes less chemical necrosis than paint or solvent.
They combine pressure injury with chemical tissue toxicity. Oil-based paint, thinner and solvent mixtures can produce progressive necrosis even after the first debridement.
Gas may track widely and cause emphysema, but selected patients without pain, vascular compromise or compartment signs can sometimes be observed with serial examination.
Injection Pressure and Penetration
The skin is a surprisingly weak barrier under a focused jet. Intact skin can be breached by a stream of as little as about 7 bar, roughly 100 psi, which is far below the output of any industrial device. Once the skin is breached, the same pressure that penetrated keeps driving material along the path of least resistance, so a higher delivery pressure usually means a larger injected volume, wider tissue spread and more proximal tracking. This is why injection pressure is listed as a prognostic factor alongside the type, amount and temperature of the material, and why the device should always be identified.
- Typical Pressure
- Several hundred up to several thousand psi, sometimes over 10,000 psi
- Practical Implication
- Combines high pressure with chemical toxicity; wide spread and necrosis risk
- Typical Pressure
- Can exceed 10,000 psi
- Practical Implication
- Drives dense retained material far along tissue planes
- Typical Pressure
- Often several thousand psi
- Practical Implication
- Deep penetration with toxic petroleum material
- Typical Pressure
- Often around 1,000 to 4,000 psi
- Practical Implication
- Deep contamination, possible water or gas tracking even without obvious chemical toxicity
- Typical Pressure
- About 7 bar, roughly 100 psi
- Practical Implication
- Any of the devices above vastly exceeds the pressure needed to breach skin
A device needs only about 100 psi to breach skin, and industrial guns generate many times that, so a small painless wound from a high-output device implies deep, wide deposition until imaging and serial examination prove otherwise. Higher injection pressure correlates with greater spread and worse prognosis.
Routes of Deep Spread: Palmar Spaces and Parona's Space
The hand's deep potential spaces explain why a digital or palmar injection can end up in the forearm: injected material follows the same planes that surgeons and infections use.
The flexor tendon sheaths of the index, middle and ring fingers usually end near the distal palmar crease, but the little finger sheath is continuous with the ulnar bursa and the thumb sheath, carrying flexor pollicis longus, is continuous with the radial bursa. Material injected into a thumb or little-finger sheath therefore reaches the deep palm directly. The two deep palmar spaces, the thenar space volar to adductor pollicis and the midpalmar space deep to the flexor tendons of the medial fingers, are separated by an oblique palmar septum and can each collect material under pressure. Proximally, the radial and ulnar bursae extend toward the wrist; when they communicate, a horseshoe pattern links thumb and little-finger involvement. The final common route is Parona's space, the potential space in the distal volar forearm between pronator quadratus deeply and the flexor digitorum profundus tendons superficially, into which the bursae can decompress.
- Location
- Digital; thumb sheath continuous with radial bursa, little finger with ulnar bursa
- Why It Matters in Injection Injury
- Material tracks proximally from the digit into the deep palm
- Location
- Volar to adductor pollicis, radial to the oblique septum
- Why It Matters in Injection Injury
- Closed space where pressure and material collect, threatening thumb and index
- Location
- Deep to the medial flexor tendons, ulnar to the oblique septum
- Why It Matters in Injection Injury
- Closed space communicating toward the carpal tunnel and median nerve
- Location
- Deep palm, extending to the wrist
- Why It Matters in Injection Injury
- Horseshoe communication links thumb and little finger and forms a conduit to the forearm
- Location
- Distal volar forearm, between pronator quadratus and the profundus tendons
- Why It Matters in Injection Injury
- Final common route for proximal tracking from hand into forearm
The thumb and little-finger flexor sheaths are continuous with the radial and ulnar bursae, which can decompress into Parona's space in the distal forearm. This continuity is why proximal forearm spread on the radiograph is anatomically expected rather than surprising, and why operative exposure must be planned to follow material beyond the hand.
Classification and Risk Groups
- Typical Problem
- High chemical toxicity, oedema, necrosis, stiffness, amputation risk
- Initial Strategy
- Urgent hand-surgery debridement and removal of material
- Typical Problem
- Persistent foreign material, inflammation, infection, tendon sheath spread
- Initial Strategy
- Usually urgent debridement; expect difficult material removal
- Typical Problem
- Caustic injury, hardening material, deep tissue infiltration
- Initial Strategy
- Urgent debridement and serial reassessment
- Typical Problem
- Deep contamination, tendon sheath infection, compartment syndrome possible
- Initial Strategy
- Individualise: close observation or debridement depending clinical course
- Typical Problem
- Subcutaneous emphysema, pressure effect, possible compartment syndrome
- Initial Strategy
- Serial examination if stable; decompress if compartment or vascular concern
Clinical Assessment
The history must be specific because the material and device change prognosis.
Ask:
- What device caused the injury: paint gun, grease gun, pressure washer, air line, hydraulic hose, refrigerant line, cement or sealant injector?
- What substance entered the hand: paint type, thinner, solvent, oil, diesel, grease, water, air, gas, cement, adhesive or unknown chemical?
- What was the pressure setting if known?
- Which hand, which digit, which side of the digit and whether it was the dominant hand?
- Time since injury and whether symptoms are worsening.
- First aid, washout, antibiotics, tetanus status and transfer delays.
- Worksite safety data sheet availability for chemicals.
Examination should be repeated and documented:
- Look: puncture site, swelling, discolouration, blistering, pallor, crepitus, tracking into palm or forearm.
- Feel: tenderness, tense compartments, temperature difference and crepitus.
- Move: active and passive digital motion; pain with passive stretch; tendon function.
- Neurovascular: capillary refill, colour, pulp sensation, two-point discrimination if possible, median and ulnar nerve symptoms.
- Compare: opposite hand and adjacent digits.
The entry wound often looks smaller than the injury. Reassurance is unsafe unless the material, imaging, perfusion, sensation, pain pattern and serial examinations are all reassuring.
Investigations and Imaging
Plain radiographs are the first imaging test. Order hand radiographs centred on the injured area and extend to the forearm if there is swelling, crepitus, proximal pain or suspected gas tracking.
Radiographs may show:
- subcutaneous emphysema from air or gas injection
- radiopaque paint, lime, cement or foreign material
- proximal tracking beyond the visible entry wound
- fracture, retained foreign body or soft-tissue swelling
Ultrasound may help show soft-tissue infiltration in selected settings, but it should not delay operative care when the hand is deteriorating. CT can show gas or spread into the forearm. MRI can define material extent in unusual delayed cases, but it is not a routine preoperative test when urgent debridement is indicated.

Differential Diagnosis
The injury is most often misclassified as a trivial puncture. The safer mindset is to actively exclude the conditions that share its early appearance but demand very different management.
- Overlapping Feature
- Tiny puncture, working-age patient
- Discriminating Feature
- History of paint gun, grease gun, pressure washer or air line; deep pain out of proportion
- Why It Matters
- Surgical emergency; debride high-risk liquids early
- Overlapping Feature
- Small entry wound
- Discriminating Feature
- Low-pressure mechanism, no jet device, minimal deep spread
- Why It Matters
- Usually wound care and tetanus only
- Overlapping Feature
- Painful swollen digit, pain on motion
- Discriminating Feature
- Kanavel signs, infective rather than injection history, slower onset
- Why It Matters
- Urgent washout but driven by sepsis, not material toxicity
- Overlapping Feature
- Pain out of proportion, systemic upset, crepitus
- Discriminating Feature
- Rapid systemic sepsis, skin necrosis, gas from organisms not from injected air
- Why It Matters
- Emergent radical debridement and resuscitation
- Overlapping Feature
- Puncture plus radiopaque material on X-ray
- Discriminating Feature
- Single retained object rather than a tracking jet of material
- Why It Matters
- Local exploration and removal, less compartment risk
- Overlapping Feature
- Tense painful hand, pain on passive stretch
- Discriminating Feature
- Crush mechanism without injection device
- Why It Matters
- Fasciotomy driven by pressure, not material removal
Crepitus after an injection injury usually reflects injected air or gas, not gas-forming organisms. Distinguish it from necrotising infection by the mechanism, the absence of fulminant systemic sepsis early, and the radiographic distribution along injection planes.
Management Algorithm
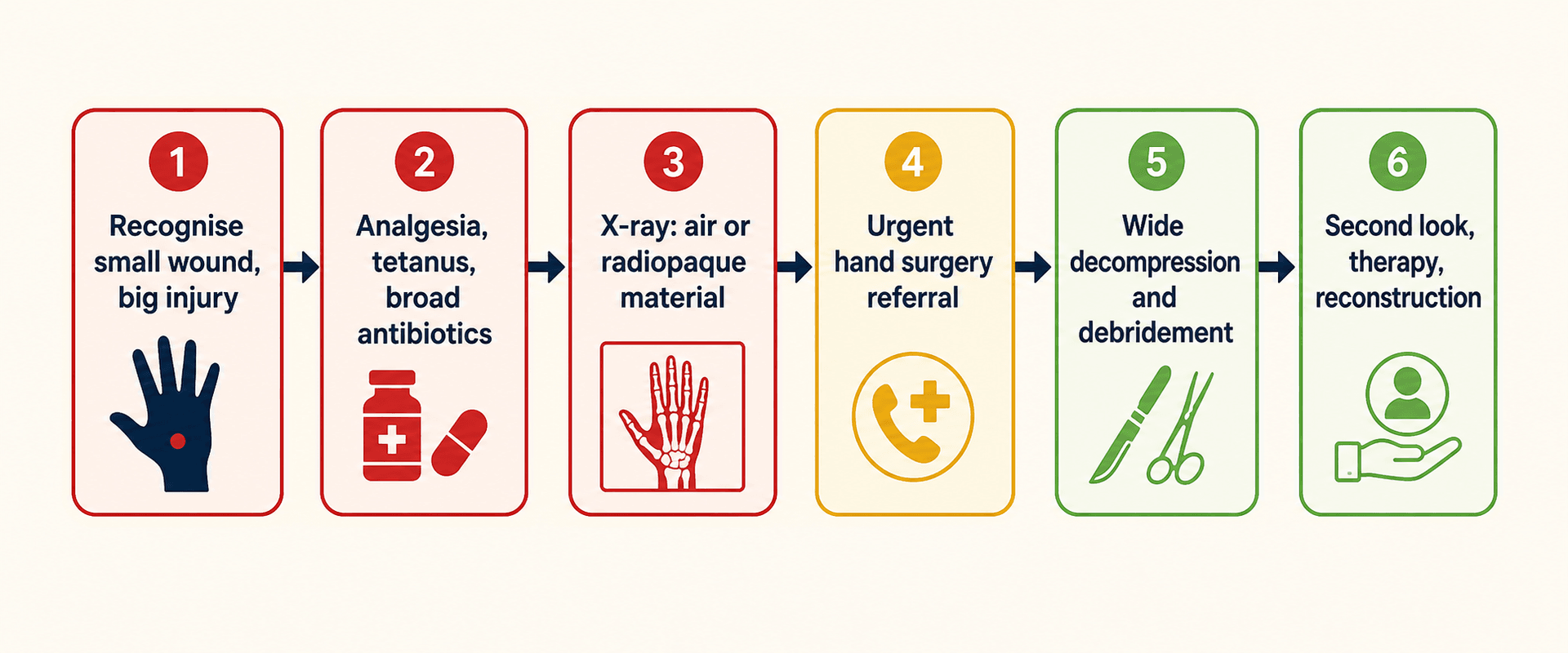
Initial management:
- Treat as a surgical emergency until a hand surgeon has assessed the risk.
- Remove rings, watches, gloves and constrictive dressings.
- Give analgesia.
- Check tetanus status.
- Start broad-spectrum antibiotics according to local open-injury policy.
- Keep the patient fasting if debridement is likely.
- Elevate but avoid tight compression.
- Obtain X-rays of the hand and forearm as indicated.
- Obtain the material safety data sheet or product label when possible.
- Discuss immediately with hand surgery.
Surgical Technique
Principles before incision:
- Review the material, pressure mechanism, time from injury and imaging.
- Document neurovascular status before anaesthesia if possible.
- Plan incisions that expose the injection track and allow decompression of threatened closed spaces.
- Use regional or general anaesthesia depending patient and urgency.
- Prepare the whole hand and forearm if proximal tracking is possible.
- Use tourniquet judgement: a bloodless field helps material removal, but perfusion must be assessed after release.
Complications
Complications are common because the injury damages tissue before the wound looks severe.
- Mechanism
- Injected volume, oedema, closed-space pressure
- Prevention or Response
- Early recognition, decompression and serial examination
- Mechanism
- Vascular compression, chemical toxicity, thrombosis
- Prevention or Response
- Urgent debridement, perfusion monitoring and staged necrosis management
- Mechanism
- Contamination, devitalised tissue, retained material
- Prevention or Response
- Antibiotics, debridement, cultures when indicated
- Mechanism
- Inflammation, sheath damage, immobilisation, scarring
- Prevention or Response
- Early supervised hand therapy once safe
- Mechanism
- Nerve irritation, scarring, ischaemia
- Prevention or Response
- Document baseline and counsel long recovery
- Mechanism
- Severe toxicity, delayed treatment, necrosis or infection
- Prevention or Response
- Early recognition and complete debridement reduce risk but cannot eliminate it
Postoperative Care and Rehabilitation
Postoperative care is active treatment, not an afterthought.
Early priorities:
- elevate and monitor swelling
- repeat neurovascular examinations
- inspect wounds and plan second look if needed
- continue antibiotics based on material, contamination and cultures
- protect exposed tendons, nerves and vessels
- maintain safe splinting position
- start hand therapy as soon as tissue safety allows
Rehabilitation focuses on tendon gliding, oedema control, scar management, sensory recovery and return-to-work planning. Many patients have residual stiffness, pain, sensory symptoms or reduced grip, even after timely surgery.
Outcomes and Prognosis
Outcome depends on material, injection location, volume, pressure, time to debridement, infection, vascular compromise and completeness of material removal.
Paint, solvent and oil-based material have historically been associated with high morbidity. Contemporary series suggest outcomes may be improving, particularly for some latex-based paints, but this should not make the initial assessment casual. The safe position remains: high-risk material needs early surgical assessment and likely debridement.
Prognostic factors to state clearly:
- substance toxicity
- volume and pressure
- digit versus palm location
- delay to recognition
- delay to debridement when indicated
- infection or compartment syndrome
- need for serial operations
- ability to start rehabilitation
Guidelines, Registries & Global Practice
High-pressure injection injury is rare but globally consistent: it is overwhelmingly an occupational injury of working-age men, classically affecting the non-dominant index finger, with grease and paint the commonest materials worldwide. Because it is uncommon there is no dedicated arthroplasty-style registry; evidence comes from single-centre series and pooled literature reviews across multiple countries.
- Emphasis
- Emergency hand-trauma pathways and prompt specialist referral
- Practical Point
- Treat as a hand emergency; early hand-surgery involvement and tetanus and antibiotic cover
- Emphasis
- Risk stratification by injected material and time to debridement
- Practical Point
- Organic solvents and grease usually need emergent wide debridement, ideally within hours
- Emphasis
- Specialist hand-unit management and staged reconstruction
- Practical Point
- Low threshold for second look and microsurgical reconstruction
- Emphasis
- Education and prevention in industrial and resource-limited settings
- Practical Point
- Worker awareness and early transfer reduce delay-related amputation
High- versus limited-resource practice variation. In well-resourced systems the standard is urgent imaging, early specialist debridement, planned second look and structured hand therapy. In limited-resource or remote settings the dominant problem is delayed recognition and delayed transfer, which drives higher necrosis, infection and amputation rates. The single most transferable intervention everywhere is early recognition of the mechanism and rapid referral, rather than any specific implant or technology.
Documentation that carries value anywhere: the material, device and pressure, time of injury, neurovascular findings, imaging, treatment delay, hand-surgery discussion and rehabilitation plan. Antibiotic choice, tetanus prophylaxis and chemical-toxicity advice should follow local emergency, infectious-disease and poison-information protocols, supported by the product label or safety data sheet when available.
Controversies and Areas of Uncertainty
This is a rare injury with no randomised trials, so much of the evidence is Level IV-V and several questions remain genuinely open.
Steroids are proposed to limit the inflammatory necrosis of solvent injuries, but the largest pooled review (Hogan and Ruland, 435 cases) found no effect on amputation or infection. They are at best a selective adjunct and never a substitute for decompression and debridement.
Debridement within 6 hours is repeatedly linked to limb salvage for organic solvents, but this is derived from retrospective pooled data. It should drive urgency, not be misread as a hard threshold that makes later surgery futile.
Historical series quote amputation around 30 percent, while recent single-institution data report rates near 2 percent, partly attributed to modern latex-based paints. The optimism is real but rests on small contemporary cohorts; high-risk material still warrants aggressive treatment.
Selected air, gas or low-pressure water-jet injuries without compartment or vascular concern can be observed, but the boundary is judgement-based. Reliable serial examination and senior hand-surgery agreement are mandatory before choosing non-operative care.
MCQ Practice Points
Q: What is the key danger of a tiny puncture wound after pressure-device exposure? A: The visible wound may be minor while injected material has tracked deeply and proximally through the hand.
Q: Which injected materials should raise immediate concern? A: Paint, thinner, solvent, grease, oil, diesel, cement and adhesives because chemical toxicity and retained material drive necrosis.
Q: Why are plain radiographs useful? A: They may show subcutaneous air, radiopaque material or proximal spread, but a normal X-ray does not rule out toxic liquid infiltration.
Q: Are antibiotics alone adequate for a deteriorating high-risk injection injury? A: No. Decompression, removal of injected material and debridement are the key interventions when indicated.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A painter presents with a tiny puncture wound on the index finger after a high-pressure paint gun injury. The finger is mildly swollen.”
“A patient has a pressure washer injury with hand crepitus and radiographic gas extending into the forearm, but perfusion and sensation are normal.”
“A mechanic presents 24 hours after grease gun injection into the palm with increasing pain, swelling and numbness.”
Recognise
- Pressure device plus hand wound is a hand emergency until proven otherwise.
- Skin wound can be tiny and painless.
- Ask material, pressure, time, location and safety data sheet.
Assess
- Pain, swelling, crepitus, colour, capillary refill and sensation.
- Active and passive motion; pain with passive stretch.
- X-ray hand and forearm if gas or proximal spread is suspected.
Treat
- Remove constriction, analgesia, tetanus, broad antibiotics.
- Urgent hand-surgery consultation and fasting if operation likely.
- High-risk liquid or particulate materials usually need debridement.
Operate
- Excise entry wound and follow the track.
- Release threatened compartments and tendon sheaths.
- Remove material and non-viable tissue.
- Leave open or plan second look when viability is uncertain.
Warn
- Compartment syndrome, necrosis, infection and amputation.
- Stiffness, tendon adhesions, sensory loss and chronic pain.
- Repeat surgery and prolonged hand therapy may be required.
Evidence Base
Current treatment concepts
- Classic presentation is a puncture wound on the non-dominant index finger of a working-age man in his mid-thirties.
- Initial care: tetanus prophylaxis, broad-spectrum antibiotics and urgent hand-surgery consultation; best outcomes when liquid injections are debrided within 6 hours.
- Air, gas or small amounts of veterinary vaccine may be observed with serial examination only when there is no compartment concern; organic and caustic materials carry higher amputation rates.
435-case literature review of upper-limb injection injury
- Across 435 pooled cases the overall amputation rate was 30 percent; organic-solvent injection into the fingers carried the highest risk, while thumb or palm injections had far lower tissue loss.
- Wide debridement within 6 hours significantly reduced amputation risk after organic-solvent injection.
- Adjuvant steroids did not change the amputation rate or infection incidence.
Fourteen-year descriptive study (32 hand cases)
- Among 32 cases, grease was the most common injected material (53 percent), followed by paint (25 percent); mean age 32.7 years.
- The palm (31 percent) and index finger (25 percent) were the commonest sites; mean presentation delay was 12 hours.
- Debridement was performed in 91 percent; chronic pain occurred in 9 percent and amputation in 3 percent, with delay linked to amputation risk.
Surgical outcomes series (14 cases, 2-year follow-up)
- Across 14 surgically treated injuries, prognostic factors were the type, amount and temperature of material and the injection pressure.
- Ten required debridement and foreign-body removal, six needed reconstructive microsurgery and one underwent digital-tip amputation.
- Paint, automotive grease, solvents and diesel oil were the typical industrial substances.
Revisiting amputation rates (53 cases, 2007-2023)
- Among 53 cases at a level-1 trauma centre the amputation rate was only 2.2 percent, far below the historical 30 percent figure.
- Latex-based paints showed more favourable outcomes than grease or oil-based paints, with fewer reoperations and complications.
- Evolution of paint formulations may underlie the more optimistic contemporary prognosis.
Solvent injection, local toxicity and the steroid debate
- Dry-cleaning solvents (isoparaffinic hydrocarbons, methoxypropanol, dichlorofluoroethane) cause severe local tissue necrosis despite limited systemic toxicity, often leading to digit loss.
- Recommended treatment is prompt surgical exploration, careful debridement and irrigation, and intravenous antibiotics.
- High-dose systemic corticosteroids were suggested only as a selective adjunct, never a substitute for surgery.