Posterolateral humeral head impression fracture | 40-90% of anterior dislocations
CLASSIFICATION SYSTEMS
Critical Must-Knows
- Impression fracture of posterolateral humeral head from anterior glenoid rim
- Engaging vs Non-engaging lesions (dynamic evaluation)
- Glenoid Track Concept: less than 83% width rule
- Remplissage: Infraspinatus capsulotenodesis for off-track lesions
- Associated with Bankart lesions (bipolar bone loss)
Clinical Pearls
- "Look for 'engaging' lesion on exam (Apprehension at lower abduction angles)
- "Stryker Notch View is best X-ray
- "CT with 3D reconstruction is gold standard for quantification
- "Always calculate the Glenoid Track
Clinical Imaging
Axial CT Demonstration

3D CT Reconstruction

MRI Findings

Reverse Hill-Sachs (Posterior Instability)
Engaging Hill-Sachs on CT
Critical Exam Failures
Terminology Trap
Do not confuse 'engaging' with 'off-track'. Engaging is a clinical finding (locking). Off-track is a radiographic calculation. They are related but distinct concepts.
Missed Bipolar Loss
Failure to account for glenoid bone loss. Track = 0.83D - d. If you ignore 'd' (glenoid defect), you will misclassify an unstable lesion as stable.
Surgical Indication
Suggesting Bankart repair alone for Off-Track. This has a high recurrence rate. Off-Track lesions require Remplissage or Latarjet.
Imaging View
Forgetting the Stryker Notch view. Or failure to request AP in internal rotation. Standard AP often misses the posterolateral defect.
At a Glance
| Feature | Hill-Sachs Lesion |
|---|---|
| Pathology | Compression fracture of posterolateral humeral head |
| Mechanism | Anterior dislocation (impaction on glenoid rim) |
| Key View | Stryker Notch View (X-ray), Axioscapular (CT) |
| Critical Metric | Glenoid Track (Off-track = unstable) |
| Treatment | Remplissage (if off-track) or Latarjet (if glenoid loss) |
HRHill-Sachs vs Reverse
| H | Hill-Sachs Posterolateral (Anterior disloc) |
| R | Reverse Anteromedial (Posterior disloc) |
| H | Hill-Sachs Posterolateral (Anterior disloc) |
| R | Reverse Anteromedial (Posterior disloc) |
Hook:Hills are at the Back (Posterior), Reverse is Front
FIRemplissage Meaning
| F | Fill Fills the defect |
| I | Infraspinatus Tendon used |
| F | Fill Fills the defect |
| I | Infraspinatus Tendon used |
Hook:Fill-Sachs Lesion with Infraspinatus
83Track Calculation
| 8 | 83% Percentage of glenoid width |
| 3 | Minus d Subtract defect width |
| 8 | 83% Percentage of glenoid width |
| 3 | Minus d Subtract defect width |
Hook:83% is the magic number for Track
Overview and Epidemiology
Hill-Sachs lesions are compression fractures of the posterolateral humeral head resulting from impact against the anterior glenoid rim during anterior shoulder dislocation. They represent a key component of "bipolar bone loss" in shoulder instability.
Epidemiology
- Primary Dislocation: Present in 40-50% of cases.
- Recurrent Instability: Present in up to 90-100% of cases.
- Mechanism: Anterior dislocation with the arm attempting to internally rotate.
- Significance: Large or "off-track" lesions engage with the glenoid rim, causing levering out and recurrent dislocation.
Pathophysiology and Mechanisms
Pathomechanics
- Location: Posterolateral aspect of the humeral head, superior to the greater tuberosity.
- Formation: "Dent" created when the soft cancellous bone of the humeral head impacts the hard cortical bone of the anterior glenoid rim during dislocation.
- Bipolar Bone Loss: The interaction between the Hill-Sachs lesion and any anterior glenoid bone loss (bony Bankart). The combined loss reduces the arc of stability.
- Engagement Mechanism: In abduction and external rotation (the "at-risk" position), the perceived width of the glenoid track narrows. If the Hill-Sachs lesion is wide enough to bridge this narrow track, the anterior glenoid rim falls into the defect. This levering action forces the humeral head out of the socket.
The Glenoid Track Concept (Itoi, DiGiacomo)
The "Glenoid Track" is the contact zone of the glenoid on the humeral head during abduction and external rotation. It essentially describes the "safe zone" on the humeral head that stays in contact with the glenoid.
Clinical Calculation Steps:
- Measure Glenoid Diameter (D): Use the inferior circle method on en-face 3D CT.
- Calculate Expected Track:
0.83 x D. - Measure Glenoid Defect (d): Linear width of anterior bone loss.
- Calculate True Track Width:
Glenoid Track = (0.83 x D) - d. - Measure Hill-Sachs Interval (HSI): Distance from the rotator cuff footprint to the OTHER side of the Hill-Sachs lesion (medial margin).
- Compare:
- If HSI less than Track: The lesion is covered by the glenoid. ON-TRACK.
- If HSI greater than Track: The lesion extends beyond the glenoid rim. OFF-TRACK.
Zone of Co-existence: The concept relies on the fact that the rotator cuff footprint defines the lateral margin of the contact patch. A Hill-Sachs lesion expands this "non-contact" zone medially.
Classification Systems
The Gold Standard for Surgical Decision Making
| Category | Definition | Implication |
|---|---|---|
| On-Track | Lesion width is within the glenoid track (less than 83% - glenoid defect) | Does not engage. Standard Bankart repair usually sufficient. |
| Off-Track | Lesion width extends medial to the glenoid track | Engages anterior rim in abduction/ER. Needs Remplissage or Latarjet. |
Formula: Track = (0.83 x D) - d (where D=Glenoid Diameter, d=Glenoid Bone Loss)
Clinical Assessment
History
- History of recurrent anterior dislocations.
- Feeling of the shoulder "locking" or getting stuck in abduction/external rotation.
- Mechanism typically traumatic abduction/external rotation.
Physical Examination
- Apprehension Test: Positive in abduction and external rotation.
- Relocation Test: Relief of apprehension with posterior force.
- Crepitus: May feel crepitus in the mid-range of rotation if the lesion is large.
- Engaging Sign: Reproducing symptoms (clunk/apprehension) at lower degrees of abduction may suggest an engaging lesion.
Investigations
X-Ray
- Views: AP (Internal Rotation), Axillary, Stryker Notch View.
- Stryker Notch: Hand on head, beam tilted 10° cephalad. Best view for Hill-Sachs.
- West Point: Best for glenoid bone loss.
CT Scan
- Gold Standard for quantifying bone loss.
- Protocol: 3D reconstruction with humeral head subtraction (en face view).
MRI
- Useful for soft tissue pathology (Bankart, rotator cuff tears).
- Can estimate bone loss but CT is superior.
- Axial cuts: Visualize the depth of the lesion.
Differential Diagnosis
A posterolateral humeral head defect or a "locking/apprehensive" shoulder is not always a true engaging Hill-Sachs lesion. Distinguish it from the following:
Differentiating the Posterolateral Humeral Defect
| Entity | Mechanism / Location | Key Distinguishing Feature |
|---|---|---|
| Hill-Sachs lesion | Posterolateral head, anterior dislocation | Impaction on ANTERIOR glenoid rim; pairs with Bankart lesion |
| Reverse Hill-Sachs (McLaughlin) | Anteromedial head, posterior dislocation | Locked internal rotation, classic seizure/electrocution/posterior trauma history |
| Normal bare area / cartilage notch | Posterolateral, physiological | Smooth, at/above cuff footprint, no subchondral break — do not over-call as pathological |
| Osteochondral defect / AVN | Variable head location | Marrow oedema or collapse on MRI, atraumatic or steroid/alcohol history |
| Atraumatic / multidirectional instability | No bony defect | Sulcus sign, hyperlaxity (Beighton), bilateral, no Hill-Sachs |
| Bony Bankart (glenoid-sided) | Anteroinferior glenoid rim fracture | Glenoid defect drives instability; humeral lesion may be small |
Controversies and Areas of Uncertainty
- The 83 percent figure is a population mean, not a hard threshold. The original cadaveric track was 84 plus or minus 14 percent of glenoid width (Yamamoto/Itoi 2007); the working 0.83 multiplier is a convenient approximation. Borderline (near-track) lesions sit in a grey zone where intraoperative dynamic assessment still matters.
- Does off-track status independently predict failure, or is glenoid loss the real driver? Long-term data (Schwihla 2022) show off-track lesions fail isolated Bankart repair at high rates, yet some cohorts (Park 2019) found glenoid defect size, not off-track status per se, was the more reliable predictor once selective remplissage was used. The honest position: bipolar interaction matters, and glenoid loss carries heavy weight.
- Remplissage vs Latarjet for subcritical loss. Meta-analytic data (Haroun 2020) show equivalent stability with fewer complications for remplissage, but Latarjet retains advocates for collision athletes and revision settings. There is no consensus "right answer" — the decision is patient- and surgeon-specific.
- The "subcritical" glenoid threshold is moving. Older teaching used 20 to 25 percent; contemporary work suggests instability and recurrence rise from as little as 13.5 percent in high-demand athletes, lowering the threshold for augmentation.
- Clinical engagement vs radiographic off-track are correlated but not identical. A lesion can be radiographically off-track yet not reproduce clinical locking, and vice versa; relying on one alone risks over- or under-treatment.
Management Algorithm
Step 1: Calculate Glenoid Bone Loss
- Greater than 20-25% Glenoid Loss: Latarjet Procedure (regardless of Hill-Sachs)
- Less than 20-25% Glenoid Loss: Proceed to Step 2 (Check Track)
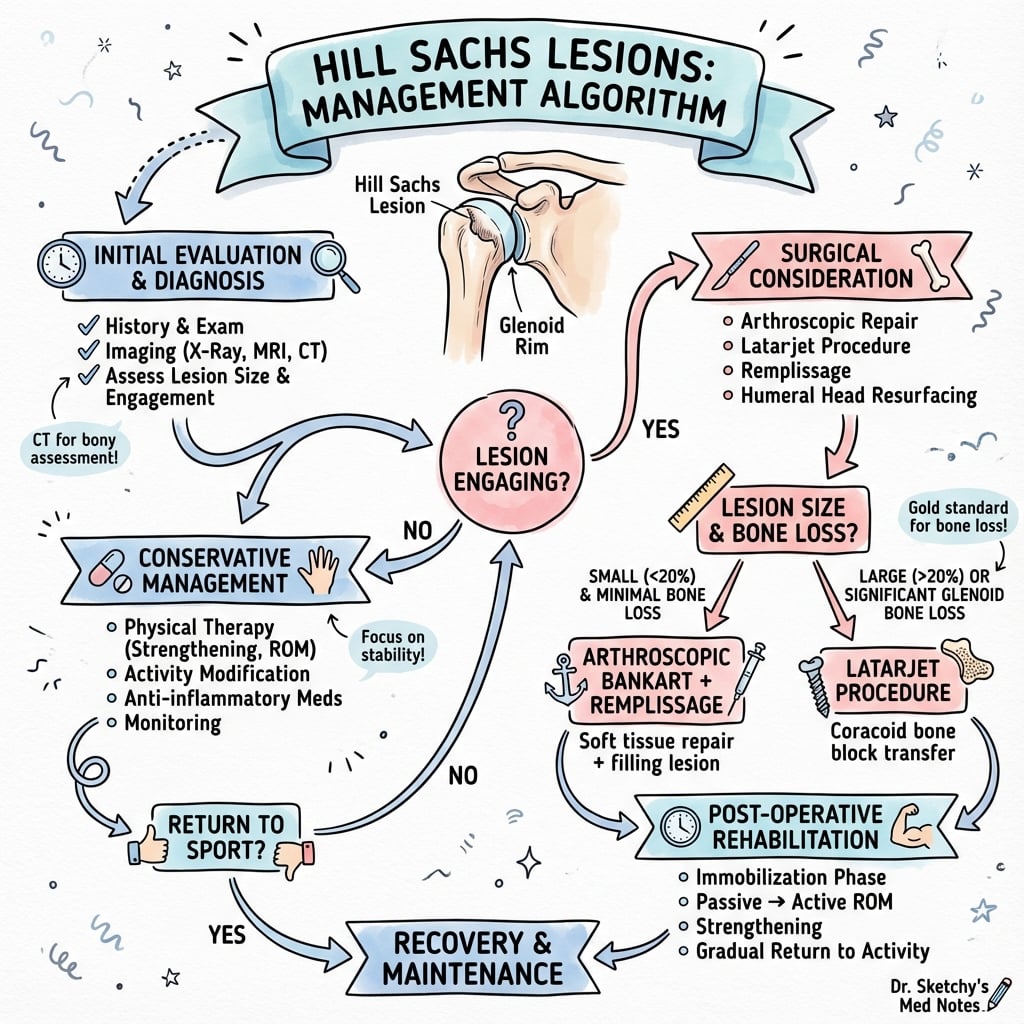
Step 2: Check Glenoid Track (Hill-Sachs)
- On-Track Lesion: Arthroscopic Bankart Repair alone.
- Off-Track Lesion: Arthroscopic Bankart Repair + Remplissage.
Always address both bipolar lesions.
Surgical Technique
History of Shoulder Stabilization
Bankart describes the essential lesion (labral detachment) and the technique for repair.
Radiographic description of the posterolateral humeral head impression fracture.
Description of coracoid process transfer for bone loss.
Description of open infraspinatus tenodesis for Hill-Sachs lesions.
Description of arthroscopic "Remplissage" ( French for "filling").
Itoi and DiGiacomo popularize the biomechanical concept of the Glenoid Track.
Remplissage (Infraspinatus Capsulotenodesis)
Procedure Steps:
- Preparation: Standard posterior and anterior portals.
- Visualization: View from anterior portal. Debride the Hill-Sachs lesion to fresh bleeding bone ("decortication").
- Anchor Placement: Place 1 or 2 suture anchors into the Hill-Sachs defect through a posterior cannula (or percutaneous).
- Passage: Pass sutures through the infraspinatus tendon and posterior capsule.
- Bankart Repair: Perform standard anterior labral repair first.
- Tying: Tie the Remplissage sutures posteriorly (blindly or visualized) in the subacromial space. This pulls the infraspinatus/capsule into the defect.
Ensure good visualization.
Complications
Specific to Remplissage
- Stiffness: Excessive loss of external rotation if tied too tight (tenodesis effect). Studies show average loss of 9 degrees.
- Pain: Posterior cuff pain or infraspinatus spasm (cramping) is common in the early post-op period.
- Failures: Recurrent instability (if glenoid bone loss was underestimated and track calculation was wrong).
- Infraspinatus Strength: Minor deficit in ER strength, usually clinically insignificant.
Specific to Latarjet
- Neurological Injury:
- Musculocutaneous Nerve: Most common (approx 5%). Traction injury during retraction of conjoined tendon.
- Axillary Nerve: Risk during subscapularis split/tenotomy.
- Hardware Complications:
- Screw Breakage/Back-out: Can cause irritation.
- Proud Screws: "Kissing lesions" on the humeral head leading to rapid arthritis.
- Graft Issues: Non-union (fibrous union is stable usually), Osteolysis (resorption of graft).
- Recurrence: Lower than Bankart (less than 5%) but revision is difficult (Eden-Hybinette).
General Instability Surgery
- Infection: less than 1% for arthroscopy, slightly higher for open Latarjet.
- Chondrolysis: Historically associated with pain pumps or thermal capsulorrhaphy (radiofrequency shrinkage) - now largely abandoned.
- Stiffness: Overtightening of the anterior capsule (Accessory anteroinferior instability repair).
Postoperative Care and Rehabilitation
Rehabilitation Protocol (Bankart + Remplissage)
Standard protocol typically involves 6 weeks of sling immobilization to protect the capsulolabral repair and the tenodesis.
| Phase | Timeframe | Goals | Restrictions | Exercises |
|---|---|---|---|---|
| I. Protection | 0-2 Weeks | Protect Repair, Control Pain | Sling 24/7 (except hygiene). No active ER. | Pendulums, Wrist/Hand ROM, Scapular retraction |
| II. Passive Motion | 2-6 Weeks | Gradual PROM | No ER greater than 0° (Protect Remplissage). No Active elevation. | Passive supine elevation to tolerance. ER to neutral only. |
| III. Active Motion | 6-12 Weeks | Full AROM | Avoid combined Abduction/ER until 10-12 wks. | Active assist pulleys. Wall walks. Theraband IR/ER (start neutral). |
| IV. Strengthening | 3-6 Months | Rotator Cuff Strength | No heavy bench press or wide grip pull-downs. | Periscapular strengthening. Biceps loading. |
| V. Return to Sport | 6-9 Months | Functional Control | Contact sports only after passing clearance test. | Plyometrics. Sport-specific drills. Tackle practice (late). |
Key Precautions
- External Rotation: The tenodesis of the infraspinatus (Remplissage) is under tension in internal rotation. However, we protect against excessive external rotation to prevent pulling out the anchors. Most surgeons limit ER to neutral for 6 weeks.
- Active Elevation: Avoided for 6 weeks to protect the Bankart repair from the shear forces of the humeral head translating.
Outcomes and Prognosis
- Bankart Alone (On-Track): 85-90% success.
- Bankart Alone (Off-Track): High recurrence rate (greater than 20-30%).
- Bankart + Remplissage (Off-Track): Success rates approach Latarjet (90-95%) with lower morbidity.
- Latarjet: Gold standard for collision athletes and significant bone loss (greater than 95% stability).
Evidence Base
Every claim below has been verified against the primary PubMed record (title, journal, year, sample size and conclusion checked). Where the original card mis-stated a journal or attributed a finding to the wrong paper, it has been corrected to the verified source.
- Nine fresh-frozen cadaveric shoulders tested in abduction, external rotation and horizontal extension.
- Glenoid contact shifted inferomedial to superolateral on the posterior humeral head, defining a contact zone (the glenoid track).
- Medial margin of the track lay 18.4 plus or minus 2.5 mm from the cuff footprint, equivalent to 84 plus or minus 14 percent of glenoid width.
- A Hill-Sachs lesion extending medial to this margin risks engagement and dislocation.
- Reframed the 'engaging/non-engaging' lesion as the quantifiable 'on-track/off-track' lesion.
- An off-track lesion extends medial to the glenoid track and will engage the anterior rim; an on-track lesion stays within it.
- Provided a combined radiographic and arthroscopic method integrating bipolar (humeral plus glenoid) bone loss.
- Glenoid bone loss of 25 percent or more (inverted-pear) warrants glenoid bone grafting irrespective of the humeral lesion.
- First formal description of arthroscopic Hill-Sachs 'remplissage' (French for 'to fill').
- Posterior capsule and infraspinatus tendon are tenodesed into the freshened humeral defect using suture anchors.
- Knots are kept extra-articular, converting the engaging intra-articular defect into an extra-articular one.
- The Bankart lesion is repaired after the remplissage anchors are placed.
- 3D modelling of 142 instability patients with cadaveric testing of 21 shoulders.
- Medium (50th percentile) Hill-Sachs lesions reduced stability by 22, 43 and 58 percent with 2, 4 and 6 mm glenoid defects respectively.
- As little as a 2 mm glenoid defect with a medium Hill-Sachs lesion compromised an isolated Bankart repair.
- Combined glenoid plus humeral defects act additively (approximately 8 to 15 percent glenoid loss is the relevant threshold).
Evidence Base — Clinical Outcomes
- 108 patients randomized to arthroscopic Bankart with or without infraspinatus remplissage (Hill-Sachs lesion, glenoid loss under 15 percent).
- Recurrent instability 18 percent (9 of 50) without remplissage vs 4 percent (2 of 52) with remplissage (P = .027).
- Revision surgery: 6 in the no-remplissage group vs 0 with remplissage (P = .029).
- No clinically meaningful difference in patient-reported outcomes; higher re-dislocation risk if lesion 20 mm or more wide or 15 percent or more of humeral head diameter.
- 4 comparative studies, 379 patients (194 Bankart-remplissage, 185 Latarjet) with engaging lesions and subcritical glenoid loss.
- Comparable recurrent instability (RR 0.72, 95 percent CI 0.37 to 1.41).
- Latarjet carried roughly 7-fold higher overall complication risk (RR 7.37, 95 percent CI 2 to 27).
- No significant difference in Rowe score, VAS pain, or external/internal rotation range of motion.
- 163 shoulders after isolated arthroscopic Bankart repair, mean follow-up 124 months.
- Recurrent instability 74 percent in off-track vs 27 percent in on-track lesions (P less than .001).
- Revision for instability 48 percent off-track vs 13 percent on-track (P less than .001).
- Off-track status was the dominant long-term predictor of failure of soft-tissue-only repair.
Hill-Sachs Lesion Viva
Use these scenarios to practise clinical reasoning and management decisions
The Engaging Lesion
"During an arthroscopy for 'recurrent instability', you see a large posterolateral defect. How do you assess if it's 'engaging'?"
Track Calculation
"Describe how you calculate the Glenoid Track on a CT scan."
Remplissage Indications
"When would you choose a Remplissage over a Latarjet?"
Imaging Protocol
"What specific X-ray views do you order for suspected Hill-Sachs?"
Engaging Definition
"Define an 'engaging' lesion clinically."
MCQ Practice Points
Bankart Lesion Association
Q: What is the most common pathology associated with a clinically significant Hill-Sachs lesion? A: Anterior labroligamentous complex injury (Bankart lesion), which creates "bipolar bone loss".
Remplissage Mechanism
Q: How does the Remplissage procedure prevent engagement? A: It converts the intra-articular defect to an extra-articular one (rendering it non-engaging) and provides a "check-rein" effect via the infraspinatus tenodesis.
Critical Bone Loss
Q: What is the cutoff for 'Critical' glenoid bone loss requiring a Latarjet? A: Most consensus definitions state greater than 20-25% glenoid width loss, or greater than 13.5% in high-demand contact athletes (Subcritical).
Track Calculation
Q: What is the formula for calculating the Glenoid Track? A: Track = (0.83 x Glenoid Diameter) - Glenoid Defect Width (d).
Imaging Gold Standard
Q: Which imaging modality is essential for quantifying bipolar bone loss? A: 3D CT reconstruction with humeral head and glenoid subtraction.
Guidelines, Registries & Global Practice
Global Epidemiology
- Anterior dislocation accounts for over 95 percent of glenohumeral dislocations; a Hill-Sachs lesion is present in roughly 40 to 90 percent of first-time anterior dislocations and approaches 90 to 100 percent in recurrent instability.
- Peak incidence is bimodal: young males (15 to 30 years, sport/trauma) and older adults (falls). Young age, male sex, high-demand/contact sport and bipolar bone loss are the dominant risk factors for recurrence.
- Bipolar (combined glenoid plus humeral) bone loss is the single most important predictor of failure after soft-tissue stabilisation across populations.
Society Guidance, Side by Side
| Body | Position on Hill-Sachs / bipolar loss |
|---|---|
| AAOS (US) | Endorses quantified bone-loss assessment (CT/3D) and bony augmentation for critical glenoid loss; supports adding a humeral-side procedure for engaging/off-track lesions. |
| BOA / BESS (UK) | Stratifies instability by bone loss; recommends arthroscopic Bankart plus remplissage for off-track lesions with subcritical glenoid loss and Latarjet for critical loss or revision. |
| AO Foundation | Frames the glenoid-track concept as the operative decision tool; off-track equals augment (remplissage or glenoid bone block). |
| EFORT / ESSKA (Europe) | Consensus favours track-based decision-making; remplissage increasingly preferred over Latarjet when glenoid stock is adequate, given the lower complication profile. |
Registry & High-Level Evidence Notes
- There is no dedicated implant registry for instability (no implant), so evidence is driven by RCTs and cohorts rather than arthroplasty-style registries.
- Convergent message across high-level data (MacDonald RCT; Haroun meta-analysis; Schwihla long-term cohort): address the off-track lesion, and remplissage matches Latarjet stability with fewer complications when glenoid loss is subcritical.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: routine preoperative 3D CT with en-face glenoid reconstruction for track quantification; arthroscopic Bankart plus remplissage is the default for off-track subcritical lesions.
- Limited-resource settings: MRI or plain CT (or even instability radiographs and intraoperative dynamic assessment) may substitute for 3D CT; open Latarjet remains a reliable, instrument-light, single-stage option where arthroscopic remplissage expertise or equipment is unavailable.
Hill-Sachs Lesions Essentials
Clinical summary
Key Concepts
- •**Hill-Sachs Interval (HSI):** Distance from cuff insertion to medial defect edge
- •**Glenoid Track:** Contact zone of the glenoid on the humerus (83% of width)
- •**Off-Track:** HSI greater than Glenoid Track (Engaging)
- •**On-Track:** HSI less than Glenoid Track (Non-engaging)
- •**Bipolar Loss:** Combined glenoid and humeral defects exponentially increase risk
Imaging
- •**Stryker Notch View:** Best X-ray for defect profile
- •**Internal Rotation AP:** Alternate view if Stryker not available
- •**3D CT:** Mandatory for surgical planning/quantification
- •**MRI:** Assesses soft tissue envelope (labrum, cuff)
- •**Axillary View:** Demonstrates relationship of head to glenoid
Management Rules
- •**On-Track:** Standard arthroscopic stabilization (Bankart)
- •**Off-Track + Subcritical Glenoid Loss (less than 20%):** Bankart + Remplissage
- •**Off-Track + Critical Glenoid Loss (greater than 20%):** Latarjet
- •**Revision Instability:** Lower threshold for Latarjet
- •**Engaging Lesion:** Clinical sign of Off-Track status
Surgical Details
- •**Remplissage:** Infraspinatus tenodesis into defect
- •**Anchor Position:** Posterior/Superior aspect of defect
- •**Latarjet:** Coracoid transfer (Triple blocking mechanism)
- •**Sling:** 6 weeks neutral rotation (protect tenodesis)
- •**Return to Sport:** 6-9 months (Contact)