Thompson-Epstein Classification | Pipkin Fractures | Urgent Reduction
THOMPSON-EPSTEIN CLASSIFICATION
Critical Must-Knows
- 6-hour golden window for reduction - AVN risk increases from 5% (under 6h) to 40%+ (over 12h)
- Thompson-Epstein classification - Type I (simple), Type II-V (with fractures)
- Pipkin classification for femoral head fractures - Type I (below fovea), Type II (above fovea), Type III (+ neck), Type IV (+ acetabulum)
- Sciatic nerve at risk in posterior dislocations (10-20%) - peroneal division most vulnerable
- CT post-reduction mandatory - assess concentric reduction, loose bodies, fractures
Clinical Pearls
- "Hip fracture-dislocation = true orthopaedic emergency - reduce within 6 hours
- "Thompson-Epstein Type V = Pipkin fracture - use Pipkin classification to guide treatment
- "Posterior wall over 40% = unstable - requires ORIF
- "Pipkin III (head + neck) = disaster - double blood supply insult, high AVN risk
Clinical Imaging
Imaging Gallery



Critical Hip Fracture-Dislocation Exam Points
True Orthopaedic Emergency
6-hour golden window for reduction - AVN risk increases from 5% (under 6 hours) to 40%+ (over 12 hours). This is a true orthopaedic emergency. Reduce as soon as possible, even before CT if needed.
Thompson-Epstein Classification
Type I (simple), Type II (posterior wall), Type III (comminuted wall), Type IV (acetabular floor), Type V (femoral head/Pipkin) - Classification guides treatment. Type V uses Pipkin classification for femoral head fracture management.
Pipkin Classification
Pipkin I (below fovea), Pipkin II (above fovea), Pipkin III (+ neck), Pipkin IV (+ acetabulum) - Fovea is key landmark. Above fovea = weight-bearing = must fix. Below fovea = may excise if small.
Sciatic Nerve at Risk
10-20% sciatic nerve injury in posterior dislocations. Peroneal division most vulnerable. Document nerve function BEFORE and AFTER reduction. Most recover by 2 years.
Hip Fracture-Dislocations - Quick Decision Guide
| Type | Associated Fracture | Treatment | AVN Risk |
|---|---|---|---|
| Type I | None | Urgent closed reduction | 5% (under 6h) |
| Type II | Posterior wall | Reduce, assess wall, ORIF if over 40% | 10-15% |
| Type III | Comminuted wall | Reduce, ORIF posterior wall | 15-20% |
| Type IV | Acetabular floor | Reduce, ORIF acetabulum | 20-25% |
| Type V (Pipkin) | Femoral head | Reduce, Pipkin classification guides | 20-40% |
HIPHip Fracture-Dislocation Features
| H | Hour 6-hour golden window for reduction |
| I | Injury High-energy, associated injuries common |
| P | Pipkin Type V = Pipkin classification |
| H | Hour 6-hour golden window for reduction |
| I | Injury High-energy, associated injuries common |
| P | Pipkin Type V = Pipkin classification |
Hook:HIP: Hour (6-hour window), Injury (high-energy), Pipkin (Type V)!
TYPESThompson-Epstein Types
| T | Type I Simple dislocation, no fracture |
| Y | Type II Posterior wall fracture |
| P | Type III Comminuted posterior wall |
| E | Type IV Acetabular floor fracture |
| S | Type V Femoral head fracture (Pipkin) |
| T | Type I Simple dislocation, no fracture | E | Type IV Acetabular floor fracture |
| Y | Type II Posterior wall fracture | S | Type V Femoral head fracture (Pipkin) |
| P | Type III Comminuted posterior wall |
Hook:TYPES: Type I simple, Type II wall, Type III comminuted, Type IV floor, Type V Pipkin!
PIPKINPipkin Classification
| P | Pipkin I Below fovea (non-weight-bearing) |
| I | Pipkin II Above fovea (weight-bearing) |
| P | Pipkin III Plus femoral neck fracture |
| K | Pipkin IV Plus acetabular fracture |
| I | Inferior Pipkin I = inferior to fovea |
| N | Neck Pipkin III = neck fracture = disaster |
| P | Pipkin I Below fovea (non-weight-bearing) | P | Pipkin III Plus femoral neck fracture | I | Inferior Pipkin I = inferior to fovea |
| I | Pipkin II Above fovea (weight-bearing) | K | Pipkin IV Plus acetabular fracture | N | Neck Pipkin III = neck fracture = disaster |
Hook:PIPKIN: Pipkin I below fovea, Pipkin II above fovea, Pipkin III plus neck (disaster), Pipkin IV plus acetabulum!
Overview and Epidemiology
Hip fracture-dislocations are high-energy injuries combining hip dislocation with associated fractures (femoral head, acetabulum, femoral neck). They are true orthopaedic emergencies requiring urgent reduction within 6 hours to minimize AVN risk. The Thompson-Epstein classification guides treatment based on associated fractures.
Mechanism of Injury
Posterior dislocation (90%):
- Dashboard injury: Knee strikes dashboard with hip flexed
- High energy: Motor vehicle accident, fall from height
- Associated fractures: Femoral head (Pipkin), posterior wall, femoral neck
Anterior dislocation (10%):
- Forced abduction: Hip forced into abduction and external rotation
- Less common: Usually lower energy
- Associated fractures: Less common
Central dislocation:
- Acetabular fracture: Medial displacement through acetabulum
- High energy: Usually part of complex acetabular fracture pattern
True Orthopaedic Emergency
Hip fracture-dislocation = true orthopaedic emergency - reduce within 6 hours. AVN risk increases from 5% (under 6 hours) to 40%+ (over 12 hours). Every hour of delay increases AVN risk. Reduce as soon as possible, even before CT if needed.
Epidemiology
- Incidence: 5-10% of hip dislocations have associated fractures
- Age: Peak 20-40 years (high-energy trauma)
- Gender: Male predominance (3:1 ratio)
- Laterality: Usually unilateral
- Associated injuries: Other fractures (20-30%), head injury (10-15%), knee injuries (10-15%)
Anatomy and Pathophysiology
Hip Joint Anatomy
The hip joint:
- Ball-and-socket: Femoral head in acetabulum
- Stability: Bony and ligamentous (labrum, capsule, ligaments)
- Blood supply: MFCA (80%), retinacular vessels, ligamentum teres (under 10%)
- Nerves: Sciatic nerve (posterior), femoral nerve (anterior)
Posterior structures at risk:
- Sciatic nerve: Lies posterior to hip, vulnerable in posterior dislocation
- Peroneal division: Most vulnerable (lateral position)
- Tibial division: Less vulnerable (medial position)
Pathophysiology
Posterior dislocation mechanism:
- Dashboard injury: Knee strikes dashboard with hip flexed
- Force transmission: Posterior force on flexed hip
- Dislocation: Femoral head dislocates posteriorly
- Associated fractures: Femoral head (impaction), posterior wall (shear), femoral neck (rare)
Blood supply disruption:
- Retinacular vessels: Disrupted with displacement
- MFCA: May be stretched or torn
- AVN risk: Increases with time to reduction
- 6-hour window: Critical for blood supply preservation
Associated fracture patterns:
- Femoral head (Pipkin): Impaction or shear fracture
- Posterior wall: Shear fracture from dislocation
- Acetabular floor: Central dislocation pattern
- Femoral neck: Rare but devastating (Pipkin III)
Sciatic Nerve at Risk
Sciatic nerve injury occurs in 10-20% of posterior dislocations. Peroneal division is most vulnerable (lateral position). Always document nerve function BEFORE and AFTER reduction. Most injuries recover by 2 years, but explore if no recovery by 6 months.
Classification Systems
Thompson-Epstein Classification (Posterior)
Type I: Dislocation with no or insignificant fracture
- Simple dislocation
- Treatment: Urgent closed reduction
- AVN risk: 5% (under 6 hours)
Type II: Dislocation with single large posterior wall fracture
- Posterior wall fracture
- Treatment: Reduce, assess wall size, ORIF if over 40%
- AVN risk: 10-15%
Type III: Dislocation with comminuted posterior wall fracture
- Comminuted posterior wall
- Treatment: Reduce, ORIF posterior wall
- AVN risk: 15-20%
Type IV: Dislocation with acetabular floor fracture
- Acetabular floor fracture (unstable)
- Treatment: Reduce, ORIF acetabulum
- AVN risk: 20-25%
Type V: Dislocation with femoral head fracture
- Femoral head fracture (Pipkin)
- Treatment: Reduce, Pipkin classification guides treatment
- AVN risk: 20-40%
Thompson-Epstein classification guides treatment based on associated fractures.
Clinical Assessment
History
Mechanism: High-energy trauma
- Dashboard injury: Motor vehicle accident (posterior dislocation)
- Fall from height: High-energy fall
- Sports: Contact sports, high-impact activities
Symptoms:
- Immediate severe pain
- Inability to bear weight
- Leg deformity (shortening, rotation)
- Numbness or weakness (if nerve injury)
Physical Examination
Inspection:
- Posterior dislocation: Leg shortened, adducted, internally rotated
- Anterior dislocation: Leg externally rotated, abducted
- Deformity obvious
- Swelling (may be minimal initially)
Palpation:
- Tenderness over hip
- Palpable femoral head (posterior or anterior)
- Greater trochanter position abnormal
Range of Motion:
- Severely limited (pain, mechanical block)
- Fixed deformity
Neurovascular Status:
- Sciatic nerve: Assess dorsiflexion, plantarflexion, sensation (first web space, lateral foot)
- Vascular: Distal pulses, capillary refill
- Document BEFORE reduction: Critical for medicolegal and clinical assessment
Clinical Examination Key Point
Document sciatic nerve function BEFORE reduction - critical for medicolegal and clinical assessment. Peroneal division most vulnerable (assess dorsiflexion, first web space sensation). Most injuries recover by 2 years, but explore if no recovery by 6 months.
Associated Injuries
- Femoral head fracture (Pipkin): 10-15%
- Posterior wall fracture: 20-30%
- Acetabular fracture: 10-15%
- Femoral neck fracture: 5-10% (Pipkin III)
- Knee injuries: 10-15% (PCL, patella)
- Other fractures: 20-30%
Investigations
Standard X-ray Protocol
Views: AP pelvis and lateral hip (if possible).
Key findings:
- Dislocation: Femoral head out of acetabulum
- Associated fractures: Femoral head, acetabulum, femoral neck
- Femoral neck fracture: MUST exclude before reduction (risk of displacement)
Pre-reduction X-ray essential - exclude femoral neck fracture before attempting reduction.
Management Algorithm
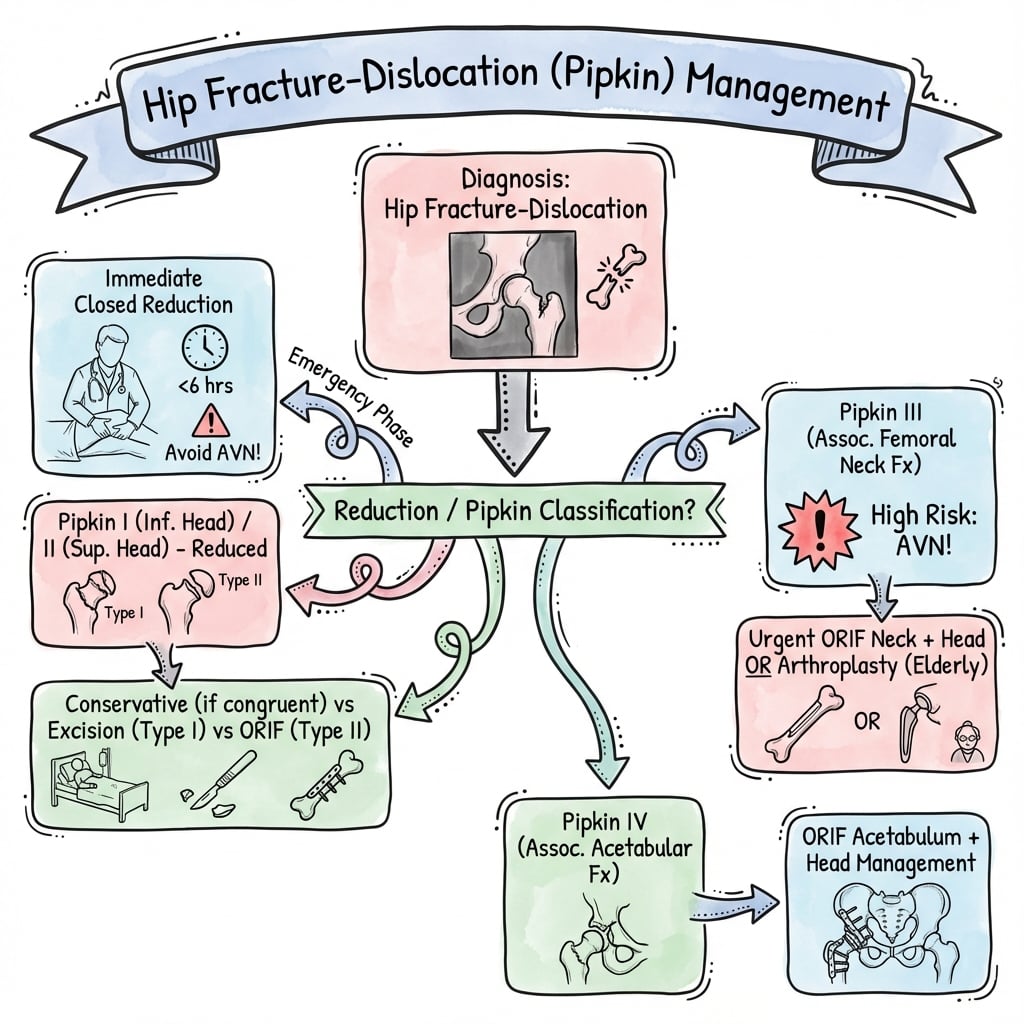
Management Pathway
Hip Fracture-Dislocation Management
Reduce within 6 hours (golden window). Pre-reduction X-ray to exclude femoral neck fracture. Closed reduction in ED or OR. Document nerve function before reduction.
CT scan mandatory after reduction. Assess concentric reduction, loose bodies, fractures (Pipkin, acetabular, neck). Plan definitive treatment.
If no fractures, observe. Protected weight bearing 6-8 weeks. Monitor for AVN (X-ray at 6, 12 weeks, 1 year).
Type II: ORIF posterior wall if over 40%. Type III: ORIF comminuted wall. Type IV: ORIF acetabulum. Type V: Pipkin classification guides treatment.
Surgical Technique
Posterior Wall Fixation
Indications:
- Posterior wall over 40% (unstable)
- Comminuted wall (Type III)
- Non-concentric reduction
Technique:
- Kocher-Langenbeck approach
- Identify and protect sciatic nerve
- Reduce wall fragments
- Spring plate or buttress plate fixation
- Assess stability with fluoroscopy
Critical: Sciatic nerve at risk - identify and protect before any dissection.
Sciatic Nerve Protection
Sciatic nerve lies directly posterior to hip - at risk during posterior approach. Always identify and protect sciatic nerve before any dissection. Use vessel loops to retract. Avoid excessive retraction. Document nerve function before and after surgery.
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| AVN | 5-40% | Time to reduction, displacement, Pipkin type | Urgent reduction (under 6h), anatomic reduction |
| Sciatic nerve injury | 10-20% | Posterior dislocation, surgical approach | Protect nerve, document function |
| Heterotopic ossification | 20-30% | Surgical approach, delayed reduction | Prophylaxis (indomethacin, radiation) |
| Post-traumatic arthritis | 20-30% | Cartilage injury, AVN, malreduction | Anatomic reduction, early reduction |
| Recurrent dislocation | 5-10% | Instability, inadequate fixation | Secure fixation, assess stability |
AVN
5-40% incidence (depends on timing and pattern):
- Cause: Disruption of blood supply, delayed reduction, displacement
- Prevention: Urgent reduction (under 6 hours), anatomic reduction
- Management: Monitor with X-rays (6, 12 weeks, 1 year), THA if symptomatic
Sciatic Nerve Injury
10-20% incidence:
- Cause: Dislocation itself or surgical approach
- Prevention: Protect nerve during approach, document function
- Management: Observation (most recover by 2 years), explore if no recovery by 6 months
Heterotopic Ossification
20-30% incidence:
- Cause: Surgical approach, delayed reduction, associated injuries
- Prevention: Prophylaxis (indomethacin, radiation)
- Management: Excision if symptomatic (wait for maturity)
Differential Diagnosis
The acutely painful, deformed hip after trauma has a focused differential. The priority is to distinguish a true dislocation (reduce now) from an isolated fracture (different pathway), and to never miss an occult femoral neck fracture before pulling on the leg.
Differentiating the Deformed Traumatic Hip
| Diagnosis | Typical Limb Position | Key Discriminator | Action |
|---|---|---|---|
| Posterior fracture-dislocation | Shortened, adducted, internally rotated | Femoral head out of acetabulum on AP; wall/head fragment | Emergent reduction, then CT |
| Anterior dislocation | Abducted, externally rotated, often extended | Head medial/inferior to acetabulum | Emergent reduction, exclude vascular injury |
| Femoral neck fracture | Shortened, externally rotated | Lucency across neck, head IN acetabulum | Do NOT attempt dislocation-style reduction; fix neck |
| Intertrochanteric fracture | Shortened, markedly externally rotated | Fracture line trochanter to trochanter | Fixation pathway (DHS/IM nail) |
| Isolated acetabular (central) fracture | Variable, may be subtle | Head migrated medially through floor | Judet views/CT, acetabular pathway |
| Native/prosthetic hip dislocation (atraumatic) | Pattern depends on direction | History of THA, low-energy event | Closed reduction, assess components/instability |
Never Miss the Occult Neck Fracture
Always scrutinise the femoral neck on the pre-reduction radiograph. Attempting a vigorous closed reduction across an undiagnosed femoral neck fracture can convert it into a displaced fracture and devastate the blood supply. If a neck fracture coexists (Pipkin III), the strategy changes fundamentally.
Controversies and Areas of Uncertainty
The 6-hour rule
The traditional 6-hour window is widely taught but not a sharp biological threshold. Meta-analysis evidence shows the strongest, statistically robust step-up in AVN occurs around the 12-hour mark (odds ratio about 5.6). The pragmatic message is unchanged: reduce as soon as safely possible.
Closed vs open / surgical hip dislocation
For displaced femoral head fractures, debate continues between anterior approaches, posterior approaches and the Ganz surgical hip dislocation. Surgical hip dislocation gives the best articular view but adds a trochanteric osteotomy; reported AVN rates are comparable rather than clearly superior.
Posterior wall stability threshold
The "40% = unstable" rule oversimplifies. Static CT poorly predicts stability in the 20-50% indeterminate zone, and examination under anaesthesia remains the reference standard for borderline walls.
Pipkin I: excise or fix?
Small infra-foveal fragments may be excised, but excision of larger fragments risks instability and degenerative change. There is no consensus fragment-size cut-off; decisions are individualised to fragment size, comminution and joint congruity.
How to Handle Controversy in the Viva
State the conventional teaching, then show you understand its limits: "The classic teaching is reduction within 6 hours, although the best evidence shows the major rise in AVN is after 12 hours, so my principle is emergent reduction as soon as the patient is safe." This demonstrates consultant-level nuance.
Postoperative Care
Immediate Postoperative
- Immobilization: None (early mobilization)
- Weight bearing: Depends on associated fractures
- Simple dislocation: Touch-down weight bearing 6-8 weeks
- With fractures: Non-weight bearing until fractures heal
- ROM: Early hip ROM (immediate)
- PT: Hip ROM, strengthening
Rehabilitation Protocol
Weeks 0-2:
- Touch-down or non-weight bearing (depending on fractures)
- Hip ROM exercises
- Quadriceps and hip strengthening
- Ice and elevation
Weeks 2-6:
- Continue protected weight bearing
- Progressive ROM and strengthening
- Balance and proprioception
Weeks 6-12:
- Progressive weight bearing (if fractures healed)
- Full ROM
- Progressive activity
Weeks 12+:
- Return to sport (when strength and ROM normal)
- Continue monitoring for AVN (X-rays at 6, 12 weeks, 1 year)
Return to Sport
Criteria:
- Full ROM (equal to contralateral)
- Strength greater than 90% of contralateral
- No pain or instability
- Functional testing passed
- No AVN on imaging
Timeline: Usually 6-12 months postoperatively, depending on associated injuries.
Outcomes and Prognosis
Overall Outcomes
Simple dislocation (Type I):
- Success rate: 85-90% (with urgent reduction)
- Functional outcomes: 80-85% return to pre-injury level
- Complications: 10-15% (AVN, HO, arthritis)
With fractures (Type II-V):
- Success rate: 70-85% (depends on fracture pattern)
- Functional outcomes: 70-80% return to pre-injury level
- Complications: 20-30% (AVN, HO, arthritis, nerve injury)
Functional Outcomes
Return to sport:
- Timeline: 6-12 months postoperatively
- Rate: 70-85% return to pre-injury level
- Factors: Associated injuries, AVN, rehabilitation compliance
Functional testing:
- Hip strength: 90%+ of contralateral
- ROM: Full (if no complications)
- No pain or instability
Long-Term Prognosis
AVN risk:
- Type I (under 6h): 5-10%
- Type I (over 12h): 40%+
- Type II-V: 20-40% (depends on timing and pattern)
- Pipkin III: 40-60% (disaster)
Post-traumatic arthritis:
- Type I: 20-30% (at 10 years)
- Type II-V: 30-40% (at 10 years)
- Risk factors: Cartilage injury, AVN, malreduction
Factors Affecting Outcomes
Positive factors:
- Urgent reduction (under 6 hours)
- Simple dislocation (Type I)
- No associated fractures
- Complete rehabilitation
Negative factors:
- Delayed reduction (over 12 hours)
- Associated fractures (Type II-V)
- Pipkin III (head + neck)
- Incomplete rehabilitation
Prevention and Return to Sport
Prevention
Primary prevention:
- Seatbelt use (prevents dashboard injury)
- Airbag deployment
- Safe driving practices
- Protective equipment in sports
Secondary prevention (after injury):
- Complete rehabilitation before return to sport
- Continued strength and conditioning
- Gradual return to activity
Return to Sport Criteria
Clinical:
- Full ROM (equal to contralateral)
- Strength greater than 90% of contralateral
- No pain or instability
- No AVN on imaging
Functional:
- Single-leg hop test (greater than 90% of contralateral)
- Agility testing passed
- Sport-specific drills completed
Timeline: Usually 6-12 months postoperatively, depending on associated injuries and AVN risk.
Evidence Base
Time to Reduction and AVN Risk
- Posterior dislocation AVN event rate 10.6-43%, rising with Thompson-Epstein grade
- Odds ratio of AVN 5.6 for reduction after 12 hours versus before 12 hours
- Injury severity correlates with both AVN and post-traumatic arthritis
Long-term Outcome of Simple Dislocation
- 24% developed osteoarthritis at mean 14.6-year follow-up
- Higher OA rate in manual workers (up to 45% in pit-accident miners)
- Even Thompson-Epstein Type I carries meaningful long-term arthritis risk
Pipkin Classification (Original)
- Defines the four femoral-head fracture subtypes still used today
- Fovea is the landmark separating type I (below) from type II (above)
- Type III (with neck fracture) recognised as the worst prognostic group
Sciatic Nerve Injury in Hip Dislocation
- Sciatic nerve injury approximately 10% in adults, peroneal branch most affected
- At least partial recovery in 60-70% of patients
- Prompt reduction relieves nerve distortion; document function before and after
Posterior Wall Stability: CT vs EUA
- Walls under 20% usually stable, over 40-50% usually unstable
- Static CT unreliable in the indeterminate 20-50% range
- Dynamic EUA is the preferred determinant of hip stability
Surgical Hip Dislocation for Femoral Head Fractures
- Satisfactory outcome 85%, anatomic reduction 74%
- AVN 12%, heterotopic ossification 25%, osteoarthritis 16%
- Surgical hip dislocation gives controlled head exposure with acceptable vascular safety
Femoral Neck Fracture Drives AVN in FHFD
- AVN occurred only in patients with displaced femoral neck fractures (Pipkin III)
- Good or excellent outcome in the majority at 5.1 years
- Confirms Pipkin III as the dominant AVN risk subtype
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Posterior Dislocation with Pipkin II
"A 30-year-old man presents to ED after a motor vehicle accident. He was the driver and his knee struck the dashboard. He has a painful hip and cannot move his leg. Examination shows leg shortened, adducted, and internally rotated. X-ray shows posterior hip dislocation. After urgent closed reduction, CT shows a Pipkin II femoral head fracture (fragment above fovea, weight-bearing surface)."
Scenario 2: Type II with Posterior Wall
"A 35-year-old athlete presents after a high-energy fall. He has a posterior hip dislocation with a large posterior wall fracture. After urgent closed reduction, CT shows posterior wall fracture involving 45% of the wall. Examination under anesthesia shows instability."
Scenario 3: Pipkin III and the Irreducible Hip
"A 45-year-old man is brought in after a head-on collision. AP pelvis shows a posterior hip dislocation, and on close inspection there is a lucency across the femoral neck. Two gentle closed reduction attempts under sedation fail. How do you proceed and how does the neck fracture change your plan?"
MCQ Practice Points
Golden Window
Q: What is the golden window for hip dislocation reduction? A: 6 hours - AVN risk increases from 5% (under 6 hours) to 40%+ (over 12 hours). This is a true orthopaedic emergency. Reduce as soon as possible.
Thompson-Epstein Type V
Q: What does Thompson-Epstein Type V indicate? A: Femoral head fracture (Pipkin) - Type V = dislocation with femoral head fracture. Use Pipkin classification (I-IV) to guide treatment of the head fracture.
Pipkin II Treatment
Q: What is the treatment for Pipkin II femoral head fracture? A: ORIF with headless screws - Pipkin II = fragment above fovea (weight-bearing surface). Must fix to restore articular surface. Anterior approach to avoid posterior blood supply.
Posterior Wall Threshold
Q: What posterior wall size requires ORIF? A: Over 40% - Posterior wall over 40% = unstable, requires ORIF. Wall 20-40% = may be stable (assess with EUA). Wall under 20% = usually stable.
Sciatic Nerve Injury
Q: What is the incidence of sciatic nerve injury in posterior hip dislocations? A: 10-20% - Peroneal division most vulnerable (lateral position). Most injuries recover by 2 years. Document nerve function before and after reduction.
Pipkin III
Q: Why is Pipkin III (head + neck fracture) considered a disaster? A: Double blood supply insult - Both femoral head and neck blood supply disrupted. Very high AVN risk (40-60%). Often requires THA, even in young patients.
Guidelines, Registries & Global Practice
Global Epidemiology
- Hip dislocation overall is uncommon; roughly 5-15% of all traumatic dislocations and the great majority follow high-energy mechanisms (road traffic collisions, falls from height).
- Posterior pattern accounts for around 90% of cases; associated fractures (femoral head, posterior wall, neck) are present in a substantial minority and define the fracture-dislocation subgroup.
- Strong male predominance (roughly 3:1) with a young peak (20-40 years), mirroring high-energy trauma demographics worldwide.
- In low- and middle-income settings the same injury skews toward motorcycle and pedestrian trauma, and pre-hospital delay is the dominant modifiable risk factor for AVN.
Side-by-Side Guidance
How Major Bodies Frame Management
| Body | Emphasis | Practical Recommendation |
|---|---|---|
| AO Foundation / OTA | Emergency reduction + anatomic articular restoration | Urgent closed reduction, post-reduction CT, ORIF of displaced head/wall fragments via appropriate approach |
| BOA / BOAST (UK) | Polytrauma pathway and timely senior decision-making | Treat within an ATLS framework, escalate to pelvic/acetabular network for column or complex wall fractures |
| AAOS (US) | Evidence-informed individualised care | Reduce emergently, document neurovascular status, CT all fracture-dislocations before definitive fixation |
| EFORT / European consensus | Centralisation of acetabular surgery | Refer complex acetabular/Pipkin patterns to high-volume units; consider surgical hip dislocation for selected head fractures |
Registries and Practice Variation
- Dedicated dislocation registries are limited, but national arthroplasty registries (NJR UK, AJRR US, AOANJRR Australia, SHAR Sweden) capture the downstream burden: post-traumatic arthritis and AVN are recognised indications for conversion to total hip arthroplasty in young adults.
- High-resource centres: 24/7 trauma access, immediate CT, fellowship-trained pelvic/acetabular surgeons and surgical-hip-dislocation capability.
- Limited-resource centres: emphasis on rapid closed reduction (the single highest-value intervention), selective transfer for complex fixation, and pragmatic non-operative management of small fragments.
Orthopaedic Exam Relevance
Hip fracture-dislocations are a common viva topic. Know that this is a true orthopaedic emergency (urgent reduction, AVN risk rises sharply after 12 hours), the Thompson-Epstein classification (Type I-V), the Pipkin classification for Type V (I-IV), the posterior wall stability question (around 40%, confirmed by EUA), sciatic nerve at risk (about 10%), and urgent reduction technique. Be prepared to discuss surgical approaches and complications.
HIP FRACTURE-DISLOCATIONS
Clinical summary
Key Anatomy
- •Hip joint: Ball-and-socket, femoral head in acetabulum
- •Sciatic nerve: Posterior to hip, vulnerable in posterior dislocation
- •Blood supply: MFCA 80%, retinacular vessels, ligamentum teres under 10%
- •Fovea: Key landmark for Pipkin classification (above vs below)
Classification
- •Thompson-Epstein: Type I (simple), Type II (wall), Type III (comminuted), Type IV (floor), Type V (Pipkin)
- •Pipkin: I (below fovea), II (above fovea), III (+ neck), IV (+ acetabulum)
- •By timing: Acute (under 6h), Subacute (6-12h), Delayed (over 12h)
- •Posterior wall threshold: over 40% = unstable = ORIF required
Treatment Algorithm
- •Urgent closed reduction within 6 hours (golden window)
- •Post-reduction CT mandatory (assess reduction, fractures, loose bodies)
- •Type I: Observe, protected weight bearing 6-8 weeks
- •Type II-V: Address fractures (ORIF wall, Pipkin, acetabulum)
Surgical Pearls
- •Kocher-Langenbeck approach for posterior, protect sciatic nerve
- •Anterior approach for Pipkin (preserves blood supply)
- •Posterior wall over 40% = unstable = ORIF required
- •Pipkin II = weight-bearing = ORIF required
Complications
- •AVN: 5-40% (depends on timing - under 6h = 5%, over 12h = 40%+)
- •Sciatic nerve injury: 10-20% (most recover by 2 years)
- •Heterotopic ossification: 20-30% (prophylaxis with indomethacin)
- •Post-traumatic arthritis: 20-30% (at 10 years)