Metal-on-Metal | Young Active Males | Now Rarely Performed | ALVAL and Pseudotumor Complications
- Hip resurfacing has largely been abandoned due to metal-on-metal complications
- ALVAL (aseptic lymphocytic vasculitis-associated lesion) is the signature complication
- Pseudotumors can occur from metal debris and require revision
- Femoral neck fracture occurs in 1-2% annually in the first 5 years
- Current role is extremely limited - only highly selected young males if any use
- “Hip resurfacing preserves femoral bone stock but has higher revision rate than THA
- “Metal-on-metal bearing leads to elevated blood cobalt and chromium levels
- “ASR (Articular Surface Replacement) was recalled in 2010 due to high failure rates
- “Birmingham Hip Resurfacing was the most successful design but still problematic
- “Female patients have 2-3x higher failure rate than males
Hip resurfacing was popular in 2000s as bone-preserving alternative to THA for young patients. The ASR recall in 2010 and recognition of ALVAL complications led to dramatic decline. Know this history for exam context.
Metal debris from the bearing generates cobalt and chromium ions. This causes ALVAL (inflammatory reaction), pseudotumors, and systemic metal toxicity. These complications led to abandonment of the procedure.
The femoral neck remains under the implant and is at risk of fracture (1-2% per year). Risk factors include notching, varus positioning, AVN, and osteoporosis. Requires urgent conversion to THA.
Extremely limited in 2024. Occasionally considered in young (under 55), active, large males with good bone quality. Most surgeons have completely abandoned the technique. Know the contraindications.
- Hip Resurfacing
- Preserves femoral neck and metaphysis
- Conventional THA
- Removes femoral head and neck
- Hip Resurfacing
- Metal-on-metal (MoM) only
- Conventional THA
- Multiple options (ceramic, polyethylene, MoM)
- Hip Resurfacing
- Lower (large head size 40-60mm)
- Conventional THA
- Higher with smaller heads
- Hip Resurfacing
- 1-2% per year (unique to resurfacing)
- Conventional THA
- Not applicable
- Hip Resurfacing
- 10-15% (major problem)
- Conventional THA
- Less than 1% with modern non-MoM bearings
- Hip Resurfacing
- Higher rate (15-20% at 10 years)
- Conventional THA
- Lower rate (5-10% at 10 years)
- Hip Resurfacing
- Marketed as better (unproven)
- Conventional THA
- Excellent with modern implants
- Hip Resurfacing
- Declined over 95% since 2010
- Conventional THA
- Gold standard for hip replacement
Overview and Historical Context
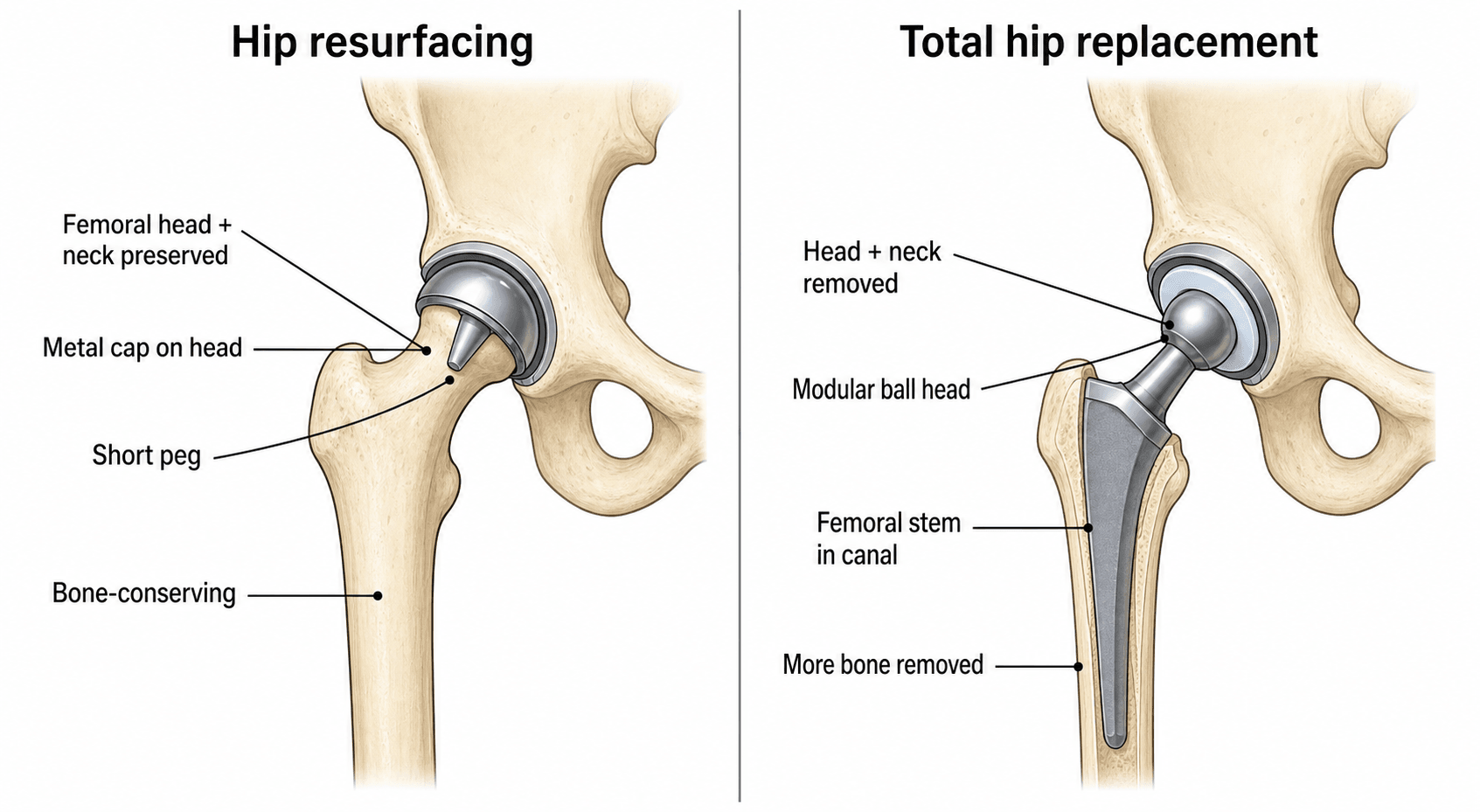
Hip resurfacing arthroplasty is a bone-conserving alternative to total hip arthroplasty where the femoral head is retained and resurfaced with a metal cap rather than being excised. A metal acetabular component articulates with the metal femoral component creating a metal-on-metal (MoM) bearing.
Historical development:
- 1950s-1970s: Early resurfacing attempts failed due to poor fixation and polyethylene wear
- 1990s: Metal-on-metal bearings revived the concept (Birmingham Hip Resurfacing)
- 2000-2010: Rapid adoption, marketed as bone-preserving for young active patients
- 2010: ASR recall marked beginning of decline
- 2012-2015: Recognition of ALVAL complications led to dramatic reduction in usage
- 2015-present: Essentially abandoned except in very select cases
The fundamental problem with hip resurfacing was the metal-on-metal bearing. While large diameter MoM bearings have lower volumetric wear than small diameter bearings, they generate metal debris (cobalt and chromium particles) that causes ALVAL, pseudotumors, and systemic toxicity. This proved to be an insurmountable problem.
- DePuy ASR (Articular Surface Replacement) introduced 2003
- Marketed heavily as minimally invasive bone-preserving solution
- 40% revision rate at 6 years (compared to 5% for standard THA)
- Recalled worldwide in August 2010
- Led to thousands of lawsuits and billions in settlements
- Destroyed confidence in hip resurfacing as a concept
- Usage declined over 95% from peak
- Some surgeons still perform in highly selected cases (young males with large femoral heads)
- Most organizations recommend against routine use
- Patients with existing resurfacing require metal ion monitoring
Indications and Contraindications
Original indications (2000-2010):
Hip resurfacing was marketed for young active patients as a bone-preserving alternative. The ideal candidate profile was:
- Age under 65 years (typically under 55)
- Male gender (females 2-3x higher failure rate)
- Active lifestyle with desire to return to high-demand activities
- Good bone quality (no osteoporosis)
- Large femoral head (over 50mm diameter ideal)
- Normal hip anatomy (no dysplasia)
- Good femoral neck geometry
- No femoral head cysts
- Primary osteoarthritis preferred
- Post-traumatic arthritis acceptable
- Inflammatory arthritis (relative contraindication)
Female patients have 2-3 times higher failure rate than males. This is due to smaller femoral head size (leading to smaller components and higher wear), thinner femoral neck (higher fracture risk), and possibly hormonal effects on bone quality. This became one of the reasons to abandon the procedure.
Anatomy and Biomechanics
Femoral head blood supply (critical for resurfacing):
The femoral head receives blood supply from:
- Medial femoral circumflex artery (MFCA) - primary supply (60-80%)
- Deep branch supplies superior and posterior head
- Travels in capsular reflection
- Lateral femoral circumflex artery - minor contribution
- Artery of ligamentum teres - variable (often inadequate alone)
- Intraosseous supply from femoral neck
Hip resurfacing compromises femoral head blood supply through:
- Surgical dislocation disrupting capsular vessels
- Reaming and thermal necrosis during preparation
- Cement exotherm if cemented components used This contributes to AVN risk and femoral neck fracture.
Femoral neck anatomy considerations:
- Clinical Significance
- Varus increases fracture risk, valgus preferred
- Clinical Significance
- Narrow neck (under 35mm) is contraindication
- Clinical Significance
- Notching during preparation increases fracture risk
- Clinical Significance
- Cysts or osteoporosis are contraindications
- Resurfacing uses large femoral heads (40-60mm diameter)
- Larger heads reduce volumetric wear (lower liner velocity)
- Improved stability and range of motion
- BUT higher contact stresses and edge loading if malpositioned
- Normal hip: load transfers through cancellous bone of femoral head
- Resurfacing: load transfers through metal cap into remaining femoral head
- Stress concentration at bone-implant interface
- Stress shielding can weaken femoral neck over time
While large diameter heads reduce volumetric wear, they increase surface area and thus total metal debris production. This is why MoM resurfacing failed despite theoretically better tribology than small diameter MoM bearings in conventional THA.
Classification Systems
Major hip resurfacing systems:
- Company
- Smith & Nephew
- Key Features
- First modern MoM resurfacing, best long-term data
- Status
- Still available but rarely used
- Company
- DePuy
- Key Features
- Single-use instruments, recalled 2010
- Status
- Withdrawn
- Company
- Wright Medical
- Key Features
- Press-fit acetabular component
- Status
- Withdrawn 2013
- Company
- Corin
- Key Features
- Hybrid fixation
- Status
- Limited use
- Company
- Zimmer
- Key Features
- High carbon content metal
- Status
- Withdrawn
- Introduced 1997 by Derek McMinn
- Cast high-carbon cobalt-chromium alloy
- Cemented femoral component
- Uncemented acetabular component
- Best registry data of all resurfacing systems
- Even BHR showed higher revision rate than conventional THA
- Introduced 2003 as easier alternative to BHR
- Shallow acetabular component (high edge-loading)
- Poor femoral component design
- Exceptionally high failure rates led to recall
- Became the poster child for MoM failure
Understanding these implant differences helps explain why some patients did better than others with resurfacing.
Clinical Assessment
- Symptoms of hip arthritis (pain, stiffness, functional limitation)
- Previous hip procedures or trauma
- Activity level and goals
- Medical comorbidities (renal disease critical)
- Medication allergies (metal sensitivity)
- Occupation and sports participation
- Gait assessment
- Hip range of motion (flexion, abduction, rotation)
- Leg length discrepancy
- Trendelenburg test (abductor function)
- Lumbar spine examination (referred pain)
- Key Points
- Male, young, active, large frame
- Decision Impact
- Core indication criterion
- Key Points
- DEXA scan if osteoporosis suspected
- Decision Impact
- Contraindication if T-score under -2.5
- Key Points
- Measure femoral head size on AP X-ray
- Decision Impact
- Under 50mm diameter is contraindication
- Key Points
- Assess for dysplasia, deformity, cysts
- Decision Impact
- Abnormal anatomy is contraindication
- Key Points
- Creatinine and eGFR
- Decision Impact
- Renal disease is contraindication
- Key Points
- Modern THA outcomes and options
- Decision Impact
- Most patients better with conventional THA
If considering hip resurfacing today (which is rare), honest patient counseling is essential. Patients must understand that conventional THA has better outcomes with lower complication rates. The theoretical benefits of bone preservation do not outweigh the real risks of ALVAL, pseudotumor, and femoral neck fracture.
Differential diagnosis of the painful hip resurfacing:
A patient with pain after resurfacing (or a painful MoM hip) requires a structured differential. The signature resurfacing-specific causes are femoral neck fracture and adverse reaction to metal debris (ARMD), but infection and referred pain must always be excluded.
- Typical clue
- Sudden severe pain, unable to weight bear, often within first 2 years
- Key discriminator / test
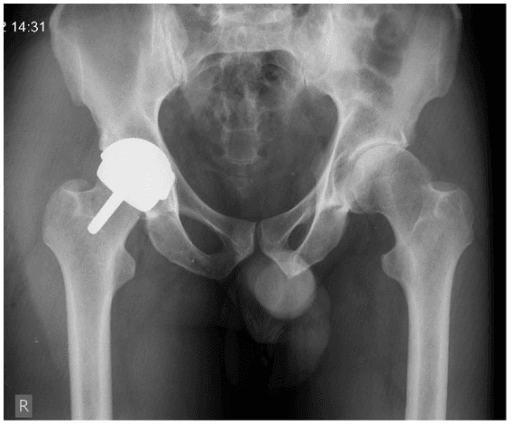
- Plain radiograph shows subcapital/transcervical fracture under the cap - surgical emergency
- Typical clue
- Insidious groin or buttock pain, swelling, clunking; raised or rising Co/Cr
- Key discriminator / test
- MARS-MRI or ultrasound shows fluid collection or soft-tissue mass; type IV hypersensitivity histology [PMID 19949118]
- Typical clue
- Rest pain, warmth, raised CRP/ESR, sinus
- Key discriminator / test
- Joint aspiration (culture, synovial WCC) - MUST exclude before attributing pain to metal debris
- Typical clue
- Start-up pain, progressive; lucent lines or migration
- Key discriminator / test
- Serial radiographs (EBRA), absent infection markers
- Typical clue
- Anterior groin pain on active hip flexion; oversized or uncovered acetabular component
- Key discriminator / test
- Reproduced on resisted flexion; dynamic ultrasound; diagnostic injection
- Typical clue
- Pain with retained bone stock; risk if AVN was original diagnosis
- Key discriminator / test
- MRI (MARS); often a contraindication that was overlooked
- Typical clue
- Back-dominant pain, radicular features, normal hip exam
- Key discriminator / test
- Spinal examination and imaging; hip injection negative
Investigations
- Measure femoral head diameter (both hips for comparison)
- Assess acetabular bone stock
- Look for dysplasia (center-edge angle, acetabular index)
- Identify osteophytes and cysts
- Assess bone quality
- Assess anterior femoral neck shape
- Look for cam impingement morphology
- Evaluate femoral head sphericity
- Femoral head diameter (must be over 50mm)
- Neck-shaft angle (varus is contraindication)
- Femoral neck width (must be over 35mm)
- Assess femoral head cysts (size and location)
- Evaluate femoral neck geometry
- Measure bone quality
- Rule out AVN if suspected
- Assess soft tissue pathology
- Evaluate cartilage loss patterns
- Full blood count
- Renal function (creatinine, eGFR) - critical
- Liver function
- Metal allergy testing (if history suggestive)
- Cobalt (baseline should be under 1 microgram per L)
- Chromium (baseline should be under 1 microgram per L)
- Establishes pre-operative baseline for future monitoring
Obtaining baseline metal ion levels pre-operatively is essential. This allows comparison with post-operative levels and helps distinguish implant-related elevation from other sources (dietary cobalt, occupational exposure).
Management Decision-Making
-
Conservative management first
- Activity modification
- Physiotherapy and core strengthening
- NSAIDs and analgesia
- Weight loss if applicable
- Intra-articular steroid injection
-
Surgical options when conservative fails:
- Ceramic-on-polyethylene bearing (most common)
- Ceramic-on-ceramic bearing (ultra-low wear)
- Excellent long-term outcomes (over 95% survival at 15 years)
- Established monitoring protocols
- Well-understood complication profile
- Hip arthroscopy for FAI (if primarily labral/cartilage pathology)
- Periacetabular osteotomy for dysplasia
- Femoral osteotomy for deformity
- Only in exceptional circumstances
- Young male with very large femoral head
- Patient insists after full counseling
- Surgeon experienced with technique
The vast majority of young patients are better served with conventional THA using modern bearing surfaces.
Surgical Technique
- Patient lateral decubitus
- Standard posterior incision
- Detach external rotators and capsule
- Posterior dislocation of hip
- Excellent femoral head exposure
- Familiar to most surgeons
- Good visualization of femoral head
- Easier to achieve valgus positioning
- Disrupts posterior capsule and blood supply
- Higher dislocation risk (mitigated by large head)
- External rotator repair required
- Patient supine
- Interval between TFL and gluteus medius
- Anterior hip capsulotomy
- Anterior dislocation
- Preserves posterior structures
- Lower dislocation risk
- May preserve some blood supply
- More difficult femoral exposure
- Risk of abductor damage
- Challenging to achieve valgus position
The posterior approach remains most popular for surgeons still performing resurfacing.
Complications
- Incidence
- 1-2% per year (first 5 years)
- Management
- Urgent revision to conventional THA
- Incidence
- 10-15% (symptomatic)
- Management
- Revision to THA with soft tissue debridement
- Incidence
- 5-10%
- Management
- Revision surgery, may need extensive debridement
- Incidence
- Common (over 50% have some elevation)
- Management
- Monitor levels, revise if over 7 micrograms per L
- Incidence
- 5-10% at 10 years
- Management
- Revision to THA
- Incidence
- 3-5% at 10 years
- Management
- Revision with bone grafting if needed
- Incidence
- Under 1% (large head protective)
- Management
- Closed reduction, rarely requires revision
- Incidence
- Under 1%
- Management
- Debridement or revision as per THA protocols
- Incidence
- 5-10%
- Management
- NSAIDs or radiation prophylaxis
- Incidence
- 1-2%
- Management
- Leads to collapse and need for revision
- Sudden onset hip pain
- Unable to weight bear
- Usually within first 2 years (but can occur later)
- Female gender
- Small femoral head (under 50mm)
- Varus component positioning
- Anterior neck notching
- Pre-existing cysts or AVN
- Osteoporosis
- Urgent revision to conventional THA
- Remove femoral resurfacing component
- Prepare femoral canal for stem
- Usually requires cemented stem due to bone loss
- Good outcomes if treated promptly
Femoral neck fractures after resurfacing are typically subcapital or transcervical. They occur from combination of stress concentration under the component, compromised blood supply, and mechanical factors (varus, notching). The fracture propagates from the tensile (superior) side.
- Type IV delayed hypersensitivity reaction to metal debris
- Lymphocytic and plasma cell infiltration
- Perivascular inflammation and necrosis
- Leads to soft tissue destruction
- Pain (commonest symptom)
- Soft tissue mass (pseudotumor)
- May be asymptomatic with only elevated metal ions
- Can cause nerve compression or muscle necrosis
- Elevated blood metal ions (cobalt and chromium over 7 micrograms per L)
- MRI shows soft tissue masses and fluid collections
- Metal artifact reduction sequence (MARS) MRI protocol
- Ultrasound can also show pseudotumors
- Revision surgery required
- Remove both components (even if acetabulum looks good)
- Thorough debridement of necrotic tissue
- Revise to conventional THA (ceramic or polyethylene bearing)
- Warn patient that soft tissue damage may be permanent
- Soft tissue mass from organized inflammatory response
- Can be cystic or solid
- May cause pain, swelling, nerve compression
- Associated with high metal ions
- Type 1: Fluid-filled cysts
- Type 2: Solid masses
- Type 3: Mixed solid and cystic
- MRI best for detection
- May be large (up to 10cm or more)
- Often posterior to hip
- Revision surgery with pseudotumor excision
- May require extensive soft tissue debridement
- Outcomes variable depending on tissue damage
- Baseline pre-operative cobalt and chromium
- Check at 6 months post-op
- Then annually lifelong
- More frequent if symptomatic or concerning trend
- Normal: under 2 micrograms per L
- Moderate elevation: 2-7 micrograms per L (monitor closely)
- High: over 7 micrograms per L (consider revision)
- Component malposition (edge loading)
- Large component size (more surface area)
- Poor component seating
- ALVAL or pseudotumor
Very high metal ion levels (over 20 micrograms per L) can cause systemic toxicity including neurological symptoms, cardiomyopathy, and thyroid dysfunction. This is rare but documented. Patients with high ions need multi-system assessment before revision.
Beyond the local hip problem, very high systemic cobalt from a failing MoM bearing can cause arthroprosthetic cobaltism, a recognised multi-system toxicity that examiners expect you to name. The constellation includes a dilated cardiomyopathy (the most dangerous, potentially fatal), neurological features (peripheral neuropathy and, characteristically, optic and auditory impairment — visual change and sensorineural hearing loss), hypothyroidism/goitre, polycythaemia and cognitive/psychiatric changes. It is classically described with markedly elevated blood cobalt (often well above 20 micrograms per L) and is especially seen after revision of a fractured ceramic bearing to a metal-on-metal articulation, where retained ceramic debris acts as an abrasive and accelerates cobalt release. Management is source control — urgent removal/revision of the metal bearing (cobalt falls once the source is gone), supported by cardiology, endocrine and neurology assessment; chelation has only an adjunctive, unproven role. The exam point: in a MoM/resurfacing patient with new cardiac, visual, auditory or thyroid symptoms, check the cobalt and think systemic cobaltism, not coincidence.
Converting a failed MoM resurfacing to a conventional THA is technically and biologically harder than a standard revision, and outcomes are correspondingly worse (registry re-revision rates after a failed resurfacing are high). The reason is the soft-tissue destruction caused by ARMD/ALVAL — the metal debris and pseudotumour necrose the hip abductors and capsule, so even after the bearing is removed the hip is left unstable, with a markedly raised dislocation rate. This drives the reconstruction: surgeons frequently need larger femoral heads, a dual-mobility cup or even a constrained liner to compensate for the deficient soft-tissue envelope, and must debride necrotic tissue thoroughly while accepting that abductor function may not recover. The corollary principle is to revise early — before the pseudotumour has destroyed the abductors — rather than watching a symptomatic, ion-rising hip drift toward irreversible soft-tissue loss. The exam point: the threat after resurfacing failure is not just removing the metal, it is the unstable, soft-tissue-deficient hip the metal leaves behind.
Postoperative Care and Monitoring
Immediate post-operative care:
- Standard post-operative analgesia
- DVT prophylaxis (mechanical and chemical)
- Mobilize same day or next day with physiotherapy
- Weight bearing as tolerated (cement sets immediately)
- Hip precautions if posterior approach (avoid flexion over 90 degrees, internal rotation)
- Progressive mobilization
- Continue hip precautions for 6 weeks (posterior approach)
- Outpatient physiotherapy
- Wound monitoring
- Discontinue DVT prophylaxis at 4-6 weeks
- Discharge from hip precautions
- Progressive strengthening
- Return to light activities
- Driving when safe (usually 6-8 weeks)
- Full range of motion exercises
- Progressive return to activities
- Impact activities after 6 months
- Return to sports gradual
- First surveillance appointment at 6 months
- 6 weeks (wound check, early mobilization)
- 6 months (first metal ions, X-ray)
- Annually lifelong thereafter
-
Clinical assessment:
- Pain assessment (any new or worsening pain)
- Function questionnaire (Oxford Hip Score, WOMAC)
- Examination (range of motion, stability, swelling)
- Any systemic symptoms (neurological, thyroid, cardiac)
-
Radiographs:
- AP pelvis
- Lateral hip
- Look for lucent lines, component migration
- Assess for fracture or AVN
-
Blood metal ion levels:
- Whole blood cobalt and chromium
- Trend over time is important (rising levels concerning)
-
MRI if indicated:
- Pain not explained by X-ray
- Elevated or rising metal ions
- Palpable mass or swelling
- Use MARS protocol to reduce metal artifact
Rising metal ion levels are more concerning than absolute values. A patient with stable ions at 5 micrograms per L may be observed, but a patient rising from 2 to 5 micrograms per L over 2 years warrants urgent MRI and consideration for revision. Rate of change matters.
- Walking, swimming, cycling, golf
- Low-impact sports
- Gym work avoiding impact
- Daily living activities without restriction
- High-impact sports (running, jumping)
- Contact sports
- Heavy lifting (over 20kg repeatedly)
- Activities with high fall risk
- Most patients achieve good function
- Pain relief usually excellent initially
- May deteriorate over time with complications
- Higher revision rate than conventional THA
- Need lifelong monitoring commitment
Outcomes and Registry Data
Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) data:
The AOANJRR has been critical in documenting the failure of hip resurfacing.
- Hip resurfacing: 15-20% at 10 years
- Conventional THA (ceramic-on-polyethylene): 5-7% at 10 years
- Conventional THA (ceramic-on-ceramic): 4-6% at 10 years
- Male resurfacing: 12-15% at 10 years
- Female resurfacing: 25-30% at 10 years
- Gender difference is highly significant
- Primary OA: 15% at 10 years
- AVN: 30-40% at 10 years (should be contraindication)
- Developmental dysplasia: 25-30% at 10 years
- Birmingham Hip Resurfacing: 15% at 10 years (best performer)
- ASR: 40% at 6 years (withdrawn)
- Conserve Plus: 25% at 8 years (withdrawn)
- Femoral fracture (30%)
- Loosening (25%)
- ALVAL/adverse soft tissue reaction (20%)
- Pain (unexplained) (15%)
- Infection (5%)
- Dislocation (under 5%)
The AOANJRR data was instrumental in documenting the failure of hip resurfacing in real-world practice. While some surgeons reported excellent results in selected patients, the registry showed that across the board, resurfacing underperformed conventional THA. This led to the dramatic decline in usage.
- Similar findings to AOANJRR
- 15-year revision rate for resurfacing 18% vs 8% for THA
- Female revision rate double that of males
- Higher revision rates for resurfacing in all age groups
- Benefit not seen even in young patients
- Hip Resurfacing
- 80-85%
- Modern THA
- 95%
- Hip Resurfacing
- Good-excellent 75%
- Modern THA
- Good-excellent 90%
- Hip Resurfacing
- Variable data
- Modern THA
- Similar or better
- Hip Resurfacing
- Under 1%
- Modern THA
- 2-3%
- Hip Resurfacing
- Straightforward
- Modern THA
- Standard
- Hip Resurfacing
- Lifelong
- Modern THA
- Standard
The data clearly shows conventional THA is superior in almost all metrics.
Guidelines, Registries & Global Practice
Global epidemiology and current role:
Metal-on-metal hip resurfacing (MoMHRA) was used worldwide as a bone-conserving alternative to THA for young, active patients, peaking around 2006-2008. Following the 2010 DePuy ASR recall and registry evidence of excess revision, global usage collapsed to a small fraction of its peak. The candidate population was always small: even in the most favourable registry analyses, only a minority of patients (men under 65 with primary osteoarthritis and a large femoral head over 50 mm) achieved survivorship comparable to THA. [PMID 23036895; 20012720]
Registry evidence (side by side):
- Key finding
- In women, resurfacing was inferior to stemmed THR at every head size (5-yr revision 6-8% versus ~1.5% for cemented MoP THR); acceptable only in men with large heads
- Source
- Smith et al. Lancet 2012 [PMID 23036895]
- Key finding
- Higher cumulative revision than THA overall (5-yr CRR ~3.7% versus 2.7%); equivalent only in men under 65 with primary OA (2.5% versus 2.8%); ASR an outlier and recalled
- Source
- Corten & MacDonald, CORR 2010 [PMID 20012720]
- Key finding
- All registries showed increased revision for large-head MoM and resurfacing versus other bearings; outcome device-dependent
- Source
- Graves et al. JBJS Am 2011 [PMID 22262422]
- Key finding
- Best-case durability: ten-year survival 98% in men with the Birmingham implant
- Source
- Treacy et al. JBJS Br 2011 [PMID 21196539]
Major guidance, side by side:
- Position on MoM resurfacing
- Lifelong surveillance of all MoM hip patients - annual clinical review, whole-blood cobalt and chromium, and cross-sectional imaging (MARS-MRI or ultrasound) if symptomatic or with rising/raised ions
- Position on MoM resurfacing
- THA implants should meet a benchmark revision rate; resurfacing is not recommended for the general arthritic population and is reserved, if at all, for highly selected young men
- Position on MoM resurfacing
- FDA approved specific resurfacing devices (e.g. BHR) for a narrow indication (younger men, larger heads); MoM total hips and most resurfacing systems have been withdrawn or restricted; emphasis on shared decision-making and surveillance
- Position on MoM resurfacing
- Registry-driven consensus that resurfacing is not indicated in women and only in carefully selected men; THA with a non-MoM bearing is the default for young active patients
Metal ion / imaging thresholds (regulatory consensus):
- Action
- Cross-sectional imaging (MARS-MRI or ultrasound) and closer review
- Action
- Repeat and image - rate of change matters more than a single value [PMID 23482990]
- Action
- Consider revision to a non-MoM THA
Global practice variation:
- In high-resource settings, resurfacing is now rare and concentrated in a few specialist surgeons treating young men; established patients are kept under lifelong surveillance pathways.
- In lower-resource settings, the original attraction (bone preservation, lower cost than some THA constructs, large stable head) has faded as the surveillance burden, metal ion testing and revision complexity outweigh any saving.
- Wherever performed, informed consent must document the higher revision rate versus THA, the contraindications excluded, and the commitment to lifelong monitoring.
For any orthopaedic exam, know that hip resurfacing is largely historical rather than current practice. Understand the complications (ARMD/ALVAL, femoral neck fracture, elevated metal ions), why it failed (the metal-on-metal bearing), and that conventional THA with a non-MoM bearing is superior. If asked about a young patient, recommend modern THA; reserve resurfacing only for a counselled young man with a large femoral head and primary OA.
MCQ Practice Points
Q: What bearing surface is used in hip resurfacing arthroplasty? A: Metal-on-metal (MoM) only. This is the fundamental problem with the procedure - metal debris from the large diameter MoM bearing causes ALVAL and pseudotumors.
Q: What is ALVAL in the context of hip resurfacing? A: Aseptic Lymphocytic Vasculitis-Associated Lesion - a type IV delayed hypersensitivity reaction to metal debris from the MoM bearing. Characterized by lymphocytic infiltration, perivascular inflammation, and soft tissue necrosis. Occurs in 10-15% of patients.
Q: What are absolute contraindications to hip resurfacing? A: Female gender (2-3x higher failure rate), small femoral head (under 50mm), AVN (high fracture risk), large femoral head cysts (over 1cm), renal disease (cannot clear metal ions), osteoporosis, and metal allergy.
Q: According to the AOANJRR, what is the 10-year cumulative revision rate for hip resurfacing compared to conventional THA? A: Hip resurfacing 15-20% vs conventional THA 5-7%. This disparity led to abandonment of hip resurfacing by most surgeons.
Q: What blood metal ion level should prompt consideration for revision surgery in a patient with hip resurfacing? A: Levels over 7 micrograms per L (for cobalt or chromium) should prompt urgent MRI and consideration for revision. Rising levels are more concerning than absolute values.
Q: What was the ASR and why was it recalled? A: The ASR (Articular Surface Replacement) was a DePuy hip resurfacing system that had 40% revision rate at 6 years due to high rates of ALVAL, pseudotumors, and component failure. It was recalled worldwide in August 2010, marking the beginning of the decline in hip resurfacing.
At a Glance Table
- Key Information
- Bone-conserving hip replacement - resurface femoral head with metal cap, metal acetabular component
- Key Information
- Metal-on-metal (MoM) only - THIS IS THE PROBLEM
- Key Information
- Popular 2000-2010, declined over 95% since ASR recall (2010)
- Key Information
- Essentially abandoned - rarely performed except exceptional cases
- Key Information
- ALVAL (10-15%), femoral neck fracture (1-2% per year), pseudotumor (5-10%)
- Key Information
- 15-20% at 10 years (vs 5-7% for conventional THA)
- Key Information
- Young male, large femoral head (over 55mm), excellent bone quality, primary OA
- Key Information
- Female gender, small head (under 50mm), AVN, cysts, renal disease, osteoporosis
- Key Information
- Annual blood metal ions (cobalt, chromium), X-rays, MRI if symptomatic
- Key Information
- Documented failure - higher revision rate in all patient groups vs THA
- Key Information
- Conventional THA with ceramic-on-polyethylene or ceramic-on-ceramic bearing
- Key Information
- Historical procedure with proven problems - conventional THA is superior
This table provides a rapid overview of why hip resurfacing has been largely abandoned in modern orthopaedic practice.
METALMETAL - Metal-on-Metal Complications
Hook:METAL reminds you of the metal-on-metal complications that ended hip resurfacing
ASRASR - The Failed Implant
Hook:ASR was the most notorious failure in hip resurfacing history - know this for exam context
FRACTUREFRACTURE - Femoral Neck Fracture Risk Factors
Hook:FRACTURE lists the risk factors for the most common early failure mode
YOUNGYOUNG MALE - Ideal Candidate Profile (Historical)
Hook:YOUNG MALE describes the very narrow indication (now largely abandoned)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male engineer presents with severe hip OA. He has researched hip resurfacing online and wants to know if he is a candidate. He is concerned about the limitations after conventional THA. How do you counsel him?”
“A 52-year-old male had Birmingham Hip Resurfacing 8 years ago. Annual surveillance shows his cobalt level has risen from 3 to 8 micrograms per L over 2 years. He has mild hip pain. What is your assessment and management?”
“A 48-year-old female with hip resurfacing 18 months ago presents to ED with sudden onset severe hip pain after a minor slip. X-ray shows a displaced subcapital femoral neck fracture under the resurfacing component. How do you manage this?”
HISTORICAL CONTEXT
- Bone-preserving alternative to THA (2000-2010)
- Peak usage 2008-2010, then declined 95%
- ASR recall (2010) marked beginning of end
- ALVAL recognition (2011-2015) led to abandonment
- Now rarely performed except exceptional cases
METAL-ON-METAL PROBLEMS
- Metal debris generates cobalt and chromium ions
- ALVAL: aseptic lymphocytic vasculitis (10-15%)
- Pseudotumors: soft tissue masses from debris
- Elevated blood metal ions require monitoring
- Systemic toxicity possible with very high levels
MAJOR COMPLICATIONS
- Femoral neck fracture: 1-2% per year (first 5 years)
- ALVAL: 10-15% (requires revision to THA)
- Pseudotumor: 5-10% (extensive debridement needed)
- Higher revision rate: 15-20% at 10 years vs 5-7% THA
- Metal ion elevation: common (over 50% some elevation)
ABSOLUTE CONTRAINDICATIONS
- Female gender (2-3x higher failure rate)
- Small femoral head (under 50mm diameter)
- AVN of femoral head
- Large femoral head cysts (over 1cm)
- Renal disease (cannot clear metal ions)
- Osteoporosis
- Metal allergy or hypersensitivity
CURRENT ROLE (2024)
- Extremely limited - most surgeons abandoned technique
- Occasionally: young male, large head (over 55mm), excellent bone
- Must counsel about higher revision rate than THA
- Lifelong metal ion monitoring required
- Modern THA preferred in almost all cases
MONITORING PROTOCOL
- Blood cobalt and chromium annually lifelong
- Plain X-rays annually
- MRI if symptomatic or ions over 7 micrograms per L
- Rising ions more concerning than absolute value
- Revision indicated if ALVAL on MRI or ions over 7 persistently
AOANJRR KEY DATA
- Hip resurfacing: 15-20% revision at 10 years
- Modern THA: 5-7% revision at 10 years
- Birmingham Hip: best performer (still inferior to THA)
- ASR: 40% revision at 6 years (recalled)
- Female revision rate double male rate
EXAM TRAPS
- Don't recommend resurfacing over modern THA
- Know it's historical, not current best practice
- ALVAL is signature complication
- Female gender is absolute contraindication
- Registry data proves THA is superior
Evidence Base
- Analysis of 434,560 primary hip replacements (31,932 resurfacings) from the NJR. In women, resurfacing gave worse survival than stemmed THR at every head size: predicted 5-year revision in a 55-year-old woman was 8.3% with a 42 mm head and 6.1% with a 46 mm head, versus 1.5% for a 28 mm cemented metal-on-polyethylene THR. In men, only large heads performed acceptably (4.1% at 46 mm versus 2.6% at 54 mm).
- In 660 MoM resurfacings and large-head MoM THRs, 3.4% required revision for adverse reaction to metal debris (ARMD), all in ASR bearings. The ARMD group had significantly smaller components, higher acetabular anteversion (edge loading) and higher whole-blood chromium and cobalt (all p less than 0.001). Well-positioned implants with ARMD usually showed high component wear.
- In 1419 MoM resurfacings, the 8-year cumulative revision rate for pseudotumour was 4% overall but only 0.5% in men, 6% in women over 40, and 13.1% at 6 years in women under 40. Female gender, age under 40, small components and dysplasia were significant risk factors; gender and age were independent on Cox modelling.
- Across 3497 Birmingham hip resurfacings by 89 surgeons, femoral neck fracture occurred in 1.46% (1.91% women versus 0.98% men; relative risk 1.95, p less than 0.01). Mean time to fracture was 15.4 weeks. Varus component placement, intra-operative femoral neck notching and technical problems were present in 85% of cases.
- Single-surgeon series of 144 BHRs (130 patients). Ten-year survival was 98.0% in men and 95.5% overall with aseptic revision as endpoint (93.5% including septic revisions). Median modified Oxford hip score 4.2% and median UCLA score 7.0 at ten years.
- Pooled registry review: resurfacing (SRA) had a higher overall 5-year cumulative revision rate than THA (Australian registry 3.7% versus 2.7%), BUT men under 65 with primary OA had equivalent results (2.5% versus 2.8%). Heads over 50 mm predicted better SRA survival. Re-revision of failed SRA was poor (11% at 5 years).
- Resurfacing carries a higher cumulative revision rate than conventional THA across patient groups; women have a markedly higher revision rate than men; the DePuy ASR was identified as an outlier and subsequently recalled. Resurfacing volume has fallen to a small fraction of its peak.