Iliac Crest Contusion | Contact Sports | Functional Recovery Focus
- Direct blow to iliac crest causes subperiosteal hematoma
- Pain with hip flexion/abduction and trunk rotation characteristic
- Rule out avulsion fracture in adolescents with X-ray
- Functional rehabilitation focuses on core and hip stabilizers
- Protective padding essential for return to contact sports
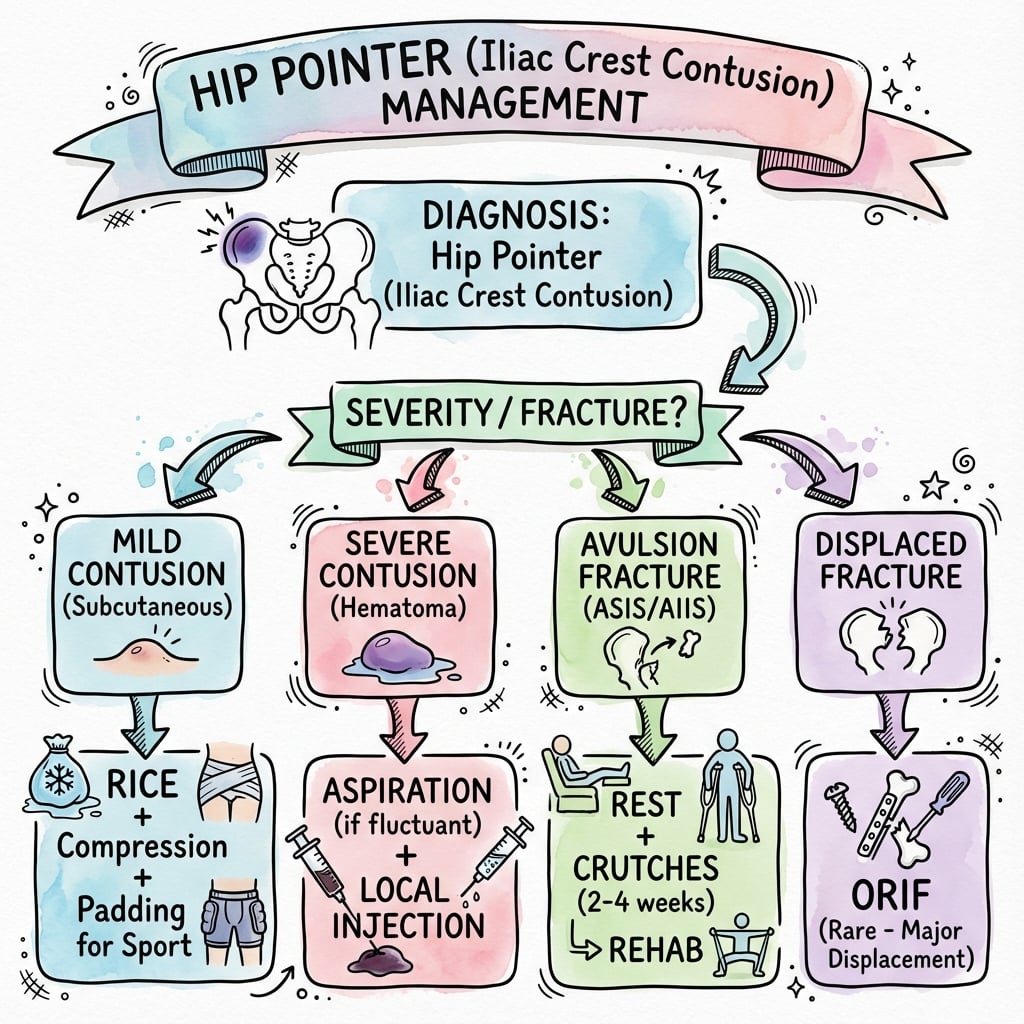
- “Hip pointer is NOT a fracture - it's a contusion with subperiosteal hematoma
- “Adolescents may have apophyseal avulsion - always X-ray if severe
- “Abdominal wall weakness may persist - ensure core strength before RTS
- “Padding placement is critical - must cover entire iliac crest
Iliac crest apophysis in adolescents vulnerable to avulsion. Attachment of abdominal obliques, transversus, and gluteal muscles make this area prone to injury.
Must rule out: ASIS/AIIS avulsion fractures, iliac wing fracture, intra-abdominal injury, hip pathology, and referred lumbar pain.
Subperiosteal hematoma size correlates with recovery time. Large hematomas may calcify. Core muscle involvement prolongs rehabilitation.
Full hip ROM, core strength, and sport-specific function required. Protective padding mandatory for first 2-4 weeks of contact.
- Clinical Features
- Localized tenderness, minimal swelling, normal gait
- Expected Recovery
- 1-2 weeks
- Key Management
- Ice, NSAIDs, relative rest, progress as tolerated
- Clinical Features
- Visible swelling, antalgic gait, pain with hip motion
- Expected Recovery
- 2-4 weeks
- Key Management
- Protected rest, gradual ROM, core rehab, padding
- Clinical Features
- Severe pain, unable to ambulate, significant hematoma
- Expected Recovery
- 4-6+ weeks
- Key Management
- X-ray to rule out fracture, consider aspiration, structured rehab
- Clinical Features
- Adolescent, sudden pop, unable to weight bear (iliac crest site is rare)
- Expected Recovery
- 6-12 weeks
- Key Management
- X-ray confirmation; mostly conservative; individualised surgery if significantly displaced or non-union
CORECORE - Return to Sport Criteria
Hook:Athletes need a strong CORE before return to contact
AVULSIONAVULSION - Adolescent Red Flags
Hook:AVULSION signs in adolescents require X-ray and orthopedic referral
Overview and Epidemiology
Hip pointer is a contusion to the iliac crest resulting in a subperiosteal hematoma and surrounding soft tissue injury. Despite the colloquial name, it does not involve the hip joint itself.
- Direct blow - helmet, knee, or shoulder strike to iliac crest
- Fall onto hard surface - lateral fall with direct impact
- Collision sports - tackle or body check impact
- American football - most common (especially running backs, linebackers)
- Rugby - high tackle situations
- Ice hockey - board checks
- Australian Rules Football - contested marking
- Combat sports - knee strikes to body
Hip pointer is a misnomer - it involves the iliac crest, not the hip joint. The name likely derives from the iliac crest being a bony prominence that "points out" from the pelvis. Be precise in clinical documentation.
Pathophysiology and Mechanisms
- Subcutaneous bony prominence from ASIS to PSIS
- Site of muscle attachments: external oblique, internal oblique, transversus abdominis, latissimus dorsi, gluteus medius, tensor fasciae latae
- Covered only by thin subcutaneous tissue - vulnerable to direct trauma
- Iliac crest apophysis appears at 13-15 years
- Fuses to ilium between 15-21 years
- Multiple ossification centers along length
- Vulnerable to avulsion injuries before fusion
Hip Pointer Evolution
Direct impact causes periosteal disruption. Subperiosteal hematoma forms as bleeding occurs beneath the periosteum. Significant pain with any muscle contraction pulling on the crest.
Hematoma organizes. Inflammatory response peaks. Surrounding muscle spasm develops. Maximum swelling and pain typically at 48 hours.
Inflammation begins to resolve. Hematoma absorption starts. Gentle ROM can begin. Muscle function gradually returns.
Progressive healing. Subperiosteal hematoma resolves or calcifies. Return of normal muscle function. Sport-specific rehabilitation progresses.
Subperiosteal calcification may develop in 10-15% of significant hip pointers, especially if aggressive mobilization occurs too early. This is benign and usually resolves but may prolong symptoms.
The periosteum is highly innervated and sensitive. Subperiosteal hematoma stretches the periosteum, causing severe pain. Additionally, multiple powerful trunk muscles attach here - any contraction causes tension on the injured periosteum.
Classification Systems
Clinical Severity Grading (most commonly used)
- Symptoms
- Localized pain, minimal swelling
- Gait
- Normal
- Muscle Function
- Mild weakness with resisted testing
- Recovery
- 1-2 weeks
- Symptoms
- Moderate swelling, ecchymosis
- Gait
- Antalgic
- Muscle Function
- Moderate weakness, pain with activity
- Recovery
- 2-4 weeks
- Symptoms
- Severe pain, significant swelling
- Gait
- Unable to ambulate
- Muscle Function
- Significant weakness, unable to contract
- Recovery
- 4-6+ weeks
Grade III injuries should prompt X-ray imaging to rule out iliac wing fracture or apophyseal avulsion. Consider aspiration for large tense hematomas.
Grading helps predict recovery timeline and guides treatment intensity.
History
- Mechanism - direct blow vs fall vs muscle contraction
- Force and direction - helmet strike vs knee vs ground
- Immediate symptoms - able to continue playing?
- Associated symptoms - abdominal pain, hip symptoms
- Age - adolescent with open apophysis?
- Abdominal pain or rigidity (intra-abdominal injury)
- Hip joint symptoms (intra-articular pathology)
- Numbness or weakness in leg (nerve involvement)
- Severe pain out of proportion (compartment syndrome rare)
Thorough history helps differentiate contusion from more serious injury patterns.
POINTERPOINTER - Clinical Assessment
Hook:A hip POINTER examination should cover all these points systematically
Examination
Physical examination
- Swelling location and extent
- Ecchymosis (may track to hip/thigh)
- Asymmetry compared to opposite side
- Gait assessment
- Point tenderness over iliac crest
- Palpable hematoma or defect
- Comparison to uninjured side
- Abdominal wall tenderness
- Active and passive hip ROM
- Trunk flexion, rotation, side-bending
- Pain with resisted hip abduction
- Pain with resisted trunk rotation
- Hip abductors (gluteus medius)
- Hip flexors (rectus femoris, iliopsoas)
- Trunk obliques
- Compare to uninjured side
Comprehensive examination rules out associated injuries and guides severity grading.
Investigations
- Not routinely required for typical contusion
- Indicated if: adolescent, severe injury, suspected fracture, not improving
- AP pelvis and oblique views of affected side
- Look for: avulsion, iliac wing fracture, widened apophysis
- Useful for assessing hematoma size
- Can guide aspiration if needed
- Shows subperiosteal fluid collection
- Dynamic assessment of muscle integrity
- Reserved for diagnostic uncertainty
- Shows extent of soft tissue injury
- Identifies bone marrow edema
- Useful for persistent symptoms
X-ray is indicated for: all adolescents with significant injury, suspected fracture, Grade III severity, or failure to improve after 2-3 weeks. Most mild-moderate adult hip pointers do not require imaging.
- Discriminating Features
- Direct blow, point tenderness on crest, pain with trunk rotation, normal hip joint
- Key Investigation
- Clinical; ultrasound for haematoma
- Why It Matters
- Benign; conservative care
- Discriminating Features
- Adolescent, sudden forceful contraction (sprint, kick), audible pop, no contact needed
- Key Investigation
- AP pelvis radiograph
- Why It Matters
- Far commoner avulsion than iliac crest; may alter RTS timeline
- Discriminating Features
- Adolescent, severe swelling, unable to weight bear
- Key Investigation
- AP pelvis radiograph
- Why It Matters
- Rare (3 of 203 in Rossi & Dragoni); usually conservative
- Discriminating Features
- High-energy mechanism, diffuse pelvic pain, possible instability
- Key Investigation
- Pelvic radiograph / CT
- Why It Matters
- May indicate higher-energy injury; assess pelvic ring
- Discriminating Features
- Lateral abdominal wall pain, pain on resisted trunk rotation, possible 2cm aponeurotic detachment
- Key Investigation
- MRI
- Why It Matters
- Rare operative variant on the hip pointer spectrum
- Discriminating Features
- Abdominal pain/rigidity, haemodynamic change, referred pain
- Key Investigation
- FAST / CT abdomen
- Why It Matters
- Life-threatening - never miss with flank/pelvic trauma
- Discriminating Features
- Burning/numbness anterolateral thigh, LFCN distribution
- Key Investigation
- Clinical; nerve block if uncertain
- Why It Matters
- Nerve, not bone - different management
- Discriminating Features
- Axial back pain, radicular features, no local crest tenderness
- Key Investigation
- Lumbar examination / MRI
- Why It Matters
- Source is spine, not pelvis
Management Algorithm
- 1Initial Assessment
History, examination, grade severity
Determine Grade I, II, or III
- 2Imaging Decision
X-ray if: adolescent, severe, suspected fracture
Rule out avulsion or fracture
- 3Acute Phase (0-72h)
RICE protocol, crutches if needed, NSAIDs after 24-48h
Control pain and swelling
- 4Subacute Phase (3-14d)
Gentle ROM, begin core activation, pain-free activity
Restore basic function
- 5Rehabilitation (2-4wk)
Progressive strengthening, sport-specific drills
Prepare for return to sport
- 6Return to Sport
Full ROM, core strength, functional testing, protective padding
Graduated return to contact
A common sideline question is whether to inject local anaesthetic to let a player return to the same game. This is genuinely controversial and must be handled carefully:
- It is only ever considered after a serious injury has been excluded - in particular intra-abdominal injury, an iliac wing or apophyseal avulsion fracture, and significant neurovascular injury. Injecting before excluding these can mask a dangerous injury.
- Local-anaesthetic infiltration of the contused iliac crest can abolish pain enough to return to play and is described in elite sport, but it removes the protective pain signal, risks aggravating the contusion/haematoma, and carries the usual injection risks.
- It should be a shared, informed and documented decision used selectively, not a routine first-line measure, and should generally be avoided in adolescents with an open apophysis.
For most athletes the safer default is to remove from play, apply ice and compression, and rehabilitate - reserving injection for selected adult elite cases in which serious injury has been excluded.
- Remove from play - do not continue with significant injury
- Ice application - 20 minutes every 2-3 hours
- Compression - elastic wrap with padding
- Crutches - for antalgic gait
- NSAIDs - commence after 24-48 hours
- Side-lying on unaffected side
- Pillow support between knees
- Avoid direct pressure on injured crest
- Avoid aggravating movements
- Bed rest not required
- Gentle walking as tolerated
Proper acute management reduces recovery time and complications.
ICEICE UP - Acute Management
Hook:ICE UP the hip pointer for optimal early management
Surgical Technique
Surgical management is rarely required:
Surgery is almost never needed for typical hip pointer injuries. The only surgical indications are:
- Significantly displaced apophyseal avulsion failing conservative care (no validated single displacement threshold - individualised)
- Large symptomatic heterotopic ossification
- Persistent painful bursitis after conservative treatment
- Symptomatic internal oblique aponeurotic avulsion in an elite athlete (rare; transosseous repair reported)
- Non-healing avulsion with displacement
- Elite athlete with time-critical return requirements
- Failed conservative management after 6 months
The vast majority of hip pointers heal completely with conservative management.
Complications
10-15% of significant hip pointers
- Severe initial injury
- Early aggressive mobilization
- Repeated trauma to area
- Large hematoma
- Persistent firm swelling
- Palpable hard mass
- May limit ROM
- Often asymptomatic
- Usually resolves spontaneously over months
- Observe if asymptomatic
- Continue protected activity
- Excision only if symptomatic and mature
Avoid aggressive early mobilization and repeated trauma to prevent calcification. Adequate initial rest followed by gradual progression is key.
Persistent localised pain after a hip pointer is not always heterotopic ossification. The posterior iliac crest is crossed by the superior cluneal nerves (cutaneous branches of the dorsal rami of L1-L3) as they pass over the crest through a tight osteofibrous tunnel, and the anterolateral crest by the lateral cutaneous branch of the iliohypogastric nerve. A direct blow, scarring, or compression from padding or a belt can entrap these nerves, producing chronic burning or shooting pain over the crest and buttock with a positive Tinel sign at a trigger point a few centimetres lateral to the midline.
This is distinct from meralgia paraesthetica (lateral femoral cutaneous nerve, anterolateral thigh - the nerve does not actually cross the iliac crest). Recognise cluneal nerve entrapment as a treatable cause of post-hip-pointer chronic pain, managed with a diagnostic/therapeutic local nerve block and, in refractory cases, surgical nerve release.
Postoperative Care
Note: Postoperative care is rarely required for hip pointer injuries as most are managed conservatively. The following applies to the uncommon cases requiring aspiration or surgical intervention.
Post-aspiration protocol
- Compression dressing over aspiration site
- Ice application 20 min every 2-3 hours
- Rest with elevation
- Monitor for reaccumulation
- Continue compression
- Gentle ROM exercises begin at 48-72 hours
- Ultrasound follow-up if concerns about reaccumulation
- Progress weight bearing as tolerated
- Progressive strengthening
- Core rehabilitation
- Repeat aspiration if significant reaccumulation
Most patients can resume sport-specific training within 2-4 weeks post-aspiration.
NSAID prophylaxis after HO excision (indomethacin 75mg daily for 3-6 weeks) may reduce recurrence risk. Timing of surgery (wait for maturity) is more important than prophylaxis for preventing recurrence.
Outcomes and Prognosis
Prognosis by grade:
- Expected Recovery
- 1-2 weeks
- Return to Sport
- Full return expected
- Long-term Outcome
- Excellent, 99%
- Expected Recovery
- 2-4 weeks
- Return to Sport
- Full return expected
- Long-term Outcome
- Excellent, 95%
- Expected Recovery
- 4-6+ weeks
- Return to Sport
- May have prolonged course
- Long-term Outcome
- Very good, 90%
- Expected Recovery
- 6-12 weeks
- Return to Sport
- Variable
- Long-term Outcome
- Good with appropriate treatment
- Severity of initial injury
- Adequacy of initial treatment
- Compliance with rehabilitation
- Use of protective padding on return
- Vast majority return to pre-injury level (return to sport achieved in nearly all avulsion cases in pooled systematic-review data, Molina et al., 2026)
- Chronic pain uncommon with proper management
- Heterotopic ossification usually asymptomatic
- Second injury possible without proper padding
- In the exceptional operative variant (internal oblique avulsion repair), elite soccer players returned to play at 55-122 days with excellent iHOT-12 scores at 9-11 years (Lohrer & Hoferlin, 2023)
- Shift from RICE toward the PEACE & LOVE soft-tissue framework, with active recovery and caution around early NSAIDs
- Recognition of a posterior hip pointer variant (subperiosteal gluteal detachment at the posterior iliac crest near the PSIS) described in elite athletes (Drigny et al., 2025, PMID 40757555)
- Lack of a validated displacement threshold for operating on adolescent pelvic avulsions remains an open question
Overall prognosis is excellent for hip pointer injuries. Nearly all athletes return to full sport participation. Keys to optimal outcome are appropriate initial rest, graduated rehabilitation, and protective padding on return.
Guidelines, Registries & Global Practice
Global epidemiology and evidence context:
Hip pointer (iliac crest contusion) is a clinical diagnosis with no dedicated registry; the best epidemiological signal comes from sport injury-surveillance systems and pelvic-avulsion cohorts. In the NCAA Injury Surveillance System (16 seasons of collegiate men's football), contusions were among the injuries most disproportionately concentrated in games versus practice, reflecting the contact mechanism that produces hip pointers; the overall game injury rate was roughly 36 per 1000 athlete-exposures versus about 4 per 1000 in practice (Dick et al., 2007, PMID 17710170). For the adolescent apophyseal injuries that constitute the key differential, the population incidence of pelvic avulsion fractures is approximately 21 per million children per year in pooled multi-centre European data, with the iliac crest being one of the rarer sites (Salasek et al., 2025).
Side-by-side guidance (note: no society has a hip-pointer-specific guideline):
- Position relevant to hip pointer
- Contusion managed conservatively; image only for red flags; injection therapy optional to expedite return to play
- Evidence level
- Level V narrative review
- Position relevant to hip pointer
- Hip contusions treated with RICE and graded rehabilitation; protective padding for return to contact
- Evidence level
- Level V consensus / patient guidance
- Position relevant to hip pointer
- Modern PEACE & LOVE framework favours active recovery over prolonged ice/rest; avoid routine NSAIDs in the earliest phase
- Evidence level
- Level V consensus / expert
- Position relevant to hip pointer
- Apophyseal avulsions: conservative for most; site-specific displacement cut-offs (no validated single threshold)
- Evidence level
- Level III systematic review
- Imaging: Ultrasound (haematoma sizing, dynamic muscle assessment) is favoured in sports-medicine settings with ready point-of-care ultrasound access; plain radiographs remain first-line where apophyseal avulsion is suspected; MRI is reserved for diagnostic uncertainty or the rare avulsion variant.
- Acute care philosophy: North American protocols traditionally emphasise RICE; UK/European sports medicine increasingly follows PEACE & LOVE, de-emphasising prolonged ice and early NSAIDs in favour of optimism, load and active recovery.
- Injection therapy: Local-anaesthetic infiltration to expedite elite return to play is described in sports-medicine literature (Hall & Anderson, 2013) but is used selectively.
- Surgery: Operative reattachment for an internal oblique avulsion variant has been reported in elite European soccer (Lohrer & Hoferlin, 2023) but remains exceptional.
- Hip and iliac crest padding integrated into football protective equipment.
- Rule modifications and tackle-technique education in junior competitions.
- Conditioning of trunk/core musculature to tolerate impact loads.
There is no hip-pointer-specific society guideline anywhere in the world - it is managed under general contusion and soft-tissue injury principles. The examinable controversy is the shift from classic RICE to PEACE & LOVE, and the lack of a validated displacement threshold for operating on the adolescent avulsion differential.
MCQ Practice Points
High-yield MCQ topics for hip pointer injuries:
Q: What structure is involved in a hip pointer injury? A: Iliac Crest. It is a subperiosteal hematoma of the iliac crest, NOT the hip joint itself.
Q: A 15-year-old hears a 'pop' at the hip. What must be ruled out? A: Apophyseal Avulsion. The iliac crest apophysis remains open until age 21. X-ray is mandatory.
Q: What is mandatory for return to contact sports? A: Protective Padding. Hard shell padding over the iliac crest reduces recurrence risk significantly.
Q: What is a potential complication of severe hip pointers? A: Heterotopic Ossification. Occurs in 10-15% of cases. Management is usually conservative unless mature and symptomatic.
Q: What is the primary management for Grade I-II injuries? A: Conservative. RICE, NSAIDs, and progressive rehab. Surgery is rarely indicated except for significant displaced avulsions.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old rugby player presents after receiving a knee to the lateral hip during a tackle. He has significant swelling over the iliac crest and an antalgic gait. How would you assess and manage this injury?”
“A 15-year-old football player is brought in after a severe blow to his pelvis during a game. He reports hearing a pop and is unable to bear weight. There is marked swelling over the iliac crest. How does this change your approach?”
“A 28-year-old ice hockey player sustained a hip pointer 6 weeks ago. Despite rest and rehabilitation, he still has persistent pain over the iliac crest and a palpable firm mass. What is your differential diagnosis and management?”
Key Facts
- Iliac crest contusion with subperiosteal hematoma
- NOT a hip joint injury - involves pelvic brim
- Common in football, rugby, ice hockey
- Most recover fully in 2-4 weeks
Severity Grading
- Grade I: Minimal swelling, normal gait - RTS 1-2 weeks
- Grade II: Antalgic gait, moderate swelling - RTS 2-4 weeks
- Grade III: Unable to ambulate - RTS 4-6+ weeks, X-ray
- Adolescent: Check for avulsion
Imaging Indications
- Adolescent with severe injury
- Suspected fracture or avulsion
- Grade III severity
- Not improving after 2-3 weeks
Adolescent Considerations
- Apophysis open until 15-21 years
- Vulnerable to avulsion (iliac crest site is rare; ASIS/AIIS/ischial commoner)
- X-ray mandatory if severe
- No validated displacement threshold - surgery individualised
Management Principles
- RICE protocol acutely
- NSAIDs after 24-48 hours
- Core and hip strengthening rehabilitation
- Protective padding mandatory for RTS
Complications
- Heterotopic ossification in 10-15%
- Usually asymptomatic, resolves over months
- Surgery only for mature, symptomatic lesions
- Prevention: avoid early aggressive mobilization
Evidence Base
Hip Pointers - Defining Narrative Review
- Mechanism is a direct blow to the iliac crest in contact and collision sport
- Conservative management is the standard and is reliably successful
- Local-anaesthetic injection therapy can shorten time lost from play
Pelvic Apophyseal Avulsions - Location and Sport Distribution
- Iliac crest avulsion is rare - only 3 of 203 pelvic avulsions
- Ischial tuberosity, AIIS and ASIS are the common avulsion sites
- Avulsions follow sudden forceful muscle-tendon contraction, not the contact mechanism of a hip pointer
Conservative vs Surgical Avulsion Treatment - Systematic Review
- Both operative and non-operative treatment give favourable outcomes for most avulsions
- No validated displacement cut-off proves surgery superior
- Operative management offered faster return to sport for some ASIS fractures
Pelvic Avulsion Epidemiology and Displacement Cut-offs
- Population incidence approximately 21 per million children per year
- All iliac crest avulsions in the cohort were managed conservatively
- Site-specific displacement cut-offs guide osteosynthesis better than a single 2cm rule
Surgical Repair of Internal Oblique Avulsion at the Iliac Crest
- Internal oblique avulsion is a rare operative variant on the hip pointer spectrum
- Transosseous reattachment gave reliable return to elite sport
- Long-term function (iHOT-12) was excellent at 9-11 years
Muscle Contusion and Myositis Ossificans Prevention
- Avoid corticosteroids in muscle contusion
- Early pain-limited range of motion reduces myositis ossificans risk
- Asymptomatic heterotopic ossification needs no treatment; excise only mature symptomatic lesions