HIV-Associated Arthropathy | Opportunistic Infection | Avascular Necrosis | Perioperative Care
- HIV patients have 10-15 times higher risk of septic arthritis than the general population
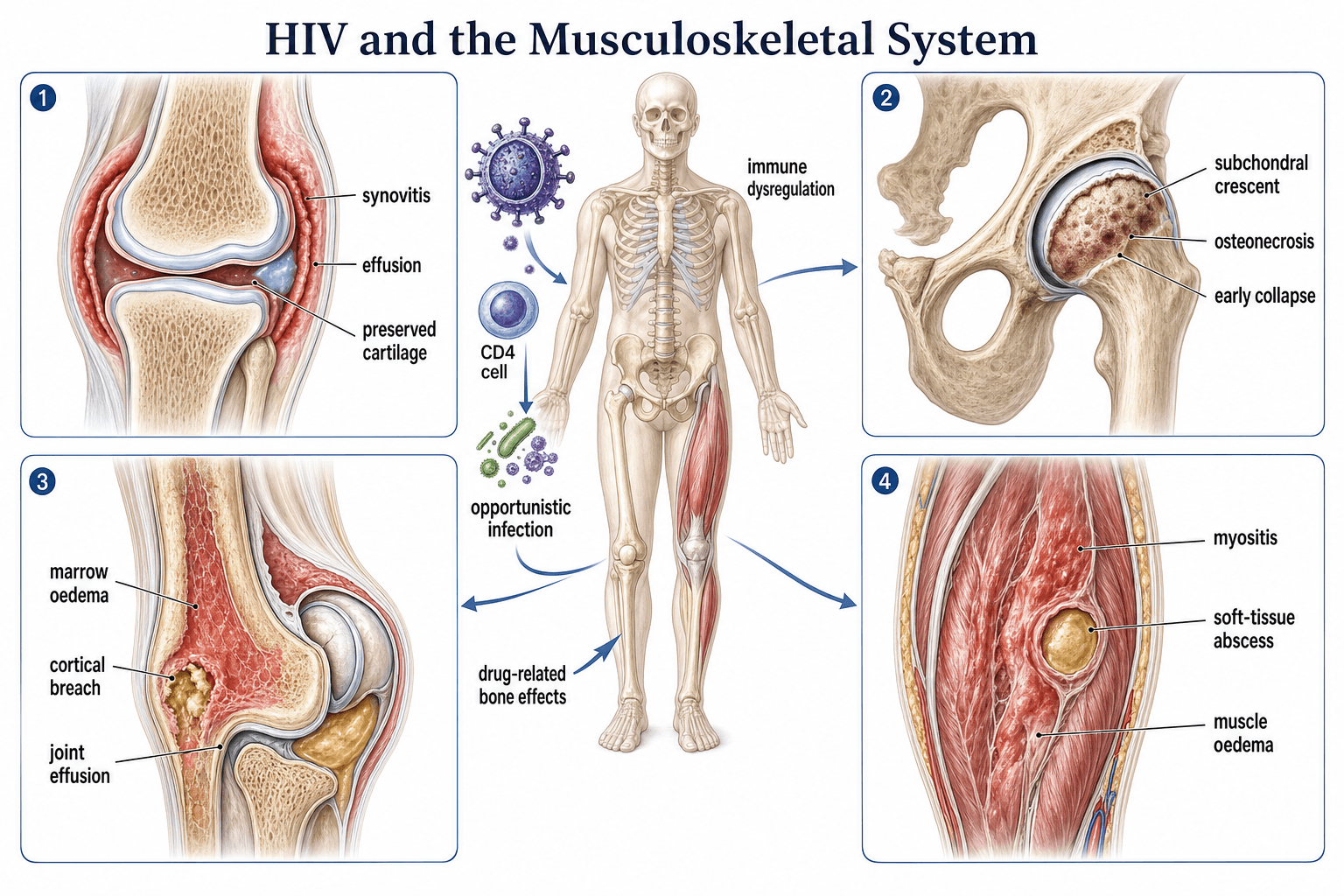
- Avascular necrosis is associated with both HIV infection itself and protease inhibitor-based ART
- CD4 count and viral load guide perioperative risk stratification, not HIV status alone
- Occupational needlestick: start PEP within 1 hour ideally, and never after 72 hours
- ART (especially tenofovir) reduces bone mineral density and increases fragility fracture risk
- Atypical organisms (Salmonella, Mycobacteria, Candida) must be considered when CD4 is low
- “Septic arthritis in HIV is most commonly Staph aureus, but think atypical organisms when CD4 is less than 200
- “Multifocal AVN in a young patient without steroid use should prompt HIV testing
- “ART must NOT be stopped perioperatively: continuity prevents viral resistance and IRIS
- “Fracture healing is generally normal if CD4 count is preserved and nutrition is adequate
HIV massively elevates musculoskeletal infection risk. Septic arthritis is 10-15 times more common than in the general population. Organisms depend on CD4 count: Staph aureus at any level, but consider Salmonella, Mycobacterium tuberculosis, atypical mycobacteria, and Candida when CD4 is less than 200 cells/uL.
AVN in HIV is multifocal in up to 40% of cases. Femoral head is most common, but humeral head, femoral condyles, and tibial plateau can be affected. Both HIV itself and protease inhibitor use are implicated. Presents with insidious groin pain and loss of internal rotation.
CD4 greater than 200 cells/uL = generally safe for elective surgery. CD4 less than 200 = increased wound infection and complication risk; optimise first. CD4 less than 50 = defer elective surgery, high mortality risk. Always check viral load alongside CD4.
Start PEP within 1 hour, never after 72 hours. Three-drug regimen (tenofovir/emtricitabine plus dolutegravir or bictegravir) for 28 days. Report the incident immediately. Baseline HIV, hepatitis B, and hepatitis C serology required. Follow-up testing at 6 weeks, 3 months, and 6 months.
- Likely Diagnosis
- Septic arthritis (atypical organisms likely)
- Key Action
- Urgent aspiration with full panel, broad-spectrum plus anti-atypical antimicrobials
- Exam Pearl
- Always culture for AFB and fungi in HIV patients
- Likely Diagnosis
- Avascular necrosis of femoral heads
- Key Action
- MRI both hips, screen for multifocal disease
- Exam Pearl
- Multifocal AVN is classic for HIV: scan other sites
- Likely Diagnosis
- Occupational exposure requiring PEP
- Key Action
- Wash wound, start PEP within 1 hour, 28-day course
- Exam Pearl
- PEP efficacy drops sharply after 72 hours
- Likely Diagnosis
- Perioperative risk assessment
- Key Action
- Ensure CD4 greater than 200, viral load suppressed, continue ART
- Exam Pearl
- Never stop ART for surgery; outcomes good if optimised
SAAFEHIV Musculoskeletal Manifestations
Hook:SAAFE = keep yourself and your HIV patients safe from musculoskeletal complications!
SMACAtypical Organisms in HIV Septic Arthritis
Hook:SMAC the atypical organisms but never forget Staph aureus is still number one!
RAPIDPEP After Needlestick Injury
Hook:Be RAPID with PEP: every hour counts after a needlestick!
Overview and Epidemiology
Musculoskeletal complications of HIV affect 20-40% of patients and are tested regularly in orthopaedic examinations. With effective antiretroviral therapy, HIV-positive patients are living longer and presenting for elective and trauma orthopaedic surgery in increasing numbers. The orthopaedic surgeon must understand the spectrum of HIV-associated musculoskeletal pathology, the altered infection risk, the perioperative implications of HIV and ART, and occupational exposure management. This knowledge is essential for safe clinical practice and a common exam theme.
- Global HIV prevalence: approximately 39 million people living with HIV worldwide
- Sub-Saharan Africa: highest burden; musculoskeletal disease dominated by infection and trauma
- High-income settings: ageing HIV cohort; degenerative disease and elective surgery increasing
- MSK symptoms: 20-40% of HIV-positive patients develop musculoskeletal complaints
- Septic arthritis: 10-15 times general population risk
- Osteonecrosis: up to 1-4% prevalence in HIV-positive patients (higher than age-matched controls)
- Fracture risk: 30-70% increased incidence of fragility fractures on ART
- Perioperative infection: higher SSI rates if CD4 less than 200 or viraemic at surgery
Pathophysiology
HIV affects the musculoskeletal system through multiple overlapping mechanisms: direct viral effects on immune cells and bone turnover (HIV Tat and gp120 proteins activate the RANKL pathway), opportunistic infection due to immunosuppression, ART toxicity (bone mineral density loss from tenofovir, AVN from protease inhibitors), immune reconstitution inflammatory syndrome (IRIS) causing paradoxical inflammation after ART initiation, and systemic chronic inflammation driving rheumatologic-type arthropathies even on suppressive ART.
- Effect on MSK
- Increased osteoclast activity, reduced osteoblast function
- Associated Conditions
- Osteopenia, osteoporosis, fragility fracture
- Key Mediator
- HIV proteins (Tat, gp120) activate RANKL pathway
- Effect on MSK
- Opportunistic infection susceptibility
- Associated Conditions
- Septic arthritis, osteomyelitis, spinal TB
- Key Mediator
- CD4 less than 200 = major risk threshold
- Effect on MSK
- Bone mineral density loss, lipid abnormalities
- Associated Conditions
- AVN, fragility fractures, tendon rupture
- Key Mediator
- PIs cause dyslipidaemia; tenofovir causes BMD loss
- Effect on MSK
- Paradoxical inflammatory reaction
- Associated Conditions
- Worsening arthritis after ART initiation
- Key Mediator
- Rapid CD4 recovery triggers inflammation
- Effect on MSK
- Rheumatologic-type disease
- Associated Conditions
- HIV-associated arthropathy, reactive arthritis, vasculitis
- Key Mediator
- Persistent immune activation even on suppressive ART
RANKL/RANK/OPG pathway: HIV proteins upregulate RANKL expression, promoting osteoclast differentiation and bone resorption.
Tenofovir (TDF): proximal renal tubular toxicity causes phosphate wasting, further reducing bone mineral density.
Protease inhibitors: alter vitamin D metabolism and lipid profiles, contributing to AVN risk through vascular mechanisms.
Chronic inflammation: persistent cytokine elevation (TNF-alpha, IL-6) drives ongoing bone loss.
Mechanism: rapid immune recovery after ART initiation in a patient with existing opportunistic infection.
MSK manifestation: new or worsening arthritis, tenosynovitis, or osteomyelitis within weeks of starting ART.
Management: continue ART, treat the underlying infection, consider NSAIDs or short-course corticosteroids for inflammation.
Exam point: IRIS occurs while CD4 is rising and viral load is falling. This differentiates it from treatment failure.
Classification and Types
HIV-Associated Arthropathy
- Features
- Migratory arthralgia, no joint destruction, self-limiting
- CD4 Context
- Any CD4 level, often at seroconversion
- Treatment
- NSAIDs, rest; resolves in weeks
- Features
- Asymmetric oligoarthritis, enthesitis, dactylitis
- CD4 Context
- Often early HIV, higher CD4
- Treatment
- NSAIDs, sulphasalazine; ART may help
- Features
- Distal joint involvement, nail changes, psoriasis
- CD4 Context
- Variable CD4
- Treatment
- NSAIDs, methotrexate (caution), biologics if refractory
- Features
- Severe acute joint pain hours to days, no swelling
- CD4 Context
- Advanced HIV (low CD4)
- Treatment
- NSAIDs; self-limiting but distressing
HIV-associated arthropathy is a diagnosis of exclusion after infection has been ruled out. Always aspirate a swollen joint in an HIV patient before attributing pain to inflammatory arthritis.
A swollen, painful joint is not the only soft-tissue infection in HIV - bacterial pyomyositis is a classic, frequently-missed manifestation that this MSK topic must include. Pyomyositis is a primary bacterial infection of skeletal muscle (not contiguous spread from bone or skin); HIV is the dominant risk factor in both tropical ("tropical pyomyositis") and temperate settings. Staphylococcus aureus causes roughly 90 percent of cases. It favours the large muscles of the lower limb and pelvis - quadriceps, gluteals and iliopsoas - and is multifocal in up to a quarter of HIV cases.
- Stage 1 - invasive/diffuse: crampy deep muscle pain with woody induration and low-grade fever; pus has not yet formed and overlying skin looks normal, so it is repeatedly mistaken for a strain, DVT or cellulitis.
- Stage 2 - suppurative (around 2 to 3 weeks): a frank intramuscular abscess with fluctuance and systemic upset. Most patients present here.
- Stage 3 - late/septic: bacteraemia, metastatic abscesses and septic shock.
MRI is the best test (muscle oedema then a rim-enhancing collection); ultrasound guides aspiration; inflammatory markers are raised but creatine kinase is often normal or only mildly elevated (a clue that distinguishes it from a primary myositis). Management: anti-staphylococcal antibiotics (empirical MRSA cover per local prevalence) for the early invasive stage, and drainage (image-guided or open) once an abscess has formed; in advanced HIV send pus for AFB and fungal culture too. A deep muscle with woody induration and normal overlying skin in an HIV patient should trigger immediate suspicion.
Clinical Assessment
- HIV-specific: duration of diagnosis, current ART regimen, CD4 count, viral load
- Risk stratification: CD4 trajectory, opportunistic infection history, AIDS-defining illness
- ART side effects: tenofovir (bone density), protease inhibitors (AVN, dyslipidaemia)
- MSK symptoms: joint pain pattern, swelling, duration, fever, weight loss, night pain
- Exposure history: needlestick injury, occupation, travel to TB-endemic areas
- General: cachexia, Kaposi lesions, oral candidiasis (markers of advanced HIV)
- Musculoskeletal: joint effusion, range of motion, tenderness, erythema, warmth
- Hip AVN: internal rotation loss (earliest sign), FABER positive, groin pain on flexion/internal rotation
- Spinal TB: gibbus deformity, spinous process tenderness, neurological deficit
- Septic joint: painful, hot, swollen, restricted range, fever, systemic signs
When aspirating a joint in an HIV-positive patient, send fluid for:
- Standard: Gram stain, aerobic and anaerobic culture, cell count and differential, crystals
- Extended in HIV: AFB stain and culture (for tuberculosis), fungal culture, viral PCR if indicated
- CD4-guided: if CD4 less than 200, extended mycobacterial and fungal cultures are mandatory
- Blood cultures: always draw simultaneously if septic arthritis is suspected
The threshold for aspiration should be lower in HIV patients than in the general population. Any acutely swollen joint in an HIV patient warrants aspiration to exclude infection before considering inflammatory causes.
- Clinical Clues
- Acute monoarthritis, fever, swollen hot joint
- Investigation
- Joint aspiration (Gram, culture, AFB, fungal)
- Key Discriminator
- Positive culture from aspirate; cannot exclude clinically
- Clinical Clues
- Subacute oligoarthritis, enthesitis, no joint destruction
- Investigation
- Inflammatory markers, negative cultures
- Key Discriminator
- Culture-negative aspirate; inflammatory pattern
- Clinical Clues
- Insidious hip/groin pain, weight-bearing, preserved early ROM
- Investigation
- MRI (gold standard), radiographs (late findings only)
- Key Discriminator
- Serpiginous low-signal line on T1-weighted MRI
- Clinical Clues
- Indolent back pain, constitutional symptoms, endemic area
- Investigation
- MRI spine, AFB culture, biopsy, GeneXpert
- Key Discriminator
- Multilevel disc-space destruction plus paraspinal abscess on MRI
- Clinical Clues
- Worsening arthritis within weeks of ART initiation
- Investigation
- Rising CD4 count, falling viral load
- Key Discriminator
- Temporal correlation with ART start; improving immune parameters
- Clinical Clues
- Symmetric small-joint pain starting after ART change
- Investigation
- Temporal link to drug initiation; exclusion of infection
- Key Discriminator
- Improves on drug switch or withdrawal
In HIV-positive patients, septic arthritis can mimic inflammatory arthropathy clinically. The consequences of missing septic arthritis are joint destruction and systemic sepsis. Always aspirate any swollen joint before starting disease-modifying therapy. Extended cultures (AFB, fungal) should be routine in HIV, especially when CD4 is less than 200 cells/uL.
Investigations
Investigation Protocol
Blood tests: FBC, CRP, ESR, LFTs, renal function, calcium, phosphate, ALP, vitamin D
HIV-specific: CD4 count (current and nadir), HIV viral load, current ART regimen
Serology: rheumatoid factor, anti-CCP (if inflammatory pattern), hepatitis B and C
Purpose: establish immune status, nutritional bone health, inflammatory markers for monitoring
Joint aspirate: mandatory for any swollen joint; Gram, culture, AFB, fungal, crystals, cell count
Plain radiographs: AP and lateral of affected joint; look for AVN (crescent sign, collapse), osteopenia, erosions
Ultrasound: detect effusion, guide aspiration, assess synovitis and tenosynovitis
Limitation: plain radiographs are normal in early AVN and early infection
MRI: gold standard for avascular necrosis (double-line sign on T2), osteomyelitis, spinal TB (disc destruction, paraspinal collection)
CT: assess bone destruction in chronic osteomyelitis; guide surgical planning for spinal TB
Nuclear medicine: bone scan if multifocal AVN suspected; whole-body screening for asymptomatic sites
MRI sensitivity: detects AVN before radiographic changes appear; essential in high-risk patients with hip pain
DEXA scan: baseline bone mineral density recommended for all HIV patients over 40, or any patient on tenofovir
FRAX score: incorporate HIV as a secondary cause of osteoporosis
Biochemistry: 25-OH vitamin D, PTH, calcium, phosphate (screen for tenofovir-induced renal phosphate wasting)
Monitoring: repeat DEXA every 2-3 years in patients on tenofovir or with low baseline BMD
MRI is the gold standard for diagnosing avascular necrosis. The characteristic finding is a serpiginous low-signal line on T1-weighted images surrounding a high-signal area (the double-line sign on T2). Plain radiographs are often normal in early AVN; by the time the crescent sign or subchondral collapse appears, the disease is already Ficat Stage III or higher. If AVN is suspected clinically, request MRI immediately.
Management Algorithm
HIV-Associated Arthropathy
Goal: control symptoms, maintain joint function, optimise ART
Treatment Protocol
NSAIDs: first-line for pain and inflammation (naproxen, ibuprofen)
Analgesia: paracetamol as adjunct
Physical therapy: range of motion exercises, strengthening, activity modification
ART optimisation: ensure viral suppression; some arthropathies improve with ART alone
DMARDs: sulphasalazine or methotrexate (monitor CD4 and LFTs closely)
Caution: methotrexate immunosuppression compounds HIV-related immunosuppression
Corticosteroids: intra-articular injections for monoarthritis; short oral courses for flares
Biologics: TNF-alpha inhibitors in refractory cases (caution with concurrent infection)
IRIS: continue ART, consider short-course corticosteroids, NSAIDs for inflammation
Psoriatic pattern: dermatology co-management; methotrexate or biologics if severe
Drug-induced: switch ART agent if temporal link is clear and no other cause identified
Critical rule: always exclude infection before escalating immunosuppressive therapy
Perioperative Considerations
The orthopaedic surgeon operating on an HIV-positive patient must address three domains: immune status optimisation (CD4 count and viral load), ART continuation (never stop perioperatively), and drug interaction management (ART interactions with anaesthetic agents, antibiotics, and analgesics). Multidisciplinary involvement with HIV medicine, anaesthetics, and pharmacy is essential.
- Risk Level
- Low risk
- Recommendation
- Proceed with elective surgery
- Key Points
- Comparable infection and wound healing to HIV-negative patients
- Risk Level
- Moderate risk
- Recommendation
- Proceed with optimisation; confirm viral load suppressed
- Key Points
- SSI risk modestly elevated; ensure ART adherence
- Risk Level
- Increased risk
- Recommendation
- Optimise CD4 before elective surgery if possible; emergency surgery proceeds
- Key Points
- Significant wound infection risk; may need extended antibiotics
- Risk Level
- High risk
- Recommendation
- Defer elective surgery; treat emergencies with full support
- Key Points
- Very high infection and mortality risk; ICU support likely needed
- Risk Level
- Very high risk
- Recommendation
- Defer all elective surgery; resuscitate and optimise first
- Key Points
- Severe immunosuppression; ensure PCP and MAC prophylaxis
Principle: continue ART throughout the perioperative period without interruption
- Nil by mouth: ART should be taken with a sip of water on the morning of surgery
- Post-operative: resume as soon as the patient can take oral medication
- Interrupted ART: risks viral rebound, drug resistance, and IRIS on restarting
- Protease inhibitors: interact with CYP450; warn the anaesthetist; may alter analgesic metabolism
- Pre-operative: check ART regimen for interactions with planned anaesthetic and analgesic drugs
Nutritional optimisation: albumin, zinc, vitamin C and D; consider dietitian referral
Wound care: meticulous surgical technique; delayed primary closure in contaminated cases
Antibiotic prophylaxis: standard surgical prophylaxis; consider extended cover if CD4 less than 200
Hepatitis co-infection: common (HBV, HCV); check LFTs and coagulation pre-operatively
Smoking cessation: critical; compounds HIV-related and surgical wound healing risks
ART must NOT be stopped perioperatively. Interruption causes viral rebound within days, risks drug resistance development, and can trigger IRIS on restarting. If the patient is nil by mouth, coordinate with the anaesthetist to allow ART with a small sip of water. The only exception is specific drug interactions (e.g., ritonavir-boosted regimens with certain sedatives), which require physician-guided temporary substitution rather than cessation.
Occupational Exposure and PEP
Orthopaedic surgeons have one of the highest occupational exposure rates among surgical specialties due to frequent use of sharp instruments, K-wires, pins, and power tools in a bloody field. All theatre staff must know the PEP protocol. The source patient must be identified and tested immediately. PEP is started based on the exposure risk, not the source patient's known status (a patient may be HIV-positive and undiagnosed).
PEP Protocol After Occupational Exposure
Wash wound: irrigate thoroughly with water or saline; encourage gentle bleeding
Do NOT: squeeze the wound, apply antiseptics, or cauterise
Report: notify occupational health, theatre manager, and senior colleague immediately
Risk assessment: depth of injury, device type (hollow-bore needle = highest risk), visible blood
Source patient: test for HIV, hepatitis B, and hepatitis C with consent
Start PEP: ideally within 1 hour; efficacy drops rapidly, never start after 72 hours
Three-drug regimen: tenofovir/emtricitabine (TDF/FTC or TAF/FTC) plus dolutegravir or bictegravir
Duration: 28 days of continuous treatment
Baseline bloods: HIV test of the exposed person, hepatitis B and C serology, LFTs, renal function
Counselling: discuss side effects (nausea, fatigue, myalgia), adherence importance, follow-up schedule
Week 6: HIV antibody test (4th generation), assess adherence, manage side effects
Week 12: repeat HIV test; hepatitis C RNA if source was HCV-positive
Week 24: final HIV antibody test to confirm negative status
Documentation: complete incident report, occupational health follow-up, psychological support
- Risk Level
- Highest (approximately 0.3%)
- PEP Recommendation
- Full three-drug PEP always
- Notes
- Greatest volume transferred; highest seroconversion risk
- Risk Level
- Moderate (approximately 0.1%)
- PEP Recommendation
- Three-drug PEP recommended
- Notes
- Lower volume but still significant if blood visible on device
- Risk Level
- Low (approximately 0.09%)
- PEP Recommendation
- Three-drug PEP; risk-benefit discussion
- Notes
- Conjunctiva, mouth; rinse immediately with water
- Risk Level
- Negligible
- PEP Recommendation
- PEP not recommended
- Notes
- Wash thoroughly; document; no PEP needed
PEP efficacy is time-dependent. Starting within 1 hour provides the highest protection. Efficacy declines rapidly after 24 hours and PEP should not be started after 72 hours. The orthopaedic theatre is a high-risk environment: K-wires, drill bits, and sharp instruments in bloody fields create frequent exposure opportunities. Know your hospital PEP protocol, where the starter pack is stored, and who to call. Do not wait for occupational health to open: start PEP in the emergency department if the starter pack is available.
Fracture Healing in HIV
- Effect on Healing
- Normal healing expected
- Management
- Standard fracture management
- Evidence
- Comparable union rates to HIV-negative patients
- Effect on Healing
- Delayed union, non-union, higher infection risk
- Management
- Augmented fixation, extended antibiotic prophylaxis
- Evidence
- Higher deep wound infection and delayed union rates
- Effect on Healing
- Reduced BMD, renal phosphate wasting
- Management
- Vitamin D and calcium supplementation; consider TAF switch
- Evidence
- TDF associated with 1-3% BMD loss per year
- Effect on Healing
- Impaired callus formation, delayed union
- Management
- Nutritional optimisation; albumin, zinc, vitamin C
- Evidence
- Common in advanced HIV; improve before elective surgery
- Effect on Healing
- Significantly higher infection risk in HIV
- Management
- Urgent debridement within 6 hours, extended antibiotics
- Evidence
- Infection rates approach 30% with CD4 less than 200
- Closed fractures: standard fixation techniques; comparable union if CD4 greater than 350
- Open fractures: prompt debridement (within 6 hours), extended antibiotics, staged management
- Peri-articular fractures: standard approaches; be aware of AVN risk at already-compromised sites
- Implant choice: no specific implant superiority in HIV; use standard fixation principles
- Weight-bearing: standard protocols for well-controlled HIV; caution in advanced disease
- DEXA: baseline recommended for all HIV patients on ART over age 40
- Vitamin D: check 25-OH vitamin D; supplement to greater than 30 ng/mL
- Calcium: ensure adequate intake (1000-1200 mg/day)
- Tenofovir switch: consider switching from TDF to TAF if BMD loss is significant
- Exercise: weight-bearing exercise to maintain bone density
In well-controlled HIV (CD4 greater than 350, undetectable viral load on ART), fracture healing and union rates are comparable to the general population. Problems arise in advanced, uncontrolled HIV with malnutrition and immunosuppression. For open fractures in HIV-positive patients with low CD4 counts, infection rates approach 30%, so early aggressive debridement, extended antibiotic cover, and careful soft tissue management are essential.
Complications
- Risk
- High - most devastating MSK complication
- Mechanism
- Delayed diagnosis; atypical organisms with indolent course
- Management
- Low threshold for aspiration; extended cultures in all HIV patients
- Risk
- 2-5x higher than general population
- Mechanism
- Immunosuppression, viraemia at surgery
- Management
- Optimise CD4 and viral load before elective arthroplasty
- Risk
- Common if not diagnosed early
- Mechanism
- Progressive osteocyte death from HIV and ART
- Management
- MRI screening for contralateral hip; early core decompression
- Risk
- 30-70% increased incidence on ART
- Mechanism
- Tenofovir BMD loss, chronic inflammation, vitamin D deficiency
- Management
- DEXA screening, vitamin D, calcium; consider TAF switch
- Risk
- 10-25% of patients starting ART
- Mechanism
- Immune recovery causes paradoxical inflammation
- Management
- Continue ART; NSAIDs or short-course corticosteroids
- Risk
- Increased if CD4 less than 200 or malnourished
- Mechanism
- Impaired wound healing, poor nutritional status
- Management
- Nutritional optimisation; CD4 greater than 200 before elective surgery
The most devastating musculoskeletal complication in HIV patients is joint destruction from undiagnosed septic arthritis. Because HIV patients have a higher baseline prevalence of arthralgia and inflammatory arthritis, there is a real risk of attributing a hot swollen joint to HIV-associated arthropathy when it is actually septic. The consequences are rapid chondral destruction, osteomyelitis, and permanent functional loss. Always aspirate before treating empirically as inflammatory arthritis.
The muscle can also fail without infection, and distinguishing the causes is a recognised exam discriminator. Three non-infective muscle problems occur in HIV:
- HIV-associated polymyositis (inflammatory): symmetrical proximal weakness and myalgia with a markedly raised creatine kinase (often more than ten times normal). It can appear at any stage, including at seroconversion; muscle biopsy shows an inflammatory infiltrate. Treat with corticosteroids or IVIG alongside ART optimisation.
- Zidovudine (AZT) toxic mitochondrial myopathy: chronic zidovudine inhibits mitochondrial DNA polymerase gamma, producing "ragged red fibres" on biopsy, proximal weakness, myalgia, a raised creatine kinase and a raised serum lactate. The cardinal discriminator is that it improves after stopping or switching zidovudine - a temporal link to the drug and recovery on withdrawal separates it from HIV polymyositis.
- HIV-associated wasting / sarcopenia: unintentional loss of more than 10 percent of body weight with muscle depletion is an AIDS-defining process and compounds peri-operative and fracture-healing risk.
The statin trap: ritonavir- or cobicistat-boosted protease inhibitors inhibit CYP3A4 and sharply raise the levels of CYP3A4-metabolised statins (simvastatin, lovastatin), precipitating myositis and even rhabdomyolysis. Use pravastatin, rosuvastatin or low-dose atorvastatin instead, and consider a drug interaction whenever an HIV patient on a boosted regimen develops new muscle pain or weakness. Finally, remember that new muscle inflammation soon after starting ART, while the CD4 is rising and viral load falling, may be IRIS rather than a primary myopathy.
Outcomes and Prognosis
- HIV Control
- Well-controlled (suppressed VL)
- Expected Outcome
- Good symptom control with NSAIDs and ART optimisation
- Long-term Prognosis
- Many cases resolve or improve with sustained viral suppression
- HIV Control
- Any CD4 with early treatment
- Expected Outcome
- Joint preservation if drained within 48 hours
- Long-term Prognosis
- Good if early; guarded if diagnosis delayed or atypical organisms
- HIV Control
- Often advanced HIV (CD4 less than 200)
- Expected Outcome
- Prolonged treatment; joint damage common
- Long-term Prognosis
- Guarded; requires multi-drug therapy for 6-12 months
- HIV Control
- CD4 greater than 200, suppressed VL
- Expected Outcome
- Comparable outcomes to non-HIV THA
- Long-term Prognosis
- Good implant survival if infection avoided
- HIV Control
- CD4 less than 200 or viraemic
- Expected Outcome
- Higher infection and complication rates
- Long-term Prognosis
- Guarded; increased revision risk
- HIV Control
- Well-controlled
- Expected Outcome
- Normal healing and union rates
- Long-term Prognosis
- Excellent; standard rehabilitation
Best prognosis: well-controlled HIV (CD4 greater than 350, suppressed viral load), early presentation, prompt treatment of infection, good nutritional status, ART adherence.
Poor prognosis: advanced HIV (CD4 less than 200), viraemia at surgery, delayed diagnosis of septic arthritis, malnutrition, atypical organisms (TB, fungal), open fractures.
Key threshold: CD4 200 cells/uL is the single most important perioperative decision point. Above 200, outcomes approach non-HIV patients; below 200, complication rates rise significantly.
Guidelines, Registries & Global Practice
- Approximately 39 million people living with HIV worldwide (UNAIDS data)
- Sub-Saharan Africa: highest prevalence; orthopaedic burden dominated by infection, trauma, and TB spine
- Asia-Pacific: growing epidemic; orthopaedic services developing
- High-income settings: ageing HIV cohort; degenerative disease and elective surgery increasing
- ART coverage improving globally but uneven; untreated patients present with advanced MSK complications
- High-resource: DEXA screening, CD4-guided perioperative protocols, multidisciplinary HIV-orthopaedic clinics
- Limited-resource: clinical assessment, urgent aspiration for any swollen joint, empiric broad-spectrum therapy
- Universal principle: always aspirate a swollen joint in HIV before diagnosing inflammatory arthritis
- TB endemic regions: high index of suspicion for musculoskeletal tuberculosis alongside septic arthritis
- Perioperative HIV Guidance
- CD4 testing before surgery where available; optimise ART preoperatively
- PEP Guidance
- Three-drug PEP (TDF/FTC plus INSTI); start within 72 hours; 28 days
- Bone Health
- DEXA screening for patients on tenofovir over 40; vitamin D supplementation
- Perioperative HIV Guidance
- Multidisciplinary perioperative planning; ART continuation; CD4 greater than 200 target
- PEP Guidance
- Three-drug PEP; dolutegravir-based preferred; 28 days
- Bone Health
- DEXA at diagnosis and every 2 years on tenofovir; calcium and vitamin D
- Perioperative HIV Guidance
- ART continuation throughout; check CD4 and viral load within 6 months of elective surgery
- PEP Guidance
- Three-drug PEP; raltegravir or dolutegravir preferred with TDF/FTC
- Bone Health
- BMD screening for all HIV patients aged 50 or on tenofovir
- Perioperative HIV Guidance
- Continue all ART including during surgery; no routine extended prophylactic antibiotics
- PEP Guidance
- Same three-drug approach; start immediately; 28 days
- Bone Health
- TAF preferred over TDF when bone health is a concern
There is no specific orthopaedic implant registry for HIV-positive patients. Major arthroplasty registries (NJR, AJRR, AOANJRR) do not routinely collect HIV status, limiting population-level outcome data. Current evidence comes from institutional case series and systematic reviews. As the HIV-positive surgical population expands globally, there is a growing need to capture HIV status in arthroplasty registries.
Document in every HIV-positive surgical patient:
- Current CD4 count and viral load (with dates)
- ART regimen and adherence history
- Hepatitis B and C co-infection status
- Nutritional status assessment (albumin, BMI)
- Occupational exposure documentation if applicable
A missed diagnosis of septic arthritis in an HIV patient, or failure to start PEP after a needlestick, carries significant clinical and medicolegal consequences. Document risk assessment, informed consent regarding elevated complication rates, and multidisciplinary involvement.
Controversies & Areas of Uncertainty
Consensus favours CD4 greater than 200 for elective orthopaedic surgery, but the exact threshold is not defined by high-quality trials. Some evidence suggests CD4 greater than 350 may be preferable for arthroplasty. The decision is individualised based on surgical urgency, procedure type, and viral load.
Protease inhibitors are associated with AVN in observational studies, but causation is debated. Modern integrase inhibitor-based regimens may carry lower AVN risk, but long-term data are lacking. Switching from PI-based ART to reduce AVN risk is reasonable but not evidence-mandated.
Whether HIV patients need extended perioperative antibiotic prophylaxis (beyond the standard 24-hour course) is uncertain. Some centres extend to 48-72 hours for patients with CD4 less than 200, but no prospective data support this practice.
TNF-alpha inhibitors are increasingly used for refractory HIV-associated arthropathy, but long-term safety in immunocompromised patients remains limited. Early reports suggest tolerance when infection is excluded and ART optimised, but registry-level evidence is awaited.
MCQ Practice Points
Q: A 45-year-old HIV-positive man with a CD4 count of 120 cells/uL presents with a swollen, painful ankle. What is the most important investigation? A: Joint aspiration with extended microbiology (Gram stain, culture, AFB stain and culture, fungal culture). In HIV patients with CD4 less than 200, atypical organisms including Salmonella, Mycobacterium tuberculosis, and fungi must be actively sought. Aspiration is mandatory before attributing joint swelling to inflammatory arthritis.
Q: A 30-year-old man with HIV on protease inhibitor-based ART presents with bilateral hip pain. Which investigation has the highest sensitivity? A: MRI of both hips. MRI detects avascular necrosis before radiographic changes appear and identifies the characteristic serpiginous low-signal line on T1-weighted images. MRI also allows screening of the contralateral hip and other sites for multifocal disease.
Q: Should antiretroviral therapy be stopped before elective orthopaedic surgery? A: No. ART must NOT be stopped perioperatively. Interruption causes viral rebound within days, risks drug resistance, and can trigger IRIS on restarting. ART should be continued throughout, coordinating with the anaesthetist to allow administration with a sip of water if nil by mouth.
Q: A theatre nurse sustains a deep needlestick from an HIV-positive patient. What is the maximum window to start post-exposure prophylaxis? A: 72 hours, but ideally within 1 hour. PEP efficacy declines rapidly with time. The standard regimen is three drugs (tenofovir/emtricitabine plus dolutegravir or bictegravir) for 28 days. Baseline HIV, hepatitis B, and hepatitis C serology are required with follow-up at 6 weeks, 3 months, and 6 months.
Q: How does HIV affect fracture healing in a patient with a CD4 count of 500 cells/uL on ART? A: Fracture healing is comparable to the general population in well-controlled HIV (CD4 greater than 350, suppressed viral load on ART). Standard fracture management applies. Problems arise in advanced HIV (CD4 less than 200), with malnutrition or open fractures, where delayed union, non-union, and infection rates are significantly higher.
Q: Which antiretroviral agent is most associated with reduced bone mineral density? A: Tenofovir disoproxil fumarate (TDF). TDF causes proximal renal tubular dysfunction leading to phosphate wasting and reduced bone mineral density. Tenofovir alafenamide (TAF) has significantly less bone impact and should be considered as a switch when BMD loss is identified.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old man known to be HIV-positive presents with a 3-day history of a painful, swollen right knee. He is on antiretroviral therapy but his last CD4 count was 180 cells/uL and his viral load is detectable. Examination reveals a hot, tender, effused right knee with painful restricted range of movement. His temperature is 38.2 degrees Celsius. How would you manage this?”
“A 32-year-old man diagnosed with HIV two years ago presents with 6 months of insidious bilateral groin pain. He is on a protease inhibitor-based antiretroviral regimen. His CD4 count is 420 cells/uL and his viral load is undetectable. He drinks 10 units of alcohol per week and has never used corticosteroids. Examination reveals pain on internal rotation of both hips with restricted internal rotation bilaterally. How would you investigate and manage him?”
HIV-Associated MSK Manifestations
- SAAFE mnemonic: Septic arthritis, Avascular necrosis, Arthropathy, Fracture risk, Exposure/perioperative care
- 20-40% of HIV patients develop musculoskeletal symptoms
- Septic arthritis 10-15x more common than in the general population
- AVN is multifocal in up to 40% of HIV cases; femoral head most common site
- ART (especially tenofovir) increases fragility fracture risk 30-70%
Septic Arthritis in HIV
- Always aspirate any swollen joint in HIV before diagnosing inflammatory arthritis
- Send aspirate for Gram, culture, AFB stain and culture, fungal culture, crystals, cell count
- CD4 greater than 200: Staph aureus most likely; CD4 less than 200: add atypical organisms (SMAC)
- SMAC mnemonic: Salmonella, Mycobacteria, Aspergillus/fungi, Common organisms still predominant
- Treatment: surgical drainage plus targeted antimicrobials for 4-6 weeks (6-12 months for TB)
Avascular Necrosis
- Risk factors: HIV itself plus protease inhibitor ART plus corticosteroids plus alcohol
- MRI is gold standard; plain radiographs miss early disease entirely
- Ficat I-II: core decompression; Ficat III-IV: total hip arthroplasty
- Screen for multifocal disease (humeral head, femoral condyles, tibial plateau)
- THA outcomes comparable to non-HIV if CD4 greater than 200 and viral load suppressed
Perioperative Considerations
- ART must NOT be stopped perioperatively (viral resistance and IRIS risk)
- CD4 greater than 200: proceed with elective surgery; CD4 less than 200: optimise first
- Check hepatitis B/C co-infection, nutritional status, drug interactions pre-operatively
- Protease inhibitors interact with CYP450: warn the anaesthetist
- SSI risk higher if viraemic at surgery: ensure viral suppression before elective cases
Occupational Exposure / PEP
- RAPID mnemonic: Report, Assess risk, PEP within 1 hour, Investigate baseline, Duration 28 days
- Three-drug PEP: tenofovir/emtricitabine plus dolutegravir or bictegravir
- Never start PEP after 72 hours; efficacy drops sharply with time
- Follow-up HIV testing at 6 weeks, 3 months, and 6 months
- Orthopaedics: high-risk specialty for needlestick; know your hospital PEP protocol
Fracture Healing in HIV
- CD4 greater than 350 plus suppressed viral load: normal healing expected
- CD4 less than 200: delayed union, non-union, higher infection risk
- Open fractures in HIV: infection rates approach 30% if CD4 less than 200
- Tenofovir causes BMD loss via renal phosphate wasting; consider TAF switch
- DEXA screening recommended for all HIV patients on ART over age 40
Evidence Base and Key Trials
High prevalence of osteonecrosis of the femoral head in HIV-infected adults
- High prevalence of osteonecrosis of the femoral head in HIV-infected adults compared to general population
- Femoral head most commonly affected; multifocal disease in substantial proportion
- Patients younger than typical non-HIV AVN and with fewer traditional risk factors
- Both HIV infection itself and protease inhibitor ART implicated
Bone disease in HIV infection: a practical review and recommendations for HIV care providers
- Bone mineral density loss common in HIV-positive patients on ART
- Tenofovir associated with greater BMD reduction than other agents
- Fracture risk increased 30-70% in HIV patients compared to general population
- Screening with DEXA recommended for patients over 40 or on tenofovir
Late fracture-related infections in HIV-positive patients: a prospective cohort study
- Prospective cohort demonstrating elevated late infection risk after fracture fixation in HIV-positive patients
- CD4 count and viral load at time of injury strongly predict infection risk
- Open fractures and low CD4 associated with infection rates approaching 30%
- Early ART optimisation and extended antibiotics improve outcomes in advanced HIV
Outcomes of total hip and knee arthroplasty in special populations: a synopsis and critical appraisal of systematic reviews
- Systematic review synopsis showing HIV-positive patients have higher infection rates after THA/TKA than HIV-negative
- Infection risk significantly reduced when CD4 greater than 200 and viral load suppressed
- Modern ART regimens have improved arthroplasty outcomes compared to pre-ART era
- Perioperative optimisation of HIV parameters is the key modifiable factor