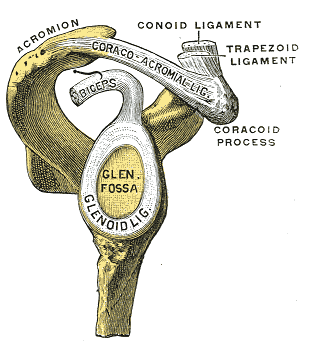
Glenohumeral Stability | Rotator Cuff Force Couples | Scapulothoracic Rhythm
- Scapulothoracic rhythm: 2:1 ratio (for every 2° GH abduction, 1° ST upward rotation)
- Rotator cuff force couple: Subscapularis/infraspinatus-teres minor balance humeral head centering
- Deltoid-rotator cuff force couple: Deltoid elevates, RC depresses and centers humeral head
- Glenoid covers only 25% of humeral head (inherent instability requires dynamic stabilizers)
- Concavity-compression: RC compresses head into glenoid concavity for stability
- “Critical arc of abduction 60-120°: supraspinatus most active, impingement risk highest
- “Capsular volume 2x humeral head volume allows large ROM but sacrifices stability
- “Labrum deepens glenoid socket 50% (increases stability)
- “Inferior glenohumeral ligament (IGHL) is primary anterior stabilizer in abduction-external rotation
2:1 ratio throughout abduction arc. 180° total arm elevation = 120° GH + 60° ST. Disruption causes scapular dyskinesis and impingement.
Coronal plane: Deltoid (superior) vs subscapularis/infraspinatus (inferior). Transverse plane: Subscapularis (anterior) vs infraspinatus-teres minor (posterior). Centers humeral head.
RC compresses humeral head into glenoid concavity. Creates suction seal and depth. Accounts for 50% of GH stability. Loss with RC tear causes superior migration.
Deepens glenoid 50% (9mm to 5mm depth). Increases contact area and stability. SLAP tears compromise biceps anchor and superior stability.

CLASPSGlenohumeral Stability Mechanisms
Hook:CLASPS hold the shoulder stable: 50% dynamic (RC), 50% static (capsule/labrum)!
Overview and Introduction
Shoulder biomechanics encompasses the complex interplay of multiple joints, muscles, and ligaments that produce the greatest range of motion of any joint in the body. Understanding these principles is critical for managing instability, rotator cuff pathology, arthroplasty, and rehabilitation.
The shoulder complex includes the glenohumeral (GH), scapulothoracic (ST), acromioclavicular (AC), and sternoclavicular (SC) joints working in concert to achieve 180 degrees of abduction.
Concepts and Principles
Key Biomechanical Principles:
- Scapulothoracic Rhythm (2:1): For every 2° of GH abduction, there is 1° of ST upward rotation
- Force Couples: Coronal (deltoid vs inferior cuff) and transverse (subscapularis vs infraspinatus-teres minor)
- Concavity-Compression: RC compresses humeral head into glenoid for dynamic stability
- Labral Contribution: Deepens glenoid by 50%, critical for stability
Glenohumeral Joint Geometry and Stability
Inherent Instability vs Mobility Trade-Off
The glenohumeral joint is the most mobile but least stable joint in the body. This is due to minimal bony constraint.
- Glenoid coverage: Only 25% of humeral head surface area
- Radius mismatch: Humeral head radius greater than glenoid concavity
- Retroversion: Glenoid retroversion averages 5° (posterior tilt)
- Result: Minimal intrinsic bony stability
- Capsule volume: 2x humeral head volume
- Function: Allows large ROM (180° abduction, 90° ER/IR)
- Trade-off: Loose capsule = less static restraint
- Folds: Capsular redundancy allows motion without tension
The labrum is critical for increasing stability by deepening the glenoid socket approximately 50% (from 2.5mm to 5mm depth). This increases contact area and creates a suction seal.
Static vs Dynamic Stabilizers
Shoulder stability is 50% static, 50% dynamic.
- Structures
- Capsule, ligaments (IGHL, MGHL, SGHL), labrum, glenoid concavity
- Contribution
- Passive restraint at end ROM
- Failure Mechanism
- Capsular laxity, labral tear, Bankart lesion
- Structures
- Rotator cuff (SITS), deltoid, scapular stabilizers (serratus, trapezius)
- Contribution
- Active concavity-compression, force couples
- Failure Mechanism
- RC tear, scapular dyskinesis, nerve injury
Concavity-compression is the primary dynamic stabilizing mechanism. The rotator cuff compresses the humeral head into the glenoid concavity, creating stability through increased friction and depth. This accounts for approximately 50% of GH stability.
Scapulothoracic Rhythm
The 2:1 Ratio
Normal shoulder elevation requires coordinated motion between the glenohumeral (GH) and scapulothoracic (ST) articulations. The classic ratio is 2:1.
- 0-30° abduction: Primarily GH motion (setting phase)
- 30-180° abduction: 2:1 ratio (2° GH for every 1° ST)
- Total 180°: 120° GH + 60° ST upward rotation
- Result: Scapula rotates upward, glenoid tracks under humeral head
- Upward rotation: 60° total (inferior angle moves laterally)
- Posterior tilt: 20-30° (acromion tilts posteriorly)
- External rotation: 15-25° (medial border moves away from spine)
- Muscles: Serratus anterior (upward rotation), trapezius (elevation)
Loss of normal ST rhythm causes impingement and instability. Serratus anterior palsy (long thoracic nerve injury) causes medial scapular winging and loss of upward rotation. This reduces subacromial space and increases impingement risk. Rehabilitation must restore scapular stability before addressing GH pathology.
Acromioclavicular Joint Contribution
The AC joint allows scapular protraction/retraction and rotation. Clavicular rotation at the sternoclavicular joint contributes 40-50° to overhead motion.
Disruption of AC joint (separation) or SC joint affects scapular position and can cause secondary impingement.
Planes of Elevation and the Scapular Plane (Scaption)
The plane in which the arm is elevated changes the demand on the capsule, the cuff and bony clearance, and is a favourite basic-science point.
The scapular plane ("scaption") lies roughly 30 to 45 degrees anterior to the coronal plane, matching the resting orientation of the scapula on the curved thorax. Elevation in this plane is the most efficient and least provocative because:
- The inferior capsule is not twisted, so the capsuloligamentous structures stay relatively relaxed and range of motion is maximal.
- Supraspinatus and deltoid are optimally aligned with the plane of the scapula, improving their mechanical advantage.
- The greater tuberosity clears the acromion without the obligatory external rotation that pure coronal abduction requires, so impingement is least.
By contrast, true coronal-plane abduction requires external rotation of the humerus to move the greater tuberosity out from under the acromion — without it the tuberosity impinges through the mid-arc. Forward flexion (sagittal plane) progressively tightens the posterior capsule. This is why rehabilitation and isolated strength testing are usually performed in the scapular plane, and why the "empty can" (Jobe) test positions the arm in scaption to load the supraspinatus.
Elevating in the plane of the scapula (~30 to 45° anterior to coronal) keeps the capsule untwisted, aligns supraspinatus and deltoid, and lets the greater tuberosity clear the acromion without needing external rotation — maximal motion for least impingement. Pure coronal abduction needs ER to avoid greater-tuberosity impingement.
Rotator Cuff Force Couples
The rotator cuff functions as two force couples to center the humeral head during motion.
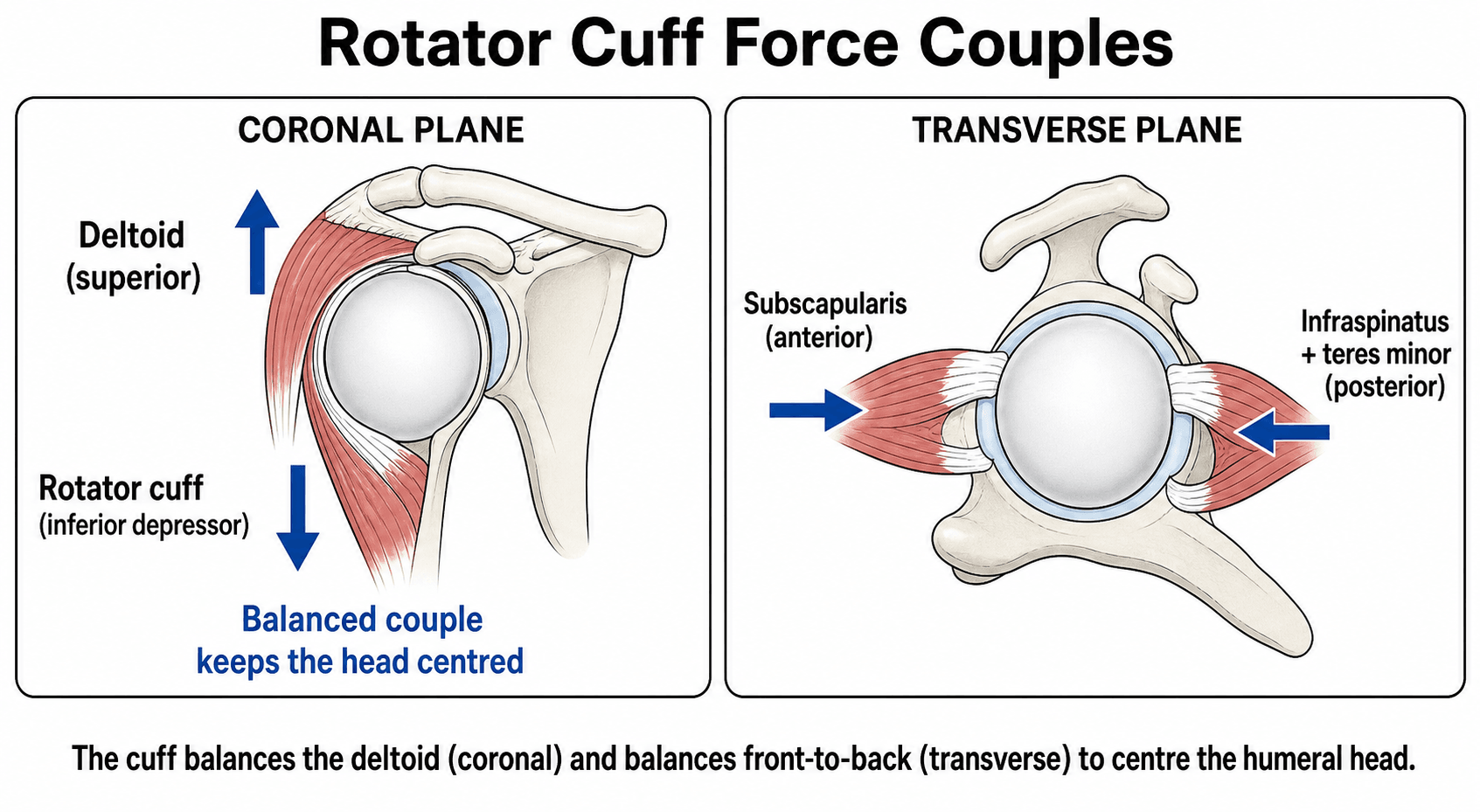
Coronal Plane Force Couple
Deltoid (superior) vs Subscapularis + Infraspinatus-Teres Minor (inferior)
- Primary abductor: Generates upward force
- Vector: Superior translation of humeral head
- Problem: Alone would cause superior migration and impingement
- Balanced by: Inferior force from rotator cuff
- Depressor force: Subscapularis + infraspinatus-teres minor pull inferiorly
- Vector: Counteracts deltoid superior pull
- Result: Humeral head stays centered in glenoid
- Clinical: RC tear allows superior migration (loss of depressor)
Supraspinatus role is debated:
- Traditional view: Primary abduction initiator
- Modern view: Primarily a humeral head depressor and compressor
- Clinical: Supraspinatus tear does not abolish abduction (deltoid compensates)
Transverse Plane Force Couple
Subscapularis (anterior) vs Infraspinatus-Teres Minor (posterior)
- Action
- Internal rotation, anterior compression
- Force Vector
- Prevents posterior subluxation
- Tear Effect
- Anterior instability, loss of IR strength
- Action
- External rotation, posterior compression
- Force Vector
- Prevents anterior subluxation
- Tear Effect
- Posterior superior migration, loss of ER
Balance is critical: Subscapularis tear leads to anterosuperior escape of humeral head. Infraspinatus-teres minor tears lead to posterosuperior instability.
SITSRotator Cuff Force Couples
Hook:SITS muscles work as force couples: Supraspinatus-deltoid (coronal), Subscapularis vs Infraspinatus-Teres (transverse)!
Glenohumeral Joint Reaction Force and Force Vectors
Beyond keeping the head centred, the muscles around the shoulder generate a substantial joint reaction force (JRF) that must be directed into the glenoid for stability. In the classic biomechanical analysis (Poppen and Walker), the resultant glenohumeral joint reaction force rises through abduction to peak at about 0.9 times body weight near 90 degrees of elevation, then falls as the arm rises further — so the mid-range is both the most heavily loaded and the most demanding of the stabilisers.
The direction of that resultant matters as much as its magnitude. For stability the resultant force vector must fall within the glenoid arc; the force-couple balance keeps it there (the "scapulohumeral balance" of Lippitt and Matsen). If it falls outside the glenoid rim — as with cuff deficiency or glenoid bone loss — the head subluxes, which is the mechanical basis of the glenoid concavity-arc and "on-track / off-track" concepts.
The deltoid line of pull illustrates this. Early in abduction the deltoid acts almost vertically, producing a large superior shear on the humeral head; the rotator cuff converts this into a compressive, centring force by adding an inferiorly and medially directed vector. As the arm elevates, the deltoid's line of action becomes progressively more compressive and less shearing — which is why superior migration in a cuff-deficient shoulder is worst in the mid-range, and why reverse arthroplasty (by medialising and distalising the centre of rotation) restores a favourable deltoid line of action and lowers the joint reaction force.
The glenohumeral joint reaction force peaks at roughly 0.9 times body weight near 90° of elevation (Poppen–Walker). Stability requires the resultant vector to stay within the glenoid arc; the cuff converts the deltoid's superior shear into glenoid compression, and loss of that balance (cuff tear, glenoid bone loss) lets the head escape.
Capsular Ligaments and Stability
Inferior Glenohumeral Ligament Complex (IGHLC)
The IGHLC is the primary anterior stabilizer in the abducted, externally rotated position (late cocking phase of throwing).
- Anterior band: Resists anterior translation in ABD-ER
- Posterior band: Resists posterior translation in ABD-IR
- Axillary pouch: Inferior capsule, resists inferior subluxation
- Insertion: Labrum (Bankart lesion disrupts IGHL anchor)
- 90° ABD-ER: Anterior band maximally loaded
- 90° ABD-IR: Posterior band maximally loaded
- Adduction: Redundant, minimal restraint
- Clinical: Bankart repair restores IGHL to labrum
Middle and Superior Glenohumeral Ligaments
MGHL is primary restraint to anterior translation at 45-90° abduction. SGHL and coracohumeral ligament restrain inferior subluxation in adduction.
Clinical Applications
Rotator Cuff Tear Biomechanical Consequences
- Loss of compression: Reduced concavity-compression stability
- Superior migration: Deltoid unopposed, head migrates superiorly
- Impingement: Acromiohumeral interval narrows (normal 7-10mm)
- Compensation: Deltoid and remaining cuff can maintain elevation
- Anterior instability: Loss of anterior force couple
- Anterosuperior escape: Head subluxes anterosuperiorly
- Loss of IR strength: Cannot internally rotate against resistance
- Clinical: Lift-off test positive, belly-press weak
Massive RC tear (greater than 2 tendons or greater than 5cm) causes:
- Loss of both force couples (coronal and transverse)
- Anterosuperior or posterosuperior escape
- Rotator cuff arthropathy (acetabularization of acromion)
Shoulder Arthroplasty Design
Understanding biomechanics guides arthroplasty:
- Design Goal
- Restore native concavity and version
- Biomechanical Basis
- Concavity-compression requires proper depth and orientation
- Design Goal
- Match native radius and offset
- Biomechanical Basis
- Maintains normal center of rotation and deltoid moment arm
- Design Goal
- Medialize center of rotation, distalize humerus
- Biomechanical Basis
- Deltoid becomes primary elevator when RC absent (biomechanical compensation)
Reverse shoulder arthroplasty (RSA) reverses normal biomechanics:
- Glenosphere becomes ball (medializes center of rotation)
- Humeral socket becomes cup (distalizes humerus)
- Deltoid becomes primary elevator (RC not needed)
- Increases deltoid moment arm and reduces joint reactive force
Differentiating Biomechanical Failure Patterns
A common exam task is to translate a clinical or imaging finding into the underlying biomechanical lesion. Use the destabilising direction and the failed force couple to reason to the diagnosis.
- Key Mechanism Lost
- Concavity-compression and coronal depressor force
- Direction of Instability/Escape
- Superior migration of the humeral head
- Hallmark Clinical Clue
- Reduced acromiohumeral interval, painful arc, weak elevation
- Key Mechanism Lost
- Anterior limb of transverse force couple
- Direction of Instability/Escape
- Anterosuperior escape
- Hallmark Clinical Clue
- Positive lift-off / belly-press, lost internal-rotation strength
- Key Mechanism Lost
- Anterior static restraint in abduction-external rotation
- Direction of Instability/Escape
- Anterior translation in the apprehension position
- Hallmark Clinical Clue
- Recurrent anterior dislocation, positive apprehension-relocation
- Key Mechanism Lost
- Stable scapular platform and upward rotation
- Direction of Instability/Escape
- Functional impingement, loss of overhead arc
- Hallmark Clinical Clue
- Medial scapular winging, abnormal scapulohumeral rhythm
- Key Mechanism Lost
- Both force couples plus articular cartilage
- Direction of Instability/Escape
- Fixed superior escape with acromial acetabularisation
- Hallmark Clinical Clue
- Pseudoparalysis, superior glenoid/acromial wear, candidate for RSA
Guidelines, Registries and Global Practice
Shoulder biomechanics is a basic-science topic, so formal disease guidelines are limited; the relevant guidance sits within instability, rotator cuff and arthroplasty pathways, and within national joint registries that track the implants these biomechanical principles inform.
Global epidemiology (context)
- Rotator cuff disease prevalence rises steeply with age and is frequently asymptomatic; full-thickness tears become common beyond the sixth decade across populations studied worldwide.
- Anterior glenohumeral instability disproportionately affects young males in contact and overhead sport, the group in whom IGHL/labral biomechanics are most exam-relevant.
- Shoulder arthroplasty volumes, especially reverse arthroplasty for cuff-deficient shoulders, have grown markedly across high-income registries over the past two decades.
Side-by-side society guidance
- Focus
- Rotator cuff and glenohumeral OA management
- Biomechanically Relevant Position
- Evidence-based pathways; recognises irreparable cuff tears with superior escape as a reverse-arthroplasty indication
- Focus
- Instability and cuff care pathways
- Biomechanically Relevant Position
- Structured instability assessment incorporating bone loss and direction-specific restraints before stabilisation
- Focus
- Trauma and reconstruction principles
- Biomechanically Relevant Position
- Restoration of joint line, version and the rotator-cuff force couple as goals of fixation and reconstruction
- Focus
- Arthroplasty and instability consensus
- Biomechanically Relevant Position
- Emphasis on glenoid version/inclination and centre-of-rotation restoration to protect implant survival
Registry evidence
National arthroplasty registries (NJR for England and Wales, AOANJRR in Australia, the Swedish and Norwegian registries, AJRR in the US, NZJR) track shoulder arthroplasty survival and revision. Recurring biomechanically driven signals include glenoid component loosening in anatomic replacement and scapular notching and instability after reverse arthroplasty, which inform component selection, version and centre-of-rotation choices.
High- versus limited-resource practice variation
- In well-resourced settings, advanced imaging, 3D planning and patient-specific instrumentation are increasingly used to restore version, inclination and the centre of rotation when biomechanics are disturbed.
- In limited-resource settings, structured physiotherapy targeting scapular control and the rotator-cuff force couple is the mainstay, with arthroplasty reserved and standard instrumentation used; the underlying biomechanical goals, a stable scapular platform and a centred, compressed humeral head, are identical regardless of resources.
Controversies and Areas of Uncertainty
- The 2:1 rhythm is an approximation. The frequently quoted 2:1 glenohumeral-to-scapulothoracic ratio is reproducible only at low movement speed and through a defined arc. It varies with velocity, plane of elevation, load and individual anatomy, so a rigid single ratio overstates the certainty of the data.
- Supraspinatus as initiator versus depressor. Whether supraspinatus is principally an abduction initiator or principally a head compressor-depressor remains debated; the modern view emphasises its compressive, head-centring role, since isolated supraspinatus loss does not abolish abduction when the deltoid is intact.
- Exact stability percentages are heuristic. The "50% static, 50% dynamic" and "concavity-compression provides 50% of stability" figures are useful teaching constructs derived from specific in vitro models, not precise physiological constants; their value is conceptual rather than literal.
- Critical glenoid bone-loss threshold. The amount of glenoid bone loss that mandates a bony procedure rather than soft-tissue repair (historically quoted around 20-25%, with growing attention to "on-track / off-track" and subcritical loss) continues to evolve and is genuinely unsettled.
- Optimal RSA configuration. Lateralisation versus medialisation of the centre of rotation, and glenosphere size and tilt, trade off impingement, stability, deltoid efficiency and notching; there is no single agreed optimum and design philosophy continues to change.
MCQ Practice Points
Q: What is the normal scapulothoracic rhythm ratio during shoulder abduction from 30-180 degrees? A: 2:1 (glenohumeral:scapulothoracic) - For every 2 degrees of GH abduction, there is 1 degree of ST upward rotation. Total 180° = 120° GH + 60° ST.
Q: What percentage of glenohumeral stability is provided by concavity-compression from the rotator cuff? A: 50% - Concavity-compression (RC compressing head into glenoid) provides 50% of stability. The other 50% comes from static restraints (capsule, ligaments, labrum).
Q: By what percentage does the labrum deepen the glenoid socket? A: 50% - The labrum increases glenoid depth from approximately 2.5mm to 5mm, a 50% increase. This enhances stability by increasing contact area and creating a suction seal.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Examiner asks: Describe the scapulothoracic rhythm during shoulder abduction. What happens when this rhythm is disrupted?”
“Examiner shows MRI of massive rotator cuff tear and asks: Explain the biomechanical consequences of this tear and why the patient has superior migration of the humeral head.”
“Examiner asks: A 22-year-old rugby player has recurrent anterior shoulder dislocations. Explain the biomechanical contributions to glenohumeral stability and which structure is the primary restraint in the position of apprehension.”
Stability Mechanisms
- 50% dynamic (RC concavity-compression) + 50% static (capsule/labrum)
- Glenoid covers only 25% of humeral head (inherent instability)
- Labrum deepens socket 50% (2.5mm to 5mm)
- Capsular volume = 2x head volume (allows ROM, sacrifices stability)
Scapulothoracic Rhythm
- 2:1 ratio (GH:ST) from 30-180° abduction
- 0-30° = setting phase (primarily GH)
- Total 180° = 120° GH + 60° ST upward rotation
- Scapular muscles: serratus anterior (upward rotation), trapezius (elevation)
Rotator Cuff Force Couples
- Coronal: Deltoid (superior) vs RC (inferior depressor)
- Transverse: Subscapularis (anterior) vs infraspinatus-teres (posterior)
- SITS muscles: Supraspinatus, Infraspinatus, Teres minor, Subscapularis
- RC tear causes superior migration (deltoid unopposed)
Capsular Ligaments
- IGHL = primary anterior stabilizer in ABD-ER (90°+)
- MGHL = primary restraint at 45-90° abduction
- SGHL + coracohumeral = inferior restraint in adduction
- Bankart lesion = IGHL detachment from labrum
Clinical Applications
- Acromiohumeral interval normal = 7-10mm (reduces with RC tear)
- Reverse shoulder: medializes center, distalizes humerus, deltoid primary elevator
- Scapular dyskinesis causes impingement (loss of upward rotation)
- Massive RC tear (greater than 2 tendons or greater than 5cm) may need RSA
Key Numbers
- Glenoid retroversion: 5° average
- Clavicular rotation (SC joint): 40-50°
- AC joint rotation: 20°
- Supraspinatus critical arc: 60-120° abduction (highest stress)
Evidence Base
The biomechanical understanding of the shoulder rests on a small group of landmark cadaveric, radiographic and modelling studies. Each card below has been verified against its PubMed record. Named-society guidance (AAOS, BOA, AO) is summarised in the global practice section.
Concavity-Compression: Mechanisms of Glenohumeral Stability
- Defined two key dynamic mechanisms: concavity-compression and scapulohumeral balance
- Compressing the humeral head into the concave glenoid resists translating loads
- Stability rises with greater compressive (muscle) load and with deeper glenoid concavity
- An intact labrum is essential to both mechanisms, especially in the lax mid-range
The Glenoid-Labral Socket: A Constrained Articular Surface
- Glenoid plus labrum form a socket about 9mm deep superoinferiorly and 5mm anteroposteriorly (n=25)
- The fibrous labrum contributes roughly 50% of total socket depth
- Simulated Bankart lesion reduced anteroposterior depth from about 5.0mm to 2.4mm
- Socket depth is a meaningful structural contributor to glenohumeral stability
Sequential Cutting: Stabilisers Preventing Anterior Dislocation (IGHL)
- Cadaveric sequential-cutting study of 36 embalmed and 10 fresh shoulders
- At 0° abduction subscapularis is the main anterior restraint
- At 45° subscapularis, MGHL and anterosuperior IGHL share the restraint
- At 90° abduction the inferior glenohumeral ligament is the primary check to anterior dislocation in external rotation
Scapulohumeral Rhythm: Motion Velocity and Ratio
- 19 shoulders of 10 healthy men analysed with image intensifier and high-resolution video
- At low speed the glenohumeral-to-scapulothoracic ratio was constant, agreeing with prior work
- At high speed the ratio was not fixed and differed significantly from low speed
- Glenohumeral motion dominated early abduction beyond the setting phase, then declined
3D Scapular Orientation in Rotator Cuff Tear and Impingement
- Low-dose stereoradiographic 3D scapular orientation in 65 subjects
- Resting scapular orientation did not differ between healthy, cuff-tear and cuff-tear-plus-impingement groups
- At 90° elevation, scapular upward rotation was significantly reduced only in the impingement group
- Scapular kinematic alteration in symptomatic shoulders is multifactorial, not a uniform finding
Muscle Moment Arms After Anatomic vs Reverse Shoulder Arthroplasty
- Eight cadaveric upper limbs tested pre-operatively, after anatomic TSA and after revision RSA
- Anatomic TSA lateralised the joint centre about 4.3mm, modestly increasing deltoid force and joint compression
- RSA significantly increased moment arms of abductors, flexors, adductors and extensors and reduced peak muscle forces
- RSA increased superior deltoid inclination but produced greater superior shear and less joint compression