Zone 2 | Metadiaphyseal Junction | Watershed Zone | High Nonunion Risk | Athletes Need Surgery
TORG CLASSIFICATION (RADIOGRAPHIC STAGING)
Critical Must-Knows
- Zone 2 location: metadiaphyseal junction extending INTO 4-5 intermetatarsal articulation
- Watershed blood supply - nutrient artery meets periosteal supply = poor healing
- 25-50% nonunion rate with conservative treatment (non-athletes may accept this)
- Athletes require surgery - faster healing, lower nonunion, earlier return to sport
- Screw technique critical - entry at tip of tuberosity, largest diameter (minimum 5.5mm), engage far cortex
Clinical Pearls
- "Jones fracture vs avulsion: Jones extends INTO 4-5 intermetatarsal joint, avulsion proximal to it
- "Watershed zone = poor blood supply = high nonunion = need surgical fixation in athletes
- "Conservative treatment = 6-8 weeks NWB cast = 25-50% nonunion = acceptable in sedentary patients
- "Screw size matters - a large (5.5mm or greater) solid screw is recommended in elite athletes (Hunt & Anderson 2011)
- "Bone graft for Torg Type II-III (delayed/nonunion) presentations
Clinical Imaging
Imaging Gallery




Critical Exam Points for Jones Fractures
Zone 2 Location
At metadiaphyseal junction, extends INTO 4-5 intermetatarsal articulation - this defines the Jones fracture
Watershed Blood Supply
Nutrient artery meets periosteal supply here = poor healing = high nonunion
Torg Classification
Type I - screw alone. Type II/III - need bone graft for sclerotic canal
Athlete Management
Early surgery = 8-10 week return vs 15+ weeks conservative
At a Glance: Quick Decision Guide
| Feature | Zone 1 (Avulsion) | Zone 2 (Jones) | Zone 3 (Stress) |
|---|---|---|---|
| Location | Tuberosity | Metadiaphyseal junction | Proximal diaphysis |
| Mechanism | Inversion injury | Acute or stress | Repetitive loading |
| Key Landmark | PROXIMAL to 4-5 IM joint | Extends INTO 4-5 IM joint | DISTAL to 4-5 IM joint |
| Nonunion Risk | Low (under 5%) | HIGH (25-50%) | Very High (over 50%) |
| Treatment | Conservative | Consider surgery | Usually surgical |
| Athlete Protocol | CAM boot 4-6 weeks | IM screw fixation | IM screw + graft |

JONESJONES - Key Features
| J | Junction of metaphysis and diaphysis Zone 2 |
| O | Often requires surgery especially athletes |
| N | Nonunion rate 25-50% with conservative treatment |
| E | Entry point at tip of tuberosity for screw |
| S | Screw size matters use 5.5mm minimum |
| J | Junction of metaphysis and diaphysis Zone 2 | E | Entry point at tip of tuberosity for screw |
| O | Often requires surgery especially athletes | S | Screw size matters use 5.5mm minimum |
| N | Nonunion rate 25-50% with conservative treatment |
Hook:JONES fractures need a JONES approach - Junction location, Often surgical, Nonunion risk, Entry point critical, Screw size important
Overview and Epidemiology
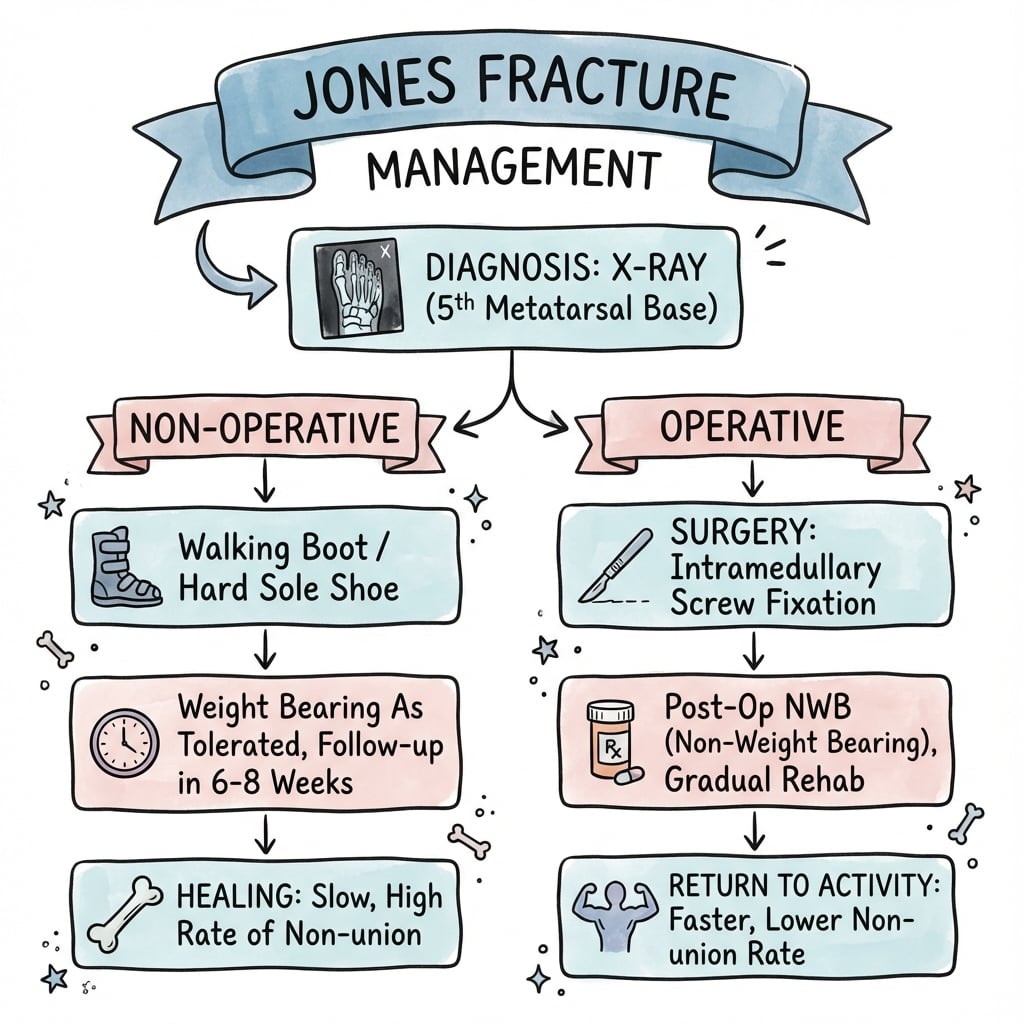
Jones Fractures - Fifth Metatarsal Zone 2
The Jones fracture is a fracture at the metadiaphyseal junction of the fifth metatarsal base (Zone 2), first described by Sir Robert Jones in 1902 (who sustained the injury himself while dancing). It is notorious for its high nonunion rate and prolonged healing time, making it a critical exam topic.
Definitions and Terminology
- Zone 1 (tuberosity avulsion): extra-articular or involving the metatarsocuboid joint; the most common proximal fifth metatarsal fracture; benign.
- Zone 2 (true Jones fracture): at the metadiaphyseal junction, the fracture line extends into the fourth-fifth intermetatarsal articulation; lies in the vascular watershed.
- Zone 3 (proximal diaphyseal stress fracture): distal to the 4-5 joint within the proximal 1.5cm of the diaphysis; usually a fatigue/stress injury with prodromal symptoms and the highest nonunion risk.
Some authors and the Torg series argue the fine anatomical distinction between Zone 2 and Zone 3 matters less than chronicity (sclerosis and canal obliteration) and patient demand, since outcomes track these factors rather than the precise level (Chuckpaiwong 2008).
Epidemiology and Risk Factors
- Peak incidence in young, active adults; strongly associated with cutting, pivoting and jumping sports.
- Mechanism: an adduction/inversion load on a plantarflexed forefoot, or repetitive lateral-column overload (acute-on-chronic).
- Predisposing factors: cavovarus / hindfoot varus alignment concentrating lateral-column load, gastrocnemius tightness, metatarsus adductus, prior fifth metatarsal injury, training-load error and inadequate footwear. Cavovarus that is not addressed is a recognised cause of refracture.
Anatomy/Biomechanics
Fifth Metatarsal Anatomy - Zone 2
Zone 2 - The Critical Location
Anatomical Boundaries:
- Proximal: Level of 4-5 intermetatarsal articulation
- Distal: Junction of metaphysis and diaphysis
- Key feature: Fracture line extends INTO the 4-5 intermetatarsal joint
Zone Differentiation - Exam Critical
How to differentiate Zone 1 from Zone 2:
| Feature | Zone 1 (Avulsion) | Zone 2 (Jones) |
|---|---|---|
| Location | Proximal to 4-5 joint | At/Into 4-5 joint |
| Mechanism | Inversion avulsion | Adduction force |
| Blood supply | Good (cancellous) | Watershed (poor) |
| Nonunion risk | Under 5% | 25-50% |
| Treatment | Almost always conservative | Athletes need surgery |
The key radiographic landmark: Does the fracture line extend INTO the 4-5 intermetatarsal articulation? If YES = Jones (Zone 2).
Classification
Torg Classification
The Torg classification is the most widely used system for Jones fractures, based on radiographic appearance and indicating chronicity.
TORGTORG - Radiographic Classification
| T | Type I Sharp fracture line (acute), no sclerosis |
| O | Type II sclerOsis beginning, widened line (delayed) |
| R | Type III sclerotic medullary canal, Refracture/nonunion |
| G | Graft needed for Type II-III |
| T | Type I Sharp fracture line (acute), no sclerosis | R | Type III sclerotic medullary canal, Refracture/nonunion |
| O | Type II sclerOsis beginning, widened line (delayed) | G | Graft needed for Type II-III |
Hook:TORG tells you if bone Graft is needed
Torg Classification - Jones Fractures
| Type | Radiographic Features | Clinical Scenario | Treatment |
|---|---|---|---|
| Type I - Acute | Sharp fracture margins, no medullary sclerosis, no widening | First-time injury, no prodromal symptoms | Cast (non-athletes) or screw (athletes) |
| Type II - Delayed Union | Widened fracture line, evidence of medullary sclerosis | Previous treatment failure, chronic symptoms | IM screw + consider bone graft |
| Type III - Nonunion | Complete obliteration of medullary canal, sclerosis | Established nonunion, chronic pain | Screw + bone graft + curettage of canal |
Zone I - Avulsion
Torg Type II - Delayed
Torg Type III - Nonunion
Treatment Implications by Torg Type
Radiographic Findings:
- Sharp, well-defined fracture line
- No periosteal reaction
- No medullary sclerosis
- Narrow fracture gap
Treatment Options:
Non-Athletes:
- Non-weight-bearing short leg cast
- 6-8 weeks immobilization
- Accept 25-50% nonunion rate
Athletes:
- Primary intramedullary screw fixation
- Faster union (8-10 weeks vs 15+ weeks)
- Lower nonunion rate (under 5% vs 25-50%)
- Earlier return to sport
Proper technique and attention to detail ensure optimal outcomes.
Clinical Assessment
History and Examination
History
Key Questions:
- Mechanism: How did the injury occur? (acute vs insidious)
- Prodromal symptoms: Any previous lateral foot pain? (suggests chronic component)
- Activity level: Athlete vs sedentary (treatment implications)
- Previous injury: Prior fifth metatarsal fracture (risk factor)
- Timing: When did symptoms begin? (acute vs chronic)
Red Flags for Chronic Component:
- Gradual onset of symptoms before acute event
- History of similar pain that resolved
- Prolonged activity-related pain
- Previous treatment for lateral foot pain
Physical Examination
Inspection:
- Lateral foot swelling
- Ecchymosis (lateral foot)
- Comparison with contralateral foot
Palpation:
- Point tenderness over Zone 2 (metadiaphyseal junction)
- Assess entire fifth metatarsal
- Palpate peroneal tendons
Special Considerations:
- Hindfoot alignment - varus predisposes to lateral overload
- Gastrocnemius tightness - Silverskiold test
- Ankle stability - lateral ligament integrity
- Neurovascular status - usually intact
Location of Tenderness
Differentiating by palpation:
- Zone 1 (Avulsion): Tenderness at tuberosity, at peroneus brevis insertion
- Zone 2 (Jones): Tenderness at metadiaphyseal junction, 1.5cm distal to tuberosity
- Zone 3 (Stress): Tenderness more distal, along proximal shaft
Differential Diagnosis
Lateral foot and fifth metatarsal base pain has several mimics. The key examiner discriminator is whether the fracture line involves the 4-5 intermetatarsal articulation and whether an accessory ossicle (normal corticated margins) is present.
Differential Diagnosis of Proximal Fifth Metatarsal / Lateral Foot Pain
| Condition | Distinguishing Features | Imaging | Management |
|---|---|---|---|
| Zone 1 tuberosity avulsion | Inversion mechanism; tenderness at peroneus brevis insertion; line proximal to 4-5 joint | Transverse line at tuberosity, extra-articular or into cuboid joint | Almost always conservative; symptomatic boot |
| Zone 2 Jones fracture | Acute or acute-on-chronic; line at metadiaphyseal junction into 4-5 joint; watershed zone | Sharp line (Torg I) to sclerotic canal (Torg III) | Screw fixation in athletes; cast option in sedentary |
| Zone 3 proximal diaphyseal stress fracture | Insidious onset, prodromal pain; runners; distal to 4-5 joint | Periosteal reaction, cortical thickening, sclerosis | High nonunion risk - usually screw +/- graft |
| Os peroneum / os vesalianum | Asymptomatic accessory ossicle; smooth corticated margins | Rounded ossicle, no acute lucent line | No treatment unless symptomatic |
| Peroneus brevis/longus tendinopathy or tear | Pain on resisted eversion; tendon-line tenderness; no bony point tenderness | Radiographs normal; ultrasound/MRI shows tendon pathology | Rehabilitation; surgery for tears |
| Lisfranc / tarsometatarsal injury | Midfoot swelling, plantar ecchymosis; pain on midfoot stress | Weight-bearing views, fleck sign; CT for occult injury | Often surgical - missed Lisfranc causes nonunion and arthrosis |
| Cuboid fracture/contusion | Lateral midfoot tenderness over cuboid, not metatarsal base | Oblique radiograph; CT for nondisplaced | Usually conservative |
Investigations
Imaging
Plain Radiographs
Standard Views:
- AP foot - best view for zone identification
- Lateral foot - assess angulation
- Oblique foot - fifth metatarsal profile
Key Radiographic Features:
- Fracture line location relative to 4-5 joint
- Presence of medullary sclerosis
- Fracture line width
- Periosteal reaction
- Evidence of previous healing attempts
SCLEROSISSCLEROSIS - Signs of Chronicity
| S | Sclerotic margins at fracture site |
| C | Canal obliteration medullary |
| L | Lucent zone around fracture |
| E | Evidence of periosteal reaction |
| R | Resorption at fracture edges |
| O | Old callus formation Old callus formation |
| S | Separation of fracture fragments |
| I | Increased density of bone ends |
| S | Suggest bone graft will be needed |
| S | Sclerotic margins at fracture site | E | Evidence of periosteal reaction | S | Separation of fracture fragments |
| C | Canal obliteration medullary | R | Resorption at fracture edges | I | Increased density of bone ends |
| L | Lucent zone around fracture | O | Old callus formation Old callus formation | S | Suggest bone graft will be needed |
Hook:See SCLEROSIS on X-ray = chronic injury = needs bone graft
CT Scan
Indications:
- Assess degree of medullary sclerosis
- Surgical planning for nonunion
- Evaluate for refracture after previous fixation
- Assess healing progress post-operatively
Key Information:
- Medullary canal patency
- Fracture healing
- Hardware position
MRI
Indications:
- Stress reaction without fracture line
- Soft tissue assessment
- Bone marrow edema pattern
- Differentiating acute vs chronic
Findings:
- T1: Low signal at fracture (marrow edema)
- T2/STIR: High signal (edema)
- Chronic: Sclerosis visible
Management
Treatment Algorithm
Management Decision Tree
Key Decision Points:
-
Is the patient an athlete requiring rapid return to sport?
- YES: Surgical fixation (IM screw)
- NO: Consider non-operative if Torg Type I
-
What is the Torg Type?
- Type I: Screw alone may suffice
- Type II: Screw + consider bone graft
- Type III: Screw + bone graft + curettage
-
Has conservative treatment failed?
- YES: Surgical fixation mandatory
- Consider bone grafting
Indications: Sedentary patients, low functional demands, Torg Type I acute fractures, patient accepts 25-50% nonunion risk.
Protocol: Short leg non-weight-bearing cast with strict non-weight-bearing for 6-8 weeks. Serial radiographs every 2-3 weeks. Gradual weight-bearing when radiographic healing seen. Total treatment time 12-20 weeks.
Expected Outcomes: Union rate 50-75%, time to union 15-20 weeks, return to sport 4-5 months if healing occurs.
Surgical Technique
Intramedullary Screw Fixation
Patient Setup: Supine on radiolucent table with bump under ipsilateral hip. Foot must be accessible for fluoroscopy.
Equipment: Fluoroscopy (C-arm), 5.5mm or 6.5mm cannulated screws, guidewires, cannulated drill, and countersink.
Surgical Steps: (1) Approach via direct lateral incision over tuberosity (2-3cm), protecting sural nerve. (2) Entry point critical at tip of tuberosity ("high and medial"). (3) Introduce guidewire under fluoroscopy, confirm central position. (4) Measure screw length, ream if needed (overream 0.5mm). (5) Insert largest screw that fits (5.5mm minimum), engage far cortex. (6) Final check with fluoroscopy AP/lateral/oblique, confirm compression.
Complications
Complications
Risk Factors: Conservative treatment (25-50% rate), Torg Type II-III at presentation, inadequate immobilization, early weight-bearing, smoking, and diabetes.
Treatment: Surgical fixation with bone graft, curettage of sclerotic bone, and consideration of larger screw or plate fixation.
Postoperative Care
Rehabilitation Protocol
Week 0-2: Posterior splint with non-weight-bearing. Elevation and ice for swelling control.
Week 2-6: CAM boot with progressive weight-bearing in boot. ROM exercises out of boot. Pool therapy if available.
Week 6-8: Transition to athletic shoe with full weight-bearing. Progressive strengthening including stationary bike and swimming.
Week 8-10: Sport-specific training begins with cutting and jumping progression. Return to play when criteria met.
Outcomes/Prognosis
Surgical Outcomes
Pooled union rate of approximately 97% with intramedullary screw fixation in athletes (Attia 2021 meta-analysis). Return to sport averages 9-10 weeks. Overall refracture rate is approximately 10% in athletic cohorts; a large solid screw (5.5mm or greater) is recommended to reduce this risk. Hardware removal is rarely needed unless symptomatic.
Conservative Outcomes
Union rate of 50-75% for Torg Type I. Time to union is 6-12 weeks if successful. Refracture risk is higher than surgical. Best reserved for non-athletes with Torg Type I fractures.
Outcomes by Torg Classification
| Type | Union Rate (Non-Op) | Union Rate (Surgical) | Return to Sport |
|---|---|---|---|
| Type I (Acute) | 75% | 95% | 8-10 weeks |
| Type II (Delayed) | 50% | 90% (with graft) | 10-12 weeks |
| Type III (Nonunion) | 25% | 85% (with graft) | 12-16 weeks |
Screw Size and Outcomes
Screw diameter is a key technical factor. A large (5.5mm or greater) solid screw that fills the canal and engages the far cortex is recommended, particularly in elite athletes where undersized hardware is implicated in refracture (Hunt and Anderson 2011). Always use the largest diameter that fits the medullary canal.
Evidence Base
Key Evidence
Early Screw Fixation versus Casting for Acute Jones Fractures (RCT)
- 37 patients randomised (19 screw, 18 cast). Cast group had a 44% failure rate (5 nonunions, 1 delayed union, 2 refractures) versus 1 failure in the screw group. Median time to union and return to sport: 7.5 and 8.0 weeks (screw) versus 14.5 and 15.0 weeks (cast).
Intramedullary Screw Fixation of Jones Fractures: Analysis of Failure
- 15 patients after cannulated screw fixation: 6 failures (4 refractures, 2 symptomatic nonunions). Failures were concentrated among elite (Division I/professional) athletes (83% of failures). Return to full activity before complete radiographic union was the dominant predictor of failure.
Torg Classification of Fifth Metatarsal Base Fractures
- 46 fractures of the fifth metatarsal base distal to the tuberosity, followed for a mean of 40 months. Defined three radiographic types: acute (narrow line, no sclerosis), delayed union (widened line, intramedullary sclerosis), and nonunion (canal obliterated by sclerotic bone). Of 25 acute fractures, 14 of 15 treated by non-weight-bearing cast healed in a mean of 7 weeks; weight-bearing methods healed only 4 of 10. Nonunions were treated by medullary curettage and inlay bone grafting.
Revision Screw Fixation with Bone Grafting for Nonunion/Refracture in Elite Athletes
- 21 elite athletes with Jones fracture nonunion or refracture treated by revision intramedullary screw fixation with autograft or bone-marrow aspirate plus demineralised bone matrix. All achieved cortical union and returned to their previous level of competition at a mean of 12.3 weeks; only 1 subsequent refracture.
Return to Play in NFL Players After Operative Jones Fracture Treatment
- 25 consecutive NFL players treated with a Jones-specific intramedullary screw plus iliac crest bone marrow aspirate and demineralised bone matrix, bone stimulator and orthoses. Return to play was 100%; among the 9 eligible to return in-season, mean return to play was 8.7 weeks. Three players (12%) refractured and required revision.
Return to Play and Union after Surgery for Jones Fractures: Systematic Review and Meta-analysis
- 22 studies, 646 Jones fractures in athletes. Return to play with intramedullary screw fixation 98.8% versus 71.6% nonoperative; time to return to play 9.6 versus 13.1 weeks. Pooled operative union 97.3% versus 71.4% nonoperative; overall refracture rate 10.2%. The authors recommend surgical fixation for all Jones fractures in athletes.
Distinguishing Jones from Proximal Diaphyseal Fifth Metatarsal Fractures
- 32 Jones and 29 proximal diaphyseal fractures. Clinical outcomes did not differ between the two locations; operatively treated patients returned to sport faster. Operative patients with fracture-site sclerosis or canal obliteration had lower satisfaction and higher complication rates.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 22-year-old professional basketball player presents with acute lateral foot pain after landing awkwardly. X-rays show a fracture at the metadiaphyseal junction of the fifth metatarsal with the fracture line extending into the 4-5 intermetatarsal articulation. There is no medullary sclerosis."
Diagnosis:
- Jones fracture (Zone 2 fifth metatarsal fracture)
- Torg Type I (acute) - no sclerosis, sharp fracture margins
- Confirmed by fracture extending into 4-5 intermetatarsal joint
Why NOT an avulsion (Zone 1):
- Zone 1 avulsions are PROXIMAL to the 4-5 joint
- This fracture extends INTO the 4-5 joint = Zone 2 = Jones
Management for Professional Athlete:
- Surgical fixation - intramedullary screw
- Faster return to sport (8-10 weeks vs 15+ weeks conservative)
- Lower nonunion rate (under 5% vs 25-50%)
Surgical Technique:
- Direct lateral approach over tuberosity
- Entry point at tip of tuberosity (high and medial)
- Guidewire across fracture, confirm position fluoroscopically
- 5.5mm or larger solid or cannulated screw
- Engage far cortex, countersink head
Postoperative:
- CAM boot, progressive weight-bearing by 2-4 weeks
- Expected return to sport: 8-10 weeks
- Radiographic healing must be confirmed before return
"A 28-year-old recreational runner had a Jones fracture treated conservatively 4 months ago. She remains symptomatic with lateral foot pain on walking. X-rays show widened fracture line with medullary sclerosis but no complete canal obliteration."
Assessment:
- Failed conservative treatment of Jones fracture
- Torg Type II (Delayed Union) - widened line, partial sclerosis
- Persistent symptoms after 4 months = needs intervention
Why Conservative Treatment Failed:
- Jones fractures have inherently poor blood supply (watershed zone)
- 25-50% nonunion rate with conservative treatment is expected
- This is a predictable outcome, not a complication
Treatment Plan:
- Surgical fixation with bone grafting
- Type II fractures benefit from bone graft to address sclerosis
Surgical Technique:
- Lateral approach to fifth metatarsal base
- Curet the fracture site and medullary canal (remove sclerotic bone)
- Harvest bone graft (proximal tibia or iliac crest autograft)
- Pack morselized graft into canal and around fracture
- Intramedullary screw fixation (5.5mm minimum)
- Confirm position fluoroscopically
Expected Outcome:
- Union rate greater than 90% with screw + graft
- Healing expected 10-14 weeks
- Return to running 3-4 months post-surgery
"A 19-year-old soccer player had Jones fracture fixation with a 4.5mm screw 6 months ago. He returned to play at 8 weeks. He now presents with recurrent lateral foot pain. X-rays show a refracture around the previous screw, which remains in place."
Diagnosis:
- Jones fracture refracture around previous fixation
- Risk factors identified: 4.5mm screw (undersized), early return to sport
Why This Happened:
- Screw too small - undersized hardware is a recognised cause of refracture; a large solid screw (5.5mm or greater) is recommended (Hunt and Anderson 2011)
- Early return to play at 8 weeks before radiographic union - the dominant predictor of failure (Larson 2002)
- Stress concentration at screw tip
Management Plan:
- Remove previous hardware
- Assess medullary canal - likely has sclerosis (Torg Type II-III pattern)
- Curet canal and remove sclerotic bone
- Bone graft - autograft from proximal tibia or iliac crest
- Revision fixation with larger screw (6.5mm if canal allows)
Alternative if Canal Compromised:
- If medullary canal severely damaged or sclerosed
- Consider plantar plate fixation
- Low-profile locking plate on plantar surface
Prevention for Future:
- Use adequate screw size (5.5mm minimum)
- Wait for radiographic healing before return to sport
- Address any biomechanical factors (hindfoot varus, gastrocnemius tightness)
- Consider leaving hardware in place long-term
MCQ Practice Points
Location Question
Q: Where is the Jones fracture located and what distinguishes it from a tuberosity avulsion?
A: Jones fracture is at the metadiaphyseal junction (Zone 2), extending INTO the 4-5 intermetatarsal joint. Tuberosity avulsion (Zone 1) is PROXIMAL to this joint and involves the peroneus brevis insertion.
Blood Supply Question
Q: Why do Jones fractures have a high nonunion rate?
A: The Zone 2 area is a watershed zone where the nutrient artery (entering from medial cortex) meets the periosteal blood supply. This relatively avascular area compromises healing potential.
Classification Question
Q: How does the Torg classification guide treatment?
A: Type I (acute) - screw alone. Type II (delayed union) - screw plus bone graft. Type III (nonunion) - screw plus bone graft plus curettage of sclerotic bone. The classification is based on radiographic appearance.
Surgical Technique Question
Q: What is the minimum recommended screw size for Jones fracture fixation and why?
A: A large (minimum 5.5mm) solid screw is recommended, particularly in elite athletes, because undersized hardware is implicated in refracture and nonunion (Hunt and Anderson 2011). Use the largest diameter that fits and fills the canal with threads crossing the fracture.
Return to Sport Question
Q: When can an athlete return to sport after Jones fracture fixation?
A: 8-10 weeks with radiographic evidence of healing (bridging callus across 3 of 4 cortices). Earlier return risks refracture, especially with undersized screws.
Guidelines, Registries & Global Practice
Global Epidemiology
Proximal fifth metatarsal fractures are among the most common forefoot injuries, and the Zone 2 (Jones) and Zone 3 (proximal diaphyseal stress) patterns are over-represented in cutting and pivoting field sports worldwide - American football, basketball, soccer, rugby and Australian Rules football. Their disproportionate impact on elite athletes (high-profile in-season injuries in the NFL, NBA and European football) has driven a strong international convergence toward early operative fixation in this population (Attia 2021 meta-analysis; Porter 2017).
Side-by-Side Guidance and Evidence Synthesis
There is no single high-level society practice guideline dedicated to Jones fractures; practice is instead anchored on synthesised evidence and expert consensus. The dominant positions across major bodies and the strongest evidence are summarised below.
Practice Positions and Evidence Base for Jones Fractures
| Source / Body | Position | Evidence Level |
|---|---|---|
| AJSM meta-analysis (Attia 2021) | Recommend surgical IM screw fixation for ALL Jones fractures in athletes; superior return to play, union and time to union vs nonoperative | Level IV systematic review of mostly Level IV studies |
| Randomised trial (Mologne 2005) | Early screw fixation halves time to union and return to sport vs casting; 44% cast failure | Level I RCT |
| AO Foundation (AO Surgery Reference) | Acute Zone 2/3: IM screw the standard for active patients; conservative (non-weight-bearing) reasonable for low-demand acute Torg I | Expert consensus / textbook |
| Foot & ankle expert reviews (Porter 2017; Foot Ankle Clin) | IM screw is the preferred construct; 'fit and fill' the canal; biological augmentation and large solid screws for elite athletes and chronic/sclerotic fractures | Level V expert opinion / narrative review |
| General orthopaedic / sports medicine consensus | Sedentary patients with acute Torg I may be offered non-weight-bearing immobilisation after counselling on the substantial nonunion risk | Consensus, supported by RCT and meta-analysis |
Guideline-Level Take-Home
The evidence pyramid for Jones fractures is unusual: a single Level I RCT (Mologne 2005) plus a large meta-analysis (Attia 2021) both point the same way - operative fixation for athletes and active patients, conservative care reserved for low-demand patients who accept a high failure rate. No body recommends routine nonoperative treatment in athletes.
Registry and Real-World Evidence
Unlike arthroplasty, there is no dedicated international Jones-fracture registry; population-level data derive from large athletic cohorts and league injury surveillance (e.g. NFL and professional soccer datasets), which consistently report return-to-play rates above 95% with operative treatment and a persistent refracture rate of roughly 10% (Attia 2021; Lareau 2015). These real-world series confirm that the principal modifiable failure factors are undersized hardware, inadequate biology in sclerotic fractures, uncorrected cavovarus alignment, and premature return to sport before radiographic union (Larson 2002; Hunt and Anderson 2011).
Practice Variation
International practice varies chiefly at the margins rather than the core: the threshold for operating on the recreational or sedentary patient, routine use of biological augmentation (bone marrow aspirate concentrate, demineralised bone matrix, autograft), choice between cannulated and solid screws, and the aggressiveness of return-to-sport timelines. Plantar plating is reserved for revision or canals that cannot accommodate an adequate screw.
Australian Context
Jones fractures are commonly seen in the Australian sporting population, particularly AFL, rugby and soccer players, typically during rapid change of direction or push-off. Australian practice mirrors international consensus, with surgical fixation preferred for athletes and active patients and non-operative management reserved for Torg Type I fractures in low-demand patients after explicit counselling about the high nonunion risk. Sports physicians and orthopaedic surgeons collaborate on staged rehabilitation and return-to-play decisions guided by radiographic healing. Prevention focuses on managing training load, addressing biomechanical factors such as hindfoot varus, and appropriate footwear; smoking cessation support (Quitline 13 7848) is relevant given the adverse effect of smoking on union.
Jones Fractures - Exam Day Essentials
Clinical summary
Key Numbers
- •Zone 2 = Jones fracture location (metadiaphyseal junction)
- •25-50% = Nonunion rate with conservative treatment
- •5.5mm = Minimum recommended screw diameter
- •8-10 weeks = Return to sport after surgical fixation
- •4-5 joint = Fracture extends INTO this joint
Examiner Favorites
- •Differentiate Jones from tuberosity avulsion (Zone 1 vs Zone 2)
- •Why high nonunion rate? Watershed blood supply
- •Describe Torg classification and treatment implications
- •Surgical technique for Jones fracture fixation
Common Mistakes
- •Confusing Zone 1 (avulsion) with Zone 2 (Jones)
- •Using undersized screw (under 5.5mm) leads to refracture
- •Treating athletes conservatively
- •Not recognizing Torg Type II-III need bone grafting
Exam Day Tips
- •Jones = Zone 2 = fracture INTO 4-5 intermetatarsal joint
- •Watershed zone = poor healing
- •Athletes get surgical fixation
- •Torg I = no graft, Torg II-III = bone graft