Salvage Procedure | Failed TKA | PJI | Young Active Patient
- Positioning critical: 0-15° flexion, 5-7° valgus, neutral rotation - allows sitting and walking
- IM nail preferred: Better biomechanics than external fixation, higher union rate (90% vs 75%)
- Limb shortening inevitable: 3-5cm average, requires shoe raise, compensates for stiff knee gait
- Infection control first: In PJI, use 2-stage with antibiotic spacer, minimum 6 weeks antibiotics
- Energy expenditure doubled: Walking requires 50-100% more energy than normal gait
- “Knee arthrodesis is a SALVAGE procedure - last resort after multiple failed revisions
- “Position: 0-15° flexion for sitting, 5-7° valgus for gait, neutral rotation
- “IM nail (modular or long) provides superior fixation vs external fixator
- “Bone grafting essential for metaphyseal defects - allograft or autograft
0-15° flexion, 5-7° valgus, neutral rotation - Wrong position causes severe disability. Too much flexion = cannot walk. Too much extension = cannot sit. Varus = thrust and pain.
Massive bone loss = poor union - Need adequate contact for healing. Bone graft all defects. Consider modular segmental replacement for extreme bone loss (over 10cm).
Never fuse an infected knee - 2-stage approach mandatory for PJI. Antibiotic spacer 6-12 weeks. CRP normalization before fusion. Culture-guided antibiotics.
Young, active, unilateral - Best candidates. Bilateral arthrodesis devastating. Consider amputation vs fusion discussion. Counsel extensively about permanent disability.
- Approach
- Single stage
- Fixation
- Long IM nail
- Key Pearl
- Shortening 3-5cm expected
- Approach
- 2-stage
- Fixation
- Antibiotic spacer then nail
- Key Pearl
- 6-12 week antibiotic holiday
- Approach
- Segmental replacement
- Fixation
- Modular prosthesis
- Key Pearl
- Consider amputation
- Approach
- Primary fusion
- Fixation
- IM nail or plate
- Key Pearl
- Best functional outcomes
Overview and Epidemiology
Knee arthrodesis is the surgical fusion of the distal femur to the proximal tibia, eliminating the knee joint. It is a salvage procedure typically performed after multiple failed total knee arthroplasty revisions, recurrent periprosthetic joint infection, or in cases of massive bone or soft tissue loss where reconstruction is not possible.
- Incidence: 1-2% of failed TKA cases
- Increasing due to rising TKA revision rates
- Male predominance (PJI more common in males)
- Age: Variable (younger patients may prefer limb salvage)
Knee fusion was common before arthroplasty era. Modern indications are almost exclusively salvage after failed reconstruction. The procedure permanently sacrifices knee motion in exchange for a stable, pain-free limb.
Classification and Indications
Indications for Knee Arthrodesis
- Recurrent PJI: Failed 2-stage revision, resistant organisms
- Massive bone loss: Cannot support revision implant
- Extensor mechanism loss: Irreparable quadriceps/patellar tendon rupture
- Failed allograft-prosthetic composite: No remaining reconstruction options
- Young, active patient preferring limb salvage over amputation
- Multiple failed revisions (over 2-3 revisions)
- Severe ligamentous instability not correctable with constrained implant
- Post-traumatic arthritis with severe bone/soft tissue damage
The decision between knee arthrodesis and above-knee amputation should be individualized. Younger, active patients often prefer fusion (limb salvage). Elderly or those with poor bone stock may do better with amputation (better prosthetic function).
FAILEDKnee Fusion Indications
Hook:When TKA has FAILED beyond repair, fusion is the salvage answer!
STOPContraindications to Knee Fusion
Hook:STOP and reconsider if these contraindications are present!
Anatomy and Biomechanics
The fused knee position determines functional outcome. 0-15° flexion allows sitting on chairs. 5-7° valgus matches normal mechanical axis for gait. Neutral rotation prevents abnormal foot progression angle.
-
Bone stock: Often severely deficient after failed TKA/revisions
-
Femoral canal: May be damaged, sclerotic, or have cement
-
Tibial canal: Similar concerns; may have previous stem tracts
-
Soft tissue: Often compromised, previous incisions, extensor mechanism damage
Careful assessment of these anatomical factors is critical for successful fusion.
-
Optimal position:
- Flexion: 0-15° (10-15° preferred for sitting)
- Valgus: 5-7° (matches mechanical axis)
- Rotation: Neutral (0-5° external rotation acceptable)
-
Limb shortening:
- Average 3-5cm after fusion
- Required for foot clearance (stiff knee cannot flex)
- Compensated with shoe raise
-
Energy expenditure:
- Walking requires 50-100% more energy
- Patients have significantly altered gait
- Hip and ankle compensate for lost knee motion
- Too Little
- Cannot sit comfortably
- Optimal
- 0-15°
- Too Much
- Cannot walk (over 30° = wheelchair)
- Too Little
- Varus thrust, pain
- Optimal
- 5-7°
- Too Much
- Excessive valgus, awkward gait
- Too Little
- Toe-out gait
- Optimal
- Neutral
- Too Much
- Toe-in gait, tripping
Clinical Assessment
- Previous surgeries: Number of revisions, infections, complications
- Current symptoms: Pain, instability, drainage
- Infection history: Organisms, antibiotic sensitivities
- Functional status: Ambulatory, walking aids, wheelchair
- Patient expectations: Understand permanent disability
- Skin: Scars, sinuses, soft tissue coverage
- Extensor mechanism: Quadriceps function, patellar tendon
- Stability: Gross instability, range of motion
- Neurovascular: Pulses, sensation, motor function
- Contralateral limb: Function, any abnormalities
Key Assessment Points:
-
Infection status:
- Active drainage/sinus = active infection
- ESR/CRP levels elevation
- Previous culture results and sensitivities
-
Bone stock assessment:
- Previous explant status
- Bone loss quantification
- Canal integrity
-
Soft tissue assessment:
- Multiple incisions
- Skin viability
- Muscle/fascia coverage
- May need plastic surgery consultation
-
Patient counseling:
- Permanent loss of knee motion
- Limb shortening (3-5cm)
- Shoe raise requirement
- Altered gait, increased energy expenditure
- 50% patient satisfaction rate

Investigations
Investigation Protocol
ESR, CRP, WBC - Infection markers. CRP should normalize before definitive fusion in 2-stage protocol. Albumin/prealbumin for nutritional status.
AP/Lateral weight-bearing of entire limb. Assess bone loss, implant position, alignment. Long leg films for mechanical axis planning.
3D reconstruction for bone stock assessment, canal patency, cement location. Essential for surgical planning.
If infection suspected but not confirmed. Tagged WBC scan most specific for PJI.
Aspiration:
- If any suspicion of infection, aspirate before surgery
- Send for cell count, culture (aerobic, anaerobic, fungal, AFB)
- Synovial fluid WBC over 3000 or PMN over 80% = infection


Differential: Choosing the Salvage Option
When standard revision arthroplasty is no longer viable, the decision is between competing salvage strategies. Distinguishing them on the right grounds is a classic viva test.
- Best suited to
- Young, active, unilateral; good bone for apposition
- Key advantage
- Stable painless weight-bearing limb; function better than AKA in ambulators
- Key drawback / discriminator
- Permanent loss of flexion; difficult sitting; shortening
- Best suited to
- Poor bone stock, uncontrollable infection, fit prosthesis users
- Key advantage
- Definitive sepsis control; smoother gait with MPK prosthesis
- Key drawback / discriminator
- Limb loss; phantom pain; energy cost
- Best suited to
- Low-demand, comorbid, non-ambulatory
- Key advantage
- Less surgery; controls infection
- Key drawback / discriminator
- Unstable, often painful flail knee
- Best suited to
- Unfit for surgery; well-fixed implant
- Key advantage
- Avoids major surgery
- Key drawback / discriminator
- Does not eradicate infection; not curative
- Best suited to
- Reconstructable bone, sensitive organism, intact extensor
- Key advantage
- Preserves a mobile knee
- Key drawback / discriminator
- Not viable after repeated failure or major bone/extensor loss
Management Algorithm
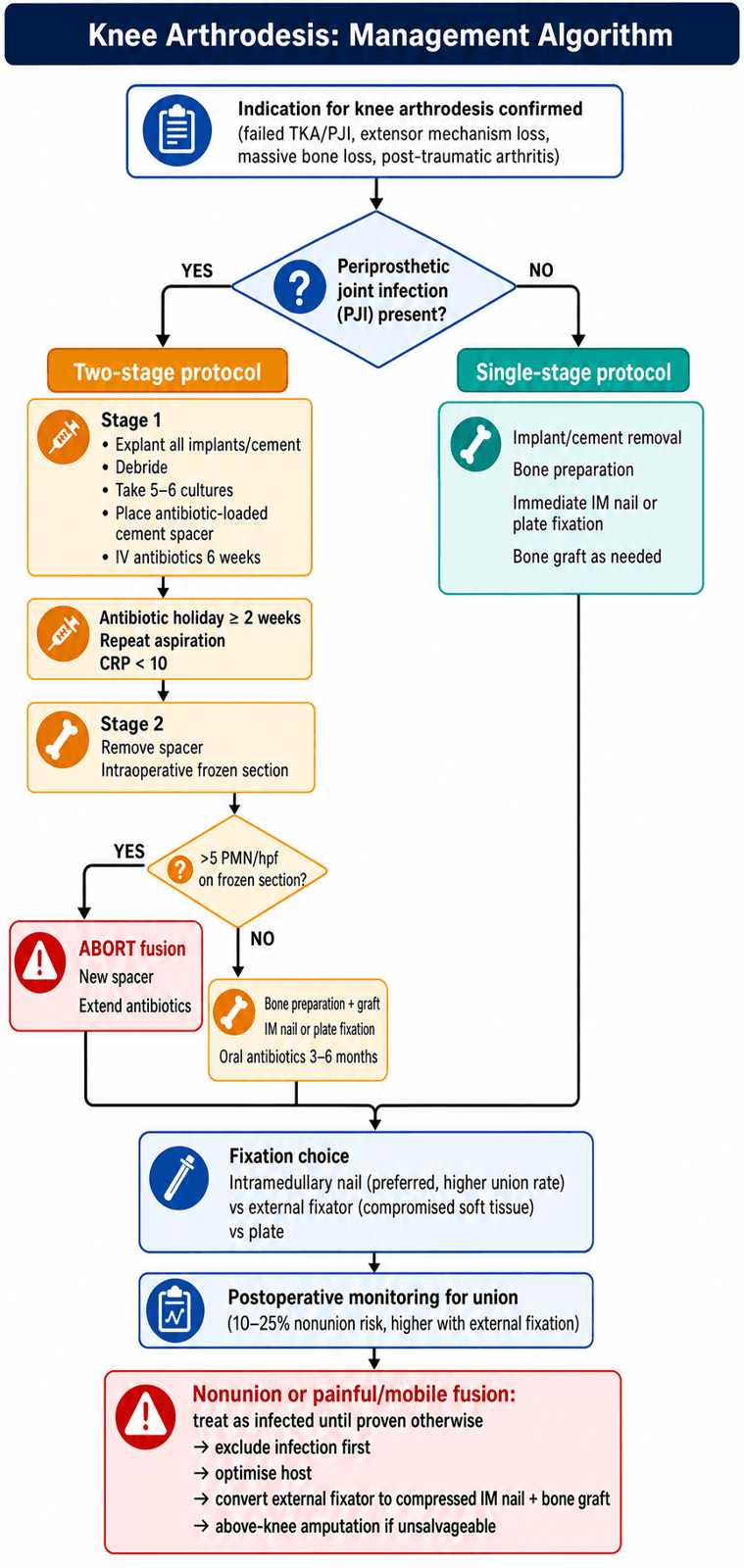
2-Stage Knee Arthrodesis (For PJI)
Stage 1: Explant and Spacer
- Remove all implants and cement
- Aggressive debridement of infected tissue
- Multiple tissue cultures (5-6 samples)
- Antibiotic-loaded cement spacer placement
- IV antibiotics 6 weeks (culture-guided)
Antibiotic Holiday:
- Minimum 2 weeks off antibiotics before Stage 2
- Repeat aspiration to confirm eradication
- CRP should normalize (under 10 mg/L)
Stage 2: Definitive Fusion
- Remove spacer
- Intraoperative frozen section (over 5 PMN/hpf = abort)
- Bone preparation (remove sclerotic bone)
- Bone grafting if needed
- IM nail or plate fixation
- Continue oral antibiotics 3-6 months
If frozen section shows over 5 PMN per high-power field, ABORT the fusion. Place new antibiotic spacer and extend antibiotic treatment. Proceeding with fusion in active infection = high failure rate.
Surgical Technique
Intramedullary Nail Technique (Preferred)
- Supine on radiolucent table
- Bump under ipsilateral hip
- Ensure C-arm access for both AP and lateral views
- Previous midline incision (if present)
- Medial parapatellar arthrotomy
- Remove all implants and cement
IM Nail Steps
Resect to bleeding cancellous bone. Remove sclerotic surfaces. Create flat, opposing surfaces for contact. Aim for maximum bone-to-bone contact.
Ream femoral and tibial canals sequentially. Start with narrow reamer, increase 0.5mm increments. Ream 1mm larger than planned nail diameter.
Align femur to tibia with guide wire. Confirm position: 10-15° flexion, 5-7° valgus, neutral rotation. Use C-arm for AP and lateral confirmation.
Insert modular or long fusion nail. Confirm position fluoroscopically. Lock proximally and distally (2-3 screws each end).
Pack all defects with bone graft (autograft from resected bone, allograft, or combination). Ensure circumferential graft around fusion site.
Nail Options:
- Long TKA revision nail (shortest option, need cement or modular)
- Modular fusion nail (purpose-built, adjustable length)
- Two nails technique (femoral + tibial retrograde/antegrade)
Modular Intramedullary Fusion Nails: What the 'Modular Nail' Actually Is
The OnePager, the decision table and Scenario 3 all reach for a "modular fusion nail" or "modular arthrodesis prosthesis" without defining it - a classic unanswered viva follow-up ("What is a modular fusion prosthesis?"). Being able to describe the hardware is what justifies device selection under examination.
- A long single-piece (through-knee) nail is a full-length nail passed from the piriformis fossa or greater trochanter down across the fused knee into the tibia (as in Puranen's trochanteric-entry series). It gives one continuous column but must violate the hip on insertion, cannot generate compression at the fusion interface, and cannot independently match a mismatched femoral and tibial canal diameter.
- A modular fusion nail is a two-component construct - a femoral segment and a tibial segment joined at a central coupling at the level of the old joint line. Each segment is sized to its own canal, inserted through the knee wound only, and the coupling is then engaged to actively compress the resected femoral and tibial surfaces together. The Wichita Fusion Nail is the archetypal example; other purpose-built systems use a Morse-taper or clamp coupling.
- Compression at the interface improves bone-to-bone contact - the single strongest predictor of union emphasised across the evidence base (Puranen; Conway).
- Independent sizing accommodates the widened, often mismatched canals left after implant and cement removal.
- The hip and ankle are spared - insertion is through the knee, so the nail does not have to transit the hip, and the construct does not create a knee-to-hip stress column.
- Easier exchange/revision than a single long nail if one segment fails.
- Trade-offs: the coupling is a potential mechanical weak point that can loosen, and a modular nail does not bridge a large segmental defect on its own - a gap of more than a few centimetres still needs bone graft, an allograft-prosthetic composite, or a segmental (endoprosthetic) fusion construct.
The modular fusion nail's decisive advantage is active compression across the fusion site with independent femoral and tibial sizing, inserted through the knee without violating the hip. A long single-piece trochanteric-entry nail gives a continuous column but transits the hip and cannot compress. Neither device bridges a large segmental defect alone - that needs grafting or a segmental construct.
Complications
- Incidence
- 10-25%
- Risk Factors
- Infection, bone loss, external fixation
- Management
- Revision surgery, bone graft, change fixation
- Incidence
- 5-15%
- Risk Factors
- Previous PJI, diabetes, immunosuppression
- Management
- Debridement, antibiotics, may need amputation
- Incidence
- 5-10%
- Risk Factors
- Technical error, bone loss
- Management
- Corrective osteotomy (rarely)
- Incidence
- 100%
- Risk Factors
- Inherent to procedure
- Management
- Shoe raise (3-5cm)
- Incidence
- 30-50%
- Risk Factors
- Altered biomechanics
- Management
- Hip/ankle arthritis treatment
Specific Complications:
-
Nonunion: Most common complication. Risk factors include infection, inadequate bone contact, poor fixation. Management: Revision surgery with bone graft and improved fixation.
-
Persistent infection: May require amputation if cannot be controlled. Continuous suppressive antibiotics may be option in some cases.
-
Hardware failure: Nail breakage can occur at fusion site. Usually indicates nonunion.
-
Periprosthetic fracture: Stress riser at nail tip. May need revision fixation.
Managing the Nonunited Knee Arthrodesis
Nonunion is the topic's own most common complication (10-25%, higher after external fixation and in infected or bone-deficient knees), yet the failed fusion deserves its own framework rather than a single line of "revision surgery."
First, exclude infection. Occult or persistent low-grade sepsis is the leading biological cause of a knee-fusion nonunion, so any painful or mobile fusion is treated as infected until proven otherwise - inflammatory markers, interface aspiration and, if operating, intraoperative samples and frozen section drive the plan. (Detailed PJI work-up is covered in the periprosthetic-joint-infection topic.)
- Biological - inadequate bone contact or a residual gap, and a poor host (smoking, malnutrition, low vitamin D, diabetes, immunosuppression).
- Mechanical - insufficient stability or compression (a common reason compression external frames fail), or a broken nail signalling an established nonunion.
- Optimise the host - stop smoking, correct nutrition and vitamin D, and control diabetes before any revision.
- Improve mechanics and biology together - for a failed external-fixation fusion, convert to an intramedullary nail (higher union rate) or re-apply compression; for a failed nail, consider exchange nailing, added compression, or dual-plate augmentation, always combined with bone grafting (autogenous iliac crest, or structural allograft for a defect).
- Biological adjuncts - graft the interface circumferentially; a vascularised fibular graft is an option for a large segmental defect.
- Endpoint - when the limb cannot be salvaged (uncontrolled infection, repeated failure, or unreconstructable bone), above-knee amputation is the definitive alternative (see the amputation topics).
A painful or mobile knee arthrodesis is infected until proven otherwise - work it up before reoperating. Once sepsis is excluded and the host optimised, treat the mechanical and biological deficit together: convert an external frame to a compressed IM nail, add bone graft to every defect, and reserve above-knee amputation for the truly unsalvageable limb.
FUSEKnee Arthrodesis Positioning
Hook:FUSE the knee in the right position to allow the patient to sit and walk!
Postoperative Care
Rehabilitation Protocol
Immobilization: Hinged knee brace locked in extension or long leg cast. NWB with crutches or walker. Wound care. DVT prophylaxis.
TTWB to WBAT as tolerated once X-rays show early callus. Continue brace. Serial X-rays every 3-4 weeks.
Full weight bearing when radiographic union achieved (bridging callus on 3/4 cortices). Wean brace. Shoe raise fitting.
Annual follow-up. Monitor for adjacent joint arthritis. Gait training. Activity modification counseling.
Weight-Bearing Protocol:
- Non-weight bearing 6 weeks minimum
- Progress based on radiographic healing
- Average time to union: 4-6 months
- Some patients require up to 12 months
Outcomes and Prognosis
- IM nail: 85-95%
- External fixation: 65-75%
- Plate fixation: 75-85%
- Walking with aid: 75-80%
- Community ambulator: 60-70%
- Return to work (sedentary): 50-60%
- High satisfaction: 40-50%
- Bone stock quality
- Infection control
- Patient compliance
- Fixation method
- Comorbidities (diabetes, vascular disease)
Counsel patients that knee arthrodesis is a salvage procedure, not a reconstructive one. Expectations should be: pain relief (80-90%), stable limb for ambulation (70-80%), but permanent disability (100%), altered gait (100%), and only moderate satisfaction (50%).
Arthrodesis vs Amputation:
- Knee Arthrodesis
- Yes
- Above-Knee Amputation
- No
- Knee Arthrodesis
- Increased 50-100%
- Above-Knee Amputation
- Increased 40-60%
- Knee Arthrodesis
- Stiff-legged, asymmetric
- Above-Knee Amputation
- Smoother with prosthesis
- Knee Arthrodesis
- Difficult (leg straight)
- Above-Knee Amputation
- Better (prosthesis off)
- Knee Arthrodesis
- N/A
- Above-Knee Amputation
- 30-50%
- Knee Arthrodesis
- 20-30%
- Above-Knee Amputation
- 10-15%
Guidelines, Registries & Global Practice
Global Epidemiology:
- Arthrodesis is performed in roughly 1-2% of failed/infected TKA, but absolute numbers are rising worldwide as primary TKA volume and revision burden grow.
- The dominant modern indication everywhere is unsalvageable periprosthetic joint infection (PJI), followed by extensor mechanism loss and massive bone loss.
- Major joint registries (NJR, AJRR, AOANJRR, SHAR, Norwegian, NZJR) do not track arthrodesis as a distinct procedure; it is captured indirectly within revision/removal codes, so registry data quantify the upstream revision burden rather than fusion outcomes.
- Region
- International
- Position relevant to arthrodesis
- Defines PJI and staged management; arthrodesis/amputation reserved for unreconstructable or uncontrollable infection
- Region
- US
- Position relevant to arthrodesis
- PJI diagnosis/management guidance; salvage (fusion or amputation) after failed staged revision
- Region
- UK
- Position relevant to arthrodesis
- Joint infection pathways through specialist centres; fusion as limb-salvage when revision not viable
- Region
- International
- Position relevant to arthrodesis
- Technical principles of IM nail / plate fusion and compression
- Region
- Europe
- Position relevant to arthrodesis
- Bone & joint infection consensus underpinning staged eradication before fusion
- High-resource settings: MDT care (arthroplasty surgeon, infectious diseases, plastic surgery, microbiology); modular fusion nails and segmental endoprostheses available; microprocessor-controlled prosthetic knees make amputation a competitive functional alternative.
- Limited-resource settings: External fixation (compression frames, Ilizarov) remains a mainstay where implant cost or supply limits modular nails; longer treatment in-frame is accepted in exchange for low hardware cost and the ability to manage active infection.
- Document the permanent loss of knee motion, 3-5 cm shortening with shoe raise, altered high-energy gait, and only moderate satisfaction.
- Record that amputation and continued non-operative management were discussed as genuine alternatives, with realistic union and reinfection figures.
Controversies & Areas of Uncertainty
Comparative cohorts (Hungerer 2017; Trouillez 2021) show similar reinfection and overall function, but amputees with microprocessor knees may report less pain and better quality of life. No randomised data exist; the choice remains values-based.
IM nailing gives higher union but, in infected cases, a higher recurrent-infection risk than external fixation (Mabry 2007). The trade-off, not a single "best" device, drives selection.
Two-stage remains the default for established PJI, but single-stage fusion is debated for sensitive organisms and good soft tissues, mirroring the single- vs two-stage revision debate. Evidence is low-level.
Most authors fuse in slight flexion (0-15°) and 5-7° valgus, but the ideal flexion for balancing sitting against gait energy cost is not standardised and varies with patient height and contralateral limb.
MCQ Practice Points
Q: What is the optimal position for knee arthrodesis? A: 10-15° flexion, 5-7° valgus, neutral rotation. This allows sitting (flexion), matches mechanical axis (valgus), and prevents gait abnormalities (neutral rotation).
Q: Which fixation method has the highest union rate for knee arthrodesis? A: IM nail (85-95%) has superior union rates compared to external fixation (65-75%) or plate fixation (75-85%).
Q: What is an absolute contraindication to knee arthrodesis? A: Ipsilateral hip or ankle fusion. This would create a "flail limb" with no functional joints. Bilateral knee fusion is also a relative contraindication.
Q: How much limb shortening is expected after knee arthrodesis? A: 3-5cm. This is intentional to allow foot clearance during swing phase (stiff knee cannot flex). Compensated with shoe raise.
Q: When should Stage 2 of a 2-stage knee fusion be aborted? A: If intraoperative frozen section shows over 5 PMN per high-power field. This indicates persistent infection. Place new spacer and extend antibiotics.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old male presents with recurrent MRSA PJI following two failed 2-stage revisions for infected TKA. His CRP is elevated at 45 mg/L, he has a draining sinus, and he walks with a frame. His contralateral knee has a well-functioning TKA. X-rays show massive bone loss in the distal femur and proximal tibia. How would you manage this patient?”
“A 58-year-old female had a TKA 3 years ago complicated by patellar tendon rupture. She had two attempts at reconstruction with allograft, both of which failed. She now has no functional extensor mechanism, walks with a locked knee brace, and has valgus instability. There is no evidence of infection. What are your options?”
“A 70-year-old male had multiple revision TKAs, the last being explant for infection with antibiotic spacer in situ. Infection is now controlled (CRP normal, aspiration negative). CT shows greater than 15cm combined bone loss (8cm distal femur, 7cm proximal tibia). His femoral and tibial canals are patent but widened. What are your options for limb salvage?”
Indications
- Failed multiple TKA revisions
- Recurrent PJI (resistant organisms)
- Extensor mechanism loss
- Massive bone loss
Positioning
- Flexion: 10-15° (allows sitting)
- Valgus: 5-7° (matches MA)
- Rotation: Neutral
- Shortening: 3-5cm expected
Fixation
- IM nail preferred (90% union)
- External fix for active infection
- Modular nail for bone loss
- Bone graft all defects
2-Stage Protocol
- Stage 1: Explant + spacer
- IV antibiotics 6 weeks
- Antibiotic holiday 2 weeks
- Stage 2: Fusion if CRP normal
Complications
- Nonunion 10-25%
- Infection 5-15%
- Malposition 5-10%
- Adjacent joint OA 30-50%
Evidence Base
IM Nail vs External Fixation for Infected TKA
- 85 consecutive arthrodeses for infected TKR; retrospective comparison
- IM nail union 23/24 (96%) vs external fixation 41/61 (67%)
- Deep infection recurrence higher with IM nail (8.3%) than ex-fix (4.9%)
- Major complications in 34 patients (40%) irrespective of technique
Arthrodesis of the Knee (Instructional Review)
- Comprehensive instructional review of indications and technique
- Infected TKA is the most common modern indication
- Deficient bone stock and poor apposition reduce fusion success
- Function after arthrodesis is superior to above-knee amputation
Salvage of Infected Total Knee Fusion
- Review of fusion techniques for failed infected TKA
- Compression external fixators least successful when severe bone loss present
- Ilizarov technique achieves rigid fixation despite bone loss
- Internal fixation (IM nail, plate) best for fusion when severe bone loss present
Arthrodesis With Long Intramedullary Nail
- 33 knee arthrodeses with a long trochanteric-entry IM nail
- 29/33 united at first attempt; 32/33 eventually united after correction
- Fusion achieved even in the presence of prior infection; no new infections
- Good bone-to-bone contact between resected surfaces was critical to union
Modular Arthrodesis vs Above-Knee Amputation (Septic TKA)
- Cohort of 113 patients (81 modular arthrodesis, 32 amputation) after septic TKA failure
- Major complication in over one-third of both groups; reinfection 22% (arthrodesis) vs 35% (amputation)
- Functional outcome (LEFS) and physical SF-12 comparable between groups
- Amputees fitted with microprocessor-controlled knees scored significantly higher (LEFS 56)
Above-Knee Amputation vs Arthrodesis (Recurrent PJI)
- Case-control study of 43 patients (20 amputation, 23 arthrodesis) for recurrent knee PJI
- Recurrent infection 10% (amputation) vs 21.7% (arthrodesis); difference not significant
- Amputation group had less pain, better mobility and better SF-36 quality of life
- Mean follow-up 6.7 years