Congenital Cervical Fusion | Segmentation Failure | Classic Triad
- Definition: Congenital fusion of at least two cervical vertebrae due to failure of segmentation.
- Classic Triad: Low posterior hairline, Short neck, Limited cervical ROM (Triad seen in only less than 50% of patients).
- Associations: High rate of associated anomalies. Sprengel's Deformity (30%), Renal (30%), Cardiac (15%), Hearing Loss (30%).
- Instability: The risk is at the hyper-mobile segment adjacent to the fusion. Concern for catastrophic injury.
- Screening: Mandatory Renal US and Cardiac Check. Flexion/Extension views for stability.
- “The most consistent physical finding is Limited Cervical ROM (not the full triad).
- “Radiculopathy/myelopathy occurs in multi-level patterns (Samartzis Type II and III), not single blocks; Type I tends to cause axial neck pain.
- “Think 'VACTERL' - Klippel-Feil overlaps this spectrum of segmentation/formation defects.
- “Avoid collision sports with multi-level or high (C1-C2) fusions or any demonstrated instability.
Adjacent Segment Disease. The segments above or below the fusion compensate with increased motion. This leads to instability and early degeneration.
Contraindication. Patients with multi-level fusions (Type II non-contiguous or Type III contiguous), high (C1-C2) fusion, or demonstrated instability should AVOID collision sports (Rugby, American Football) due to risk of catastrophic cord injury.
30% Association. Renal agenesis, ectopic kidney. Mandatory Renal Ultrasound.
30% Association. Congenital high scapula (omovertebral bone). Always examine the scapula level.
- Incidence
- 30%
- Pathology
- Sprengel's Deformity, Scoliosis
- Action
- X-ray Spine/Scapula
- Incidence
- 25-30%
- Pathology
- Agenesis, Horseshoe kidney
- Action
- Renal Ultrasound
- Incidence
- 15%
- Pathology
- VSD, ASD
- Action
- Echocardiogram
- Incidence
- 30%
- Pathology
- Sensorineural or Conductive Loss
- Action
- Audiology Refer
- Incidence
- 20%
- Pathology
- Synkinesis (Mirror movements), Diastematomyelia
- Action
- MRI Spine
K-FEILKlippel-Feil Associations
Hook:Think 'K-FEIL' to remember the systemic associations.
Overview and Epidemiology
Klippel-Feil Syndrome (KFS) is a congenital condition characterized by the abnormal fusion of two or more cervical vertebrae. It results from a failure of normal segmentation of cervical somites during the 3rd to 8th weeks of gestation.
- Prevalence: Estimated at 1 in 40,000 to 42,000 births (likely under-reported as asymptomatic cases exist).
- Gender: Slight female predominance (60%).
- Genetics:
- Most cases are sporadic.
- Autosomal Dominant and Recessive forms exist (GDF6, GDF3, MEOX1 mutations identified).
- Low Posterior Hairline.
- Short Neck.
- Limited Cervical Range of Motion. Note: This classic triad is present in less than 50% of patients.
- Many patients with limited fusion (Type I) are asymptomatic and live normal lives.
- Symptomatic patients present with neck pain, radiculopathy, or myelopathy, usually in the 2nd or 3rd decade due to degeneration at adjacent overdrive segments.
Pathophysiology and Mechanisms
- Somitogenesis: The vertebral column forms from sclerotomes.
- Segmentation: Requires precise regulation (Notch signaling pathway).
- Failure: KFS is a Failure of Segmentation. (Contrast with Hemivertebra which is Failure of Formation).
- The "Fused" Segment: Is immobile.
- The "Adjacent" Segment: Must compensate to maintain head motion.
- Hyper-mobility: The level above or below the fusion experiences increased stress and range of motion.
- Instability: This hyper-mobility can lead to ligamentous laxity and frank instability.
- Wash-boarding: On flexion-extension views, the segment moves excessively compared to normal.
- C2-C3 Fusion: Most common. Often autosomal dominant.
- C5-C6 Fusion: Second most common. Autosomal recessive association (MEOX1).
- Occipitocervical: Rare but dangerous.
Classification
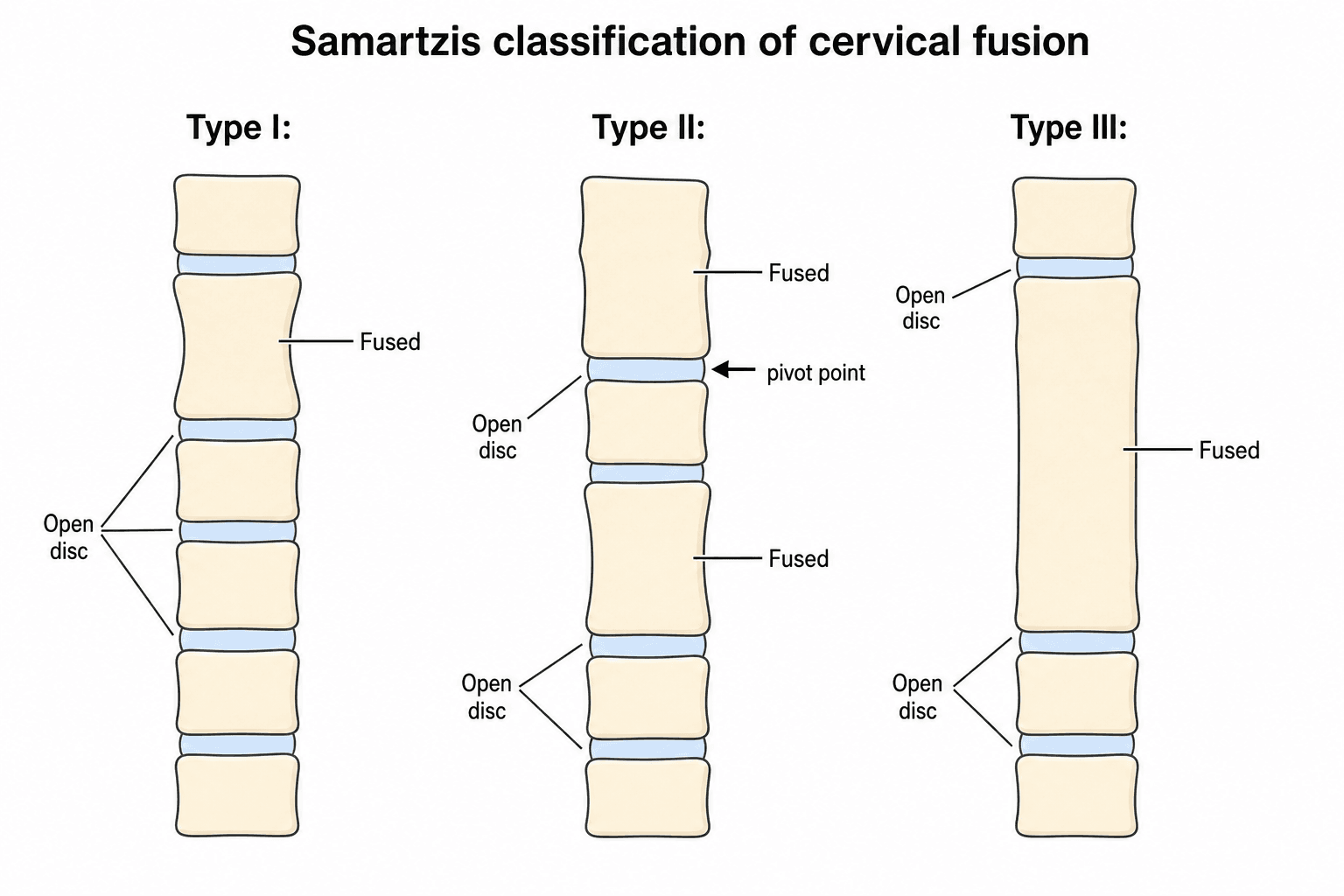
Samartzis Classification
Based on the pattern of fusion and risk of progression.
-
Type I: Single congenital block vertebra.
- Risk: Low. Usually asymptomatic.
-
Type II: Multiple Non-Contiguous fused segments.
- Example: C2-3 fused AND C5-6 fused, with an open intercalated segment.
- Risk: The intercalated open segment becomes a "pivot point" bearing concentrated stress, the classic biomechanical substrate for hypermobility and adjacent-level degeneration.
-
Type III: Multiple Contiguous fused segments.
- Example: C2-3-4-5 all fused into one block.
- Risk: Long stiff lever; tends to show the full clinical triad and, in the Samartzis series, carried the highest rate of radiculopathy/myelopathy.
Key nuance: in Samartzis's own cohort, neurologic symptoms (radiculopathy/myelopathy) arose in Type II AND Type III patients - never Type I (which presented with axial neck pain). Both multi-level patterns warrant surveillance; do not reassure on the basis of a "stable-looking" film alone.
The Craniovertebral Junction: Occipitalization and Basilar Invagination
The most dangerous fusion pattern in KFS sits at the top of the spine. Occipitalization (atlanto-occipital assimilation) - congenital fusion of the atlas to the occiput - concentrates motion at C1-C2 and opens the door to two linked craniovertebral-junction problems.
- Atlantoaxial instability: with the occiput-C1 segment fused, the C1-C2 joint becomes the compensating mobile level and can become unstable, threatening the cord at the cervicomedullary junction.
- Basilar invagination: progressive superior migration of the odontoid through the foramen magnum, which can compress the brainstem and upper cord and produce myelopathy, sleep apnoea or sudden death. The risk rises with the number of fused segments - four or more fused levels confer roughly a sevenfold risk of significant superior odontoid migration (more than about 4.5 mm), and occipitalization is an independent predictor.
- Implication: in a long or high fusion, deliberately assess the craniovertebral junction (CT and MRI, dynamic views) for instability and invagination - it is the lesion most likely to be catastrophic.
Q: A KFS patient has four contiguous fused cervical levels with occipitalization - what is the key craniovertebral-junction risk? A: Basilar invagination from superior odontoid migration (often with atlanto-axial instability), which can compress the brainstem and upper cord. Four or more fused segments and occipitalization markedly increase the risk, so the craniovertebral junction must be specifically imaged and monitored rather than focusing only on the visible block.
Clinical Assessment
- Appearance: Parents notice short neck or asymmetry.
- Function: Difficulty turning head (turning whole body).
- Pain: Neck pain (mechanical) or radicular symptoms (nerve compression).
- Neuro: Weakness, clumsiness (Myelopathy signs).
- Inspection:
- Short neck appearance ("Head sits on shoulders").
- Low hairline.
- Webbed neck (Pterygium colli) - Differentiate from Turner Syndrome.
- Torticollis or facial asymmetry.
- Sprengel's deformity (High scapula).
- Range of Motion:
- Restricted rotation and lateral bending usually.
- Flexion/Extension may be preserved if segments are open.
- Neurology:
- Reflexes (Hyperreflexia? Hoffman's? indicates Myelopathy).
- Strength and Sensation.
- Mirror Movements (Synkinesis): Involuntary movement of one hand when the other moves. Indicates failure of decussation of corticospinal tracts.
- MUST examine for other anomalies (Heart murmur, Scoliosis check).
Short-Low-StiffClinical Triad
Hook:The Classic Triad (though only present in 50%).
Investigations
- Views: AP, Lateral, Open Mouth Odontoid.
- Dynamic: Flexion / Extension views are Critical.
- Look for instability (greater than 3.5mm translation or greater than 11 degrees angulation).
- Look for hyper-mobility at adjacent segments.
- Findings:
- WASP waist appearance (narrowing at fused disc space).
- Loss of disc height.
- Fusion of posterior elements (facets/lamina).
- CT Scan:
- Best for bony architecture.
- Define extent of fusion (anterior vs posterior).
- Surgical planning.
- MRI Spine (Total):
- Mandatory if neuro signs or before surgery.
- Assess cord compression (stenosis at adjacent levels).
- Screen for Chiari malformation, Syringomyelia, Diastematomyelia.
- Renal Ultrasound:
- Screen for agenesis/anomalies (30%).
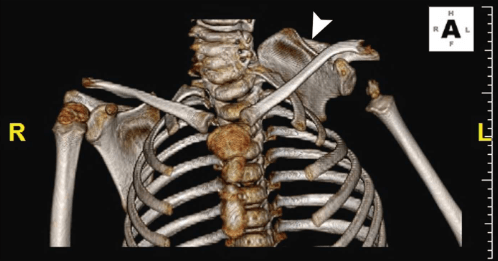

Managing the Associated Sprengel's Deformity
Sprengel's deformity (a congenitally high, hypoplastic, medially-rotated scapula from failure of scapular descent) occurs in roughly 30% of KFS and is often the visible clue to the diagnosis. It deserves its own assessment and plan.
- Grading (Cavendish): clinical severity from Grade 1 (very mild, invisible when dressed) to Grade 4 (severe, the superomedial scapular angle near the occiput, with neck webbing).
- The omovertebral bone: a fibrous, cartilaginous or bony bar tethering the superomedial scapula to a lower cervical spinous process or lamina (present in a substantial minority); it restricts abduction and must be excised when releasing the scapula.
- Surgery (for function and cosmesis, usually around age 3 to 8 years): scapular repositioning by the Woodward procedure (detach and reinsert the medial parascapular muscle origins more inferiorly) or the Green procedure (extraperiosteal muscle detachment with cable traction), combined with omovertebral-bone excision and resection of the prominent superomedial scapular angle.
- The key hazard: brachial plexus traction injury as the scapula is brought down; many surgeons add a clavicular osteotomy (morcellation) before repositioning to reduce this risk during caudal translation.
Q: What is the principal complication when surgically lowering a Sprengel's scapula, and how is it mitigated? A: Brachial plexus traction injury as the scapula is translated caudally. It is mitigated by a clavicular osteotomy (morcellation) before repositioning and by excising the omovertebral bone and superomedial scapular angle so the scapula descends without over-stretching the plexus. Repositioning (Woodward or Green) is best done in early childhood for the greatest remodelling and functional gain.
Differential Diagnosis
A short, stiff neck or congenital cervical fusion has several mimics. The key is to distinguish a true segmentation failure from acquired fusion and from syndromic short-neck appearances.
- Key feature
- Congenital failure of segmentation of 2+ cervical vertebrae
- Discriminator from KFS
- 'Wasp-waist' block vertebra, fused facets/posterior elements present from birth
- Key feature
- Acquired apophyseal joint ankylosis, hypoplastic vertebrae
- Discriminator from KFS
- Inflammatory history, gradual onset, normal disc height early; ankylosis develops over time
- Key feature
- Webbed neck, short stature, gonadal dysgenesis
- Discriminator from KFS
- Karyotype 45,X; cervical vertebrae are NOT fused
- Key feature
- Hemifacial microsomia, epibulbar dermoids, ear anomalies
- Discriminator from KFS
- Craniofacial asymmetry dominates; vertebral fusion may coexist (overlap spectrum)
- Key feature
- KFS + Duane retraction + sensorineural deafness
- Discriminator from KFS
- Triad with abducens/ocular involvement; almost exclusively female
- Key feature
- Acquired bony bridging
- Discriminator from KFS
- Disc space preserved or scarred; clinical history of infection or prior surgery
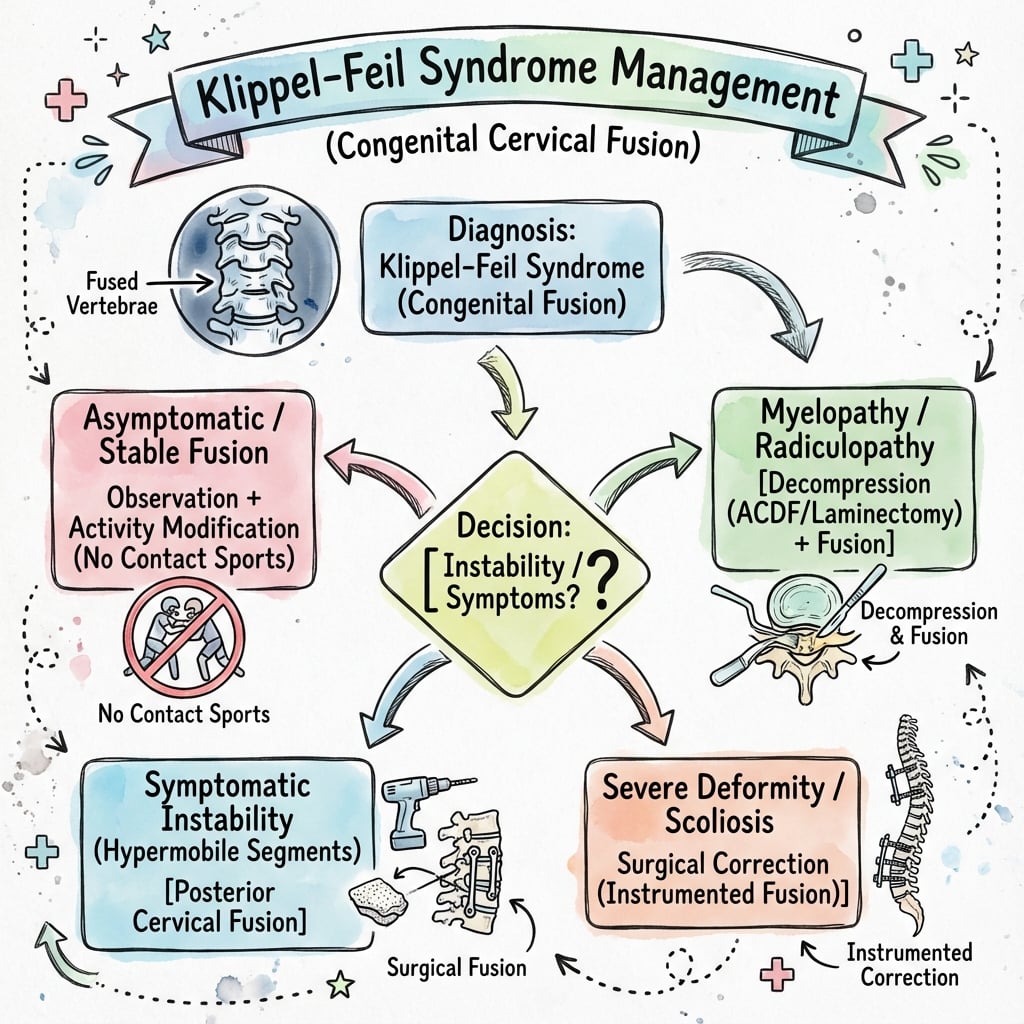
Management Algorithm
Observation and Modification
The mainstay of treatment for most patients (Type I and stable Type III).
- Observation: Regular follow-up to monitor for symptoms of degeneration.
- Activity Modification:
- Collision Sports: AVOID if multi-level fusion (Type II/III), C1-C2 involvement, stenosis, or demonstrated instability (per Torg guidelines).
- Allowed: Swimming, cycling, non-contact sports.
- Physical Therapy: Maintain ROM and strength, but avoid aggressive manipulation (risk of injury).
- NSAIDs: For mechanical neck pain.
Always counsel on the importance of avoiding high-velocity trauma.
Surgical Technique
Posterior Cervical Fusion
Standard for stabilizing an unstable segment.
- Positioning: Prone. Mayfield tongs/halo. Neuro-monitoring essential (SSEP/MEP).
- Exposure: Midline posterior approach. Subperiosteal dissection.
- Instrumentation:
- Lateral Mass Screws (C3-C6).
- Pedicle Screws (C2, C7, T1).
- Wiring: Older technique, less rigid.
- Grafting: Autograft (Iliac crest) or Allograft.
Careful exposure! Anomalous vertebral arteries are common in KFS.
Surgical Tips
- Vascular Study: Pre-operative CTA/MRA is recommended to map the Vertebral Arteries. They often have aberrant courses (enter at C4 or C5) in KFS.
- Intubation: Difficult airway anticipated (limited neck extension). Use Fiberoptic.
7-UpSurgical Risk (Vertebral Artery)
Hook:Vertebral Artery is anomalous (enters Up high) in KFS.
Complications
- Risk Level
- High
- prevention
- Abnormal anatomy + Stenosis. Use Monitoring.
- Risk Level
- Moderate
- prevention
- Pre-op CTA to identify anomalous course.
- Risk Level
- Very High
- prevention
- Fusing one level stresses the next. Inevitable long-term.
- Risk Level
- Low-Mod
- prevention
- Rigid fixation required.
Postoperative Care
Fusion Protocol
- Neuro-checks.
- Collar (Rigid Miami J or Halo depending on fixation).
- Mobilize.
- X-ray check.
- Maintain collar.
- No lifting greater than 5lbs.
- Wean collar if fused.
- Isometrics.
- Lifestyle: Permanent restriction from contact sports often advised if fusion is long.
Outcomes
Prognosis by Type
- Type I (Single block): Usually benign; when symptomatic, typically axial mechanical neck pain rather than neurologic compromise.
- Type II (Non-contiguous): Intercalated open segment is the classic site of hypermobility, instability and accelerated adjacent degeneration; a recognised source of radiculopathy/myelopathy.
- Type III (Contiguous, multi-level): Often presents with the full clinical triad and, in the Samartzis cohort, the highest rate of radiculopathy/myelopathy. Prognosis is further modified by associated anomalies.
Long-Term Considerations
Patients with Klippel-Feil syndrome face unique long-term challenges:
- Accelerated adjacent segment disease: Open segments bear increased stress, leading to early degeneration
- Sports participation: Patients with stable spines who avoid contact sports generally have good function
- Occupational considerations: May need activity modification for jobs involving heavy lifting or neck strain
- Life expectancy: Generally normal unless associated with severe cardiac or renal anomalies
Surgical Outcomes
- Fusion success rate: Generally high (greater than 90%) for posterior cervical fusion
- Symptom relief: Good pain relief and neurological improvement in appropriately selected patients
- Adjacent segment disease: Risk of progression despite successful fusion
- Revision surgery: May be required for pseudarthrosis or adjacent level pathology
Multidisciplinary Care
Optimal management of Klippel-Feil syndrome requires a coordinated team approach with input from orthopaedics, paediatrics, cardiology, nephrology, and genetics to address the full spectrum of associated anomalies and ensure comprehensive patient care.
Guidelines, Registries & Global Practice
Global epidemiology
- Estimated prevalence approximately 1 in 40,000-42,000 live births, with under-reporting because many single-level (Type I) blocks are asymptomatic and found incidentally.
- Slight female predominance reported across series. Most cases are sporadic; familial autosomal dominant (often C2-C3, GDF6) and autosomal recessive (often C5-C6, MEOX1) forms are described.
- KFS overlaps the VACTERL spectrum and syndromes such as fetal alcohol syndrome, Goldenhar (oculo-auriculo-vertebral) and Wildervanck syndrome.
Side-by-side guidance (no single-country frame)
- Focus
- Collision-sport clearance
- Practical recommendation
- Single sub-C3 fusion with full ROM, no stenosis/instability = generally permitted; multi-level, C1-C2 or unstable patterns = relative/absolute contraindication
- Focus
- Screening + surveillance
- Practical recommendation
- Renal ultrasound and echocardiography at diagnosis; dynamic flexion-extension films for stability; MRI if any neurologic sign
- Focus
- MDT pathway
- Practical recommendation
- Tertiary paediatric spine referral; audiology and renal/cardiac screening; counsel on activity restriction
- Focus
- Craniocervical risk
- Practical recommendation
- Heightened vigilance for occipitalization, basilar invagination and superior odontoid migration in long fusions
Registry context
- There is no disease-specific KFS implant registry; KFS is rare and surgery is uncommon. Cervical instrumentation outcomes are extrapolated from national spine and arthroplasty registries and from paediatric deformity databases rather than KFS-specific data.
High- vs limited-resource practice variation
- Well-resourced settings: routine MRI of the whole neuraxis, CT angiography/MRA for vertebral artery mapping, intra-operative neuromonitoring, and panel genetic testing (GDF6, GDF3, MEOX1, RIPPLY2).
- Limited-resource settings: diagnosis often rests on plain radiographs and a careful clinical examination; renal ultrasound (cheap, high-yield) remains the single most valuable screening test; advanced imaging and genetics may be unavailable, raising the importance of clinical screening for cardiac murmurs, hearing loss and scoliosis.
Controversies & Areas of Uncertainty
-
Which fusion pattern is truly "most dangerous"? Classic teaching emphasises the Type II intercalated open segment as the biomechanical risk for instability. However, the Samartzis 2006 cohort found radiculopathy/myelopathy in both Type II and Type III, with Type III carrying the highest neurologic rate. The honest answer for examiners: neurologic risk lives in multi-level patterns (Type II and III), and a single radiograph cannot fully predict an individual's trajectory.
-
Sports clearance thresholds are consensus, not trial-based. The Torg framework is built from registry data and expert opinion; there is no randomised evidence defining a safe level of collision-sport exposure in KFS. Practice therefore errs toward caution, particularly for high (C1-C2) or long fusions.
-
Prophylactic stabilisation is not established. There is no high-level evidence supporting prophylactic fusion of an asymptomatic hypermobile adjacent segment. Surgery remains reserved for instability, progressive deformity, or neurologic compromise.
-
Genetic heterogeneity. GDF6, GDF3, MEOX1 and RIPPLY2 explain only a minority of cases; many patients have no identified mutation, and newer panels implicate additional candidate genes. Genotype-phenotype correlation remains weak, limiting prognostic use of genetics.
-
Optimal screening cadence is undefined. While renal ultrasound and echocardiography at diagnosis are widely accepted, the frequency and duration of subsequent cervical surveillance imaging are not standardised across societies.
MCQ Practice Points
Q: What is the most common associated anomaly in KFS? A: Musculoskeletal (Scoliosis, Sprengel's). Extraspinal: Renal (30%).
Q: Which Samartzis types develop radiculopathy/myelopathy? A: Type II and Type III - never Type I (which causes axial neck pain). In the Samartzis 2006 series, Type III carried the highest rate of radiculopathy/myelopathy, while Type II's intercalated open segment is the classic source of hypermobility/instability.
Q: What is the Torg Ratio significance? A: Used to assess cervical stenosis. Ratio of canal diameter to vertebral body diameter. Less than 0.8 indicates significant stenosis.
Q: What is the 'Wasp-Waist' sign involved in KFS? A: It refers to the narrowing of the vertebral body at the level of the fused disc space, seen on AP/Lateral X-rays. A classic radiographic sign of congenital fusion.
Q: What is the significance of synkinesis (mirror movements)? A: It indicates a failure of decussation of the corticospinal tracts. Often seen in KFS and other midline defects.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe your approach to this patient.”
“Classify this lesion and predict the natural history.”
“What is the connection between this and the cervical fusion?”
Classification (Samartzis)
- Type I: Single Block (axial pain, C2-3 most common)
- Type II: Non-Contiguous (pivot-segment instability)
- Type III: Contiguous (full triad; highest neuro risk)
- Neuro symptoms only in Type II/III, never Type I
Triad (less than 50%)
- Short Neck (Head on shoulders)
- Low Posterior Hairline
- Limited ROM (Most consistent)
- Webbed Neck (Pterygium)
Associations (VACTERL)
- Renal (30%) - URGENT US
- Cardiac (15%) - Echo required
- Sprengel's (30%) - Omovertebral bone
- Hearing Loss (30%) - Audiology
- Scoliosis (60%)
Management
- Observe (Type I / Asymptomatic)
- Modify Activity (No Rugby)
- Fusion (Instability greater than 3.5mm)
- Decompression (Myelopathy)
- Osteotomy (Rare, High Risk)
Evidence Base
Samartzis Radiographic Classification and Symptom Risk
- Single-institution radiographic and clinical review of 28 KFS patients (mean clinical follow-up 8.5 years).
- Defined Type I (single fused segment, 25%), Type II (multiple non-contiguous, 50%) and Type III (multiple contiguous, 25%).
- 64% had no cervical complaints; axial neck symptoms were most strongly associated with Type I.
- Radiculopathy and myelopathy occurred only in Type II and Type III patients, with Type III carrying the highest risk of radiculopathy/myelopathy.
- Mean age at onset of cervical symptoms was 11.9 years; symptomatic neurologic cases diagnosed at a mean of 17.9 years.
Associated Anomalies - the Original Constellation
- Classic series of 50 KFS patients establishing the systemic anomaly constellation.
- Fewer than half had the complete classic clinical triad.
- More than half had scoliosis; approximately one-third had renal anomalies.
- Sprengel's deformity in 21, hearing impairment in 15, synkinesis in 9 and congenital heart disease in 7 patients.
Return-to-Play Guidelines for Cervical Anomalies
- Consensus management guidelines built from over 1,200 cervical lesions in the National Football Head and Neck Injury Registry.
- Stratifies congenital, developmental and post-injury cervical lesions into no, relative, or absolute contraindication to collision sport.
- A single-level fusion below C3 with full motion and no stenosis or instability is generally no contraindication.
- Multi-level fusion, fusion involving C1-C2, occipitocervical fusion, instability or stenosis represent relative or absolute contraindications.
Superior Odontoid Migration Risk
- Prospective radiographic and retrospective clinical review of 27 KFS patients (mean age 13.5 years).
- Mean superior odontoid migration 5.0 mm; C2-C3 was the most commonly fused segment (74%).
- Four or more fused segments conferred an approximately sevenfold relative risk of migration greater than 4.5 mm.
- Occipitalization and increasing number of fused segments were the strongest predictors of migration.
Genetic Basis - GDF6 Mutations
- Identified mutations at the GDF6 locus in familial and sporadic KFS, including a recurrent p.Leu289Pro missense change.
- GDF6 is expressed at developing vertebral, carpal and tarsal boundaries and within the adult disc.
- GDF6 knockdown in Xenopus produced anterior axial (vertebral) defects, supporting a causal role.
- Implicates a bone morphogenetic protein family member in segmentation failure.
Genotype-Phenotype and the Symptomatic Type III Pattern
- Cohort of 25 KFS patients with multigene panel sequencing.
- Limited cervical range of motion was the single most common clinical feature (48%).
- Type III (multiple contiguous) patients were significantly more likely to manifest short neck and limited ROM than Type I or II.
- Novel candidate variants (e.g. COL6A1, CDAN1) detected, broadening the known mutational spectrum beyond GDF6/MEOX1.