Clonal proliferation of CD1a+ dendritic cells - spectrum from eosinophilic granuloma to multisystem disease
- CD1a+ and Langerin+ on immunohistochemistry (pathognomonic)
- Spectrum: Eosinophilic granuloma (unifocal) to Letterer-Siwe (disseminated)
- Skull (50%), femur (20%), ribs (10%), vertebrae (7%)
- Vertebra plana with PRESERVED disc spaces (vs infection)
- BRAF V600E mutation in 50-60% - therapeutic target for refractory disease
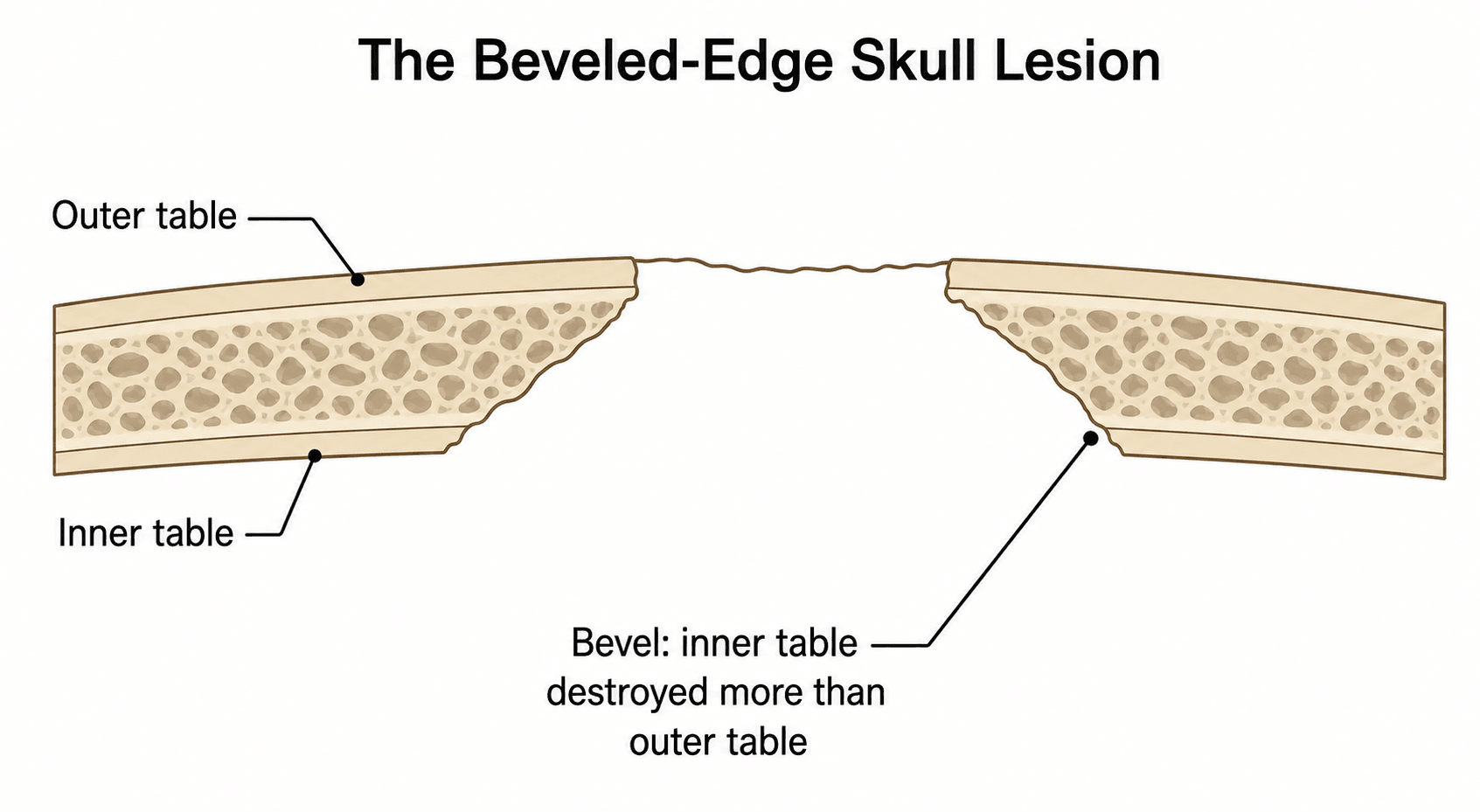
- “Beveled edge skull lesion = pathognomonic for LCH in children
- “Unifocal: observation is valid (50% spontaneous resolution)
- “Risk organs (liver, spleen, marrow) determine prognosis
- “Diabetes insipidus develops in 18-25% with skull lesions
Langerhans Cell Histiocytosis
Epidemiology & Pathogenesis
Demographics
- Peak Incidence: 5-10 years (80% of cases under 15 years)
- Adult Cases: 20% of all LCH, usually unifocal bone
- Neonatal: Rare, often multisystem involvement
- Median Age: 7 years for skeletal LCH
- Male to female ratio: 2:1 overall
- Unifocal disease: Male to female 1.5:1
- Multisystem disease: Male to female 3:1
- Overall: 4-9 cases per million children per year
- Skeletal involvement: 80% of all LCH cases
- Multisystem disease: 20% of LCH cases
- Geographic variation: Higher in Caucasian populations
- Skull: 50% (calvarium, temporal bone, orbit)
- Femur: 20% (diaphysis more than metaphysis)
- Ribs: 10% (posterior ribs common)
- Pelvis: 10% (ilium, acetabulum)
- Vertebrae: 7% (vertebra plana, thoracic greater than lumbar)
- Mandible: 5% (loose teeth, gingival swelling)
- Other: 8% (humerus, scapula, clavicle)
Pathogenesis
-
BRAF V600E Mutation: Present in 50-60% of LCH cases
- Activating mutation in MAPK/ERK pathway
- Higher frequency in multisystem disease (60-70%)
- Associated with increased recurrence risk
- Therapeutic target for refractory disease
-
MAP2K1 Mutations: 20% of BRAF-negative cases
- Alternative MAPK pathway activation
- Similar clinical phenotype to BRAF-mutated LCH
-
Other Alterations: RAS pathway mutations, chromosomal abnormalities (rare)
- Clonal proliferation of myeloid dendritic cells
- Cells express CD1a, CD207 (Langerin), S100 protein
- Birbeck granules on electron microscopy (tennis racket appearance)
- Eosinophils, lymphocytes, macrophages in infiltrate
- sites
- Unifocal or multifocal bone
- age
- 5-30 years
- prognosis
- Excellent (greater than 90% cure)
- current_term
- Unifocal or multifocal bone LCH
- sites
- Multifocal bone + soft tissue
- age
- 2-6 years
- prognosis
- Good with treatment
- current_term
- Multifocal LCH without risk organs
- sites
- Multisystem (bone, skin, organs)
- age
- Less than 2 years
- prognosis
- Guarded (50-70% survival)
- current_term
- Multisystem LCH with risk organs
Modern Classification (Histiocyte Society):
-
Single-System LCH:
- Single-site (solitary eosinophilic granuloma)
- Multiple-site (polyostotic, pulmonary)
-
Multisystem LCH:
- Without risk organ involvement
- With risk organ involvement (liver, spleen, bone marrow, lung)
Clinical Presentation
Skeletal Manifestations
- Localized Pain: 60-70% (worse at night, not relieved by rest)
- Swelling: 50% (soft tissue mass overlying bone lesion)
- Functional Limitation: 30% (limp with lower limb lesions)
- Incidental Finding: 20% (asymptomatic, found on imaging)
- Pathological Fracture: 10-15% (long bone lesions)
- Focal tenderness over lesion
- Soft tissue fullness or mass
- Limited range of motion (vertebral or juxta-articular)
- Low-grade fever (30% of cases)
- Regional lymphadenopathy (uncommon)
- Palpable defect or "hole" in calvarium
- Scalp swelling (subperiosteal extension)
- Mastoid involvement: Chronic otitis media, external auditory canal polyp
- Orbital involvement: Proptosis, visual disturbance
- "Button sequestrum" on X-ray (central bone fragment)
- Back pain with activity
- Thoracic kyphosis (vertebra plana)
- Rarely neurological deficit (less than 5%)
- Complete vertebral collapse possible
- Adjacent disc spaces preserved (key feature)
- Diaphyseal more than metaphyseal
- Periosteal reaction simulating infection
- Pathological fracture with minor trauma
- "Onion-skin" periosteal layering possible
- Loose teeth, gingival swelling
- "Floating tooth" appearance on X-ray
- Jaw pain, trismus
Systemic Manifestations (Multisystem Disease)
- Diabetes insipidus (25% of multisystem cases)
- Exophthalmos (orbital involvement)
- Lytic skull lesions
- Liver: Hepatomegaly, jaundice, dysfunction (poor prognosis)
- Spleen: Splenomegaly, hypersplenism
- Bone Marrow: Cytopenias, pancytopenia
- Lung: Cough, dyspnea, pneumothorax (usually older children/adults)
- Seborrheic dermatitis-like rash (scalp, retroauricular)
- Papular eruption (trunk, groin)
- Present in 30-40% multisystem cases
- Lymphadenopathy (cervical, axillary)
- Hepatosplenomegaly
- Failure to thrive (disseminated disease)
LCH-II Randomised Trial — Risk Organs Drive Mortality
- International randomised trial in multisystem LCH: 193 risk patients (risk-organ involvement or age under 2 years)
- 5-year survival 74% (arm A) vs 79% (arm B); disease reactivation 46% in both arms
- Children under 2 years WITHOUT risk-organ involvement had 100% survival
- Risk-organ-positive non-responders at 6 weeks had the highest mortality
- Adding etoposide (arm B) reduced mortality in risk-organ-positive patients
Investigations
Imaging
- "Punched-out" lytic lesions, well-defined margins
- "Beveled edge" (inner table destruction greater than outer table)
- "Button sequestrum" (central bone fragment)
- "Geographic skull" (multiple coalescent lesions)
- Vertebra plana (complete vertebral collapse, pancake vertebra)
- Preserved disc spaces (key to differentiate from infection)
- Isolated vertebral body involvement
- No paraspinal soft tissue mass (vs tumor, infection)
- Lytic lesion, diaphyseal or metaphyseal
- "Moth-eaten" or permeative bone destruction
- Periosteal reaction (laminated, solid, or "onion-skin")
- Sequestrum formation possible
- Pathological fracture
- T1: Low signal intensity in lesion
- T2: High signal intensity, surrounding marrow edema
- STIR: Bright signal, extensive edema pattern
- Contrast: Marked enhancement (hypervascular)
- Purpose: Define soft tissue extension, spinal canal involvement
- Superior for cortical bone detail
- Delineate skull base and orbital lesions
- Assess vertebral body integrity
- 3D reconstruction for surgical planning
- Bone Scan (Tc-99m): Increased uptake at lesion sites
- PET-CT: Valuable for staging, detecting occult lesions
- Higher sensitivity than skeletal survey for bone lesions
- Detects extraskeletal involvement
- Useful for monitoring treatment response
- Mandatory for all LCH cases
- AP and lateral skull, spine, pelvis
- AP chest (include ribs)
- AP long bones bilaterally
- Detect multifocal disease (affects prognosis and treatment)
- Vertebra plana with PRESERVED disc spaces distinguishes LCH from infection (discitis destroys disc) and metastasis
- "Beveled edge" skull lesions are highly specific for LCH in children
- PET-CT more sensitive than skeletal survey for detecting multifocal disease
- MRI essential if spine lesion to rule out epidural extension or instability
Laboratory Investigations
- CBC: Assess for cytopenias (marrow involvement)
- ESR/CRP: Often elevated but non-specific
- LFTs: Screen for liver dysfunction
- Coagulation: PT/PTT if hepatic involvement
- Renal Function: Baseline before chemotherapy
- Water Deprivation Test: If diabetes insipidus suspected
- Urinalysis: Polyuria, low specific gravity
- Serum and Urine Osmolality: Confirm DI
- Skeletal survey (or PET-CT)
- Chest X-ray/CT (pulmonary involvement)
- Abdominal ultrasound or MRI (liver, spleen)
- Consider bone marrow biopsy if cytopenias
Histopathology
- Tan-gray soft tissue
- Granular, friable consistency
- No gross necrosis or hemorrhage
- Langerhans Cells: Large cells with abundant eosinophilic cytoplasm
- Reniform or "coffee-bean" nuclei (nuclear grooves)
- Eccentric nuclei with fine chromatin
- Eosinophils: Prominent, may form microabscesses
- Lymphocytes: T-cells, scattered macrophages
- Giant Cells: Occasional multinucleated giant cells
- Necrosis: May be present in active lesions
- CD1a: Positive (hallmark, membranous staining)
- Langerin (CD207): Positive (cytoplasmic, more specific than CD1a)
- S100 Protein: Positive (nuclear and cytoplasmic)
- CD68: Variable positivity
- Cytokeratin: Negative (helps exclude carcinoma)
- Birbeck Granules: "Tennis racket" or "zipper" appearance
- Rod-shaped cytoplasmic inclusions
- Diagnostic but not required (CD1a/Langerin sufficient)
- BRAF V600E: Mutation analysis (paraffin tissue or blood)
- Positive in 50-60% of cases
- Guides targeted therapy decisions
- Higher positivity in multisystem disease
LANGERHANSLCH Histological Diagnosis
Hook:LANGERHANS for diagnostic features

Differential Diagnosis
- Osteomyelitis: Fever, elevated WBC/CRP, metaphyseal location
- Discitis: Disc space narrowing (vs preserved in LCH vertebra plana)
- Tuberculous Osteomyelitis: Chronic course, epidemiology
- Differentiation: Blood cultures, bone biopsy, clinical course
- Ewing Sarcoma: Diaphyseal, "onion-skin" periosteal reaction, soft tissue mass
- Osteosarcoma: Metaphyseal, sunburst periosteal reaction, elevated ALP
- Metastases: Neuroblastoma (children), carcinoma (adults)
- Lymphoma: Older children/adults, systemic symptoms
- Differentiation: Biopsy, immunohistochemistry
- Erdheim-Chester Disease: Adults, bilateral femoral/tibial diaphyseal sclerosis
- Rosai-Dorfman Disease: Massive lymphadenopathy, S100+ CD1a- cells
- Juvenile Xanthogranuloma: Skin lesions, CD68+ CD1a- cells
- Fibrous Dysplasia: Ground-glass matrix, no Langerhans cells
- Hyperparathyroidism: Brown tumors, elevated PTH, multiple lesions
- Multiple Myeloma: Adults, monoclonal protein, plasma cells on biopsy
- lch
- 5-10 years peak
- ewing
- 10-20 years peak
- osteomyelitis
- Any age
- fibrous_dysplasia
- Adolescents/adults
- lch
- Skull, femur, ribs
- ewing
- Diaphysis long bones
- osteomyelitis
- Metaphysis
- fibrous_dysplasia
- Ribs, femur, skull
- lch
- Lytic, punched-out
- ewing
- Permeative, onion-skin
- osteomyelitis
- Lytic, periosteal rxn
- fibrous_dysplasia
- Ground-glass, sclerotic rim
- lch
- Minimal to moderate
- ewing
- Large soft tissue mass
- osteomyelitis
- Abscess possible
- fibrous_dysplasia
- None
- lch
- CD1a+ Langerhans cells
- ewing
- Small blue cells, CD99+
- osteomyelitis
- Inflammatory, organisms
- fibrous_dysplasia
- Fibrous stroma, woven bone
- lch
- May have multisystem
- ewing
- Metastases possible
- osteomyelitis
- Fever, sepsis
- fibrous_dysplasia
- McCune-Albright (rare)
Spinal LCH in Children — Long-Term Follow-Up
- 26 children with biopsy-proven spinal LCH (44 involved vertebrae), mean follow-up 9.4 years
- Unexpectedly high proportion of cervical lesions; 62% had multifocal skeletal disease
- Severe lesions often produced asymmetric collapse rather than classic symmetric vertebra plana
- Spinal deformity developed in only 4 children; just 2 of 26 (under 8%) required spinal fusion
- All patients were alive and well with resolution of symptoms at latest follow-up
Management
Risk Stratification
-
Unifocal Bone (60%): Solitary eosinophilic granuloma
- Prognosis: Excellent (greater than 90% spontaneous resolution or cure)
- Treatment: Observation or minimal intervention
-
Multifocal Bone (20%): Multiple bone lesions, no soft tissue
- Prognosis: Good with chemotherapy
- Treatment: Low-dose chemotherapy if 2 or more lesions
-
Without Risk Organs: Bone + skin, lymph nodes
- Prognosis: Good (greater than 90% survival)
- Treatment: Combination chemotherapy
-
With Risk Organs: Liver, spleen, marrow involvement
- Prognosis: Guarded (70-80% survival)
- Treatment: Intensive chemotherapy protocols
Treatment by Disease Extent
- Indications: Asymptomatic, non-weight-bearing bone, no structural risk
- Protocol: Clinical and radiographic monitoring every 3-6 months
- Outcome: 50% spontaneous resolution within 1-2 years
- Duration: Until lesion heals or stabilizes
- Indications: Symptomatic pain, weight-bearing bone, structural risk
- Technique: Intralesional curettage, local adjuvant (phenol, H₂O₂), autograft/allograft
- Outcomes: 90% local control, low recurrence (less than 10%)
- Complications: Pathological fracture during healing (5-10%)
- Technique: Intralesional methylprednisolone (80-120 mg)
- Indications: Vertebral lesions, inaccessible sites
- Outcomes: Effective in 70-80%, may require repeat injection
- Benefits: Minimally invasive, accelerates healing
- Indications: Expendable bones (rib, fibula, clavicle)
- Outcomes: Definitive local control (near 100%)
- Advantage: Tissue diagnosis and cure in single procedure
- Historical Use: Previously common, now avoided in children
- Current Role: Very limited (refractory cases only)
- Dose: 6-10 Gy if absolutely necessary
- Concerns: Secondary malignancy risk, growth plate damage
Unifocal Bone Treatment Principles:
- Observation is VALID first-line (50% spontaneous resolution)
- Curettage for symptomatic lesions or structural concern
- Steroid injection excellent for vertebral lesions (avoid surgery)
- En bloc resection if expendable bone (rib, fibula)
- Avoid radiation in children (malignancy risk)
- Pathological fractures heal with conservative management (cast/brace)
- Vinblastine: 6 mg/m² IV weekly x 6 weeks, then every 3 weeks
- Prednisolone: 40 mg/m² PO daily x 4 weeks, then taper
- Duration: 12 months for multifocal bone, 12-24 months for multisystem
- Add Mercaptopurine or Methotrexate
- More frequent dosing schedule
- Extended duration (24 months)
- Cytarabine (Ara-C): High-dose protocols
- Cladribine (2-CDA): 5 mg/m² IV daily x 5 days, monthly cycles
- BRAF Inhibitors: Vemurafenib, dabrafenib (if BRAF V600E+)
- MEK Inhibitors: Trametinib, cobimetinib
- BRAF V600E Inhibitors: Vemurafenib 20 mg/kg PO BID
- Indications: Refractory multisystem disease with BRAF mutation
- Response Rate: 60-70% in salvage setting
- Toxicity: Rash, photosensitivity, arthralgia
- MEK Inhibitors: For MAP2K1-mutated disease
- Observation: Usually spontaneous reconstitution (50-70%)
- Bracing: If kyphotic deformity or instability
- Steroid Injection: Accelerates healing, reduces pain
- Surgery: Very rare (neurological compromise only)
- Reconstitution: Gradual over 2-5 years, often incomplete
- MRI to assess epidural extension
- Neurosurgical consultation
- Decompression ± stabilization if cord compromise
- Chemotherapy as definitive treatment (surgery adjunct only)
- Conservative management (cast/splint)
- Lesion usually heals concurrently with fracture
- Surgery rarely needed (non-union, severe displacement)
LCH-III Trial — Prolonging Therapy Cuts Reactivation
- Risk-adjusted randomised trial: over 400 multisystem LCH patients stratified by risk-organ involvement
- Risk-organ-positive patients: 5-year survival 84%, reactivation 27% — superior to historical 6-month LCH-I/LCH-II regimens
- Adding methotrexate to vinblastine + prednisone gave no additional benefit
- Risk-organ-negative patients: 12-month treatment lowered 5-year reactivation to 37% vs 54% with 6-month treatment
- Establishes vinblastine + prednisone for 12 months as the standard first-line backbone
VE-BASKET — Vemurafenib in BRAF V600 Histiocytosis
- Histology-independent phase 2 basket study: 26 adults with BRAF V600-mutant histiocytosis (22 Erdheim-Chester disease, 4 LCH)
- Confirmed objective response rate 61.5% (95% CI 40.6-79.8); all evaluable patients achieved stable disease or better
- 2-year progression-free survival 86%, 2-year overall survival 96%
- All 15 patients assessed by FDG-PET achieved a metabolic response (80% complete metabolic response)
- Toxicity: arthralgia, maculopapular rash, fatigue, skin papilloma, QT prolongation
Surgical Considerations
- Diagnostic biopsy (confirm diagnosis)
- Symptomatic relief (pain, mass effect)
- Structural instability (pathological fracture risk)
- Neurological compromise (spinal cord compression)
- Failed conservative management
- Approach based on anatomical site
- Thorough curettage of cavity
- Local adjuvant (phenol, hydrogen peroxide)
- Bone grafting (autograft or allograft)
- Prophylactic fixation if structural concern
- Usually avoid surgery (steroid injection preferred)
- Decompression only if neurological deficit
- Posterior approach for epidural extension
- Anterior corpectomy rarely needed
- Closed reduction and casting usually sufficient
- ORIF if unstable fracture pattern
- Curettage at time of fixation (if accessible)
Management Algorithm

Complications & Prognosis
Complications
- Mechanism: Hypothalamic-pituitary axis involvement
- Presentation: Polyuria, polydipsia, hypernatremia
- Diagnosis: Water deprivation test, low urine osmolality
- Management: Desmopressin (DDAVP) lifelong
- Risk Factors: Craniofacial bone lesions, multisystem disease
- Vertebral collapse and kyphosis (10-15%)
- Limb length discrepancy (femoral lesions)
- Pathological fracture malunion/nonunion (rare)
- Joint stiffness (juxta-articular lesions)
- Premature physeal closure (metaphyseal lesions)
- Associated with multisystem disease
- Cerebellar involvement (ataxia, dysarthria)
- Behavioral and learning difficulties
- MRI: White matter changes, cerebellar atrophy
- Pneumothorax (spontaneous)
- Respiratory failure (diffuse involvement)
- Progressive fibrosis (chronic disease)
- Hearing loss (temporal bone involvement)
- Dental problems (mandibular lesions)
- Sclerosing cholangitis (liver involvement)
- Growth retardation (pituitary dysfunction)
Prognosis
- Survival: Near 100%
- Recurrence: 10-20% (usually at same site)
- Spontaneous Resolution: 50% without intervention
- Long-term Sequelae: Minimal (cosmetic deformity rare)
- Survival: 95-100%
- Disease-Free Survival: 70-80% at 5 years
- Reactivation: 30-40% (new lesions or progression)
- Permanent Disability: 20% (mainly DI, orthopedic)
- Survival: 90-95%
- Reactivation: 40-50%
- Permanent Consequences: 40% (DI, neurocognitive)
- Survival: 70-80% (significantly worse if poor initial response)
- Reactivation: 50-60%
- Permanent Sequelae: 60-70%
- Unifocal bone disease
- Age greater than 2 years
- Single-system involvement
- Good response to initial therapy
- Age less than 2 years
- Risk organ involvement (liver, spleen, marrow)
- Poor initial response to chemotherapy (6 weeks)
- Multisystem disease with greater than 3 organs
RISKORGANSLCH High-Risk Features
Hook:RISK ORGANS for poor prognosis
Neurodegenerative LCH: the Late CNS Sequela
The topic lists "neurocognitive dysfunction", cerebellar involvement, white-matter changes and cerebellar atrophy as complications, and names "neurodegenerative LCH" in its own Controversies section - but never develops this distinct, feared entity, which is a favourite "late-effects" viva.
- What it is. Neurodegenerative LCH (LCH-ND) is a progressive, non-mass CNS syndrome that can appear months to many years after the systemic disease has apparently resolved, and is a leading cause of long-term morbidity in survivors. It is distinct from a space-occupying CNS LCH lesion - there is no tumour to resect.
- Who is at risk. The strongest associations are craniofacial/"CNS-risk" lesions (orbit, mastoid, temporal, sphenoid, maxilla/zygoma), diabetes insipidus, multisystem disease, and BRAF V600E positivity - the same lesions that predict diabetes insipidus predict LCH-ND, and the two often coexist as part of the pituitary-hypothalamic/CNS-risk picture.
- How it presents and looks. Insidious cerebellar signs (ataxia, dysarthria, tremor, dysmetria), pyramidal signs, behavioural/learning decline and eventually cognitive impairment. MRI shows symmetrical T2/FLAIR high signal in the dentate nuclei/cerebellar white matter and basal ganglia, sometimes with cerebellar atrophy - changes that can precede symptoms, so at-risk children are surveilled with MRI.
- Why it matters / management. It is thought to be driven by MAPK-activated myeloid cells seeding the CNS (BRAF V600E has been found in the marrow/blood of affected patients), i.e. a neuro-inflammatory/degenerative process rather than direct tumour. Treatment is difficult and not standardised - options include chemotherapy (cytarabine), and increasingly MAPK-pathway (BRAF/MEK) inhibitors, with the hope (unproven) that early targeted therapy may prevent or halt progression. Established neurodegeneration is often irreversible, which is why recognition and surveillance matter.
Q: A child treated for LCH years ago develops progressive ataxia and dysarthria - what is it and why does it happen? A: Neurodegenerative LCH (LCH-ND) - a progressive CNS syndrome appearing months-to-years after systemic disease, strongly linked to craniofacial/CNS-risk lesions, diabetes insipidus, multisystem disease and BRAF V600E. MRI shows symmetrical dentate-nucleus/cerebellar and basal-ganglia T2/FLAIR signal and it is driven by MAPK-activated myeloid cells seeding the CNS - not a resectable mass. It is a major cause of long-term disability, often irreversible; management (cytarabine, BRAF/MEK inhibitors) is not standardised, so surveillance MRI in at-risk children is key.
Pulmonary LCH: the Smoking-Associated Adult Form
The topic repeatedly flags pulmonary LCH - "usually older children/adults", "strongly smoking-associated", "distinct natural history", with its own line in the guidelines table - but never develops it, and it is examined as a discrete entity quite unlike the paediatric bone disease.
- A different disease in adults. Isolated pulmonary LCH (PLCH) is largely a disease of young-to-middle-aged adult smokers (typically 20-40 years, roughly equal sex incidence). Unlike multisystem childhood LCH it is often a reactive, polyclonal response to cigarette smoke in many cases (though clonal BRAF V600E-positive forms also occur), which is why it behaves differently.
- Presentation. Cough and dyspnoea, or an incidental finding; a classic acute presentation is a spontaneous pneumothorax (from cyst rupture), which can be recurrent. Constitutional symptoms and extrapulmonary disease are usually absent in the isolated pulmonary form.
- Imaging. HRCT is characteristic: combined nodules and thin-walled cysts with an UPPER- and MID-zone predominance and sparing of the costophrenic angles/lung bases - the reverse of the basal predominance of many other cystic/fibrotic lung diseases. The nodules cavitate into cysts over time.
- Management - stop smoking first. Smoking cessation is first-line and can stabilise or regress disease; it is the single most important intervention. Systemic therapy (e.g. cladribine, or MAPK-directed therapy in clonal disease) is reserved for progressive disease, and lung transplantation for end-stage fibrosis (with a risk of recurrence, especially if smoking resumes). Recurrent pneumothorax may need pleurodesis.
Q: How does pulmonary LCH differ from paediatric bone LCH, and what is first-line treatment? A: PLCH is largely a young-adult smoker's disease, often a reactive polyclonal response to smoke; it presents with cough/dyspnoea or spontaneous (often recurrent) pneumothorax. HRCT shows combined nodules and thin-walled cysts with upper/mid-zone predominance and basal sparing. First-line treatment is smoking cessation (can stabilise/regress disease); reserve cladribine/MAPK-directed therapy for progression and transplant for end-stage fibrosis.
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence approximately 4-9 per million children per year; rarer in adults (1-2 per million)
- Peak 1-3 years for multisystem disease; 5-10 years for single-system bone disease
- Slight male predominance (around 1.2-2:1); reported across all populations worldwide
- Bone is the most common organ involved overall (around 80% of paediatric cases)
- Pulmonary LCH in adults is strongly smoking-associated and follows a distinct natural history
Side-by-Side Guidance
- diagnosis
- CD1a + CD207 (Langerin) mandatory; BRAF V600E testing recommended
- first_line
- Vinblastine + prednisone 12 months (LCH-III backbone)
- emphasis
- Risk-organ stratification drives intensity; structured late-effects follow-up
- diagnosis
- Molecular profiling encouraged (BRAF, MAP2K1) at diagnosis
- first_line
- Vinblastine/prednisone; early targeted therapy in refractory MAPK-mutant disease
- emphasis
- Salvage with cytarabine/cladribine; BRAF/MEK inhibitors for refractory disease
- diagnosis
- Biopsy to exclude Ewing sarcoma, osteomyelitis, lymphoma
- first_line
- Observation or intralesional steroid for unifocal bone; curettage if structural risk
- emphasis
- Avoid radiotherapy in children; surgery reserved for instability or neurology
- diagnosis
- HRCT (cysts + nodules, upper-zone), smoking history central
- first_line
- Smoking cessation first-line
- emphasis
- Systemic therapy or transplant for progressive disease
Registry & Trial Networks
- Outcome data are driven by international cooperative trials (LCH-I, LCH-II, LCH-III, LCH-IV) rather than implant/arthroplasty registries
- The Histiocyte Society coordinates global protocol enrolment; regional groups (e.g. NACHO in North America, national paediatric oncology groups in Europe) feed shared datasets
- BRAF/MAPK genotyping is increasingly captured prospectively to stratify targeted-therapy use
High- vs Limited-Resource Practice
- High-resource: routine BRAF/MAP2K1 genotyping, PET-CT staging, access to BRAF/MEK inhibitors and cladribine/cytarabine salvage, long-term endocrine/neurocognitive surveillance
- Limited-resource: diagnosis may rest on morphology plus CD1a/S100 where Langerin and molecular testing are unavailable; skeletal survey substitutes for PET-CT; vinblastine + prednisone remains the affordable, effective backbone; targeted agents often inaccessible
- Universal principles: confirm tissue diagnosis, stage for risk organs, avoid radiotherapy in children, and screen lifelong for diabetes insipidus
Controversies & Areas of Uncertainty
- Reactive vs neoplastic: the discovery of clonal MAPK mutations (BRAF V600E, MAP2K1) reframed LCH as an inflammatory myeloid neoplasm, yet the prominent inflammatory infiltrate keeps the "neoplasia vs immune dysregulation" debate alive.
- Optimal duration of targeted therapy: BRAF/MEK inhibitors produce rapid responses but disease frequently rebounds on cessation, and the ideal duration, role of combination with chemotherapy, and long-term toxicity in children remain undefined.
- Vertebra plana management: the balance between observation, intralesional steroid and bracing is not standardised; most lesions reconstitute, but predicting the minority that deform is imprecise.
- Neurodegenerative LCH: progressive cerebellar/brainstem neurodegeneration can appear years after apparent cure; its pathogenesis, screening interval, and whether early MAPK-directed therapy prevents it are unresolved.
- Role of PET-CT vs skeletal survey: PET-CT is more sensitive for occult and extraskeletal disease, but cost, radiation and access limit universal use, so staging strategy varies by setting.
MCQ Practice Points
Q: What are the diagnostic immunohistochemical markers for Langerhans cell histiocytosis?
A: CD1a positive and Langerin (CD207) positive - these are pathognomonic. Also S100 positive. Cytokeratin negative (differentiates from metastatic carcinoma). Histologically shows Langerhans cells with characteristic coffee-bean nuclei in a background of abundant eosinophils. Birbeck granules (tennis racket shape) on electron microscopy are diagnostic but no longer required.
Q: What is the classic radiographic finding of LCH in the spine?
A: Vertebra plana - complete collapse of a vertebral body with preserved disc spaces. This differentiates LCH from infection (disc destruction) and metastases (variable disc involvement). Most commonly affects thoracic and lumbar spine. Despite dramatic appearance, most cases reconstitute spontaneously and are treated conservatively with observation or bracing.
Q: What is the BRAF mutation significance in LCH?
A: BRAF V600E mutation is present in 50-60% of LCH cases. This establishes LCH as a clonal neoplastic proliferation rather than reactive disorder. Has therapeutic implications - BRAF inhibitors (vemurafenib, dabrafenib) can be used for refractory multisystem disease. Also useful for differentiating from other histiocytic disorders if tissue diagnosis unclear.
Q: How is LCH classified and what determines prognosis?
A: Unifocal (eosinophilic granuloma): Single bone lesion, excellent prognosis (90%+ cure). Multifocal unisystem: Multiple bone lesions, good prognosis. Multisystem without risk organ involvement: Involves bone plus other organs (skin, nodes). Multisystem with risk organ involvement (liver, spleen, bone marrow): Worst prognosis, 70-80% survival. Risk organs define need for systemic chemotherapy.
Q: What is the orthopaedic management approach for unifocal LCH (eosinophilic granuloma)?
A: Conservative management is first-line for most lesions. Options include: Observation alone (many lesions resolve spontaneously), intralesional corticosteroid injection (methylprednisolone), or curettage with bone grafting for large lesions or impending fracture. Surgery indicated only for: neurological compromise, pathological fracture, or diagnostic uncertainty. Radiation reserved for unresectable locations (skull base).
At a Glance
Langerhans cell histiocytosis (LCH) is a clonal proliferation of CD1a+ and Langerin+ dendritic cells with a spectrum ranging from solitary eosinophilic granuloma to disseminated multisystem disease (Letterer-Siwe). It predominantly affects children aged 5-10 years with male predominance (2:1), with the skull (50%) and femur (20%) being the most common skeletal sites. Characteristic findings include "punched-out" lytic skull lesions, vertebra plana in the spine, and histology showing Langerhans cells with coffee-bean nuclei and Birbeck granules. BRAF V600E mutation is present in 50-60% and is a therapeutic target. Treatment ranges from observation/curettage for unifocal bone disease to chemotherapy for multisystem involvement.
SKULLFIRSTLCH Skeletal Sites
Hook:SKULL FIRST for anatomical distribution
Exam Essentials:
- Clonal proliferation of CD1a+ and Langerin+ dendritic cells
- Spectrum: Eosinophilic granuloma (unifocal) to Letterer-Siwe disease (disseminated)
- Peak incidence: Children 5-10 years, males more than females (2:1)
- Skull and femur most common skeletal sites (50% and 20%)
- Biopsy shows Langerhans cells with coffee-bean nuclei and Birbeck granules
- BRAF V600E mutation in 50-60% of cases
- Treatment: Observation (solitary lesion) to chemotherapy (multisystem)
- Prognosis: Excellent for unifocal (90% cure), guarded for disseminated
Clinical Imaging
Imaging Atlas
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old boy presents with a painless scalp swelling for 2 months. X-ray shows a 3 cm well-defined lytic lesion in the left parietal bone with 'beveled edge' appearance. Parents are very concerned about cancer.”
“A 12-year-old girl presents with 3-month history of mid-thoracic back pain. MRI shows complete collapse of T7 vertebral body (vertebra plana) with preserved disc spaces and no epidural extension. Biopsy confirms Langerhans cell histiocytosis. Parents want aggressive treatment to restore vertebral height.”
“A 6-year-old presents with a limp and thigh pain. Radiographs show a lytic, mildly expansile diaphyseal lesion of the femur with laminated periosteal reaction. The referring team is worried about Ewing sarcoma.”
Must-Know Facts
- DEFINITION: Clonal proliferation of CD1a+ and Langerin+ dendritic cells
- SPECTRUM: Eosinophilic granuloma (unifocal) to Letterer-Siwe (disseminated)
- AGE: Peak 5-10 years, males more than females 2:1
- SITES: Skull 50%, femur 20%, ribs 10%, vertebrae 7% (vertebra plana)
- MOLECULAR: BRAF V600E mutation in 50-60% (therapeutic target)
- PROGNOSIS: Unifocal 90%+ cure, multisystem with risk organs 70-80% survival
Diagnostic Triad
- RADIOLOGY: Lytic lesion, punched-out (skull), beveled edge, vertebra plana with preserved discs
- HISTOLOGY: Langerhans cells with coffee-bean nuclei, abundant eosinophils
- IMMUNOSTAINS: CD1a POSITIVE, Langerin (CD207) POSITIVE, S100 positive, cytokeratin negative
- ELECTRON MICROSCOPY: Birbeck granules (tennis racket) - diagnostic but not required
- STAGING: Skeletal survey or PET-CT (PET more sensitive for multifocal)
- LABS: CBC, LFTs, urinalysis - screen for multisystem involvement
Classification & Prognosis
- UNIFOCAL BONE (60%): Single lesion, greater than 90% cure, observation or curettage
- MULTIFOCAL BONE (20%): 2+ bone lesions, 95% survival, chemotherapy if symptomatic
- MULTISYSTEM NO RISK ORGANS: Bone + skin/LN, 90-95% survival, chemotherapy
- MULTISYSTEM WITH RISK ORGANS: Liver/spleen/marrow, 70-80% survival, intensive chemotherapy
- RISK ORGANS: Liver, spleen, bone marrow (poor prognostic factors)
- DIABETES INSIPIDUS: 18-25% develop (higher with skull lesions), permanent in majority
Management Algorithm
- UNIFOCAL ASYMPTOMATIC: Observation (50% spontaneous resolution) OR curettage ± bone graft
- UNIFOCAL SYMPTOMATIC: Curettage + steroid injection OR en bloc if expendable bone (rib, fibula)
- VERTEBRA PLANA: Steroid injection preferred (NOT surgery), 50-70% reconstitution over 2-5 years
- MULTIFOCAL BONE (2+ lesions): Vinblastine + prednisolone x 12 months
- MULTISYSTEM DISEASE: Vinblastine + prednisolone +/- mercaptopurine x 12-24 months
- REFRACTORY: Cladribine, cytarabine, BRAF inhibitors (if V600E+), MEK inhibitors
Viva Traps to Avoid
- DON'T: Recommend surgery for vertebra plana (reconstitutes spontaneously 50-70%)
- DON'T: Skip skeletal survey - must determine unifocal vs multifocal (changes treatment)
- DON'T: Miss diabetes insipidus screening - ask about polyuria/polydipsia on follow-up
- DON'T: Offer radiation in children - avoid due to secondary malignancy risk
- DON'T: Confuse with infection - LCH vertebra plana has PRESERVED disc spaces
- DO: Always check CD1a and Langerin on biopsy (both must be positive)
- DO: Test BRAF V600E mutation (guides targeted therapy if refractory)
- DO: Involve pediatric oncology for multifocal/multisystem disease
Quick Differentials
- EWING SARCOMA: Age 10-20, diaphyseal, large soft tissue mass, CD99+, small blue cells
- OSTEOMYELITIS: Fever, elevated WBC/CRP, metaphyseal, disc space narrowing (vs preserved in LCH)
- FIBROUS DYSPLASIA: Ground-glass matrix, medullary, no Langerhans cells, any age
- METASTASES: Neuroblastoma (children), history of primary, multifocal
- KEY DISTINGUISHER: Biopsy with CD1a+ and Langerin+ cells confirms LCH
Key Evidence & References
Badalian-Very — Discovery of Recurrent BRAF V600E
- Oncogenic BRAF V600E identified in 35 of 61 archived LCH specimens (57%)
- BRAF V600E tended to occur in younger patients but was independent of disease site or stage
- Langerhans cells stained for phospho-MEK and phospho-ERK regardless of mutation status
- Reframed LCH from a reactive process to a clonal neoplasm of the MAPK/ERK pathway
Héritier — BRAF V600E Predicts High-Risk Disease
- French cohort of 315 children: BRAF V600E present in 54.6%
- BRAF V600E enriched in severe disease — 87.8% of multisystem LCH with risk organs vs 43.9% of single-system LCH
- Resistance to first-line vinblastine + corticosteroid: 21.9% (mutant) vs 3.3% (wild-type)
- Higher 5-year reactivation (42.8% vs 28.1%) and more permanent sequelae (27.9% vs 12.6%)
Euro Histio Net / Histiocyte Society Guidelines
- Consensus guidelines for diagnosis, work-up, treatment and long-term follow-up of LCH up to age 18
- Mandate CD1a/CD207 (Langerin) confirmation and systematic staging for risk-organ involvement
- Define single-system vs multisystem disease and risk-organ stratification as the basis for treatment intensity
- Recommend structured surveillance for late effects (diabetes insipidus, neurodegeneration, endocrinopathy)