FLNB (Filamin B) Osteochondrodysplasia | Multiple Congenital Large-Joint Dislocations | Cervical Kyphosis
- FLNB (filamin B) gain-of-function mutations cause the classic autosomal dominant Larsen syndrome by disrupting the actin cytoskeleton of chondrocytes
- Multiple large-joint dislocations - bilateral knees (anterior), hips and elbows - are the defining orthopaedic feature
- Cervical kyphosis (typically mid-cervical) with hypoplastic vertebrae is the dangerous lesion - it can cause progressive myelopathy and sudden death
- Dysmorphic facies (flat/dish face, prominent forehead, depressed nasal bridge, hypertelorism) plus spatulate thumbs and accessory carpal/tarsal bones
- Treat the spine first conceptually - always image and monitor the cervical spine before any anaesthetic or limb surgery
- “The classic neonatal picture is a baby with hyperextended (back-to-front) knees, dislocated hips and bilateral clubfeet - think Larsen syndrome or arthrogryposis
- “Cervical kyphosis is the leading cause of death - screen every patient with a lateral cervical radiograph and treat instability before it causes myelopathy
- “Supernumerary (accessory) carpal and tarsal ossification centres and a short, broad, spatulate distal thumb phalanx are highly suggestive of an FLNB mutation
- “Distinguish from arthrogryposis - Larsen joints are dislocated and often mobile, whereas arthrogrypotic joints are rigidly contracted
- “Order of limb surgery is usually knees and feet first, then hips - reducing the knees makes hip reduction and rehabilitation achievable
Mid-cervical kyphosis with hypoplastic, anteriorly wedged vertebrae is the single most dangerous feature of Larsen syndrome. It can progress to compressive myelopathy and has caused sudden death. EVERY patient needs a lateral cervical spine radiograph, and instability must be evaluated and treated - often by posterior fusion - before it causes neurological deterioration.
The classic autosomal dominant Larsen syndrome is caused by heterozygous missense or small in-frame mutations in FLNB, which encodes the cytoskeletal protein filamin B. The mutations cluster in specific domains (the actin-binding/calponin-homology domain and filamin repeats 14 to 17) and act through a gain-of-function mechanism, not simple loss.
Bilateral large-joint dislocations are the orthopaedic hallmark: anterior knee dislocation (hyperextended knees), hip dislocation and elbow dislocation, usually with bilateral clubfeet. The combination of dislocated knees and clubfeet in a newborn should immediately raise Larsen syndrome.
A classic exam trap. In arthrogryposis the joints are rigidly contracted with absent skin creases; in Larsen syndrome the joints are dislocated and often relatively mobile, the facies are distinctive (flat 'dish' face), and there are accessory carpal/tarsal bones and spatulate thumbs. The cervical spine risk also sets Larsen apart.
FKHOrder of Limb Surgery
Hook:Feet, Knees, Hips - work from the ground up; a reduced knee is what makes hip reduction and rehab possible.
Overview and Epidemiology
Larsen syndrome is a rare congenital osteochondrodysplasia named after the American orthopaedic surgeon Loren Larsen, who in 1950 described children with multiple congenital joint dislocations and characteristic flat facies. According to PubMed, the classic autosomal dominant form is caused by gain-of-function mutations in FLNB, encoding the cytoskeletal protein filamin B, which is essential for skeletal development (DOI). For the orthopaedic surgeon the condition is defined by multiple large-joint dislocations and, crucially, by a cervical kyphosis that can cause myelopathy and sudden death.
- Incidence: Rare; commonly cited around 1 per 100,000 live births
- Gender: Affects males and females
- Inheritance: Classic form autosomal dominant (FLNB); rare recessive forms reported
- Onset: Present at birth (dislocations and clubfeet evident neonatally)
- Penetrance: Variable expressivity; unaffected carriers described
- Intelligence: Usually normal in the FLNB-related form
- Main threat: Cervical kyphosis with myelopathy and respiratory compromise
- Limbs: Staged reconstruction over the first years of life
- Mobility: Many achieve walking after limb reconstruction
- Other: Hearing loss, airway/tracheomalacia and cardiac anomalies can occur
A Spectrum of FLNB Disorders
Larsen syndrome sits at the milder end of a spectrum of FLNB-related skeletal disorders. According to PubMed, the same gene, depending on the variant, can cause atelosteogenesis types I and III and boomerang dysplasia - which are far more severe and often perinatally lethal - as well as the milder spondylocarpotarsal synostosis syndrome (caused by loss-of-function variants) (DOI). Larsen syndrome and the atelosteogenesis-boomerang group share gain-of-function variants clustering in the calponin-homology 2 (CH2) domain and surrounding region.
Why It Matters in the Exam
Larsen syndrome is a favourite paediatric viva and ISAWE topic because it tests three skills at once: pattern recognition of a syndromic child, prioritisation of a life-threatening cervical lesion over the obvious limb deformities, and a logical staged plan for multiple joint reconstructions.
Pathophysiology and Genetics
FLNB and Filamin B
According to PubMed, autosomal dominant Larsen syndrome is caused by heterozygous missense mutations or small in-frame deletions in FLNB on chromosome 3p14, which encodes filamin B, a large cytoskeletal protein that cross-links actin filaments and anchors membrane proteins and signalling molecules (DOI). Filamin B is highly expressed in growth-plate chondrocytes and developing joints. The mutations are non-randomly distributed, clustering in the actin-binding (calponin-homology) domain and in filamin repeats 13 to 17, and they act through a gain-of-function rather than simple loss-of-function mechanism.
- Gene: FLNB on chromosome 3p14
- Protein: Filamin B - actin cross-linking cytoskeletal protein
- Key domains: Actin-binding domain (two calponin-homology domains, CH1/CH2) and Ig-like filamin repeats
- Mechanism: Gain-of-function (mutant protein with abnormal activity)
- Mutation hotspots: CH2 domain, hinge-1 region, repeats 14 to 17
- Chondrocytes: Disordered cytoskeleton and growth-plate organisation
- Joints: Failure of normal joint formation and capsule/ligament integrity leads to dislocation
- Ossification: Accessory and irregular ossification centres (carpus, tarsus, calcaneus)
- Connective tissue: Generalised laxity contributing to instability
- Result: Multiple dislocations plus vertebral and acral anomalies
Genotype, Phenotype and Hotspots
According to PubMed, a molecular and clinical study of 20 Larsen syndrome probands found that all affected individuals were heterozygous for either missense mutations or small in-frame deletions, that three mutations were recurrent (one variant, 5071G to A, was seen in 6 of 20 subjects), and that the clinical signs most strongly predictive of an FLNB mutation were supernumerary carpal and tarsal bones and short, broad, spatulate distal phalanges, particularly of the thumb (DOI). A separate series confirmed clustering of mutations in the CH2 domain and filamin repeats 14 and 15, simplifying diagnostic screening (DOI).
Inheritance and Counselling
The classic FLNB-related Larsen syndrome is autosomal dominant:
- Each child of an affected person has a 50% chance of inheriting the variant.
- Variable expressivity means severity differs even within a family, and unaffected carriers have been described - so a mildly affected parent may be missed.
- Many cases are de novo (new dominant mutation with no family history).
- Rare autosomal recessive forms of Larsen-like syndrome exist (historically more common in some isolated populations) and may carry higher mortality - distinguishing dominant FLNB disease from recessive phenocopies matters for counselling.
- Molecular confirmation of the FLNB variant enables predictive and prenatal testing.
Classification and Disease Spectrum
Larsen syndrome has no surgical "classification system" in the way a fracture does; instead it is classified by inheritance pattern, by its place on the FLNB disease spectrum, and clinically by the pattern of presentation. The tabs below summarise each axis.
Genetic Classification
- Gene / mechanism
- FLNB gain-of-function (missense / small in-frame deletion)
- Inheritance
- Autosomal dominant
- Notes
- The form tested in exams; variable expressivity, de novo cases common
- Gene / mechanism
- Distinct / heterogeneous (phenocopies)
- Inheritance
- Autosomal recessive
- Notes
- Historically reported in isolated populations; may carry worse prognosis
Clinical Features
Clinical Diagnostic Features
The classic clinical picture combines multiple dislocations, a distinctive face and acral anomalies:
- Multiple large-joint dislocations - bilateral anterior knee dislocation, hip dislocation, elbow dislocation
- Bilateral clubfeet (talipes equinovarus) or other foot deformities
- Characteristic facies - flat 'dish' face, prominent forehead, depressed nasal bridge, hypertelorism
- Hand and foot anomalies - short, broad, spatulate thumbs and accessory carpal/tarsal ossification centres
- Spinal anomalies - cervical kyphosis with vertebral hypoplasia, plus scoliosis
- Knees: Bilateral anterior dislocation (tibia dislocates forward on femur), hyperextended at birth
- Hips: Bilateral teratologic dislocation
- Elbows: Dislocation/subluxation, often radial head
- Feet: Bilateral clubfeet; accessory calcaneal ossification (double calcaneus)
- Hands: Spatulate thumbs, broad distal phalanges, accessory carpal bones
- Spine: Mid-cervical kyphosis, vertebral body hypoplasia/clefts, scoliosis
- Facies: Flat ('dish') face, frontal bossing, depressed nasal bridge, hypertelorism
- Airway: Laryngotracheomalacia - risk of airway collapse
- Hearing: Conductive/sensorineural hearing loss reported
- Cardiac: Septal defects and aortic dilatation in some
- Palate: Cleft palate in a minority
- Intellect: Usually normal in FLNB-related disease
The Two Recognised Clinical Patterns
According to PubMed, reported Larsen syndrome patients with craniovertebral involvement broadly fall into two presentation patterns - those presenting early with severe instability and myelopathy, and those presenting later as cervical deformity progresses - which influences the timing and aggressiveness of spinal surgery (DOI).
Physical Examination
- Knees fixed in hyperextension or frank anterior dislocation (the tibia sits anterior to the femur)
- Both hips dislocated; limited abduction
- Bilateral clubfeet with the rigid components of talipes equinovarus
- Broad, spatulate thumbs
- Flat, broad ('dish') face with prominent forehead
- Depressed nasal bridge and widely spaced eyes (hypertelorism)
- Palpable cervical kyphus; assess neck posture and any neurological signs
- Look for long-tract signs (hyperreflexia, clonus) suggesting cervical myelopathy
Investigations and Radiographic Features
Diagnostic Imaging
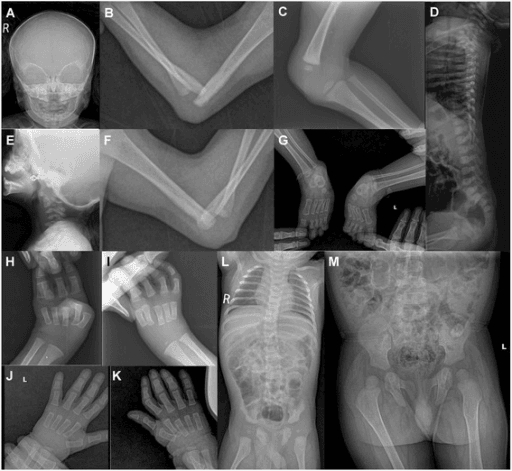
Diagnosis is clinical and radiographic. The package to obtain is: (1) a lateral cervical spine radiograph (and flexion-extension/MRI as indicated) to detect mid-cervical kyphosis, vertebral hypoplasia and instability - this is the priority; (2) radiographs of the dislocated joints (knees showing anterior tibial dislocation, hips, elbows); (3) hand and foot films showing accessory carpal/tarsal ossification centres, a double calcaneus and spatulate distal phalanges; and (4) a scoliosis/whole-spine assessment. Molecular confirmation of an FLNB variant secures the diagnosis.
Regional Findings
Radiographic Features by Region
Mid-cervical kyphosis with hypoplastic, anteriorly wedged vertebral bodies (commonly C4 to C6), often with posterior element/segmentation anomalies and subluxation. This is the lesion that threatens the cord. Cross-sectional imaging (CT/MRI) defines bony detail and cord compression; rarely, dural ectasia complicates the picture and surgery.
Anterior dislocation of the tibia on the femur - the knee is hyperextended and the tibia lies in front of the distal femur. This congenital knee dislocation is one of the most recognisable features.
Bilateral hip dislocation (teratologic) and elbow dislocation/subluxation (often radial head). Assessing hip reducibility guides the timing of open reduction.
Supernumerary carpal and tarsal ossification centres, a double (bipartite) calcaneus, and short, broad, spatulate distal phalanges of the thumb. These acral findings strongly suggest an FLNB mutation. Bilateral clubfeet are usually evident.
Confirmatory and Pre-operative Testing
- Molecular genetic testing: Sequence analysis of FLNB confirms the diagnosis; screening can focus on the mutation hotspot exons (CH2 domain, repeats 14 to 15).
- Cervical spine imaging before ANY anaesthetic: An unstable cervical kyphosis is a major airway and positioning hazard; image and plan before sedation or intubation.
- Airway and cardiac assessment: Evaluate for laryngotracheomalacia and cardiac anomalies as part of pre-operative work-up.

Differential Diagnosis
Larsen Syndrome vs Arthrogryposis Multiplex Congenita
Both present at birth with multiple joint abnormalities and clubfeet, making this the classic exam comparison. The decisive separators are the state of the joints (dislocated versus contracted) and the facies and acral anomalies.
- Larsen Syndrome
- Dislocations (knees, hips, elbows), often mobile
- Arthrogryposis (Amyoplasia)
- Rigid contractures with absent skin creases
- Larsen Syndrome
- Flat 'dish' face, hypertelorism, depressed nasal bridge
- Arthrogryposis (Amyoplasia)
- Often normal face; midline facial haemangioma in amyoplasia
- Larsen Syndrome
- Spatulate thumbs, accessory carpal/tarsal bones
- Arthrogryposis (Amyoplasia)
- Fixed wrist flexion, ulnar deviation; clubfeet
- Larsen Syndrome
- Mid-cervical kyphosis with myelopathy risk
- Arthrogryposis (Amyoplasia)
- Not a characteristic feature
- Larsen Syndrome
- FLNB (filamin B) gain-of-function, autosomal dominant
- Arthrogryposis (Amyoplasia)
- Heterogeneous; fetal akinesia (neuropathic/myopathic)
The flat facies, accessory bones and the dangerous cervical kyphosis point to Larsen; rigid contractures with absent creases point to arthrogryposis.
Management
There is no cure. Management is supportive, anticipatory and multidisciplinary, with two overriding rules. First, the cervical spine takes priority - screen, monitor and treat instability before it causes myelopathy, and protect the neck during any anaesthetic. Second, limb reconstruction follows a logical staged sequence - generally feet and knees before hips - because a reduced, mobile knee is what makes hip reduction and subsequent walking achievable. Decisions are individualised to the child's function rather than driven by trial evidence, which is sparse.
Cervical Spine Management
- Screen every patient with a lateral cervical radiograph; monitor as the child grows
- Track progression with serial imaging - deformity can worsen over time
- Operate before myelopathy - asymptomatic instability is an indication to consider fixation
- Assess the cord with MRI; look for dural ectasia which complicates surgery
- Posterior fusion/fixation is the workhorse for instability and kyphosis
- Anterior decompression added when there is anterior cord compression
- Combined (360 degree) procedures and halo immobilisation for severe deformity
- Growth-sparing constructs in very young children where appropriate
According to PubMed, an institutional series of ten children with craniovertebral junction instability treated by early posterior fixation showed improvement in Nurick myelopathy grade and a halt in disease progression, supporting early surgical stabilisation rather than watchful waiting once instability is identified (DOI). A reported case treated an asymptomatic cervical instability prophylactically with combined anterior and posterior fixation before any neurological deterioration (DOI).
Complications
- Cervical myelopathy from kyphosis/instability - can be progressive
- Sudden death related to cervical cord compression
- Dural ectasia complicating spinal surgery
- Progressive scoliosis requiring instrumentation
- Surgical complications: implant failure, rod breakage, wound problems in long fusions
- Recurrent dislocation / relapse of knees and clubfeet
- Residual stiffness or instability after joint reconstruction
- Airway collapse from laryngotracheomalacia
- Hearing loss (conductive and sensorineural)
- Cardiac: septal defects, aortic root dilatation
The most important examinable complication is cervical kyphosis causing myelopathy and sudden death. According to PubMed, even an asymptomatic cervical instability warrants serious consideration of surgical stabilisation before neurological deterioration, because the consequences of cord compression in this population are catastrophic (DOI). Never anaesthetise or position a Larsen patient without first knowing the state of the cervical spine.
Guidelines, Registries & Global Practice
Global Epidemiology
Larsen syndrome is a rare osteochondrodysplasia, commonly cited at around 1 per 100,000 live births, occurring worldwide and in both sexes. The classic form is autosomal dominant from FLNB gain-of-function variants; rarer autosomal recessive Larsen-like phenotypes have been reported, historically more frequent in some geographically isolated populations. According to PubMed, the FLNB mutation spectrum is clustered and recurrent across international cohorts, with the same gene producing a severity spectrum from Larsen syndrome to lethal atelosteogenesis and boomerang dysplasia (DOI). There is no disease-specific international registry; evidence derives from case reports, institutional series and pooled molecular studies.
Why No Society "Guideline" Exists - and What Governs Practice
No orthopaedic society (AAOS, BOA, EFORT, SICOT) publishes a condition-specific guideline for Larsen syndrome given its rarity. Practice is extrapolated from general principles applied to a child with multiple dislocations and a vulnerable cervical spine:
- Governing principle
- Screen every patient; early posterior fixation for documented instability before myelopathy
- Source of guidance
- Spine case series (Singh 2020; Madera 2008)
- Governing principle
- Serial casting, then percutaneous quadriceps recession or V-Y quadricepsplasty by grade
- Source of guidance
- Congenital knee dislocation protocols (Abdelaziz 2011)
- Governing principle
- Open reduction (teratologic), usually after knees and feet
- Source of guidance
- Case-series experience (Matar 2017)
- Governing principle
- Ponseti method for clubfeet, anticipate relapse
- Source of guidance
- General clubfoot principles
- Governing principle
- Standard surveillance and treatment thresholds, with growth-sparing options
- Source of guidance
- Scoliosis Research Society principles
- Governing principle
- Autosomal dominant FLNB, 50% recurrence, variable expressivity
- Source of guidance
- Clinical genetics standards
Registry and Evidence Notes
- Implant/arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, Norwegian, NZJR) do not capture Larsen syndrome separately; there are no registry-level outcome data specific to this condition.
- Best available synthesis: narrative reviews and institutional spine series are the closest thing to evidence-based guidance; the FLNB molecular studies provide the most robust diagnostic and counselling data.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: FLNB sequencing, MRI-based cervical assessment, multidisciplinary spine/paediatric-orthopaedic/genetics/cardiology/ENT teams, and staged reconstruction with growth-sparing spinal constructs.
- Limited-resource settings: diagnosis is clinical and radiographic (multiple dislocations plus dish facies plus accessory bones), the cervical lateral radiograph is the single highest-value investigation, and Ponseti casting plus staged open reductions deliver meaningful function at low cost.
Genetic Counselling (Universal)
- Classic FLNB form is autosomal dominant: each child of an affected person has a 50% recurrence risk.
- Variable expressivity and reported unaffected carriers mean apparently unaffected parents should be examined.
- Distinguish dominant FLNB disease from rarer recessive Larsen-like phenotypes, which may carry a worse prognosis.
- Prenatal or preimplantation genetic testing is feasible once the family's FLNB variant is known.
Controversies and Areas of Uncertainty
With an incidence around 1 in 100,000 and no randomised trials, virtually all management is extrapolated from case reports, small series and general paediatric-orthopaedic principles. Examiners reward a candidate who states the principle, prioritises the cervical spine, and frankly acknowledges the limited evidence base.
Whether to stabilise an asymptomatic cervical kyphosis prophylactically, and exactly when, is debated. The weight of opinion favours early fixation once instability is documented, given the catastrophic consequences of cord compression, but thresholds rest on small series.
Most authors favour feet and knees before hips, but the optimal order, timing and indication for each procedure (for example bilateral hip open reduction in a non-ambulator) remain individualised and based on case-series experience.
Historically reported autosomal recessive 'Larsen' cases may represent distinct entities or phenocopies. Distinguishing true FLNB-related dominant disease from recessive lethal multiple-pterygium-like conditions matters for prognosis and counselling.
Although mutations cluster in defined FLNB domains, expressivity is so variable - including unaffected carriers - that genotype cannot reliably predict an individual child's severity or course.
The Recessive Larsen-like Form (CHST3)
The topic mentions rare autosomal recessive 'Larsen-like' phenotypes several times but never names the gene.
- The recessive Larsen-like form is CHST3. The classic dominant disease is FLNB, but a distinct autosomal recessive 'Larsen-like syndrome' is caused by biallelic mutations in CHST3 (carbohydrate sulfotransferase 3, a chondroitin-6-sulfotransferase that sulfates cartilage proteoglycan). It overlaps historically with 'humero-spinal dysostosis' and 'spondyloepiphyseal dysplasia with congenital joint dislocations'.
- How it differs from FLNB disease. CHST3 disease shares congenital large-joint dislocations, clubfeet and short stature, but tends to show a spondyloepiphyseal dysplasia with progressive kyphoscoliosis, prominent elbow dislocation with limited elbow extension, and sometimes cardiac valve disease - and it lacks the FLNB acral signature (spatulate thumbs, accessory carpal/tarsal bones).
- Why it matters. The inheritance is recessive (25 percent recurrence, not 50), so distinguishing FLNB-dominant Larsen from CHST3-recessive Larsen-like disease by phenotype and gene testing changes both counselling and prognosis.
Q: What causes the recessive 'Larsen-like' syndrome, and how does it differ from classic Larsen?
A: Classic Larsen is dominant FLNB (filamin B); the recessive 'Larsen-like' form is biallelic CHST3 (carbohydrate sulfotransferase 3, a chondroitin-6-sulfotransferase - overlapping historically with humero-spinal dysostosis / spondyloepiphyseal dysplasia with congenital joint dislocations). CHST3 disease shares congenital large-joint dislocations, clubfeet and short stature but shows a spondyloepiphyseal dysplasia with progressive kyphoscoliosis, prominent elbow dislocation/limited extension and sometimes cardiac valve disease, and lacks the FLNB acral signs (spatulate thumbs, accessory bones). Inheritance is recessive (25 percent recurrence, not 50) - so distinguishing them changes counselling.
LARSENCardinal Features of Larsen Syndrome
Hook:Spell LARSEN and you recall the dislocations, the face, the gene, the deadly spine, the extra bones and the feet.
DISHLarsen versus Arthrogryposis
Hook:The flat 'DISH' face is the clue - and each letter separates Larsen from arthrogryposis.
Why the Cervical Kyphosis Progresses and Threatens the Cord
The topic repeatedly calls the cervical kyphosis the lethal lesion but never explains why it progresses or how it damages the cord.
- A deficient anterior column that cannot resist flexion. The mid-cervical (about C4 to C6) vertebral bodies are hypoplastic and anteriorly wedged, often with segmentation and posterior-element anomalies. Combined with the generalised ligamentous laxity of the syndrome, the anterior column cannot resist flexion, so the segment collapses progressively into a kyphosis apexed at the deficient vertebra.
- The cord is draped over the apex. As the kyphosis worsens, the spinal cord is stretched and compressed over the bony apex (chronic anterior compression plus traction), producing a progressive myelopathy - spasticity, long-tract signs, respiratory compromise - and the risk of sudden death.
- It worsens with growth, so treat early. The deformity is dynamic and progresses through childhood, and a collapsed kyphosis is far harder to reduce - which is the rationale for serial imaging and early posterior fixation before cord compression rather than watchful waiting.
Q: Why does the cervical kyphosis in Larsen syndrome progress and threaten the cord?
A: The mid-cervical (about C4 to C6) vertebral bodies are hypoplastic and anteriorly wedged, and combined with the syndrome's generalised ligamentous laxity the anterior column cannot resist flexion - so the segment collapses progressively into a kyphosis apexed at the deficient vertebra. As it worsens the cord is draped and stretched over the bony apex (chronic anterior compression plus traction), giving progressive myelopathy (spasticity, long-tract signs, respiratory compromise) and sudden-death risk. It progresses with growth and a collapsed kyphosis is hard to reduce - the rationale for serial imaging and early posterior fixation before cord compression, not watchful waiting.
Viva Practice Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn presents with bilateral hyperextended knees, both hips dislocated and bilateral clubfeet. The face looks flat with a depressed nasal bridge. What is your diagnosis and what is your immediate priority?”
“You have confirmed Larsen syndrome in a 6-month-old with dislocated knees, dislocated hips and clubfeet. How do you sequence the orthopaedic reconstruction, and why?”
“How would you distinguish Larsen syndrome from arthrogryposis multiplex congenita, and why does it matter?”
Must-Know Facts
- Rare osteochondrodysplasia; classic form autosomal dominant from FLNB (filamin B) gain-of-function on 3p14
- Defining feature: multiple large-joint dislocations - bilateral anterior knees, hips, elbows
- Cervical kyphosis with hypoplastic vertebrae is the life-threatening lesion (myelopathy, sudden death)
- Dish facies, hypertelorism, depressed nasal bridge; spatulate thumbs and accessory carpal/tarsal bones
- Incidence around 1 per 100,000; usually normal intelligence
Key Radiographic Findings
- Lateral cervical spine: mid-cervical kyphosis, vertebral hypoplasia, instability (priority film)
- Knees: anterior dislocation of tibia on femur (hyperextended)
- Hips and elbows: bilateral dislocation/subluxation
- Hands/feet: accessory carpal/tarsal centres, double calcaneus, spatulate distal thumb phalanx
- Bilateral clubfeet; scoliosis on whole-spine assessment
Management Principles
- Screen and treat the cervical spine first - image before any anaesthetic
- Early posterior fixation for documented cervical instability (before myelopathy)
- Limb sequence: feet and knees before hips
- Knees: casting, then quadriceps recession or V-Y quadricepsplasty by grade; hips: open reduction
- Multidisciplinary care: genetics, cardiology, ENT/airway, physiotherapy
Common Exam Traps
- Missing the cervical kyphosis by focusing on the limbs
- Confusing Larsen (dislocations) with arthrogryposis (contractures)
- Anaesthetising without knowing cervical spine status
- Attempting closed reduction of teratologic hips
- Reducing hips before knees, leaving a stiff extended knee
Evidence Base
A Molecular and Clinical Study of Larsen Syndrome Caused by Mutations in FLNB
- Twenty Larsen syndrome probands and affected relatives evaluated for FLNB mutations and phenotype
- All affected individuals were heterozygous for missense mutations or small in-frame deletions
- Three mutations were recurrent; one (5071G to A) was seen in 6 of 20 subjects
- Mutations cluster in the actin-binding domain and filamin repeats 13 to 17 (non-random)
- Supernumerary carpal/tarsal bones and short, broad, spatulate distal thumb phalanges best predict an FLNB mutation
Larsen Syndrome and Associated Spinal Deformities
- Reviews the genetic basis, clinical features and treatment of Larsen syndrome
- Caused by mutations in FLNB encoding filamin B, crucial for skeletal development
- Core features are joint dislocations, characteristic facies and spinal anomalies
- May be treated conservatively initially but usually requires surgical intervention
- Surgical options include posterior spinal fusion, anterior decompression, circumferential arthrodesis, single-stage 360-degree fixation and growth-sparing procedures
Craniovertebral Junction Instability in Larsen Syndrome: An Institutional Series and Review
- Ten symptomatic children with craniovertebral junction instability underwent 12 surgeries (2011 to 2019)
- Posterior fixation improved median Nurick myelopathy grade and reduced anti-spasticity drug needs
- Neck pain improved in nine patients; five returned to school
- Early posterior fixation halted disease progression
- Describes two clinical presentation patterns informing surgical timing
Management of Joint Dislocations of the Lower Limb in Larsen Syndrome: Practical Approach
- Larsen syndrome child with bilateral dislocated hips and knees and severe clubfeet, 7-year follow-up
- Clubfeet and dislocated knees treated early with Ponseti casts that included the knees
- Open reduction and V-Y quadricepsplasty used for a resistant knee
- Bilateral open hip reduction performed later, after the knees were addressed
- Sequence and timing of interventions guided by functional needs; clubfoot relapse needed posteromedial release