Capitellar Osteochondrosis | Self-Limiting | Boys Under 10 | Excellent Prognosis
- Osteochondrosis (avascular necrosis) of the capitellar ossification centre in young children
- Boys under 10 years, usually the dominant arm - distinct from adolescent OCD
- Whole epiphysis involved with NO loose body formation - this separates it from OCD
- Self-limiting - the capitellum reossifies and remodels with rest alone
- Excellent prognosis - surgery is essentially never required for true Panner disease
- “Age is the single best discriminator: under 10 thinks Panner, teenager thinks OCD
- “Treat with activity restriction - no throwing or weight-bearing on the elbow
- “Loose bodies or a focal unstable fragment mean OCD, not Panner disease
- “Early radiographs can be normal - MRI is the most sensitive early test
A boy younger than 10 years, typically affecting the dominant arm. This young age is the most reliable feature separating Panner disease from osteochondritis dissecans, which affects adolescents in the second decade.
Osteochondrosis (avascular necrosis) of the capitellar ossification centre. The whole epiphysis is involved during a vulnerable period of endochondral ossification, then revascularises and reossifies.
Panner involves the entire epiphysis with no loose bodies; OCD is a focal lesion that can detach and form loose bodies. They are best thought of as a continuum of disordered ossification separated mainly by age.
Self-limiting with an excellent prognosis. Activity restriction allows the capitellum to reossify and remodel. Surgery is essentially never needed for true Panner disease - operative treatment belongs to unstable OCD.
Overview and Epidemiology
Panner disease (capitellar osteochondrosis) was first described by the Danish radiologist Hans Jessen Panner in the 1920s. It is an osteochondrosis - a disturbance of the normal endochondral ossification of an epiphyseal growth centre - affecting the capitellum of the distal humerus. Avascular necrosis of the developing capitellar ossification centre is followed by spontaneous revascularisation, reossification and remodelling, giving the condition its characteristically benign course.
Epidemiology
Panner disease is rare, and most published evidence comes from case reports and small series. It characteristically affects boys younger than 10 years (most commonly around 5 to 10 years of age) and usually involves the dominant arm. It is one of the two recognised lateral compression injuries of the immature elbow, the other being osteochondritis dissecans (OCD) of the capitellum, which affects an older, adolescent age group. Both are seen more often in children exposed to repetitive valgus loading of the elbow, such as throwers and gymnasts, although Panner disease can also occur with no sporting history at all.
Pathophysiology and Anatomy
Relevant Anatomy
The capitellum is the rounded lateral part of the distal humeral articular surface that articulates with the radial head. It develops from a secondary ossification centre that is usually the first to appear at the elbow (around age 1 to 2 years) and ossifies progressively through childhood. Like other epiphyses during active ossification, its blood supply is relatively tenuous, leaving it vulnerable during periods of rapid growth and mechanical loading.
During elbow use, particularly throwing and other valgus-loading activities, the lateral side of the joint (radiocapitellar articulation) is compressed while the medial side is under tension. This lateral compression is the mechanical stress most associated with capitellar osteochondral problems.
Pathophysiology
The accepted mechanism is avascular necrosis (osteochondrosis) of the capitellar ossification centre. A combination of a vulnerable, immature blood supply and repetitive lateral compressive load is thought to disrupt perfusion of the developing centre. The result is ischaemia and necrosis of the whole epiphysis, seen radiographically as fragmentation and sclerosis. Because the entire centre is affected in a child whose growth and remodelling potential is high, the bone subsequently revascularises and reossifies, restoring near-normal architecture - explaining the excellent natural history.
Panner disease and OCD of the capitellum are widely regarded as a continuum of disordered endochondral ossification. In the younger child the whole epiphysis is involved and heals (Panner disease); in the older adolescent a focal segment of subchondral bone and overlying cartilage is affected and may become unstable or detach to form a loose body (OCD). Age at onset largely determines which pattern - and which prognosis - is seen.
Classification
Panner disease itself has no widely used formal classification; the most important clinical "classification" task is to place a capitellar osteochondral lesion on the Panner-to-OCD spectrum and, if it is OCD, to judge lesion stability.
The Clinically Useful Framework
Capitellar osteochondral lesions are best understood as a continuum of disordered ossification rather than two unrelated diseases:
- Panner disease - young child (under 10), entire capitellar epiphysis involved, no fragment separation, self-limiting.
- Osteochondritis dissecans (OCD) - adolescent, focal lesion, potential for fragment instability and loose body formation, variable prognosis.
The single most useful discriminator in the exam and clinic is age at presentation, supported by whether the lesion is diffuse versus focal and whether there is any loose body.
Clinical Presentation
History
The child typically presents with an insidious, dull ache over the lateral aspect of the elbow, sometimes related to throwing or other repetitive elbow activity, but frequently with no clear injury at all. Parents may notice the child holding the arm slightly bent or being reluctant to fully straighten it. Pain is usually mild and activity-related and the child is systemically well - fever or malaise should prompt consideration of infection instead.
Examination
There may be a small effusion or mild swelling over the lateral elbow, often subtle. The child frequently holds the elbow in slight flexion.
Tenderness over the radiocapitellar joint (lateral elbow) is the key local sign.
A mild loss of full extension (a flexion contracture of a few degrees) is characteristic. Flexion is usually preserved. Significant mechanical locking or catching is NOT typical of Panner disease - if present, it suggests a loose body and therefore OCD.
Pain may be reproduced by activities that load the radiocapitellar joint, consistent with the lateral compression mechanism.
Normal. Any neurovascular deficit points away from Panner disease.
Investigations and Diagnosis
Radiographic Findings
AP and lateral radiographs of the elbow are the first-line investigation; comparison with the unaffected side can help in a young child with immature ossification.
Typical findings include:
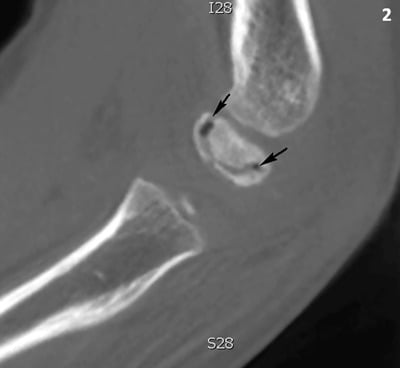
- Fragmentation and irregular ossification of the capitellar centre, which nonetheless retains its overall shape
- Sclerosis (increased density) of the affected centre
- A small joint effusion and slightly irregular articular contour
- Importantly, NO loose bodies and no large focal defect - their presence suggests OCD instead
Early radiographs can be entirely normal. A normal radiograph in a young child with a convincing clinical picture does not exclude Panner disease and should prompt MRI if symptoms persist. Over months, follow-up films show progressive reconstitution of a near-normal capitellum.
Key Differentials
1. Osteochondritis dissecans (OCD) of the capitellum - the single most important differential. OCD occurs in adolescents, is a focal lesion, and may produce loose bodies, locking and a poorer prognosis. Age, focal versus diffuse involvement and the presence of a loose body are the discriminators.
2. Little League elbow (medial epicondyle apophysitis/avulsion) - a medial overload problem of the throwing child, in contrast to the lateral pain of Panner disease.
3. Occult fracture - radial neck or lateral condyle fracture after trauma. History of injury and fracture line distinguish it.
4. Septic arthritis or osteomyelitis - the child is systemically unwell with fever and raised inflammatory markers; effusion is tense and the joint is irritable in all directions.
5. Normal ossification variant - irregular, multicentric capitellar ossification can be a normal finding in young children; clinical correlation (pain, tenderness, restricted extension) is essential before labelling it disease.

Management
Non-Operative Management
True Panner disease is managed conservatively - there is no role for surgery. The aim is symptom relief and protection of the capitellum while it reossifies.
Core measures:
1. Activity restriction - stop throwing, gymnastics and other elbow-loading activities. This is the single most important intervention.
2. Relative rest and analgesia - short-term rest, ice after activity and judicious NSAIDs for comfort.
3. Temporary immobilisation if painful - a sling or a short period of splinting/casting can settle an acutely painful elbow, followed by early gentle remobilisation to avoid stiffness.
4. Graded return - reintroduce range-of-motion and then loading only once symptoms have settled and reossification is under way, with a gradual return to sport.
Expected course: symptoms typically settle over weeks to a few months, with radiographic reconstitution of the capitellum over many months. The radiographic appearance lags behind clinical recovery.
Reconsider the diagnosis and look for osteochondritis dissecans if the child is adolescent, if there is mechanical locking or catching, or if imaging shows a focal unstable fragment or a loose body. These features take the lesion off the self-limiting Panner pathway and into the OCD pathway, where surgery may be required. Treating an unstable OCD lesion as benign Panner disease risks progressive joint damage.
Complications and Prognosis
Panner disease is fundamentally a benign, self-limiting condition, and complications attributable to the disease itself are uncommon. The main hazards are diagnostic and iatrogenic.
- Excellent natural history. With activity restriction, the capitellum reossifies and remodels, and most children regain a normal, pain-free elbow with full or near-full motion.
- Residual minor changes. A small number may have minor radiographic flattening or a slight residual loss of terminal extension, usually without functional consequence.
- Misdiagnosis as (or progression to) OCD. The most important pitfall is failing to recognise an osteochondritis dissecans lesion - especially in an older child - which can become unstable, form loose bodies, cause locking and lead to early radiocapitellar degeneration if mismanaged.
- Iatrogenic harm from overtreatment. Unnecessary surgery or prolonged rigid immobilisation (with resulting elbow stiffness) in a child who has true, self-limiting Panner disease are avoidable harms.
There is no recognised direct association between true Panner disease and later osteoarthritis; the long-term risk lies with unrecognised or unstable OCD lesions, not with the benign childhood entity.
Clinical Relevance and Exam Focus
For the FRACS and FRCS examiner, Panner disease is a discriminator topic: a candidate who simply says "osteochondrosis of the capitellum, treat with rest" has done well, but the examiner is really testing whether you can confidently separate Panner disease from osteochondritis dissecans of the capitellum and explain why that distinction changes management. The high-value points are: the young age and dominant-arm pattern, the lateral compression mechanism, the whole-epiphysis involvement with no loose body, the role of MRI when radiographs are normal, and the principle that true Panner disease never needs surgery whereas unstable OCD might. Framing the two as a continuum of disordered endochondral ossification separated largely by age signals genuine understanding.
Guidelines, Registries & Global Practice
Global Epidemiology
Panner disease is a rare paediatric osteochondrosis reported worldwide with a remarkably consistent profile across published series: boys younger than 10 years, the dominant arm, and a benign self-limiting course. Because it is uncommon and benign, the evidence base is built almost entirely from case reports and small series rather than registries or trials, and there is no arthroplasty, trauma or implant registry that tracks it. Reported associations with throwing and gymnastic activities reflect the lateral compression mechanism common to immature-elbow osteochondral lesions.
Guideline and Society Positions
- Position on Panner disease
- Clinical and radiographic diagnosis on the Panner-to-OCD spectrum; conservative management with activity restriction; no operative role for true Panner disease
- Position on Panner disease
- Managed conservatively within paediatric elbow and "the painful elbow in a child" pathways; image to exclude OCD and other causes, and reassure regarding natural history
- Position on Panner disease
- Same conservative consensus; MRI reserved for normal radiographs with persistent symptoms or to assess OCD stability
- Position on Panner disease
- Self-limiting osteochondrosis of the capitellum; treat the cause of lateral compression, restrict activity, and distinguish from OCD
No society publishes a dedicated Panner disease guideline because management is uncontroversial and uniformly non-operative; recommendations are extrapolated from the broader paediatric elbow and osteochondrosis literature.
High- vs Limited-Resource Practice
In well-resourced settings, radiographs confirm the diagnosis and MRI is available for normal-film cases or to assess OCD fragment stability. In limited-resource settings the diagnosis remains clinical and radiographic, and activity restriction with simple analgesia achieves the same excellent outcome without advanced imaging. The universal teaching point is identical everywhere: recognise the entity, separate it from osteochondritis dissecans, avoid unnecessary surgery, and reassure the family.
Why the Capitellum Is Vulnerable: the Blood Supply
The topic repeatedly says the capitellum has a 'tenuous, immature blood supply' but never explains why - which is the anatomical basis of the whole disease.
- End-arteries entering posteriorly. The capitellar ossification centre is supplied by only one or two end-arteries (from the radial and interosseous recurrent vessels) that enter the capitellum posteriorly and cross the physis to reach the epiphysis.
- A watershed with no back-up. These are isolated end-arteries with little or no anastomotic collateral, so the ossifying centre has no alternative supply if their flow is interrupted.
- Why it matters. This watershed pattern is what makes the capitellum prone to ischaemia and avascular necrosis when repetitive lateral (radiocapitellar) compression disrupts perfusion during the ossification window - the shared anatomical basis of both Panner disease and capitellar osteochondritis dissecans.
Q: Why is the capitellar ossification centre prone to avascular necrosis?
A: It is supplied by only one or two end-arteries (from the radial/interosseous recurrent vessels) that enter posteriorly and cross the physis, with little or no anastomotic collateral - a watershed territory. When repetitive lateral radiocapitellar compression disrupts perfusion during the ossification window, the centre has no back-up supply, giving ischaemia and AVN. This end-artery anatomy underlies both Panner disease (young child) and capitellar OCD (adolescent).
The Normal-Variant Trap: Irregular Capitellar Ossification
The topic twice raises 'normal, irregular, multicentric capitellar ossification' as a differential and a controversy, but never explains the trap.
- The normal variant. The capitellum normally ossifies from a single centre from about age 1, but it can ossify irregularly or from multiple (multicentric) foci, giving a fragmented, notched or mottled appearance that is a normal finding in young children.
- The mimic. This normal irregular ossification can look radiographically identical to the fragmentation and sclerosis of Panner disease.
- So the diagnosis is clinical. Panner disease equals the radiographic changes plus localised radiocapitellar tenderness, a small effusion, a slight loss of extension and activity-related lateral pain. An asymptomatic irregular capitellum (an incidental finding, or on the pain-free contralateral side) is a normal variant, not disease - do not label it Panner.
Q: Why can a radiograph alone not diagnose Panner disease?
A: The capitellum normally ossifies from a single centre (about age 1) but can ossify irregularly / multicentrically - a fragmented, notched normal variant in young children that looks radiographically identical to Panner's fragmentation and sclerosis. So Panner disease equals the radiographic changes plus localised radiocapitellar tenderness, a small effusion, a slight loss of extension and activity-related lateral pain. An asymptomatic irregular capitellum (incidental, or the pain-free contralateral side) is a normal variant, not Panner.
Controversies and Areas of Uncertainty
- Aetiology is uncertain. The cause of osteochondrosis in general, and Panner disease specifically, remains unproven; genetic, hormonal, mechanical, repetitive-trauma and vascular factors have all been proposed and likely interact during the vulnerable ossification window.
- Panner versus OCD - one disease or two? Most authorities regard them as a continuum of disordered endochondral ossification separated mainly by age, but the exact boundary is blurred and some lesions are difficult to classify, which directly affects whether surgery is considered.
- Disease versus normal variant. Irregular, multicentric capitellar ossification can be a normal radiographic finding in young children, and minor subchondral surface irregularity on ultrasound may reflect normal development rather than disease - so imaging must always be correlated with clinical findings.
- Role and timing of MRI. MRI is the most sensitive early test and is valuable when radiographs are normal or to assess OCD stability, but it is not required for every typical case and may involve sedation in very young children.
- Naming trap. Do not conflate true childhood Panner disease with adolescent OCD - misapplying the benign label to an unstable OCD lesion risks under-treating a condition that can cause loose bodies and joint damage.
At a Glance
Panner disease is an osteochondrosis (avascular necrosis) of the capitellum - the lateral ossification centre of the distal humerus - occurring in young children, classically boys under 10 years of age, usually in the dominant arm. It is one of the two main lateral compression injuries of the immature elbow, the other being osteochondritis dissecans (OCD) of the capitellum. The child presents with dull lateral elbow pain, mild swelling and a small loss of extension, often without a clear injury. Early radiographs may be normal; later they show fragmentation, sclerosis and irregular ossification of the whole capitellar centre, and MRI shows capitellar bone marrow oedema before radiographs change. The defining feature is that the entire epiphysis is involved and there are no loose bodies - this separates it from OCD, where a focal fragment can detach. Treatment is conservative: rest from throwing and elbow loading, with the capitellum reossifying and remodelling over months. The prognosis is excellent and surgery is essentially never required for true Panner disease.
- Panner Disease
- Under 10 years (first decade)
- OCD of Capitellum
- Adolescent (second decade)
- Panner Disease
- Whole capitellar epiphysis
- OCD of Capitellum
- Focal area of capitellum
- Panner Disease
- No
- OCD of Capitellum
- Possible (if fragment detaches)
- Panner Disease
- Absent
- OCD of Capitellum
- May be present with loose body
- Panner Disease
- Excellent, self-limiting
- OCD of Capitellum
- Variable, depends on stability
- Panner Disease
- Essentially never
- OCD of Capitellum
- May be needed for unstable lesions
PANNERPanner Disease Key Features
Hook:PANNER - Paediatric boy, Avascular capitellum, No loose bodies, Naturally heals, Elbow lateral pain, Rest cures it.
TENPanner vs OCD - The Age Rule
Hook:Remember TEN: the magic age is around ten - younger children get whole-epiphysis Panner disease with no loose bodies; older children get focal OCD that can detach.
POLELateral Elbow Pain in a Child - Differentials
Hook:POLE - think Panner/OCD, Occult fracture, Little League elbow and Effusion when a child has elbow pain.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 8-year-old boy presents with a few weeks of dull pain over the outer aspect of his dominant elbow and a slight inability to fully straighten it. There is a small effusion and tenderness over the radiocapitellar joint. He is otherwise well. What is your diagnosis and how would you manage him?”
“A 14-year-old competitive baseball pitcher has lateral elbow pain and intermittent catching. Radiographs show a focal lucent lesion of the capitellum with a separate ossific fragment. The referring doctor has labelled this Panner disease. What are your thoughts?”
“A 7-year-old boy has three weeks of lateral elbow pain and a small loss of extension. His elbow radiographs are reported as normal. The family wants to know why he still has pain and what you will do next. How do you proceed?”
Definition
- Osteochondrosis (AVN) of the capitellum
- Lateral ossification centre of distal humerus
- A lateral compression injury of the elbow
- Whole epiphysis involved
Demographics
- Boys under 10 years (first decade)
- Usually the dominant arm
- Rare condition
- Linked to throwing and gymnastics
Clinical Features
- Dull lateral (radiocapitellar) elbow pain
- Small effusion and mild swelling
- Slight loss of full extension
- No mechanical locking, systemically well
Imaging
- Radiographs: fragmentation and sclerosis, shape kept
- NO loose bodies (key point)
- Early films may be normal
- MRI most sensitive - diffuse capitellar marrow oedema
Panner vs OCD
- Panner = under 10, whole epiphysis, no loose body
- OCD = adolescent, focal lesion, may form loose bodies
- Continuum of disordered ossification
- Age is the best discriminator
Treatment
- CONSERVATIVE ONLY
- Activity restriction from elbow loading
- Analgesia, short immobilisation if painful
- NO surgery for true Panner disease
Prognosis
- Self-limiting, excellent outcome
- Capitellum reossifies and remodels
- Radiographic healing lags symptoms
- Main risk is misdiagnosing unstable OCD
Evidence Base
Lateral Compression Injuries: Panner Disease and OCD of the Capitellum (Key Review)
- Panner disease is an osteochondrosis of the capitellum, a rare disorder usually affecting the dominant arm in children younger than 10 years
- Symptomatic management - reduction of stressful elbow activities - is usually sufficient to allow resolution
- Healing takes a prolonged period but most patients show excellent long-term results
- OCD of the capitellum occurs in adolescents and is associated with loose body formation; Panner disease and OCD likely represent a continuum of disordered endochondral ossification with presentation and prognosis depending mainly on age at onset
Apophysitis and Osteochondrosis: Common Causes of Pain in Growing Bones
- Osteochondrosis refers to degenerative changes in the epiphyseal ossification centres of growing bones, with the capitellum being the site of Panner disease
- The aetiology of osteochondrosis is uncertain, with genetic, hormonal, mechanical, repetitive-trauma and vascular factors proposed
- Radiographs may be normal initially; MRI is more sensitive to early changes
- Osteochondrosis generally resolves with relative rest, and surgery is rarely needed