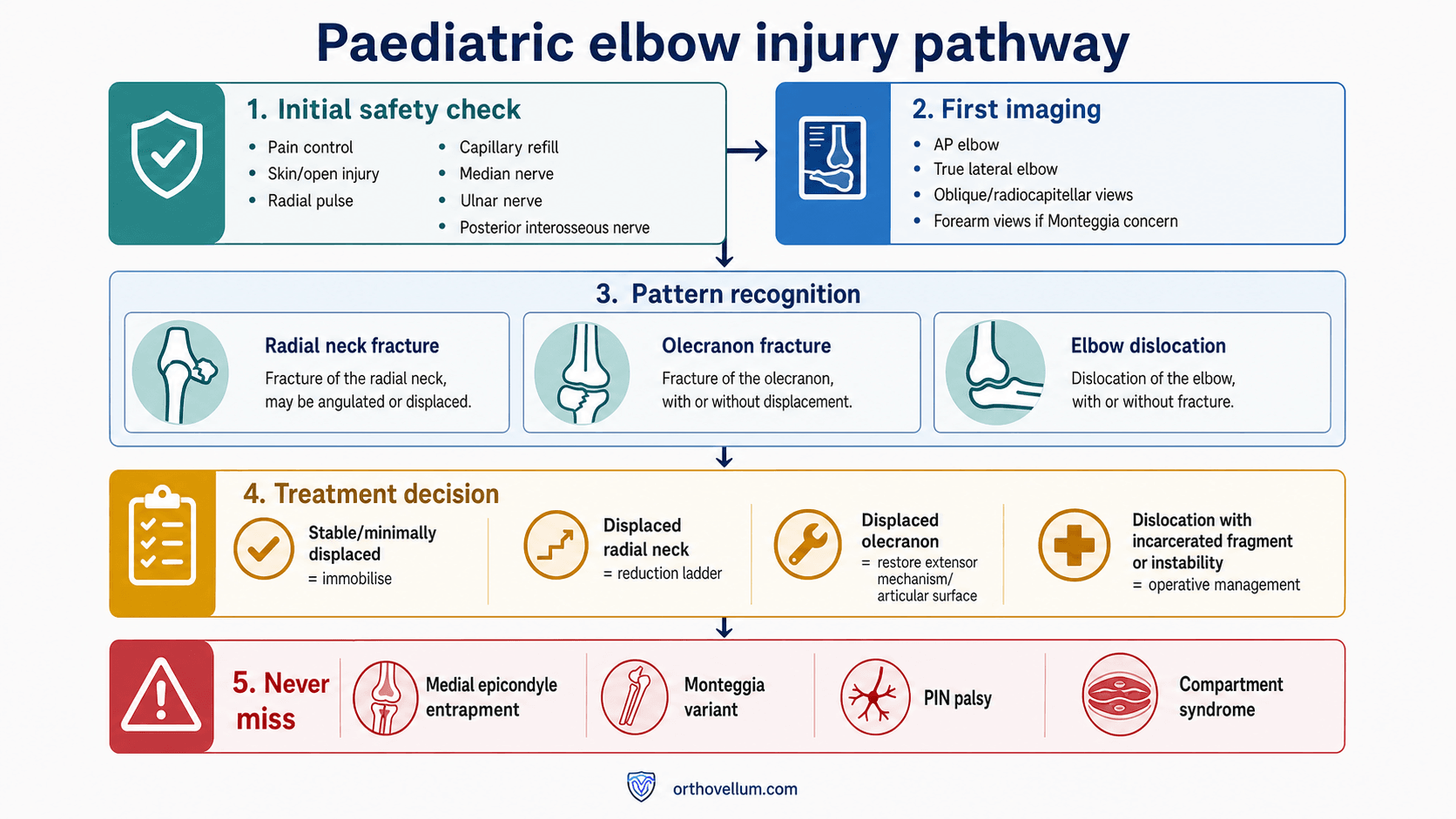
Radial neck | olecranon | elbow dislocation | medial epicondyle | Monteggia check
- Do the neurovascular exam before and after reduction. Document median, ulnar and posterior interosseous nerve function.
- A reduced elbow is not a finished assessment. Recheck the medial epicondyle, radiocapitellar line and ulna after reduction.
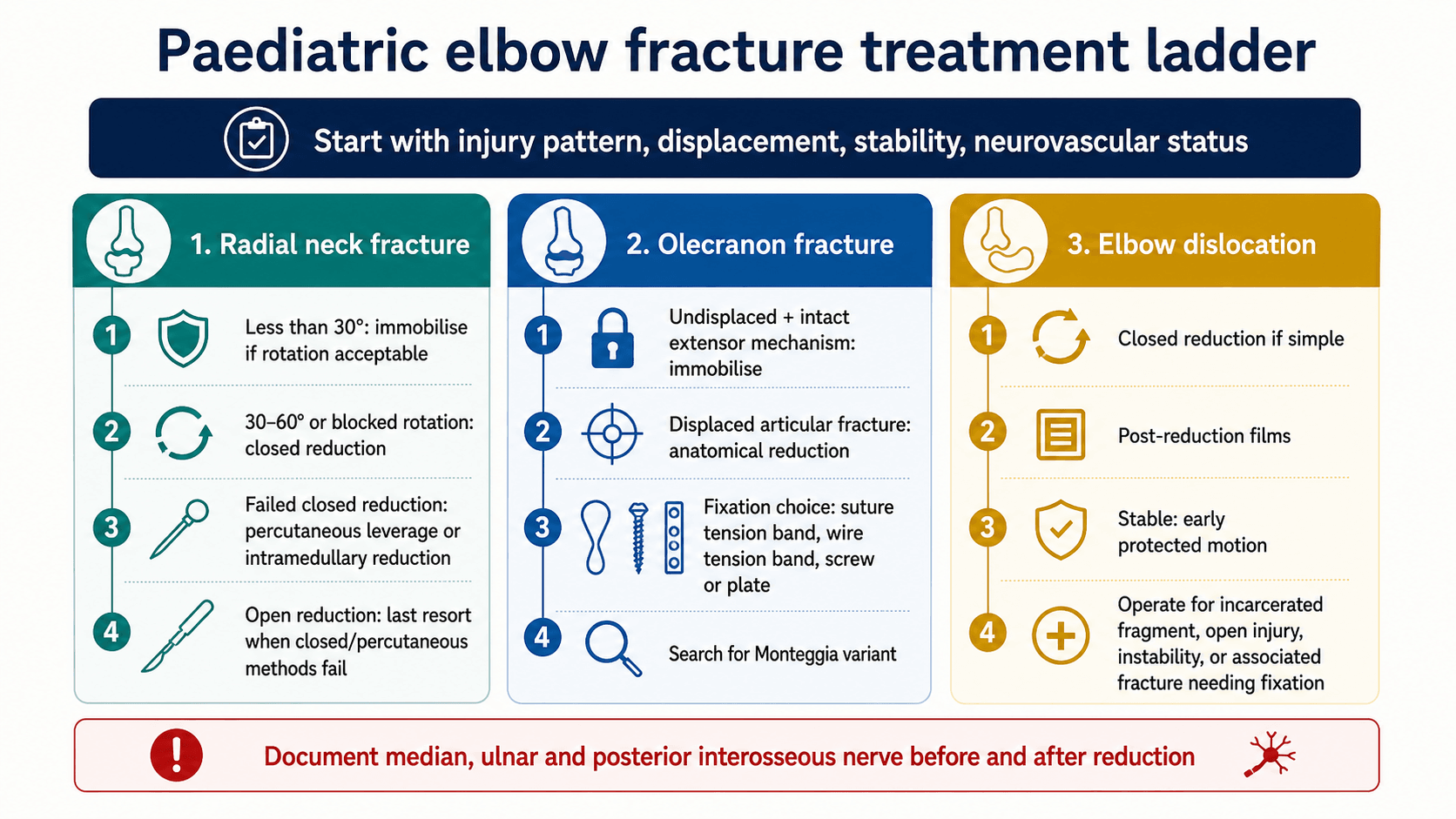
- Radial neck open reduction is a last resort. It is associated with higher stiffness and vascular complications than closed or percutaneous strategies.
- Olecranon fractures need an extensor mechanism decision. Undisplaced plus intact extension is different from displaced articular disruption.
- Look for Monteggia variants. A radial neck injury with ulna deformity or radiocapitellar malalignment is not an isolated radial neck fracture.
- “Finger MCP and thumb extension test posterior interosseous nerve function.
- “A missing medial epicondyle after dislocation may be trapped in the joint.
- “Radial neck management depends on angulation, translation, rotation block, age, associated injury and success of closed reduction.
- “Olecranon fixation choice is driven by fracture pattern, comminution, skeletal maturity and hardware prominence risk.
Do not reduce a paediatric elbow dislocation, see a congruent joint, and stop. The post-reduction film must show the medial epicondyle in the correct place, the radiocapitellar line through the capitellum, a satisfactory ulnohumeral joint, and no missed radial neck, olecranon, lateral condyle or proximal ulna injury.
- What to Check
- Radial pulse, capillary refill, hand temperature, median nerve, ulnar nerve and posterior interosseous nerve.
- Management Implication
- Vascular compromise, nerve deficit or compartment concern escalates urgency.
- What to Check
- Radiocapitellar line, ulna alignment, medial epicondyle position, olecranon cortex and lateral condyle.
- Management Implication
- Associated injuries change treatment from simple immobilisation to reduction or fixation.
- What to Check
- Angulation, translation, rotation block and age.
- Management Implication
- Acceptable injuries are immobilised; displaced or blocked injuries enter the reduction ladder.
- What to Check
- Active extension, articular displacement and comminution.
- Management Implication
- Displaced intra-articular or extensor-disrupted fractures need anatomical reduction and fixation.
- What to Check
- Post-reduction congruity, stress stability and incarcerated fragment.
- Management Implication
- Stable simple dislocations can mobilise early; unstable or incarcerated patterns need surgery.
SAFEFirst assessment | RINGRadiograph read | LADDERReduction logic |
|---|---|---|
S Skin Open injury, puckering, swelling and threatened skin. | R Radiocapitellar line Must pass through capitellum on every view. | L Less displaced Immobilise if alignment and rotation are acceptable. |
A Artery Pulse, capillary refill, colour and temperature. | I Internal epicondyle Find the medial epicondyle after dislocation. | A Attempt closed Closed reduction first for displaced radial neck and elbow dislocation. |
F Function Median, ulnar and posterior interosseous nerve function. | N Neck and olecranon Measure radial neck and inspect olecranon joint surface. | D Direct percutaneous help Leverage or joystick if closed reduction fails. |
E Elbow films True AP/lateral, associated injury search and post-reduction films. | G Gross ulna alignment Search for Monteggia variant or proximal ulna plastic deformity. | D Drive intramedullary Intramedullary reduction/fixation for selected radial neck fractures. |
E Expose last Open reduction only when lesser methods fail or a fragment is incarcerated. | ||
R Reassess Repeat nerve check and radiographs after every reduction. | ||
SAFE is the order before any reduction. | RING prevents isolated-fragment thinking. | Use a ladder before opening the radial neck. |
Overview/Epidemiology
These injuries sit close together anatomically and clinically. A child can present with a radial neck fracture, olecranon fracture or elbow dislocation, but the surgeon must actively search for the combined pattern. A radial neck fracture can accompany elbow dislocation or Monteggia injury. An olecranon fracture can be part of proximal ulna instability. A reduced elbow dislocation can hide an incarcerated medial epicondyle or nerve entrapment.
Common mechanisms
- Likely Pattern
- Radial neck fracture from compression against the capitellum.
- What It Should Trigger
- Measure radial neck angulation and check forearm rotation.
- Likely Pattern
- Elbow dislocation with medial epicondyle avulsion, capsuloligamentous injury or nerve traction.
- What It Should Trigger
- Find the medial epicondyle and document median/ulnar/PIN function.
- Likely Pattern
- Olecranon fracture, often with swelling over the extensor surface.
- What It Should Trigger
- Assess active extension and articular displacement.
- Likely Pattern
- Olecranon apophyseal or proximal ulna avulsion pattern.
- What It Should Trigger
- Treat displacement and extensor mechanism status as decision points.
- Likely Pattern
- Biepicondylar fracture-dislocation, radial neck plus dislocation, proximal ulna fracture, or open injury.
- What It Should Trigger
- Do not call it isolated until the whole elbow and forearm are imaged.
Think valgus-axial load, angulation, displacement, rotation block and posterior interosseous nerve risk.
Think articular surface, extensor mechanism, proximal ulna alignment and Monteggia variant.
Think reduction, post-reduction films, medial epicondyle, nerve injury and stability.
Surgically Relevant Anatomy
Radial neck and proximal radius
The radial head ossifies in childhood and the radial neck behaves differently from the adult radial head. The periosteal sleeve and physis contribute to remodelling, but severe angulation, translation and mechanical block to rotation are poorly tolerated. The posterior interosseous nerve passes near the proximal radius as it enters the supinator, so nerve function must be documented before and after injury manipulation.
Olecranon and proximal ulna
The olecranon is the triceps insertion and part of the greater sigmoid notch. Treatment depends on whether the articular surface and extensor mechanism remain functional. In a child, the olecranon apophysis and proximal ulna alignment can make the injury look deceptively small, but any proximal ulna deformity should raise concern for radiocapitellar instability.
Elbow dislocation and medial epicondyle
In children, the medial collateral ligament is attached to the medial epicondylar apophysis. A dislocation can therefore avulse the medial epicondyle rather than rupture the ligament midsubstance. During spontaneous or closed reduction, the fragment can become trapped in the ulnohumeral joint. The ulnar nerve runs posterior to the medial epicondyle and the median nerve can rarely be entrapped after dislocation.
Record median nerve sensation and thenar function, ulnar nerve sensation and intrinsic function, and posterior interosseous nerve motor function. A posterior interosseous nerve palsy is tested by finger MCP extension and thumb extension, not by wrist extension alone.
Pathophysiology
The common theme is failure of the paediatric elbow ring. The visible fracture may be only one part of the instability pattern.
- Pathophysiology
- Valgus and axial load compress the radial head against the capitellum. The cartilaginous head and physis make displacement harder to appreciate on plain films.
- Clinical Consequence
- Painful rotation and a mechanical block matter more than the X-ray label alone.
- Pathophysiology
- The triceps pulls the proximal fragment while the olecranon forms the articular notch of the ulnohumeral joint.
- Clinical Consequence
- Displacement threatens both the joint surface and active elbow extension.
- Pathophysiology
- The ulna and radius dislocate relative to the distal humerus, often through posterolateral instability. In children, the medial epicondyle may fail before the ligament midsubstance.
- Clinical Consequence
- A reduced joint can still hide an incarcerated epicondyle or nerve entrapment.
- Pathophysiology
- Proximal ulna deformity changes the radial head relationship with the capitellum.
- Clinical Consequence
- Restoring only the radial neck or only the dislocation misses the driver of radiocapitellar malalignment.
The treatment logic follows the biology. Young children remodel some angulation, but remodelling does not reliably correct severe translation, blocked forearm rotation, joint incongruity, incarcerated fragments or extensor mechanism failure. These are the findings that move treatment from observation to reduction or fixation.
Classification
Classification should help communication and treatment, not replace clinical judgement.
- Acceptable or minimally displaced: low angulation, little translation, no blocked rotation and no associated instability.
- Moderately displaced: angulation around the common reduction threshold, translation, or clinically important loss of rotation.
- Severely displaced or irreducible: marked angulation, major translation, complete displacement, soft-tissue interposition or failed closed reduction.
- Associated injury pattern: elbow dislocation, olecranon/proximal ulna injury or Monteggia variant changes the plan.
The descriptive groups above are practical, but examiners expect you to name a formal radial neck classification, which the topic otherwise omits:
- Judet classification (angulation-based): Type I undisplaced; Type II angulation under 30 degrees; Type III angulation about 30-60 degrees; Type IV angulation over 60 degrees (up to complete displacement, sometimes subdivided IVa/IVb). Higher Judet types are progressively harder to reduce closed and more likely to need percutaneous or intramedullary assistance.
- O'Brien classification (a simpler angulation tier): Type I under 30 degrees, Type II 30-60 degrees, Type III over 60 degrees - a commonly quoted shorthand that maps onto the same treatment ladder.
- How it links to treatment: Type I and many low Type II injuries are immobilised; the common reduction threshold sits around 30 degrees of angulation (modified by age, translation and any block to rotation); high Judet/O'Brien grades enter the closed-then-percutaneous-then-intramedullary ladder, with open reduction last.
Exam point: classify a paediatric radial neck fracture by the Judet (I-IV) or O'Brien (I-III) angulation grade, and tie the grade to the reduction ladder - reduce above roughly 30 degrees of angulation (or any rotational block), escalating from closed to percutaneous/intramedullary before open reduction.
Clinical Assessment
History
Ask enough to identify the injury pattern and urgency:
- Mechanism: fall, valgus load, direct posterior blow, dislocation event or high-energy trauma.
- Time from injury and whether the elbow was reduced before assessment.
- Pain location: radial head/neck, olecranon, medial epicondyle or diffuse elbow pain.
- Mechanical block: inability to pronate or supinate suggests radial neck displacement or intra-articular block.
- Neurological symptoms: numbness, paraesthesia, weakness, clawing, inability to extend fingers or thumb.
- Vascular symptoms: cold hand, colour change, severe swelling or escalating analgesic requirement.
- Previous elbow injury, hyperlaxity, sporting demand and hand dominance.
Examination sequence
- How To Do It
- Inspect from front, side and posterior elbow. Note swelling, deformity, bruising, skin puckering, wounds and carrying angle.
- What A Positive Finding Means
- Gross deformity suggests dislocation or displaced fracture; posterior swelling localises to olecranon; threatened skin or open injury escalates urgency.
- How To Do It
- Palpate distal humerus, medial epicondyle, lateral condyle, radial head/neck while gently rotating forearm, olecranon, proximal ulna and wrist.
- What A Positive Finding Means
- Focal radial-neck tenderness and painful rotation support radial neck injury; medial tenderness after dislocation suggests epicondyle avulsion; ulna tenderness raises Monteggia concern.
- How To Do It
- If safe, assess active flexion-extension and pronation-supination; do not force movement in a displaced injury.
- What A Positive Finding Means
- Blocked rotation suggests radial neck displacement, incarcerated fragment or radiocapitellar problem.
- How To Do It
- Ask the child to actively extend the elbow against gravity if pain and fracture pattern allow.
- What A Positive Finding Means
- Loss of active extension with olecranon fracture suggests extensor disruption and supports fixation.
- How To Do It
- After reduction, reassess congruity clinically and radiographically; avoid aggressive stress testing in an awake child.
- What A Positive Finding Means
- Persistent instability or blocked motion suggests complex dislocation, incarcerated fragment or associated fracture.
Nerve and vessel tests
- How To Test
- Radial pulse, capillary refill, hand colour, temperature and pulse oximetry if uncertain.
- Why It Matters
- A cold, pale or poorly perfused hand needs urgent escalation.
- How To Test
- Light touch to index finger pulp; thumb opposition or thenar activation if cooperative.
- Why It Matters
- Median neuropathy may occur with dislocation; persistent or delayed symptoms require urgent reassessment.
- How To Test
- Ask for the OK sign: thumb IP flexion and index DIP flexion.
- Why It Matters
- AIN deficit is a motor median-nerve branch problem; document separately from sensation.
- How To Test
- Small-finger sensation, finger abduction, crossing fingers or first dorsal interosseous activation.
- Why It Matters
- At risk with medial epicondyle avulsion, fixation and dislocation.
- How To Test
- Finger MCP extension and thumb extension with wrist supported.
- Why It Matters
- PIN palsy can accompany radial neck injury or be iatrogenic during percutaneous/open procedures.
Differential diagnosis
The painful, swollen paediatric elbow has several overlapping causes. The job is to separate them with a systematic radiograph read rather than a single glance, because the management differs sharply.
- Discriminating Features
- Lateral elbow tenderness, painful or blocked forearm rotation, valgus mechanism.
- How to Confirm
- AP/lateral plus a view at maximum deformity; measure angulation and translation.
- Why It Matters
- Drives the closed-percutaneous-open reduction ladder.
- Discriminating Features
- Posterior swelling and tenderness, possible loss of active extension.
- How to Confirm
- True lateral showing the trochlear notch; CT if articular surface unclear.
- Why It Matters
- Articular step or extensor failure mandates fixation.
- Discriminating Features
- Gross deformity, fixed posture, rapid relief after reduction.
- How to Confirm
- Pre- and post-reduction AP/lateral confirming congruity.
- Why It Matters
- Stable reductions mobilise early; instability needs more.
- Discriminating Features
- Medial tenderness, ulnar symptoms, absent medial epicondyle for age.
- How to Confirm
- Confirm the epicondyle is in position using CRITOE; CT or comparison films if doubtful.
- Why It Matters
- An incarcerated fragment is an absolute operative indication.
- Discriminating Features
- Ulna deformity or plastic bowing with a malaligned radiocapitellar line.
- How to Confirm
- Image the whole forearm; trace the radiocapitellar line on every view.
- Why It Matters
- Restoring the ulna, not the radial head alone, is the key step.
- Discriminating Features
- Distal humeral tenderness, gross swelling, high neurovascular risk.
- How to Confirm
- AP/lateral assessing the anterior humeral line.
- Why It Matters
- A different pathway; AIN and brachial artery are the priority.
- Discriminating Features
- Lateral tenderness, subtle metaphyseal fleck, late displacement risk.
- How to Confirm
- Internal-oblique view; consider CT or short-interval films.
- Why It Matters
- Articular fracture prone to non-union if displacement is missed.
- Discriminating Features
- Toddler, axial-traction history, arm held pronated, no swelling, normal films.
- How to Confirm
- Clinical diagnosis; films are normal.
- Why It Matters
- Treated by simple reduction manoeuvre, never surgery.
Investigations
What to request
Order imaging that answers the surgeon's questions, not just "elbow X-ray":
- AP and true lateral elbow radiographs: mandatory first-line views.
- Radiocapitellar or oblique view: helpful if radial neck alignment or capitellum relationship is unclear.
- Forearm AP and lateral including wrist and elbow: request when there is ulna pain, deformity, plastic bowing or any concern for Monteggia variant.
- Post-reduction AP and lateral radiographs: mandatory after elbow dislocation reduction.
- Comparison elbow radiographs: useful when ossification centres make medial epicondyle or trochlear interpretation difficult.
- CT: use for complex fracture-dislocation, articular olecranon fracture planning, incarcerated fragment uncertainty or surgical planning.
- MRI or ultrasound for nerve entrapment: not routine, but useful when neurological symptoms persist or median nerve entrapment is suspected.
How to read the films
- How To Assess
- Draw down the centre of the radial shaft and neck on AP and lateral views; it should pass through the capitellum.
- Treatment Meaning
- Failure suggests radial head dislocation, Monteggia pattern or inadequate reduction.
- How To Assess
- Measure the angle between the radial shaft axis and the radial head/neck axis on the view showing maximum deformity.
- Treatment Meaning
- Less displaced injuries may be immobilised; increasing angulation or blocked rotation pushes toward reduction.
- How To Assess
- Assess percentage displacement and head-neck contact.
- Treatment Meaning
- Translation plus angulation predicts reduction difficulty and may require percutaneous or intramedullary assistance.
- How To Assess
- Inspect the greater sigmoid notch on true lateral and AP; CT if the joint line is unclear.
- Treatment Meaning
- Displaced intra-articular fractures need anatomical reduction.
- How To Assess
- After dislocation, confirm the medial epicondyle is visible in its normal position for age.
- Treatment Meaning
- Absent or intra-articular fragment suggests entrapment and operative extraction/fixation.
- How To Assess
- Look for proximal ulna fracture, plastic deformation or bowing; image the forearm if uncertain.
- Treatment Meaning
- Monteggia variants need restoration of ulna alignment and radiocapitellar reduction.
If the child is old enough for the medial epicondyle to be visible and it is missing after a dislocation, search the joint. A trapped medial epicondyle can mimic another ossification centre and should not be dismissed as normal development.
The topic invokes CRITOE several times but never states it - and the sequence is exactly what makes the entrapment call:
- The order of ossification (CRITOE): Capitellum, Radial head, Internal (medial) epicondyle, Trochlea, Olecranon, External (lateral) epicondyle - appearing at roughly ages 1, 3, 5, 7, 9, 11 years (a useful approximation; girls slightly earlier than boys). The order is far more reliable than the exact ages.
- The decisive rule - the medial epicondyle ossifies BEFORE the trochlea. So if you can see an ossific fragment in the region of the trochlea but you cannot identify a separate medial (internal) epicondyle, the "trochlear" ossification centre cannot have appeared yet in isolation - the fragment you are seeing is the displaced/entrapped medial epicondyle sitting in the joint. A trochlear ossification centre should never be present without a medial epicondyle already being present.
- Practical use after a dislocation: run CRITOE on the film; an absent medial epicondyle for age, or an extra fragment in the joint line, means search for and extract an incarcerated medial epicondyle - use comparison films or CT if unsure.
Exam point: recite CRITOE (1-3-5-7-9-11), and apply the rule that the medial epicondyle always ossifies before the trochlea - a "trochlear" fragment with no visible medial epicondyle is an entrapped medial epicondyle until proven otherwise.
Treatment Thresholds
- Typical Features
- Low angulation, minimal translation, painless or acceptable rotation and no associated instability.
- Treatment Direction
- Above-elbow immobilisation, early review and motion when safe.
- Typical Features
- About 30-60 degrees angulation, translation or blocked rotation.
- Treatment Direction
- Closed reduction first; accept reduction only if motion and alignment are satisfactory.
- Typical Features
- Marked angulation, major translation, mechanical block or unsuccessful closed manoeuvre.
- Treatment Direction
- Percutaneous leverage, joystick technique or intramedullary reduction/fixation.
- Typical Features
- Soft-tissue interposition, complete displacement, delayed presentation or failed minimally invasive methods.
- Treatment Direction
- Open reduction only when required; preserve soft tissues and warn about stiffness/AVN/synostosis.
Management
- Action
- Provide pain control and protect the limb.
- Reason
- A calm, supported child is easier and safer to assess.
- Action
- Escalate open injury, threatened skin, vascular compromise or compartment concern.
- Reason
- These override routine fracture pathways.
- Action
- Document median, ulnar and posterior interosseous nerve function before reduction.
- Reason
- New deficit after manipulation must be recognised.
- Action
- Reduce a dislocated elbow promptly if there is no contraindication.
- Reason
- A congruent joint protects soft tissues and nerves.
- Action
- Repeat neurovascular examination and AP/lateral radiographs.
- Reason
- Find medial epicondyle entrapment, radial neck injury, olecranon injury and radiocapitellar incongruity.
Complications and Failure Management
- Where It Occurs
- All paediatric elbow trauma, especially delayed or open radial neck reduction.
- Prevention and Management
- Avoid unnecessary prolonged immobilisation; start supervised motion when stable; treat established stiffness with therapy and selective surgery.
- Where It Occurs
- Radial neck malunion, radioulnar synostosis or over-manipulation.
- Prevention and Management
- Restore radial neck alignment, avoid repeated soft-tissue trauma, monitor rotation early.
- Where It Occurs
- Severe radial neck displacement or open reduction.
- Prevention and Management
- Preserve periosteal blood supply; reserve open reduction for irreducible cases.
- Where It Occurs
- Severe proximal radius injury or open surgery.
- Prevention and Management
- Limit soft-tissue stripping and repeated attempts; manage established synostosis only when mature and functionally limiting.
- Where It Occurs
- Post-reduction elbow dislocation.
- Prevention and Management
- Always find the medial epicondyle; CT or comparison films if uncertain; open extraction/fixation if incarcerated.
- Where It Occurs
- Medial epicondyle injury or fixation.
- Prevention and Management
- Document before surgery, protect during approach, reassess after fixation.
- Where It Occurs
- Radial neck injury or percutaneous/open reduction.
- Prevention and Management
- Pre/post documentation, careful trajectory, observation for neurapraxia unless progressive or iatrogenic concern.
- Where It Occurs
- Olecranon tension band or wires.
- Prevention and Management
- Choose fixation carefully; remove symptomatic hardware after union when needed.
Operative Technique
Radial neck reduction ladder
The principle is to reduce the radial neck with the least soft-tissue stripping that gives a stable, congruent, mobile elbow.
- Technique
- Traction, varus/valgus correction as appropriate, forearm rotation, and direct pressure over the radial head/neck under image intensifier.
- Technical Points
- Do not repeatedly force the fracture. Recheck rotation and radiocapitellar alignment.
- Technique
- Use a small K-wire or elevator as a joystick/leverage tool under fluoroscopy.
- Technical Points
- Stay aware of the posterior interosseous nerve; use controlled passes and avoid multiple blind attempts.
- Technique
- A prebent elastic nail is passed from the distal radius region and rotated to elevate and reduce the radial head fragment.
- Technical Points
- Useful for displaced fractures when closed reduction is inadequate; confirm head-neck alignment and avoid physeal injury.
- Technique
- Lateral approach only when closed/percutaneous methods fail or the fracture is irreducible.
- Technical Points
- Preserve periosteum and soft tissue; warn about stiffness, avascular necrosis and synostosis.
Olecranon fixation
Use a posterior approach centred on the olecranon. The operation is directed by the fracture pattern:
- Simple transverse displaced fracture: reduce articular surface anatomically; fixation may be suture tension band, wire tension band, intramedullary screw or combined construct depending size and maturity.
- Comminuted or oblique pattern: plate fixation may provide better control than tension band alone.
- Skeletally immature child: minimise physeal/apophyseal injury and choose fixation that avoids unnecessary hardware prominence.
- Associated instability: confirm radiocapitellar congruity and ulna alignment after fixation.
Key steps:
- Position supine or lateral with image intensifier access.
- Mark olecranon, proximal ulna, medial epicondyle and ulnar nerve course.
- Posterior incision; protect skin flaps and avoid unnecessary ulnar nerve handling unless the approach extends medially.
- Clear fracture haematoma without stripping soft tissue unnecessarily.
- Reduce the articular surface and confirm on AP/lateral fluoroscopy.
- Choose fixation based on pattern: suture tension band, wire tension band, screw, plate or hybrid.
- Test elbow motion and radiocapitellar alignment before closure.
- Immobilise initially, then start motion when fixation and soft tissues allow.
Elbow dislocation with incarcerated medial epicondyle
This is a surgical problem because the fragment blocks joint restoration and carries the medial collateral ligament attachment.
- Position supine with the arm on a hand table.
- Mark the medial epicondyle, olecranon and ulnar nerve.
- Use a medial approach centred over the medial epicondyle.
- Identify and protect the ulnar nerve; transpose only if needed for exposure, instability or nerve symptoms.
- Open the joint enough to extract the incarcerated fragment.
- Reduce the medial epicondyle to its origin and fix with screw, K-wire or suture construct according to fragment size and skeletal maturity.
- Confirm ulnohumeral and radiocapitellar congruity on AP and lateral images.
- Check elbow stability through a safe arc.
- Repeat and document median, ulnar and posterior interosseous nerve function post-operatively.
Post-Operative Care and Rehabilitation
The elbow becomes stiff quickly, but unstable fixation or an unrecognised associated injury is worse than a short period of protection. Rehabilitation therefore depends on the stability achieved.
- Immobilisation
- Above-elbow cast or splint initially.
- Follow-up Focus
- Repeat radiographs, pain, rotation, extension and nerve function.
- Immobilisation
- Splint or cast until early healing; avoid prolonged immobilisation if stable.
- Follow-up Focus
- Radiocapitellar alignment, forearm rotation, PIN function and stiffness.
- Immobilisation
- Protect fixation, then progressive motion.
- Follow-up Focus
- Union, hardware symptoms, extension strength and articular congruity.
- Immobilisation
- Brief protection if stable; longer protection if complex.
- Follow-up Focus
- Stability, medial epicondyle healing, ulnar nerve symptoms and range of motion.
Parents should understand that the goal is not simply bone healing. The child also needs a congruent elbow, recovering motion, intact nerve function and no missed associated injury.
Guidelines, Registries & Global Practice
Paediatric elbow trauma is managed worldwide, and the broad principles are consistent across societies even though the supporting evidence is mostly low level. There is no implant registry for paediatric elbow fractures comparable to adult arthroplasty registries, so practice is guided by society statements, trauma networks and large series.
Global epidemiology
- Elbow fractures are among the most common paediatric fractures, with supracondylar fractures the largest group; radial neck fractures comprise roughly 5-10% of paediatric elbow fractures and about 1% of all paediatric fractures.
- Medial epicondyle fractures have an estimated incidence near 40-60 per 100,000 per year and are associated with elbow dislocation in about 60% of cases.
- Median nerve injury complicates approximately 3% of paediatric elbow dislocations, linked to medial epicondyle avulsion.
Side-by-side guidance
- Emphasis
- Least-invasive reduction first for radial neck; individualised medial epicondyle care.
- Practical Point
- Open radial neck reduction is reserved for failed closed and percutaneous methods.
- Emphasis
- Standardised paediatric trauma pathways; prioritised the medial epicondyle question (SCIENCE trial).
- Practical Point
- Displaced medial epicondyle management is treated as an evidence gap, not a fixed rule.
- Emphasis
- Pattern-based fixation principles and the least-invasive construct that restores stability.
- Practical Point
- Choose tension band, screw or plate by fracture pattern and maturity.
- Emphasis
- Recognition of associated injuries (Monteggia, medial epicondyle) and early motion.
- Practical Point
- Always trace the radiocapitellar line and avoid prolonged immobilisation.
High- versus limited-resource practice
- Typical Reality
- Fluoroscopy, CT, flexible nails and early specialist review available.
- Adaptation
- Use the full reduction ladder and image-guided percutaneous techniques.
- Typical Reality
- Variable fluoroscopy, delayed presentation, limited implants.
- Adaptation
- Prioritise safe closed reduction, K-wire constructs and reliable follow-up; refer complex fracture-dislocations early.
- Typical Reality
- More common where access is limited; chronic Monteggia or stiff radial neck malunion.
- Adaptation
- Plan reconstruction (ulnar osteotomy, annular ligament reconstruction) at a capable centre.
Controversies and Areas of Uncertainty
Much of paediatric elbow trauma rests on retrospective series rather than randomised trials, so honest examiners reward candidates who can state where the evidence is genuinely unsettled.
- Arguments For
- Younger children remodel; thresholds near 30 degrees are widely quoted.
- Arguments Against
- Remodelling is unreliable for translation and rotation; older children remodel poorly.
- Practical Position
- Treat the rotation block and the child's age, not a single angle in isolation.
- Arguments For
- Higher union odds with fixation; helps high-demand athletes and unstable elbows.
- Arguments Against
- Similar pain and function in retrospective series; non-union is often asymptomatic.
- Practical Position
- Fix incarcerated or open fractures; individualise the rest while the SCIENCE trial reports.
- Arguments For
- Wire is familiar and strong; suture avoids prominent metal and removal.
- Arguments Against
- Wire carries higher hardware-symptom and removal rates.
- Practical Position
- Match the construct to pattern and maturity; suture is a legitimate option.
- Arguments For
- Missing it leads to chronic radial head dislocation and PIN palsy.
- Arguments Against
- Over-imaging every forearm is low yield.
- Practical Position
- Trace the radiocapitellar line on every elbow film and image the forearm if the ulna looks bowed.
- Arguments For
- Removes prominent or symptomatic hardware in active children.
- Arguments Against
- A second anaesthetic and surgical risk for asymptomatic implants.
- Practical Position
- Remove for symptoms or planned protocols, not reflexively.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A 9-year-old has a radial neck fracture with about 45 degrees angulation and painful blocked rotation. The hand is perfused and PIN function is normal.”
“A 12-year-old elbow dislocation is reduced in the emergency department. Post-reduction films show a congruent joint, but the medial epicondyle cannot be seen in its normal position.”
“A child has an undisplaced olecranon fracture and can actively extend the elbow. The radiocapitellar line is normal.”
Assessment
- Document skin, perfusion and median, ulnar and posterior interosseous nerve function.
- Order true AP and lateral elbow radiographs; add forearm views if Monteggia is possible.
- After dislocation reduction, find the medial epicondyle and recheck post-reduction films.
Treatment decisions
- Radial neck treatment depends on angulation, translation, rotation block, age and associated injury.
- Use the radial neck reduction ladder: closed, percutaneous leverage, intramedullary reduction, open only if needed.
- Olecranon treatment depends on displacement, articular congruity, extensor mechanism and proximal ulna alignment.
Do not miss
- Simple stable elbow dislocations need early protected motion; complex patterns need fixation or stabilisation.
- Warn about stiffness, loss of rotation, AVN, synostosis, nerve injury, hardware prominence and missed associated injury.
- A missing medial epicondyle or abnormal radiocapitellar line after reduction changes the diagnosis.
Evidence Signals
Paediatric olecranon fixation: suture vs wire tension band
- Nine studies were pooled, with three directly comparing tension-band suturing (TBS) with tension-band wiring (TBW).
- No statistically significant differences in pain, non-union, revision fixation or extension loss.
- TBS demonstrated fewer hardware-related complications than TBW.
Metaizeau closed intramedullary pinning technique
- Radial neck fractures account for about 1% of all paediatric fractures and 5-10% of paediatric elbow fractures.
- A retrograde nail is rotated 180 degrees to reduce the radial head while preserving the tenuous periosteal blood supply; the forearm is pronated during insertion to protect the posterior interosseous nerve.
- Across cited series, good or excellent Mayo Elbow Performance Scores were reported in roughly 80-100% of selected cases.
Percutaneous leverage technique
- A modified percutaneous leverage technique (Wallace technique) plus flexible intramedullary fixation reduced eight displaced paediatric radial neck fractures at a single Level I centre.
- The technique is minimally invasive compared with open reduction and permits early elbow mobilisation.
- No patient in the series developed synostosis or sustained a peripheral nerve injury.
Surgical radial neck series: predictors of poor outcome
- 151 surgically treated children; mean angulation improved from 43 to 13 degrees and displacement from 37% to under 1%.
- Among 131 with follow-up, 31% had an unsuccessful outcome; age 10 years or more, greater displacement and open reduction were independent predictors of failure.
- Closed manipulation was predicted to fail in about half of fractures angulated 36 degrees or more, and about half displaced 65% or more needed open reduction.