Terminal Sensory Branch of the Musculocutaneous Nerve
- The lateral antebrachial cutaneous nerve (LACN, also LABCN) is the TERMINAL SENSORY continuation of the MUSCULOCUTANEOUS nerve, which arises from the lateral cord of the brachial plexus (C5-C6); after the musculocutaneous nerve pierces coracobrachialis and runs between biceps and brachialis - supplying coracobrachialis, biceps and brachialis - it emerges at the elbow LATERAL to the biceps tendon and continues as the purely sensory LACN.
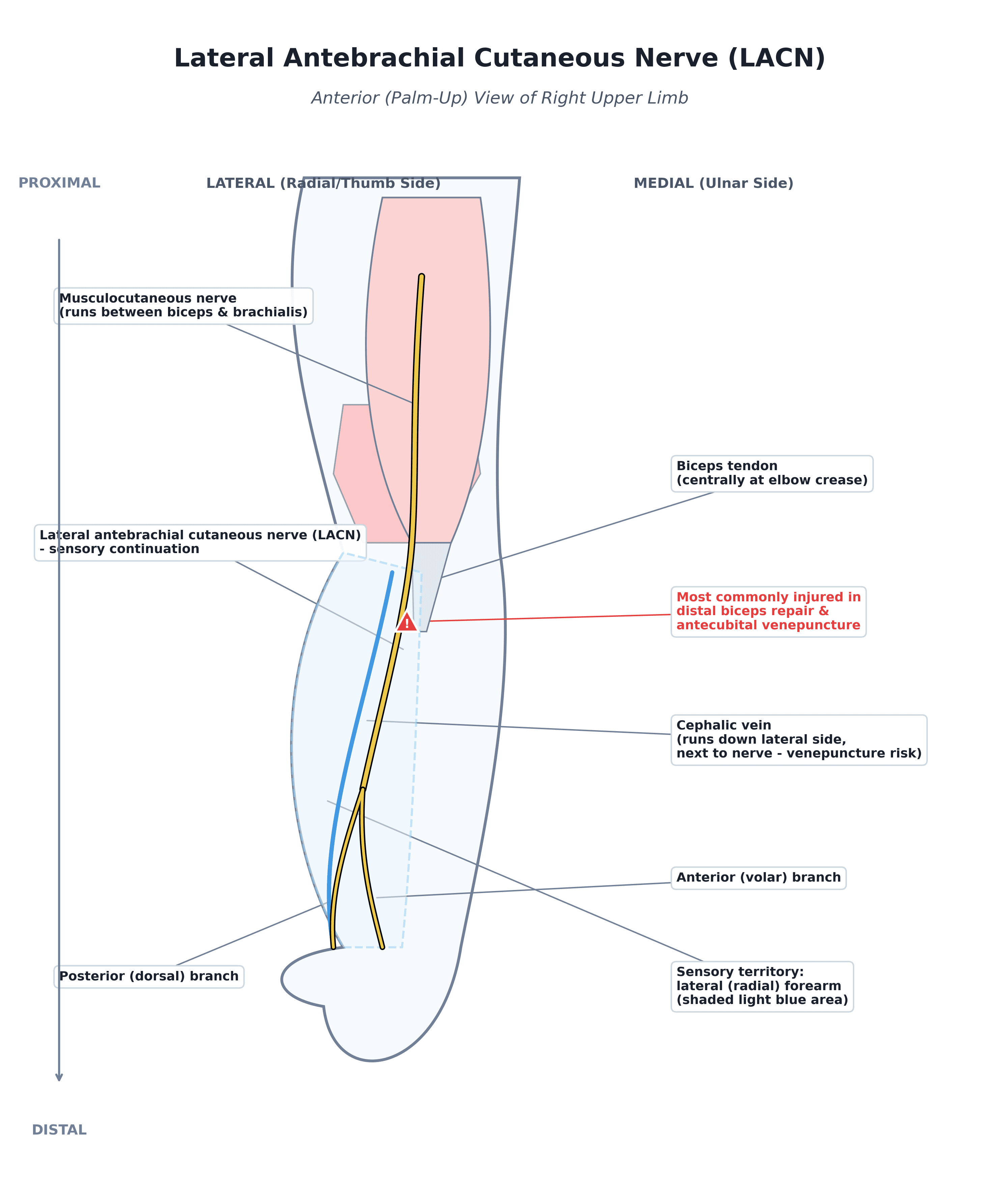
- At the elbow the LACN emerges from beneath the LATERAL border of the biceps, in the interval between the biceps and the brachialis/brachioradialis, lying LATERAL to the biceps tendon and immediately DEEP/adjacent to the CEPHALIC VEIN - an anatomical relationship that is the key to its clinical vulnerability.
- The LACN supplies SENSATION to the LATERAL (radial) aspect of the FOREARM, from the elbow down towards the wrist (and the thenar region of the wrist); it carries NO motor function (the motor supply of the musculocutaneous nerve to the arm flexors is given off proximally before it becomes the LACN).
- Because of its proximity to the distal biceps tendon and the cephalic vein, the LACN is the nerve most commonly injured during DISTAL BICEPS TENDON REPAIR (particularly anterior single-incision and the anterior limb of two-incision approaches) and during antecubital VENEPUNCTURE or cephalic vein cannulation/'traumatic phlebotomy', as well as in other lateral elbow/anterior forearm approaches.
- Injury PRESENTS with numbness, paraesthesia or dysaesthesia over the lateral forearm, sometimes with a painful NEUROMA or Tinel's sign over the nerve at the elbow; because the symptoms are sensory and overlie the lateral forearm, they can MIMIC other conditions (e.g. superficial radial nerve symptoms or lateral elbow pathology), so awareness of the nerve's location and territory is important for diagnosis.
- It is usually a CLINICAL diagnosis supported by the history (e.g. recent distal biceps surgery or venepuncture) and examination; nerve conduction studies can record LACN sensory responses (bilateral absence of LACN responses can suggest an inflammatory cause within a wider musculocutaneous neuropathy), but nerve conduction studies alone are insufficient, so the diagnosis rests on anatomy and clinical correlation, and ULTRASOUND/MRI can show LACN enlargement when needed.
- “LACN = terminal SENSORY continuation of the MUSCULOCUTANEOUS nerve (C5-C6, lateral cord); no motor function (motor branches given off proximally).
- “Emerges LATERAL to the biceps tendon at the elbow, deep/adjacent to the CEPHALIC VEIN -> supplies sensation to the LATERAL (radial) forearm (elbow to wrist).
- “Vulnerable in DISTAL BICEPS TENDON REPAIR and antecubital VENEPUNCTURE; injury = lateral forearm numbness/paraesthesia/neuroma (can mimic superficial radial nerve symptoms).
The terminal sensory branch of the musculocutaneous nerve - emerges lateral to the biceps tendon at the elbow (near the cephalic vein) and supplies the lateral forearm.
At risk in distal biceps tendon repair and antecubital venepuncture; injury -> lateral forearm numbness/paraesthesia or a painful neuroma.
Course, Territory & Clinical Vulnerability
The lateral antebrachial cutaneous nerve (LACN) is the terminal sensory continuation of the musculocutaneous nerve (C5-C6, lateral cord). After the musculocutaneous nerve pierces coracobrachialis and runs between biceps and brachialis (supplying coracobrachialis, biceps and brachialis), it emerges at the elbow lateral to the biceps tendon, in the interval between biceps and brachialis/brachioradialis and deep/ adjacent to the cephalic vein, continuing as the purely sensory LACN. It supplies sensation to the lateral (radial) forearm from the elbow to the wrist. Its close relationship to the distal biceps tendon and cephalic vein is the key to its vulnerability: it is the nerve most commonly injured in distal biceps tendon repair (anterior single-incision/two-incision) and in antecubital venepuncture/cephalic vein cannulation, causing lateral forearm numbness, paraesthesia or a painful neuroma that can mimic other neuropathies.
Branching Pattern and Sensory Boundaries
Beyond emerging lateral to the biceps tendon, the LACN has a consistent terminal branching pattern that explains both its venepuncture vulnerability and the overlap with the superficial radial nerve.
- In the forearm the LACN typically divides into an anterior (volar) branch and a posterior (dorsal) branch.
- The anterior (volar) branch - the larger - descends along the radial border of the volar forearm with the cephalic vein to the wrist and the base of the thenar eminence; its course alongside the vein is why venepuncture/cannulation injures it.
- The posterior (dorsal) branch - smaller - runs over the dorsoradial forearm towards the wrist.
- Together they supply the skin of the lateral (radial) forearm from just below the elbow to the wrist - the volar branch over the radial-volar surface and thenar base, the dorsal branch over the dorsoradial surface.
- The LACN communicates with the superficial radial nerve (and the palmar cutaneous branch of the median nerve) near the wrist - the anatomical basis for the clinical overlap with superficial-radial-nerve symptoms.
- It does not supply the hand beyond the radial wrist/thenar base - the dorsoradial hand and thumb-web are superficial radial nerve territory.
Injury, Diagnosis & Protection
- Presentation: numbness/paraesthesia/dysaesthesia over the lateral forearm, sometimes a painful neuroma or Tinel's sign over the nerve at the elbow; sensory only (no weakness).
- Diagnosis: largely clinical (history of distal biceps surgery or venepuncture + lateral forearm sensory signs); nerve conduction studies can record LACN sensory responses (bilateral loss may suggest an inflammatory musculocutaneous neuropathy), and ultrasound/MRI can show nerve enlargement.
- Distinguish from: superficial radial nerve symptoms and other lateral elbow/forearm pathology (the territory overlaps clinically).
- Protect it surgically: in distal biceps repair, careful retraction and approach (awareness lateral to the biceps tendon) reduce injury; in venepuncture, avoid the area lateral to the biceps tendon where the nerve lies with the cephalic vein.
- Management of injury: most neurapraxic/traction injuries recover; a symptomatic neuroma may need desensitisation, injection, or excision/relocation.
The practical importance of the LACN is that it is the nerve most commonly injured during distal biceps tendon repair and during antecubital venepuncture, because it lies just lateral to the biceps tendon and immediately adjacent to the cephalic vein. So during a distal biceps repair the surgeon must be aware of its position lateral to the tendon and protect it with careful retraction, and a patient who develops lateral forearm numbness or a painful, tingling area after a distal biceps repair or a 'traumatic' venepuncture should be recognised as having an LACN injury rather than having the symptom dismissed or mis-attributed. Because the territory overlaps with the superficial radial nerve, knowing that the LACN supplies the lateral forearm and emerges lateral to the biceps tendon is what makes the diagnosis - and protecting it in that interval is what prevents the injury.
Differential of Lateral Forearm Sensory Symptoms
Because the LACN territory clinically overlaps neighbouring nerves, the examiner expects a structured differential of the patient with lateral-forearm or radial-sided sensory symptoms.
- Where the symptoms are
- Lateral (radial) FOREARM, elbow to wrist
- Discriminating features
- Sensory only; history of distal biceps repair or antecubital venepuncture; Tinel lateral to the biceps tendon at the elbow; no hand or neck symptoms
- Where the symptoms are
- Dorsoradial HAND, thumb and first web (not the forearm)
- Discriminating features
- Tinel over the distal radial forearm where the nerve emerges between brachioradialis and ECRL; provoked by tight bands or forearm pronation; may coexist with de Quervain's (developed in the Wartenberg's syndrome topic)
- Where the symptoms are
- Thumb and lateral forearm in a dermatomal pattern
- Discriminating features
- Neck pain radiating distally; MOTOR weakness (biceps, wrist extensors) and a reduced biceps/brachioradialis reflex; positive Spurling test (developed in the cervical-radiculopathy topic)
- Where the symptoms are
- Lateral elbow and proximal forearm
- Discriminating features
- PAIN rather than numbness; tenderness over the extensor origin or mobile wad; pain on resisted wrist/middle-finger extension; no fixed sensory loss (developed in the lateral-epicondylitis and radial-tunnel-syndrome topics)
The classic trap is confusing the LACN with the superficial radial nerve. The LACN numbs the lateral FOREARM (elbow to wrist) and is injured at the elbow (distal biceps repair; venepuncture lateral to the biceps tendon). The superficial radial nerve numbs the dorsoradial HAND and thumb-web and is irritated in the distal forearm (Wartenberg's syndrome). Forearm-not-hand, elbow-not-wrist, and a distal-biceps or venepuncture history point to the LACN; a normal forearm with dorsoradial-hand symptoms and a distal-forearm Tinel point to the superficial radial nerve. A dermatomal pattern with neck pain and motor signs means look at the C6 root instead.
Mnemonics & Memory Aids
LACN
Hook:LACN: Lateral to biceps tendon, A musculocutaneous branch, Cutaneous (lateral forearm), Nicked in distal biceps repair/venepuncture.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the lateral antebrachial cutaneous nerve and its clinical importance.”
Origin & course
- Terminal sensory continuation of the musculocutaneous nerve (C5-C6, lateral cord)
- Musculocutaneous: pierces coracobrachialis; supplies coracobrachialis/biceps/brachialis
- Emerges at the elbow lateral to the biceps tendon (deep/adjacent to the cephalic vein)
Territory
- Sensation to the lateral (radial) forearm, elbow to wrist
- Purely sensory (no motor function)
- Overlaps clinically with superficial radial nerve territory
Vulnerability
- Most commonly injured in distal biceps tendon repair (anterior/two-incision)
- Antecubital venepuncture / cephalic vein cannulation ('traumatic phlebotomy')
- Lateral elbow / anterior forearm approaches
Injury & diagnosis
- Lateral forearm numbness/paraesthesia or painful neuroma (sensory only)
- Clinical diagnosis; nerve conduction studies/ultrasound/MRI supportive
- Protect with careful retraction lateral to the biceps tendon
Evidence & Key Studies
Sonography of the lateral antebrachial cutaneous nerve (anatomy and vulnerability)
- Lateral antebrachial cutaneous nerve abnormalities are associated with antecubital conditions such as distal biceps brachii tendon tears and traumatic cephalic vein phlebotomy.
- The close proximity of the LACN to the distal biceps tendon and the cephalic vein makes it vulnerable to compression and injury, causing lateral forearm, elbow and wrist symptoms that can mimic other disease processes.
- Symptomatic nerves showed fusiform enlargement and increased echogenicity on ultrasound, aiding diagnosis.
Musculocutaneous neuropathy (including lateral antebrachial cutaneous neuropathy)
- Isolated musculocutaneous neuropathy is uncommon and most often results from acute trauma or surgery (65%); pain and sensory disturbance are more common presentations than weakness.
- Lateral antebrachial cutaneous neuropathy was identified as a related entity; bilateral absence of LACN sensory responses suggested an inflammatory cause.
- Nerve conduction studies alone are insufficient to confirm the neuropathy, and needle EMG should be part of the evaluation.
The LACN's close relationship to the distal biceps tendon and cephalic vein and its consequent vulnerability (with distal biceps tendon tears and traumatic phlebotomy, causing lateral forearm/ elbow/wrist symptoms that mimic other conditions) and its sonographic appearance come from the cited Chiavaras study; the relationship of LACN neuropathy to musculocutaneous neuropathy, the predominance of trauma/surgery as the cause, the sensory-over-motor presentation, and the role/limits of nerve conduction studies from the cited O'Gorman study. The course as the terminal sensory branch of the musculocutaneous nerve, its emergence lateral to the biceps tendon, and its lateral-forearm sensory territory are standard, well-established anatomical teaching. (See also our Distal Biceps Rupture and Musculocutaneous Nerve topics.)