Lateral Compression Pelvic Injuries
Lateral compression (LC) injuries are the most common pelvic ring injury pattern, accounting for 50-60% of all pelvic fractures. They result from a laterally directed force causing internal rotation of the hemipelvis, with the injury severity ranging from stable rami fractures (LC-I) to rotationally and vertically unstable patterns (LC-III).
Most Common | Internal Rotation | Rami + Sacrum | LC-I Stable | LC-III Unstable
YOUNG-BURGESS LC CLASSIFICATION
Critical Must-Knows
- LC is most common pelvic ring injury pattern (50-60%)
- Internal rotation deformity - pelvis narrows (vs APC which opens)
- Anterior ring: Ipsilateral pubic rami fractures
- Posterior ring: Sacral impaction (LC-I), crescent fracture (LC-II)
- LC-III = windswept pelvis: Contralateral APC component = unstable
Clinical Pearls
- "LC injuries tend to have LESS hemorrhage than APC (pelvis closes, tamponades)
- "Head injuries common with LC (lateral impact same as head impact)
- "Morel-Lavallee lesion = closed degloving over trochanter
- "LC-I often missed initially - look for sacral impaction line
- "LC-III is rotationally unstable - don't miss contralateral injury
Exam Warning
Critical Exam Points - Lateral Compression Injuries:
- MOST COMMON pelvic ring injury (50-60%) - know this cold
- INTERNAL ROTATION deformity - pelvis narrows, hemipelvis rotates in
- LC-I: Rami + sacral impaction = most common, usually stable, often conservative
- LC-II: Adds crescent (iliac wing) fracture = may need fixation
- LC-III: Windswept = LC on one side + APC on contralateral = UNSTABLE
- Less hemorrhage than APC (pelvis closes) but DON'T be complacent
- Associated head injuries - same lateral mechanism
At a Glance: Quick Decision Guide
| Feature | LC-I | LC-II | LC-III |
|---|---|---|---|
| Anterior Injury | Ipsilateral rami fractures | Ipsilateral rami fractures | Bilateral rami or symphysis |
| Posterior Injury | Sacral impaction (Zone 1) | Crescent fracture (iliac wing) | Ipsi LC + Contra APC |
| Rotational Stability | Stable | Variable | UNSTABLE |
| Vertical Stability | Stable | Stable | Potentially unstable |
| Hemorrhage Risk | Low | Moderate | High |
| Management | Conservative | Consider fixation | Surgical fixation |
L CLC - Lateral Compression Features
| L | Lateral force causes LESS bleeding pelvis closes |
| C | Compression narrows pelvis internal rotation |
| L | Lateral force causes LESS bleeding pelvis closes |
| C | Compression narrows pelvis internal rotation |
Hook:LC = Lateral Compression = LESS bleeding, pelvis CLOSES (internal rotation)
THREETHREE - LC Types
| T | Type I = rami + sacral impaction most common, stable |
| H | Higher energy in Type II adds crescent fracture |
| R | Rotationally unstable in Type III |
| E | External rotation added contralaterally in LC-III |
| E | Each type progressively more unstable |
| T | Type I = rami + sacral impaction most common, stable | E | External rotation added contralaterally in LC-III |
| H | Higher energy in Type II adds crescent fracture | E | Each type progressively more unstable |
| R | Rotationally unstable in Type III |
Hook:LC-I = stable, LC-II = intermediate, LC-III = unstable (windswept)
Overview/Epidemiology
Epidemiology

Incidence:
- Most common pelvic ring injury pattern (50-60% of all pelvic fractures)
- LC-I accounts for 70% of lateral compression injuries
- More common in motor vehicle accidents (T-bone collisions)
- Also common in pedestrian strikes
Demographics:
- All age groups affected
- Bimodal distribution: Young (high-energy MVA) and elderly (low-energy falls)
- No significant gender predilection
- Higher incidence in areas with higher traffic volume
Mechanism Distribution:
- Motor vehicle accidents: 60-70%
- Pedestrian vs vehicle: 15-20%
- Falls from height: 10-15%
- Other mechanisms: 5%
Associated Injuries:
- Head injuries: 40-50% (same lateral impact)
- Acetabular fractures: 20-30%
- Long bone fractures: 30-40%
- Thoracic injuries: 20-30%
- Neurological injuries: 10-20% (sacral fractures)
Anatomy and Pathophysiology
Pelvic Ring Anatomy
Pelvic Ring Concept
Osseous Ring Components:
- Anterior ring: Pubic symphysis + superior/inferior pubic rami
- Posterior ring: Sacrum + sacroiliac joints + posterior ilium
Key Principle: The pelvic ring cannot break in one place - if there's an anterior injury, there MUST be a posterior injury (and vice versa). Always search for the second break.
Mechanism of Injury
Lateral Compression Force:
- Force directed laterally (side impact)
- Common scenarios: MVA (T-bone), pedestrian struck, fall from height landing on side
- Force causes internal rotation of the hemipelvis
Resultant Deformity:
- Hemipelvis rotates INTERNALLY
- Pelvis narrows (in contrast to APC which widens)
- Creates compression anteriorly and posteriorly
Understanding the Deformity
LC = Internal Rotation = Pelvis Narrows
- The involved hemipelvis rotates inward
- This CLOSES the pelvic volume (less space for hemorrhage)
- Generally less hemodynamically unstable than APC
- But don't be complacent - severe LC can still bleed significantly
Associated Injuries - Important for LC
Head Injuries:
- Very common with LC mechanism
- Same lateral force that hits pelvis also hits head
- Always assess neurological status
Morel-Lavallee Lesion:
- Closed internal degloving injury
- Shear between skin/fat and underlying fascia
- Typically over greater trochanter
- Can occur without external wound
- Delayed presentation possible
- MRI for diagnosis if suspected
Morel-Lavallee Lesion
A closed degloving injury over the trochanter caused by the same lateral force as the LC injury. Can create a large fluid collection that may become infected. Important to identify before surgical incisions. MRI is diagnostic - look for fluid collection between fat and fascia.
Pelvic Stability Determinants
Posterior Ring is Key:
- 60% of pelvic stability from posterior structures
- SI ligament complex (anterior, posterior, interosseous)
- Posterior tension band (iliolumbar, lumbosacral, sacrospinous, sacrotuberous ligaments)
In LC Injuries:
- LC-I: Posterior ligaments intact, sacral impaction only = STABLE
- LC-II: Partial posterior disruption (crescent fracture) = VARIABLE stability
- LC-III: Both SI joint disruptions (ipsi LC + contra APC) = UNSTABLE
Classification Systems
Young-Burgess Classification
LC Type I (Most Common)
Pattern:
- Anterior: Ipsilateral pubic rami fractures (superior and/or inferior)
- Posterior: Ipsilateral sacral impaction fracture (usually Zone 1)
Characteristics:
- Most common LC subtype (70% of LC injuries)
- Generally stable (both rotationally and vertically)
- Posterior ligaments INTACT
- Sacral impaction often subtle on X-ray (need CT)
Stability:
- Rotationally stable
- Vertically stable
- Often treated conservatively
Management:
- Usually conservative treatment
- Analgesia and DVT prophylaxis
- Early mobilization as tolerated
- Weight-bearing as tolerated
LC-I injuries typically have excellent outcomes with non-operative management.
LC Classification Summary
| Type | Anterior | Posterior | Stability | Treatment |
|---|---|---|---|---|
| LC-I | Ipsilateral rami | Sacral impaction | Stable | Conservative |
| LC-II | Ipsilateral rami | Crescent fracture | Variable | Consider fixation |
| LC-III | Bilateral | Ipsi LC + Contra APC | UNSTABLE | Surgical fixation |
Tile Classification Correlation
| Young-Burgess | Tile | Description |
|---|---|---|
| LC-I | B2.1 | Stable internal rotation |
| LC-II | B2.2 | Partially unstable (crescent) |
| LC-III | C | Completely unstable |
CRESCENTCRESCENT - LC-II Features
| C | Crescent fracture through posterior ilium |
| R | Rami fractures anteriorly as in LC-I |
| E | Energy higher than LC-I |
| S | SI joint partially intact fragment attached |
| C | Consider fixation variable stability |
| E | Evaluate carefully for stability |
| N | Not as unstable as LC-III |
| T | Through-and-through posterior ilium fracture |
| C | Crescent fracture through posterior ilium | S | SI joint partially intact fragment attached | N | Not as unstable as LC-III |
| R | Rami fractures anteriorly as in LC-I | C | Consider fixation variable stability | T | Through-and-through posterior ilium fracture |
| E | Energy higher than LC-I | E | Evaluate carefully for stability |
Hook:CRESCENT fracture = LC-II = posterior iliac wing fracture keeping crescent attached to sacrum
Clinical Assessment
Initial Assessment
Presentation
History:
- Mechanism of injury (lateral impact)
- Level of consciousness (associated head injury common)
- Ability to ambulate
- Pain location
Primary Survey:
- ABC assessment
- Hemodynamic status
- Pelvic stability testing (ONCE only, gently)
- Associated injuries
Examination
Inspection:
- Leg length discrepancy
- Rotational deformity
- Ecchymosis over pelvis/perineum
- Open wounds (including perineum, vagina, rectum)
- Morel-Lavallee lesion (bruising/fluctuance over trochanter)
Palpation:
- Tenderness over symphysis
- Tenderness over SI joints
- Tenderness over iliac crests
- Crepitus (may indicate unstable fragments)
Pelvic Stability Testing
Test pelvic stability ONCE and GENTLY:
- Performed during primary survey
- Apply gentle AP compression and lateral compression to iliac crests
- Do NOT repeatedly test - can disrupt clot and worsen hemorrhage
- If unstable, apply pelvic binder immediately
- Document findings clearly
Associated Injuries to Assess
Urogenital:
- Blood at urethral meatus = urethral injury (do NOT catheterize)
- Hematuria
- High-riding prostate on DRE
- Vaginal/scrotal hematoma
Neurological:
- Lumbosacral plexus injury
- L4-S1 nerve roots (sacral fractures)
- Assess motor and sensory function
Other:
- Head injury (very common with LC)
- Abdominal injuries
- Long bone fractures
- Acetabular fractures (same mechanism)
Hemodynamic Considerations
LC Injuries Generally Bleed Less Than APC:
- Internal rotation closes pelvis
- Tamponades bleeding to some extent
- But can still have significant hemorrhage
Don't Be Complacent:
- LC-III can have substantial bleeding
- Associated injuries may contribute
- Assess and reassess hemodynamic status
Differential Diagnosis
When an AP pelvis shows rami fractures or pelvic pain after a fall or collision, distinguish lateral compression from its main mimics. The discriminating features are the direction of the deforming force, the posterior ring lesion on CT, and the patient's bone quality.
Differential Diagnosis of the Lateral Compression Pattern
| Diagnosis | Mechanism / Force | Key Discriminator | Stability / Action |
|---|---|---|---|
| Lateral compression (LC) | Lateral force, internal rotation | Ipsilateral rami plus sacral impaction; pelvis narrows | LC-I usually stable; stress test if complete sacral fracture |
| Anteroposterior compression (APC) | AP force, external rotation | Symphyseal widening or diastasis; pelvis opens; high transfusion | Often unstable; binder effective; higher haemorrhage risk |
| Vertical shear | Axial / vertical force (fall, dashboard) | Vertical migration of hemipelvis; complete posterior disruption | Vertically unstable; needs reduction and fixation |
| Fragility fracture of the pelvis (FFP) | Low-energy fall, osteoporosis, elderly | Minimal trauma; FFP/Rommens classification; often bilateral sacral | Usually nonoperative; fixation if progressive pain or instability |
| Isolated pubic rami fracture | Low-energy fall in elderly | No demonstrable posterior ring injury on CT | Stable; analgesia and early mobilisation |
| Acetabular fracture | Lateral force through greater trochanter | Articular involvement on Judet views/CT; hip joint affected | Depends on dome and congruity; often operative |
Rami Fracture: Always Hunt the Posterior Lesion
A pubic rami fracture is never a diagnosis on its own - it is a sign. In a young high-energy patient it usually represents the anterior component of an LC injury and demands CT to find the posterior (sacral or iliac) lesion. In an elderly low-energy patient the same X-ray may be an isolated fragility fracture or a fragility fracture of the pelvis (FFP) with an occult sacral ala fracture - CT still changes management.
Investigations
Imaging Protocol
Plain Radiographs
AP Pelvis (First-Line):
- Standard in all trauma patients
- Assess pelvic ring continuity
- Look for rami fractures
- Assess symphysis width
- Assess SI joint symmetry
Inlet View:
- AP/internal rotation assessment
- Assess posterior displacement
- Shows sacral impaction
Outlet View:
- Superior/inferior displacement
- Assess sacral fractures
- Neural foramina assessment
CT Scan (Essential)
CT is Mandatory
CT scan is mandatory for all pelvic ring injuries to:
- Identify sacral fractures (often occult on X-ray)
- Classify injury accurately
- Assess posterior ring stability
- Identify associated injuries (acetabulum, lumbar spine)
- Plan surgical approach if needed
CT Assessment:
- Sacral fracture pattern (Zone 1, 2, 3)
- SI joint integrity
- Crescent fracture identification
- Posterior ligamentous structures
- Neural canal involvement
- Associated acetabular fractures
MRI (Selected Cases)
Indications:
- Suspected ligamentous injury without fracture
- Neurological deficit evaluation
- SI joint instability assessment
- Morel-Lavallee lesion evaluation
Sacral Fracture Zones (Denis)
| Zone | Location | Structures at Risk | LC Association |
|---|---|---|---|
| 1 | Sacral ala (lateral to foramina) | L5 nerve root | LC-I most common |
| 2 | Through foramina | S1-S4 nerve roots | LC-I, LC-II |
| 3 | Central canal | Cauda equina | Less common in LC |
Management Algorithm
Management Decision Tree
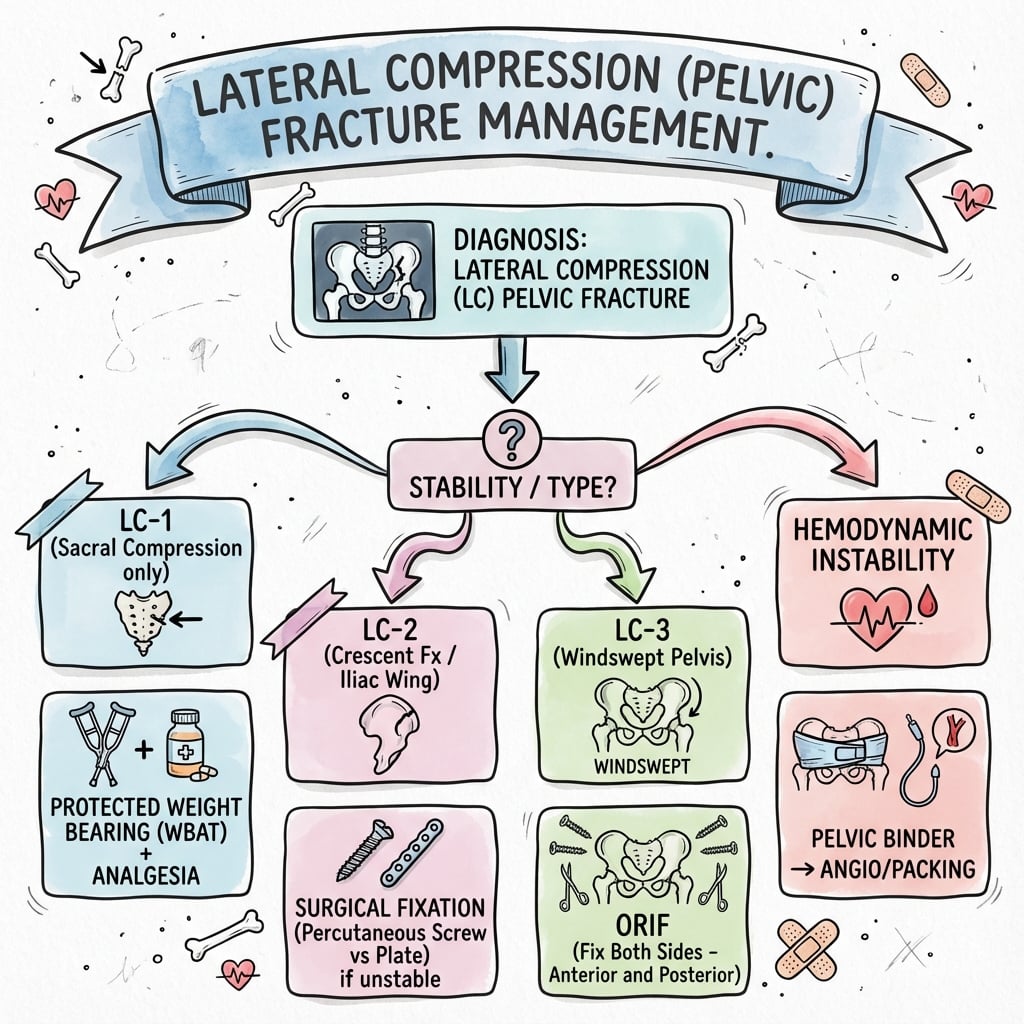
1. Hemodynamically Unstable:
- Resuscitation, pelvic binder
- Angiography/embolization vs external fixation vs preperitoneal packing
- Definitive fixation when stable
2. Hemodynamically Stable:
- Complete imaging (CT)
- Classify injury
- LC-I: Usually conservative
- LC-II: Assess stability - may need fixation
- LC-III: Surgical fixation required
Immediate Management
Resuscitation:
- ATLS protocol
- Massive transfusion protocol if needed
- Pelvic binder application
Damage Control Options:
- Angiography/embolization: First-line for arterial bleeding
- Preperitoneal packing: If angio unavailable or venous bleeding
- External fixation: Temporary stabilization
Definitive Treatment:
- Once patient stabilized
- Convert to internal fixation at 24-72 hours
Hemodynamically unstable patients require immediate resuscitation and hemorrhage control.
Initial Stabilization
Pelvic Binder:
- Apply in ED if instability suspected
- Centered at level of greater trochanters (NOT iliac crests)
- Can be improvised with sheet if commercial binder unavailable
- Monitor skin under binder
For LC Injuries:
- Binder less effective than APC (pelvis already closed)
- Still apply if unstable
- May actually worsen internal rotation - monitor carefully
Conservative Management (LC-I)
Indications:
- Stable LC-I injuries
- Minimal displacement
- Patient can tolerate limited mobilization
Protocol:
- Analgesia (multimodal)
- DVT prophylaxis (critical)
- Early mobilization as tolerated
- Weight-bearing as tolerated (depends on symptoms)
- PT assessment
- Follow-up imaging at 6 weeks
Surgical Management
Indications for Surgery:
- LC-II with instability
- All LC-III injuries
- Significant displacement
- Associated acetabular fracture requiring fixation
- Polytrauma requiring mobilization
FIXFIX - Surgical Indications
| F | Failed conservative management or LC-III |
| I | Instability rotational or vertical |
| X | X-ray shows significant displacement |
| F | Failed conservative management or LC-III |
| I | Instability rotational or vertical |
| X | X-ray shows significant displacement |
Hook:FIX LC injuries when unstable or significantly displaced
Surgical Options
Anterior Fixation:
- Symphyseal plating (if symphysis disrupted in LC-III)
- Rami plating (rarely needed for LC)
- External fixation (damage control)
Posterior Fixation:
- Percutaneous SI screws (most common)
- Posterior plating
- Spinopelvic fixation (severe instability)
Timing:
- Damage control: External fixation acutely
- Definitive fixation: When patient optimized (24-72h typically)
- LC-I may never need surgery
Surgical Technique
Fixation Techniques for LC Injuries
Posterior Fixation - Percutaneous SI Screws
Most Common Technique for LC-II/III
Positioning:
- Supine on radiolucent table
- Image intensifier with inlet and outlet views
Approach:
- Percutaneous technique
- Entry point: Lateral ilium, above greater sciatic notch
- Direction: Anterior and medial toward S1 body
Technique:
- Inlet view: Confirm anterior-posterior trajectory
- Outlet view: Confirm superior-inferior trajectory (avoid neural foramina)
- Guidewire placement under fluoroscopy
- Measure screw length (typically 80-100mm)
- Fully threaded lag screw or partially threaded compression screw
- Place 1-2 screws into S1 (S2 if needed)
Key Pearls:
- Inlet and outlet views mandatory throughout
- Avoid neural foramina (outlet view)
- Avoid anterior cortex of sacrum (inlet view)
- Compression across SI joint improves stability
Percutaneous SI screws are the gold standard for posterior ring fixation in LC injuries.
Complications
Early and Late Complications
Early Complications
Hemorrhage:
- Less than APC but still significant
- Arterial (superior gluteal, pudendal) or venous
- May need angioembolization or packing
Associated Injuries:
- Urethral injury (less common in LC than APC)
- Bladder injury
- Neurological injury (sacral fractures)
Morel-Lavallee Lesion:
- May need drainage or debridement
- Can delay wound healing
- Infection risk if not addressed
Late Complications
Malunion:
- Leg length discrepancy
- Pelvic obliquity
- Gait abnormality
- Sitting difficulty
Post-Traumatic Arthritis:
- SI joint arthritis
- May develop despite good reduction
Chronic Pain:
- SI joint pain common
- May need delayed fusion
Neurological:
- Persistent nerve injury (L5, S1-S4)
- More common with sacral fractures through foramina
Postoperative Care
Immediate Postoperative Management
First 24-48 Hours:
- Monitor neurovascular status
- Pain control (multimodal analgesia)
- DVT prophylaxis (critical - high risk)
- Incentive spirometry
- Early mobilization to chair
Weight-Bearing Status
LC-I (Conservative Treatment):
- Weight-bearing as tolerated
- May use walking aids initially
- Progress based on pain
LC-II/III (Surgical Fixation):
- First 6 weeks: Touch weight-bearing (10-15kg) with crutches or frame
- 6-12 weeks: Progressive weight-bearing if radiographic healing
- 12+ weeks: Full weight-bearing once healed
Special Considerations:
- Bilateral injuries may need wheelchair initially
- Posterior ring instability delays full weight-bearing
- Follow serial X-rays to assess healing
DVT Prophylaxis
Critical Importance:
- Pelvic fractures = high VTE risk
- Combined mechanical and pharmacological prophylaxis
Protocol:
- LMWH or fondaparinux (start when safe)
- Compression stockings/intermittent pneumatic compression
- Early mobilization
- Continue for 6 weeks minimum
- Consider 3 months for high-risk patients
Rehabilitation Protocol
Phase 1 (0-6 weeks):
- Protected weight-bearing
- Gentle ROM exercises (hip, knee)
- Core strengthening (isometric)
- Gait training with aids
Phase 2 (6-12 weeks):
- Progressive weight-bearing
- Strengthening exercises
- Balance and proprioception training
- Pool therapy if available
Phase 3 (12+ weeks):
- Full weight-bearing
- Sport-specific rehabilitation
- Return to work planning
- Address any residual deficits
Follow-Up Schedule
Timing:
- 2 weeks: Wound check, neurovascular assessment
- 6 weeks: X-rays, assess healing, advance weight-bearing
- 12 weeks: X-rays, consider full weight-bearing
- 6 months: Final X-rays, functional assessment
- 12 months: Long-term outcome evaluation
Red Flags to Monitor:
- Increasing pain (hardware failure, non-union)
- Loss of reduction
- Neurological changes
- Wound complications
- Signs of DVT/PE
Outcomes/Prognosis
Functional Outcomes by Injury Type
LC-I (Excellent Prognosis):
- Over 90% return to pre-injury function
- Most patients return to work within 3-6 months
- Low rate of chronic pain (under 20%)
- Minimal long-term disability
- Conservative treatment highly successful
LC-II (Good Prognosis):
- 70-80% return to full function
- May have residual SI joint pain (30-40%)
- Return to work 4-9 months typically
- Outcomes better with appropriate surgical fixation if unstable
- Some patients require long-term analgesia
LC-III (Fair to Good Prognosis):
- 50-70% return to baseline function
- Higher rate of chronic pain and disability
- Often limited by associated injuries
- Return to work 6-12+ months
- May require workplace modifications
- Psychological impact significant
Outcomes by LC Type
| Outcome Measure | LC-I | LC-II | LC-III |
|---|---|---|---|
| Return to Function | Over 90% | 70-80% | 50-70% |
| Chronic Pain | Under 20% | 30-40% | Over 50% |
| Need for Surgery | Under 10% | 30-50% | Over 90% |
| Return to Work | 3-6 months | 4-9 months | 6-12+ months |
| Overall Prognosis | Excellent | Good | Fair |
Prognostic Factors
Better Outcomes:
- LC-I pattern (stable)
- Younger age (under 50)
- No associated injuries
- Early mobilization
- Appropriate treatment selection
Worse Outcomes:
- LC-III pattern (unstable)
- Elderly patients (over 65)
- Multiple associated injuries
- Delayed or inadequate treatment
- Comorbidities (diabetes, osteoporosis)
Union and Healing
Pelvic Ring Healing:
- Most LC injuries unite with conservative or surgical treatment
- Healing time: 8-12 weeks typically
- Non-union rare (under 5%)
- Malunion more common than non-union
Factors Affecting Healing:
- Displacement degree
- Stability of fixation
- Patient compliance with weight-bearing restrictions
- Smoking (delays healing)
- NSAIDs (may impair healing - use cautiously)
Long-Term Considerations
Post-Traumatic Arthritis:
- SI joint arthritis develops in 20-40% of LC injuries
- Risk higher with residual displacement
- May require delayed SI fusion
Sexual Function:
- May be affected, especially in LC-III
- Discuss openly with patients
- Referral to appropriate specialists if needed
Childbirth:
- Most women can deliver vaginally after healed LC injury
- Caesarean section may be needed if significant pelvic deformity
- Discuss with obstetrics early in pregnancy
Evidence Base
Young-Burgess Classification - The Defining Study
- Landmark prospective series of 210 consecutive high-energy pelvic ring disruptions that established the mechanism-based classification (lateral compression, anteroposterior compression, vertical shear, combined mechanical) still in worldwide use.
- Mean blood replacement was markedly lower for lateral compression (3.6 units) than for anteroposterior compression (14.8 units), confirming that the internally rotated, closed pelvis bleeds less.
- Overall mortality was 8.6 percent (7.0 percent for LC versus 20.0 percent for APC); the cause of death was attributable to the pelvic fracture in fewer than half of cases, underlining the role of associated injuries.
Tile Classification - Stability Determined by the Posterior Ring
- Foundational review establishing that, although the anterior structures contribute roughly 40 percent of pelvic stiffness, the posterior sacroiliac complex is the principal determinant of ring stability - so classification is based on the posterior lesion.
- Defined Type A (stable), Type B (rotationally unstable, vertically stable) and Type C (rotationally and vertically unstable); LC injuries span all three groups, with Type A and B making up 70 to 80 percent of all pelvic injuries.
- Key point: LC-I corresponds to Type A or B2 (stable) and LC-III to Type C (unstable).
Occult Instability of LC-1 Injuries with Complete Sacral Fracture
- Prospective study of 63 LC-1 injuries assessed by intra-operative manipulation under anaesthesia; rotational instability (more than 2 cm translation) was present in every case that had a complete sacral fracture.
- Surgically stabilised patients had significantly shorter hospital stay, faster pain-free mobilisation and lower opioid requirements than nonoperatively managed patients.
- Key point: a complete posterior sacral fracture in an LC-1 pattern signals occult rotational instability that may benefit from fixation.
Emergency Department Stress Radiographs for LC-1 Stability
- Prospective study of 70 minimally displaced LC1 injuries showing that awake fluoroscopic stress examination in the emergency department is safe, well tolerated and reliable (displacement greater than or equal to 10 mm of rami overlap defined a positive result).
- A negative stress examination (57 of 70 patients, 81 percent) reliably predicted successful nonoperative treatment with union and no substantial displacement at follow-up.
- ED stress displacement matched examination under anaesthesia exactly in the 11 patients tested by both methods, supporting an awake protocol that avoids unnecessary theatre and anaesthesia.
Rami Fracture Morphology Predicts LC-1 Displacement
- Cadaveric biomechanical study showing that oblique superior pubic ramus fractures allow significantly more lateral deflection than transverse fractures in the unfixed pelvis.
- Posterior-only and combined anterior-posterior fixation reduced deflection more than no fixation or anterior fixation alone.
- Key point: oblique rami fractures on injury imaging suggest greater potential for later displacement and warrant examination under anaesthesia.
Morel-Lavallee Lesion in Pelvic Trauma
- Series of 24 closed internal degloving injuries associated with pelvic and acetabular fractures, classically over the greater trochanter (the Morel-Lavallee lesion).
- Cultures were positive in 46 percent of cases, and deep infection developed despite treatment - demonstrating the high contamination and wound-complication risk of operating through an unaddressed lesion.
- Recommended early thorough debridement before or at the time of fracture fixation, leaving the wound open with repeat debridement rather than primary closure.
Predictors of Mortality after Severe Pelvic Ring Fracture (Population-Based)
- Population-based registry study of 348 severe pelvic ring fractures; overall mortality was 19 percent.
- Independent predictors of death were age 65 years or older (adjusted OR 7.6), pre-hospital hypotension (adjusted OR 5.5), hypotension on arrival (adjusted OR 3.7) and severe chest injury (adjusted OR 2.8).
- Definitive hospital of management did not affect mortality once these factors were accounted for, underscoring that haemodynamic control - not the choice of centre - drives survival.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 45-year-old male pedestrian struck by a car presents with lateral pelvic pain. X-ray shows left pubic rami fractures. How would you assess and manage this patient?"
Initial Assessment:
- Primary survey with hemodynamic assessment
- Pelvic stability test (ONCE, gently)
- Neurovascular examination of lower limbs
- Look for associated head injury (same mechanism)
- Examine for Morel-Lavallee lesion over trochanter
- Check for open injury (perineum, vagina, rectum)
Imaging:
- AP pelvis X-ray shows rami fractures - anterior ring injury confirmed
- CT pelvis is MANDATORY to identify posterior injury
- Look for sacral impaction (LC-I) or crescent fracture (LC-II)
- Check for contralateral APC component (LC-III)
Classification:
- LC-I: Rami + sacral impaction = stable, usually conservative
- LC-II: Rami + crescent fracture = assess stability
- LC-III: Windswept = unstable, needs surgery
Management:
- If LC-I: Conservative - analgesia, DVT prophylaxis, mobilize as tolerated
- If LC-II/III: Discuss surgical fixation options
- Address associated injuries
- Follow-up imaging at 6 weeks
"How do you differentiate LC-I, LC-II, and LC-III injuries? What determines stability?"
LC-I (Most Common, Stable):
- Anterior: Ipsilateral pubic rami fractures
- Posterior: Sacral impaction fracture (usually Zone 1)
- Mechanism: Lower energy lateral compression
- Stability: Rotationally AND vertically stable
- Treatment: Usually conservative
LC-II (Variable Stability):
- Anterior: Ipsilateral pubic rami fractures
- Posterior: Crescent fracture (posterior ilium)
- Mechanism: Higher energy than LC-I
- Stability: Variable - SI joint partially disrupted
- Treatment: Assess stability, consider fixation
LC-III (Windswept, Unstable):
- Anterior: Often bilateral rami or symphysis disruption
- Posterior: LC pattern one side, APC pattern contralateral
- Mechanism: Continued force rolls pelvis through
- Stability: Rotationally UNSTABLE
- Treatment: Surgical fixation required
Key Point:
The posterior ring determines stability. In LC-I, the posterior ligaments are intact despite the sacral fracture. In LC-II, the crescent fracture partially disrupts the posterior complex. In LC-III, bilateral rotational injuries make the pelvis completely rotationally unstable.
"A patient with an LC injury has fluctuance and bruising over the greater trochanter. What is this and how do you manage it?"
Diagnosis:
- Clinical suspicion with bruising/fluctuance over trochanter
- May be occult initially - can present late
- MRI is investigation of choice
- Shows fluid collection between subcutaneous fat and fascia
Significance:
- Large cavity prone to hematoma formation
- Risk of infection and delayed wound healing
- Can compromise surgical incisions if not addressed
- May need drainage or debridement
Management:
- Identify before any surgical intervention
- Avoid incisions through the lesion if possible
- Drainage options: Percutaneous aspiration (may need repeated), open drainage
- Consider dead space management (suction drain, quilting sutures)
- Debride necrotic tissue if present
- May delay definitive fixation if extensive
Key Point:
Always examine for Morel-Lavallee lesion in LC injuries. Missing it can lead to wound complications, infection, and failed surgery. MRI before surgery if suspected.
MCQ Practice Points
High-Yield Exam Facts
Classification Essentials:
- LC injuries are the MOST COMMON pelvic ring injury pattern (50-60%)
- LC causes INTERNAL rotation - pelvis narrows (opposite of APC)
- LC-I = rami + sacral impaction = STABLE
- LC-II = rami + crescent fracture = VARIABLE stability
- LC-III = windswept pelvis = UNSTABLE (requires surgery)
Mechanism and Physics:
- Lateral force causes internal rotation deformity
- Pelvis volume DECREASES (vs APC which increases)
- Generally LESS hemorrhage than APC (pelvis closes and tamponades)
- But DON'T be complacent - can still bleed significantly
Associated Injuries:
- Head injuries COMMON - same lateral impact mechanism
- Morel-Lavallee lesion - closed degloving over trochanter
- Acetabular fractures (same mechanism)
- Neurological injury with sacral fractures (L5-S1 roots)
Diagnostic Points:
- CT scan is MANDATORY for all pelvic ring injuries
- Sacral impaction often OCCULT on X-ray - need CT
- Look for crescent fracture on CT (LC-II)
- Always check contralateral side (don't miss LC-III)
- MRI for Morel-Lavallee lesion if suspected
Treatment Principles:
- LC-I: Conservative in vast majority (over 90%)
- LC-II: Assess stability - may need fixation
- LC-III: Surgical fixation REQUIRED
- Pelvic binder less effective for LC (pelvis already closed)
- Weight-bearing as tolerated for LC-I
- Protected weight-bearing 6 weeks for LC-II/III post-surgery
Complications to Know:
- DVT/PE risk HIGH - prophylaxis critical
- Morel-Lavallee can delay surgery or cause infection
- Neurological injury with Zone 2/3 sacral fractures
- SI joint arthritis long-term
- Malunion more common than non-union
Common Exam Traps:
- Confusing LC with APC (LC = internal rotation, APC = external rotation)
- Missing sacral impaction on X-ray (need CT)
- Not recognizing LC-III (check both sides)
- Thinking pelvic binder helps LC (actually may worsen internal rotation)
- Assuming LC injuries don't bleed (they can, just less than APC)
Key Numbers:
- 50-60% = proportion of all pelvic ring injuries that are LC
- 70% = proportion of LC injuries that are LC-I
- 90% = proportion of LC-I that return to full function
- 6 weeks = typical protected weight-bearing period post-surgery
- 8-12 weeks = typical union time
Examiner Favorites:
- "What is the most common pelvic ring injury?" = Lateral compression
- "How does the pelvis deform in LC?" = Internal rotation, pelvis narrows
- "Why do LC injuries bleed less?" = Pelvis closes, tamponades bleeding
- "What must you look for on CT in LC?" = Sacral impaction/crescent fracture
- "When does LC-I need surgery?" = Rarely - usually conservative
LC vs APC
Q: How do you differentiate LC from APC injuries clinically and radiologically? A: LC = Lateral force causing INTERNAL rotation with pelvis narrowing. APC = Anteroposterior force causing EXTERNAL rotation with pelvis opening. LC has LESS bleeding than APC because the pelvis closes and tamponades. On X-ray, LC shows rami fractures with sacral impaction, APC shows symphysis widening.
Sacral Fractures on Imaging
Q: Why is CT mandatory in suspected LC pelvic injuries? A: Sacral impaction fractures in LC-I are often OCCULT on plain X-rays and easily missed. CT is mandatory to identify the posterior injury, classify the pattern accurately, and guide treatment decisions. Never rely on X-ray alone for pelvic ring injuries.
LC-I Management
Q: When does LC-I require surgical fixation? A: LC-I injuries are stable and rarely need surgery (under 10%). Over 90% can be safely managed conservatively with excellent outcomes. Indications for surgery include clinical instability on examination, polytrauma requiring early mobilization, or significant displacement causing pelvic deformity.
Morel-Lavallee Recognition
Q: What is a Morel-Lavallee lesion and why is it important? A: Closed internal degloving injury over the greater trochanter caused by the same lateral shearing force as LC injury. Creates large fluid collection between subcutaneous fat and fascia. Must identify with MRI before surgery to prevent wound complications, infection, and surgical failure.
Associated Head Injury
Q: What associated injury must you screen for in LC pelvic fractures? A: Head injury is very common with LC mechanism because the same lateral impact that hits the pelvis also impacts the head. Always perform thorough neurological assessment and maintain high index of suspicion for intracranial injury. Order head CT liberally.
LC-III Diagnosis
Q: What defines an LC-III injury and why is it important? A: LC-III is "windswept pelvis" - LC pattern on one side with contralateral APC pattern. This is rotationally UNSTABLE (unlike LC-I and LC-II) and requires surgical fixation. Don't miss it by failing to check the contralateral side - always assess both hemipelves carefully.
Guidelines, Registries & Global Practice
OrthoVellum is a worldwide resource: this section gives the global standard of care for lateral compression injuries plus the regional differences a candidate may be examined on. Lateral compression is the most common pelvic ring pattern internationally, and the principles below apply across all major trauma systems.
Global Epidemiology
| Parameter | Evidence | Source |
|---|---|---|
| LC as proportion of high-energy pelvic ring injuries | Largest single mechanism group; Type A and B (which contain most LC) make up 70-80% of all pelvic injuries | Tile 1996 (PMID 10795049) |
| Dominant mechanisms | Motor vehicle / motorcycle collisions; majority of high-energy series | Burgess 1990 (PMID 2381002) |
| Blood replacement, LC vs APC | LC mean 3.6 units vs APC 14.8 units | Burgess 1990 (PMID 2381002) |
| Mortality, severe pelvic ring fracture | 19% population-based; LC subgroup 7.0% in the original series | Gabbe 2011 (PMID 21733513); Burgess 1990 |
| Mortality predictors | Age greater than or equal to 65 (OR 7.6), pre-hospital hypotension (OR 5.5), severe chest injury (OR 2.8) | Gabbe 2011 (PMID 21733513) |
A second, growing population is the elderly low-energy fragility fracture of the pelvis, which is rising with ageing populations worldwide and behaves differently from the high-energy LC injury above.
Major Guidelines Side by Side
| Body (region) | Recommendation for LC pelvic injury | Evidence basis |
|---|---|---|
| AO Foundation (international) | Classify by Young-Burgess and Tile/AO-OTA; nonoperative weight-bearing for stable LC-I, fixation for demonstrable rotational/vertical instability | Expert consensus; biomechanical and cohort data |
| BOA / BOAST (UK) | Pelvic ring injuries managed within a network; binder at greater trochanters pre-hospital; CT in the haemodynamically stable; definitive fixation at a specialist centre | BOAST "Pelvic and Acetabular Fracture" standards (consensus) |
| NICE NG37 (UK, complex fractures) | Pelvic binder for suspected unstable injury; CT for diagnosis in stable patients; major-haemorrhage protocol and IR/packing pathway for the unstable | NICE guideline (mixed evidence) |
| AAOS / OTA (US) | No formal LC-specific guideline; OTA practice favours stress examination of minimally displaced LC1 to triage operative vs nonoperative care | DeKeyser 2022 (PMID 34921551), Level II |
| WSES (international consensus) | Algorithmic haemorrhage control: binder, then angioembolisation and/or preperitoneal packing and external fixation by mechanism and response to resuscitation | WSES classification and guidelines (consensus) |
Key area of genuine convergence: stable LC-I is treated nonoperatively with early weight-bearing; key area of evolving practice: how aggressively to detect occult instability in LC-1 with a complete sacral fracture (stress examination vs early fixation).
Registry and Trauma-System Evidence
- Trauma registries (e.g. the UK TARN and the Victorian State Trauma Registry) define the small, resource-intensive subgroup of haemodynamically unstable pelvic ring injuries and have shown that survival is driven by haemodynamic control rather than which centre delivers definitive care (Gabbe 2011, PMID 21733513).
- Joint-replacement registries (NJR, AJRR, AOANJRR) are not applicable to acute LC fixation; registry evidence here comes from trauma rather than arthroplasty registries.
Global Practice Variation
| Setting | Typical practice | Reason |
|---|---|---|
| High-resource trauma systems | Pre-hospital binders, 24/7 CT, interventional radiology, percutaneous SI screws under fluoroscopy/navigation | Mature networks and imaging access |
| Limited-resource settings | Binder/sheet, external fixation and preperitoneal packing favoured over angioembolisation; more nonoperative management | Limited IR and theatre access; emphasis on damage control |
| Ageing populations (worldwide) | Rising fragility fractures of the pelvis; lower threshold for fixation only if pain or progressive displacement | Demographic shift; poor bone quality |
Thromboprophylaxis (Global Principle)
Pelvic fractures carry a high venous thromboembolism risk, so combined mechanical and pharmacological prophylaxis is standard worldwide. Low-molecular-weight heparin is the usual agent, started once haemorrhage is controlled, with renal dose adjustment, plus intermittent pneumatic compression and early mobilisation. Extended prophylaxis (commonly up to 6 weeks, longer in high-risk patients) is recommended for major pelvic injury, in line with international guidance.
Lateral Compression Pelvic Injuries - Exam Quick Reference
Clinical summary
DEFINITION
- •Most common pelvic ring injury (50-60%)
- •Lateral force causes INTERNAL rotation
- •Pelvis NARROWS (vs APC which opens)
- •Named by direction of FORCE, not displacement
CLASSIFICATION
- •LC-I: Rami + sacral impaction (STABLE)
- •LC-II: Rami + crescent fracture (VARIABLE)
- •LC-III: Ipsi LC + contra APC = UNSTABLE
- •LC-III = windswept pelvis
KEY ASSOCIATIONS
- •Head injuries (same lateral mechanism)
- •Morel-Lavallee lesion (closed degloving)
- •Sacral fractures with nerve injury
- •Acetabular fractures
IMAGING
- •AP pelvis first
- •CT MANDATORY to classify
- •Look for sacral impaction (often occult)
- •MRI for Morel-Lavallee lesion
MANAGEMENT
- •LC-I: Usually conservative
- •LC-II: Assess stability, may need fixation
- •LC-III: Surgical fixation required
- •Less hemorrhage than APC but don't be complacent