Sports Medicine | Isolated Usually Non-Operative | Combined Injuries Need Surgery | PLC Assessment Critical
LCL INJURY GRADING
Critical Must-Knows
- LCL is primary varus stabilizer - especially at 30° flexion when cruciate contribution minimal
- Isolated LCL injuries are RARE - always assess for PLC injury (popliteus, popliteofibular ligament)
- Varus stress test at 0° and 30° - opening at 0° indicates combined cruciate injury
- Peroneal nerve at risk - courses around fibular neck, assess with every lateral knee injury
- Combined injuries require surgery - isolated Grade III may heal non-operatively, combined do not
Clinical Pearls
- "LCL injury with varus opening at 0° = combined PCL/ACL injury until proven otherwise
- "Always document peroneal nerve function BEFORE any intervention
- "MRI essential to assess PLC structures - isolated LCL rare, combined common
- "Fibular head avulsion is pathognomonic of LCL injury - check X-ray carefully
Critical LCL Injury Exam Points
Isolated LCL is RARE
Truly isolated LCL injuries are rare - the great majority of lateral-sided injuries involve the posterolateral corner. When you see lateral instability, always examine for posterolateral corner (PLC) injury. The triad of LCL + popliteus + popliteofibular ligament = complete PLC injury requiring reconstruction.
Peroneal Nerve Risk
Common peroneal nerve wraps around fibular neck - directly adjacent to LCL insertion. Document motor (ankle dorsiflexion, toe extension) and sensory (first web space) function. Peroneal nerve injury occurs in around a quarter of knee dislocations with posterolateral disruption (25%, Niall et al, 2005).
Varus at 0° = Combined Injury
At full extension, cruciates provide secondary varus restraint. If varus opens at 0°, you have combined LCL + cruciate injury (usually PCL). This CANNOT be managed non-operatively - needs surgical reconstruction.
Surgery vs Conservative
Isolated Grade I-II: Conservative (hinged brace, PT). Isolated Grade III: May heal non-operatively with bracing. Combined LCL + PLC or cruciate: Surgical reconstruction required for functional stability.
At a Glance - LCL Injury Management
| Grade | Clinical Finding | Stability Testing | Treatment |
|---|---|---|---|
| Grade I (Sprain) | Lateral tenderness, no laxity | Under 5mm varus opening at 30°, firm endpoint | Functional brace 1-2 weeks, early ROM, PRICE |
| Grade II (Partial) | Moderate pain, mild laxity | 5-10mm varus opening at 30°, endpoint present | Hinged brace 4-6 weeks, protected WB, PT |
| Grade III Isolated | Severe pain, significant laxity | Over 10mm opening at 30° only, no endpoint | Bracing 6-8 weeks may suffice - assess healing at 6 weeks |
| Grade III + PLC | Posterolateral rotatory instability | Varus + external rotation asymmetry, + dial test | Surgical reconstruction (LCL + PLC) |
| Combined + Cruciate | Multi-ligament knee injury | Varus opening at 0° AND 30° | Staged or simultaneous multi-ligament reconstruction |
FIBLCL Anatomy - 'FIB'
| F | From lateral epicondyle Origin at lateral femoral epicondyle, anterior and distal to popliteus |
| I | Inserts on fibular head Attaches to lateral aspect of fibular head (arcuate sign on X-ray) |
| B | Biceps femoris conjoint Shares insertion area with biceps femoris tendon |
| F | From lateral epicondyle Origin at lateral femoral epicondyle, anterior and distal to popliteus |
| I | Inserts on fibular head Attaches to lateral aspect of fibular head (arcuate sign on X-ray) |
| B | Biceps femoris conjoint Shares insertion area with biceps femoris tendon |
Hook:FIB = Fibula is where LCL ends. Think of a fib (lie) - isolated LCL injury is a 'fib', usually combined!
LPPPLC Structures - 'LPP'
| L | LCL Primary static varus stabilizer, taut at 30° flexion |
| P | Popliteus Dynamic stabilizer, resists external rotation, posterolateral corner anchor |
| P | Popliteofibular ligament Connects popliteus to fibular styloid, critical for PLC stability |
| L | LCL Primary static varus stabilizer, taut at 30° flexion |
| P | Popliteus Dynamic stabilizer, resists external rotation, posterolateral corner anchor |
| P | Popliteofibular ligament Connects popliteus to fibular styloid, critical for PLC stability |
Hook:LPP = All three make up the posterolateral corner. Like saying 'LP' (long play) Plus - you need all three!
ZERO-THIRTYVarus Stress Test - 'ZERO THIRTY'
| Z | Zero degrees Tests LCL + cruciates combined - opening = combined injury |
| E | Extension locks cruciates At 0°, cruciates provide secondary varus restraint |
| R | Record opening Compare to opposite side - under 5mm/5-10mm/over 10mm |
| O | Open at 0° = combined Cannot isolate LCL injury if opens at extension |
| T | Thirty degrees flexion Isolates LCL (cruciates relax), most sensitive test |
| H | Hold thigh stable Stabilize femur, apply varus force to ankle |
| I | Interpret opening Grade based on mm: I under 5, II 5-10, III over 10 |
| R | Record endpoint Firm = partial, soft/absent = complete tear |
| T | Test both sides Always compare to contralateral knee |
| Y | Yes to combined if 0° opens Cruciate injury confirmed if varus at extension |
| Z | Zero degrees Tests LCL + cruciates combined - opening = combined injury | O | Open at 0° = combined Cannot isolate LCL injury if opens at extension | I | Interpret opening Grade based on mm: I under 5, II 5-10, III over 10 | Y | Yes to combined if 0° opens Cruciate injury confirmed if varus at extension |
| E | Extension locks cruciates At 0°, cruciates provide secondary varus restraint | T | Thirty degrees flexion Isolates LCL (cruciates relax), most sensitive test | R | Record endpoint Firm = partial, soft/absent = complete tear | ||
| R | Record opening Compare to opposite side - under 5mm/5-10mm/over 10mm | H | Hold thigh stable Stabilize femur, apply varus force to ankle | T | Test both sides Always compare to contralateral knee |
Hook:Remember: TEST AT 30° to isolate LCL, TEST AT 0° to detect combined injuries
DANCEPeroneal Nerve Exam - 'DANCE'
| D | Dorsiflex ankle Test tibialis anterior - deep peroneal nerve motor |
| A | Assess eversion Test peroneus longus/brevis - superficial peroneal motor |
| N | Numbness first web space Deep peroneal sensory territory |
| C | Check dorsolateral foot Superficial peroneal sensory territory |
| E | Extend toes (EHL) Test extensor hallucis longus - deep peroneal |
| D | Dorsiflex ankle Test tibialis anterior - deep peroneal nerve motor | C | Check dorsolateral foot Superficial peroneal sensory territory |
| A | Assess eversion Test peroneus longus/brevis - superficial peroneal motor | E | Extend toes (EHL) Test extensor hallucis longus - deep peroneal |
| N | Numbness first web space Deep peroneal sensory territory |
Hook:Do the DANCE exam - if patient can't dance (foot drop), peroneal nerve is injured!
Overview and Epidemiology
Lateral Collateral Ligament (LCL) injuries are uncommon in isolation but frequently occur as part of complex multi-ligament knee injuries. The LCL is the primary static stabilizer against varus stress at the knee, working in concert with the posterolateral corner structures.
Key epidemiological points:
- Isolated LCL injuries are rare - most lateral-sided injuries occur with PLC and/or cruciate damage
- Sports-related: Contact sports (rugby, AFL, American football), skiing
- Mechanism: Varus force to weight-bearing knee, often with rotation
- Peak incidence: Males aged 20-40 years in contact sports
- Australian context: Common in Australian Rules Football due to tackle mechanisms
Clinical significance: The LCL cannot be considered in isolation. Injury to the lateral structures almost always involves the posterolateral corner, and recognition of this combined injury pattern is critical for appropriate management. Failure to identify and treat PLC injuries leads to residual instability and reconstruction failure.
Pathophysiology and Mechanisms
LCL Structure:
- Origin: Lateral femoral epicondyle, anterior and distal to popliteus origin
- Insertion: Lateral aspect of fibular head, conjoint with biceps femoris
- Length: Approximately 60mm
- Width: 5-8mm (round, cord-like structure)
- Course: Extra-articular (unlike MCL, not attached to capsule or meniscus)
Key anatomical relationships: The LCL is separated from the joint by the popliteus tendon. The common peroneal nerve passes 10mm posterior to biceps tendon insertion. The lateral inferior genicular artery runs beneath the LCL. Unlike the MCL, the LCL is not attached to the lateral meniscus (the meniscus has popliteomeniscal fascicles instead).


Clinical Pearl
The LCL is extra-articular and not attached to the lateral meniscus - this is why isolated LCL injuries don't cause meniscal damage. Compare to MCL which is intimately related to the medial meniscus.
Classification Systems
LCL Injury Classification
LCL Injury Classification
| Grade | Pathology | Varus Stress at 30° | Clinical Features |
|---|---|---|---|
| Grade I | Microscopic fiber damage, ligament intact | Under 5mm opening, firm endpoint | Tenderness, no instability, full ROM |
| Grade II | Partial macroscopic tear, some fibers intact | 5-10mm opening, endpoint present | Pain with varus stress, mild laxity |
| Grade III | Complete tear (midsubstance or avulsion) | Over 10mm opening, no endpoint | Gross laxity, may be painless (complete disruption) |
Grading is based on varus stress testing at 30° flexion to isolate the LCL.
History
Mechanism of injury:
- Varus force to weight-bearing knee (tackle from medial side)
- Non-contact hyperextension with varus moment
- Dashboard injury with knee flexed and externally rotated
- Twisting injury with foot planted
Symptoms:
- Lateral knee pain (worse with varus stress)
- Feeling of instability, especially pivoting/cutting
- "Knee giving way" with combined injuries
- Pop or snap at time of injury (less common than ACL)
Key questions to ask: Was it contact or non-contact mechanism? What was the direction of force? Was there immediate swelling (suggests cruciate involvement)? Was the patient able to weight-bear after injury? Any previous knee injuries? What are the sport and activity demands?
Examination
Inspection:
- Lateral ecchymosis (posterolateral suggests PLC)
- Effusion (intra-articular = cruciate involvement)
- Gait assessment (varus thrust in chronic injuries)
Palpation:
- LCL along its course (epicondyle to fibular head)
- Fibular head (avulsion tenderness)
- Lateral joint line
- Peroneal nerve at fibular neck
- Popliteal fossa (popliteus)
Special tests for LCL/PLC injury:
1. Varus stress test (most important) - Test at 0° extension AND 30° flexion. Grade opening as: I (under 5mm), II (5-10mm), III (over 10mm). Note endpoint quality (firm vs soft).
2. Dial test (external rotation) - Test at 30° and 90° flexion, compare ER asymmetry to contralateral side. Over 10° asymmetry at 30° only indicates isolated PLC injury. Over 10° at both 30° and 90° indicates combined PLC plus PCL injury.
3. Posterolateral drawer - At 90° flexion, apply posterior force with external rotation. Positive test indicates PLC injury.
4. Reverse pivot shift - Extend knee from flexion with valgus and external rotation. A reduction clunk indicates PLC laxity and posterolateral rotatory instability.
Peroneal Nerve Documentation
Always document peroneal nerve function (dorsiflexion power, first web space sensation) BEFORE any intervention including bracing, examination under anaesthesia, or surgery. Medicolegal significance is high.
Differential Diagnosis of Lateral Knee Instability/Pain
Differential Diagnosis - Lateral-Sided Knee Injury
| Condition | Distinguishing Features | Key Test/Investigation |
|---|---|---|
| Isolated LCL injury | Varus laxity at 30° only, normal rotation, varus stable at 0° | Varus stress at 0° and 30°; MRI confirms isolated FCL |
| Posterolateral corner (PLC) injury | Varus laxity plus increased external rotation; posterolateral rotatory instability | Dial test (over 10° asymmetry at 30°), posterolateral drawer, reverse pivot shift |
| Combined PLC + PCL injury | Posterior sag, increased ER at BOTH 30° and 90° | Dial test at 30° and 90°; posterior drawer; MRI |
| Knee dislocation / multiligament injury | Gross multidirectional instability, high-energy mechanism, neurovascular risk | ABI, CT angiography, peroneal nerve exam, MRI |
| Iliotibial band syndrome | Lateral pain with activity, no instability, tender over lateral epicondyle | Noble/Ober tests; no varus laxity |
| Lateral meniscus tear | Joint-line pain, mechanical catching/locking, no varus laxity | McMurray/Thessaly; MRI |
| Proximal fibula / fibular head fracture | Focal fibular tenderness, possible peroneal nerve signs | AP/lateral X-ray; assess associated LCL avulsion (arcuate sign) |
Investigations
Standard views:
- AP, lateral, skyline views
- Bilateral weight-bearing if chronic
- Stress views if diagnosis uncertain
Findings:
- Arcuate sign: Fibular styloid avulsion (pathognomonic of PLC injury)
- Segond fracture: Lateral tibial avulsion (anterolateral capsule - suggests ACL injury)
- Lateral capsular avulsion
- Fibular head fracture
- Varus alignment (chronic deficiency)
Stress X-rays: Varus stress at 20° flexion with side-to-side comparison. A difference over 4mm is significant. Useful for pre-operative planning and documenting degree of instability.

Clinical Pearl
The "arcuate sign" (avulsion of fibular styloid process) on X-ray is pathognomonic of PLC injury. Don't miss this - look carefully at the fibular head on every lateral knee X-ray!
Non-Operative Management
Indications for conservative management:
- Grade I injuries (all)
- Grade II injuries (most)
- Isolated Grade III injuries (selected cases)
- Elderly/low-demand patients
- Significant medical comorbidities
Acute phase (Week 0-1):
- PRICE protocol (Protection, Rest, Ice, Compression, Elevation)
- Functional hinged brace (optional)
- Weight-bearing as tolerated
- NSAIDs for pain/inflammation
Recovery phase (Week 1-3):
- ROM exercises (aim full ROM by 2 weeks)
- Quadriceps and hamstring strengthening
- Proprioception exercises
- Stationary cycling
Return to sport (Week 3-6):
- Sport-specific drills
- Functional brace for contact sports initially
- Full return when strength 90% and no pain with stress
Expected outcome: Full recovery, 2-4 weeks typical
Management Algorithm
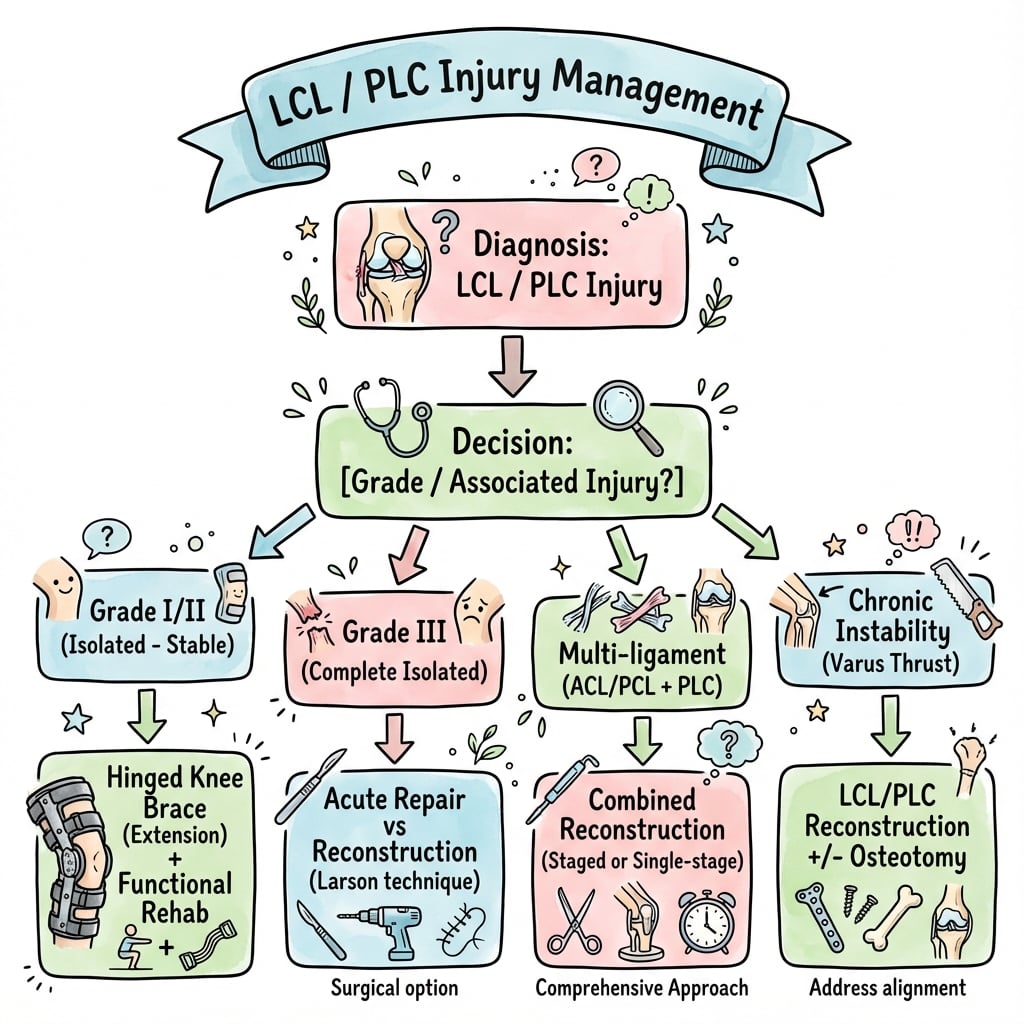
LCL Injury Management Decision Tree
| Injury Pattern | Initial Assessment | Management | Timeline |
|---|---|---|---|
| Grade I Isolated | Under 5mm varus, firm endpoint | Functional treatment, early ROM | Return 2-4 weeks |
| Grade II Isolated | 5-10mm varus, endpoint present | Hinged brace 4-6 weeks, PT | Return 6-12 weeks |
| Grade III Isolated | Over 10mm varus at 30° only | Trial bracing 6-8 weeks, reassess | Surgery if persistent laxity |
| Grade III + PLC | Varus + external rotation asymmetry | Surgical reconstruction (LCL + PLC) | Surgery within 2-3 weeks ideal |
| Combined + Cruciate | Varus at 0° AND 30°, + cruciate tests | Multi-ligament reconstruction | Staged or single-stage, surgeon preference |
Treatment decisions are based on injury severity, associated structures, and patient demands.

Surgical Management
Absolute surgical indications:
- Combined LCL + PLC injury (Fanelli B/C)
- Combined LCL + cruciate injury
- Multi-ligament knee injury
- Bony avulsion with displacement (repair/fixation)
- Peroneal nerve injury requiring exploration
- Failed non-operative treatment of isolated Grade III
Relative surgical indications:
- High-demand athlete with isolated Grade III
- Persistent symptomatic instability
- Varus thrust gait in chronic injury
Timing: Acute injuries (under 3 weeks) allow primary repair or augmented repair. Subacute injuries (3-6 weeks) can be repaired if tissue quality is adequate. Chronic injuries (over 6 weeks) require reconstruction as tissue is not repairable.
Complications
Complications of LCL Injuries and Treatment
| Complication | Risk Factors | Prevention/Management |
|---|---|---|
| Peroneal nerve injury | Grade III injury, posterolateral trauma, fibular fracture | Document pre-op function, careful dissection, explore if no recovery by 3 months |
| Residual instability | Missed PLC injury, inadequate reconstruction, non-anatomic repair | Complete assessment pre-op, anatomic reconstruction technique |
| Stiffness | Prolonged immobilization, associated intra-articular injury | Early ROM, avoid over-tensioning graft |
| Varus thrust gait | Chronic instability, failed treatment | Correct with reconstruction, may need HTO for varus malalignment |
| Cruciate reconstruction failure | Untreated posterolateral instability | Always address PLC with cruciate reconstruction |
Critical point: Untreated posterolateral corner injury is the most common cause of ACL and PCL reconstruction failure. The lateral structures must be addressed to protect cruciate grafts.
Postoperative Care
Hinged brace locked at 0°, toe-touch weight-bearing, ice and elevation, gentle quad sets, ankle pumps. No active hamstring exercises (protects PLC repair).
Progress ROM in brace (0-90° by week 4, full by week 6), progress to 50% weight-bearing by week 4, stationary cycling, pool exercises, continue quad strengthening.
Full weight-bearing, wean from brace by week 8, closed chain exercises, proprioception training, progress strengthening, avoid pivoting/cutting.
Sport-specific training progression, agility drills (straight-line first, then cutting), plyometrics, functional testing at 6 months.
Full return when passing functional tests (hop tests over 90%, isokinetic strength over 85%), sport-specific brace recommended for first season, ongoing maintenance program.
Clinical Pearl
Avoid active hamstring exercises in early postoperative period - the biceps femoris inserts with the LCL and can stress the reconstruction. Quad-dominant rehabilitation initially.
Outcomes and Prognosis
Non-operative outcomes:
- Grade I: 100% return to sport, no residual laxity
- Grade II: 95%+ return to sport, minimal residual laxity
- Isolated Grade III: 70-80% satisfactory with bracing, 20-30% need delayed surgery
Surgical outcomes:
| Procedure | Return to Sport | Stability Restoration | Complications |
|---|---|---|---|
| Acute LCL repair | 85-90% | 90%+ | Under 5% |
| Chronic LCL reconstruction | 75-85% | 80-90% | 5-10% |
| Combined LCL/PLC reconstruction | 70-80% | 75-85% | 10-15% |
| Multi-ligament reconstruction | 60-75% | 70-85% | 15-20% |
Factors affecting outcome:
- Positive: Acute surgery, isolated injury, young patient, anatomic technique
- Negative: Chronic injury, multi-ligament, varus alignment, nerve injury
Access to care (Australia):
- Private health insurance generally covers reconstruction
- Public hospital wait times may delay optimal surgical timing for combined and multiligament injuries
- Regional patients often require transfer to metropolitan centres for complex reconstruction
Evidence Base
LaPrade Anatomic Two-Graft PLC Reconstruction (Landmark Technique)
- Cadaveric study (10 specimens): two-graft technique anatomically reconstructs FCL, popliteus tendon and popliteofibular ligament
- Reconstruction significantly improved varus stability versus the cut (Grade III) state at 0°, 30°, 60° and 90° of flexion
- No significant difference in external rotation between intact and reconstructed knees at any flexion angle
- Provided the biomechanical basis for the modern anatomic PLC reconstruction
PLC Repair versus Reconstruction (Stannard)
- Prospective cohort of 64 PLC tears (39 repairs, 25 reconstructions; minimum 24-month follow-up)
- Acute primary repair failed in 13 of 35 (37%) versus 2 of 22 (9%) for reconstruction (statistically significant)
- Reconstruction using the modified two-tailed technique gave significantly better stability than repair
- Authors now favour reconstruction over repair for most high-energy PLC tears
PLC Injuries: A Serious Injury Commonly Missed (Pacheco)
- Retrospective review of 68 referred PLC injuries; injury was not identified at initial presentation in 49 of 68 patients (72%)
- Mean delay to correct diagnosis was 30 months from time of injury
- MRI correctly identified 14 of 15 injuries when performed within 12 weeks, but only 4 of 15 when performed later
- PLC injury was usually recognised only when severe multiligament injury was present
Untreated Grade III PLC Injury Increases ACL Graft Force (LaPrade)
- Cadaveric biomechanical study of ACL-reconstructed knees with sequential sectioning of the FCL, popliteofibular ligament and popliteus tendon
- ACL graft force was significantly higher after FCL sectioning during varus loading at both 0° and 30° of flexion
- Coupled varus and internal rotation moments increased graft force further beyond varus alone
- Supports the clinical observation that untreated Grade III PLC injury contributes to ACL graft failure
Common Peroneal Nerve Palsy After Knee Dislocation (Niall)
- Common peroneal nerve injury in 14 of 55 patients (25%) with knee dislocation; all had posterolateral structure disruption
- Palsy occurred in 14 of 34 (41%) of those with combined bicruciate and posterolateral injury
- Complete recovery in only 3 (21%) and partial useful motor recovery in 4 (29%); no useful recovery in 7 (50%)
- Lesions in continuity under 7 cm long recovered within 6 to 18 months
Posterolateral Attachments of the Knee: Surgical Anatomy (LaPrade)
- Cadaveric morphologic study (10 knees) quantifying attachments of the FCL, popliteus tendon and popliteofibular ligament
- FCL femoral attachment averaged 1.4 mm proximal and 3.1 mm posterior to the lateral epicondyle; fibular attachment 8.2 mm posterior to the anterior fibular head
- Popliteus tendon femoral attachment was consistently anterior to the FCL (mean separation 18.5 mm)
- Popliteofibular ligament had constant anterior and posterior divisions at the fibular styloid
Return to Play After Multiligament Knee Injury in NFL Athletes (Bakshi)
- Retrospective cohort of 50 NFL athletes; overall return-to-play rate 64%
- Athletes with ACL and PCL/LCL injury had a lower RTP rate (55.6%) and longer recovery than ACL/MCL injuries (70.8%)
- Mean time to RTP was 459 days for combined ACL and PCL/LCL injury versus 305 days for ACL/MCL injury
- Lateral-sided and bicruciate injury patterns carry a worse prognosis than medial-sided patterns
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Acute Grade III LCL with Peroneal Nerve Palsy
"25-year-old rugby player presents after a tackle from the medial side. Has lateral knee pain and weakness of ankle dorsiflexion. X-ray shows fibular styloid avulsion (arcuate sign). Varus stress at 30° shows over 10mm opening. Varus at 0° is normal."
Structured approach:
- Immediate assessment: Document complete neurological exam - motor (dorsiflexion MRC grade), sensory (first web space), vascular status
- Diagnosis: Grade III LCL injury with fibular avulsion (arcuate sign) and peroneal nerve neuropraxia. Likely isolated LCL (varus stable at 0°) but need MRI to assess PLC
- Investigations: MRI to assess PLC structures, confirm isolated vs combined injury
- Management:
- If isolated LCL with bony avulsion: ORIF of fibular avulsion fragment (restores LCL tension)
- Explore peroneal nerve intraoperatively - decompress if in continuity
- Hinged brace postoperatively, early ROM
- Nerve management: If neurapraxia - expect recovery, monitor clinically. If no recovery by 3 months, nerve conduction studies and consider exploration
- Follow-up: Clinical review at 2, 6, 12 weeks. Assess stability and nerve recovery
Combined LCL/PLC Injury
"30-year-old AFL player has lateral knee injury. Varus stress positive at 30° (Grade III). Dial test shows 15° external rotation asymmetry at 30° but not at 90°. What is your diagnosis and management?"
Analysis:
- Dial test interpretation: Asymmetry at 30° but NOT at 90° indicates isolated PLC injury (PCL intact). Asymmetry at both 30° and 90° would indicate combined PCL/PLC
- Diagnosis: Grade III LCL injury with posterolateral corner (PLC) injury - Fanelli Type C (complete PLC)
Management:
- MRI: Confirm PLC structures involved (popliteus, popliteofibular ligament)
- Surgical reconstruction: This CANNOT be managed non-operatively. Combined PLC injuries do not heal and lead to chronic instability
- Timing: Ideally within 2-3 weeks for best outcomes
- Technique: LaPrade anatomic reconstruction - two grafts (LCL + popliteofibular ligament) or Larson technique (single graft)
- Rehabilitation: Protected weight-bearing 4-6 weeks, brace for 8 weeks, avoid hamstring exercises early, return to sport 6-9 months
Failed ACL Reconstruction with Lateral Laxity
"A 28-year-old presents 18 months after ACL reconstruction with recurrent instability. Original MRI showed isolated ACL tear. Examination shows 2+ Lachman and Grade II varus laxity. What happened?"
Analysis:
- Key point: Untreated posterolateral corner deficiency is the most common cause of ACL reconstruction failure
- What happened: PLC injury was missed at initial presentation. The lateral laxity stressed the ACL graft, leading to stretching/failure
- Why missed: PLC injuries can be subtle on MRI and examination when patient is guarding
Management now:
- Investigations: New MRI to assess ACL graft (stretched vs ruptured), PLC structures, alignment
- Standing alignment X-rays: Check for varus malalignment (may need HTO)
- Surgical plan:
- Revision ACL reconstruction (new tunnels if needed)
- Concurrent PLC reconstruction (LaPrade technique)
- If varus alignment over 3°: Staged or concurrent HTO
- Key learning: ALWAYS examine for PLC injury with ACL tears - dial test, varus stress at 30°. Address lateral corner at time of ACL reconstruction
Chronic Varus Thrust Gait
"45-year-old presents with lateral knee pain and 'knee bowing outward' when walking. History of knee injury 5 years ago, managed conservatively. Standing alignment shows 8° varus. Stress testing shows Grade II varus laxity."
Diagnosis: Chronic PLC/LCL deficiency with secondary varus malalignment and early lateral compartment OA
Assessment:
- Weight-bearing long leg alignment films
- MRI: Assess LCL/PLC, lateral compartment cartilage, meniscus
- Stress X-rays to quantify laxity
Management considerations:
- If minimal OA, symptomatic instability:
- High tibial osteotomy (HTO) to correct alignment first
- Staged or concurrent PLC reconstruction
- HTO unloads lateral compartment and reduces stress on reconstruction
- If significant lateral OA:
- May need to consider arthroplasty in future
- Instability reconstruction less likely to succeed with OA
- Rehabilitation:
- Quadriceps strengthening (reduces varus thrust)
- Lateral heel wedge insoles (temporizing measure)
- Unloader brace
Key point: Chronic cases need alignment correction before or with ligament reconstruction.
MCQ Practice Points
Clinical Pearl
Q: What is the primary restraint to varus stress at 30 degrees knee flexion? A: The lateral collateral ligament (LCL) is the primary varus stabilizer, providing 69% of varus restraint at 25-30 degrees flexion. At this angle, the cruciates relax making the LCL the isolated primary restraint.
Clinical Pearl
Q: What does varus opening at both 0 and 30 degrees indicate? A: Combined injury to both the LCL AND the cruciate ligaments (particularly PCL). Opening only at 30 degrees suggests isolated LCL injury since the cruciates are taut at 0 degrees and contribute to varus restraint.
Clinical Pearl
Q: What is the dial test and what does asymmetry at 30 degrees only indicate? A: The dial test assesses external rotation of the tibia relative to the femur. Asymmetry greater than 10 degrees at 30 degrees ONLY indicates isolated PLC injury. Asymmetry at BOTH 30 and 90 degrees indicates combined PLC plus PCL injury.
Clinical Pearl
Q: What is the arcuate sign? A: A small avulsion fracture of the fibular styloid on AP knee radiograph. It is pathognomonic of posterolateral corner (PLC) injury and indicates avulsion of the conjoint tendon insertion (LCL plus biceps femoris).
Clinical Pearl
Q: Why is untreated PLC injury important in ACL reconstruction? A: Untreated posterolateral corner instability is the NUMBER ONE cause of ACL graft failure. The abnormal tibial external rotation places excessive stress on the ACL graft, leading to elongation or rupture.
Clinical Pearl
Q: What is the relationship between the common peroneal nerve and the LCL? A: The common peroneal nerve passes approximately 10mm posterior to the biceps femoris tendon at the fibular head level. Peroneal nerve injury complicates around 25% of knee dislocations with posterolateral disruption (Niall et al, 2005).
Guidelines, Registries & Global Practice
Global epidemiology. Isolated LCL injury is rare; lateral-sided injuries usually involve the posterolateral corner and are frequently part of multiligament injury or frank knee dislocation. PLC injury is commonly missed at first presentation - Pacheco et al found it was unrecognised in 72% of referred cases, with a mean diagnostic delay of 30 months (J Bone Joint Surg Br, 2011). In knee dislocation, common peroneal nerve palsy complicates around 25% and is associated with posterolateral disruption (Niall et al, 2005). Sport-related cohorts confirm that lateral and bicruciate patterns carry a worse return-to-play prognosis than medial-sided injuries (Bakshi et al, Sports Health, 2018).
Guidance across major bodies. No society has published a high-level (Level I) standalone guideline for isolated LCL/PLC injury; recommendations are consensus-based and consistent internationally.
| Body | Region | Core guidance | Evidence level |
|---|---|---|---|
| AAOS / AOSSM | USA | Reconstruct (not repair) complete PLC tears; address PLC with concomitant cruciate reconstruction | Expert consensus / Level III-V |
| BOA / BASK | UK | Early specialist referral and MRI for suspected PLC; anatomic reconstruction for complete injury | Consensus |
| NICE | UK | No condition-specific guideline; general acute knee soft-tissue injury pathways apply | n/a |
| ESSKA | Europe | Anatomic reconstruction preferred over repair for chronic/complete PLC; treat associated cruciate injury | Consensus / Level III-V |
| AO Foundation | Global | Fix displaced fibular/arcuate avulsions; reconstruct chronic ligamentous deficiency | Expert opinion |
Registry evidence. Joint-replacement registries (AOANJRR, NJR, AJRR) do not capture isolated ligament reconstruction, so there is no national LCL/PLC implant-survival dataset; the evidence base remains cohort studies and biomechanical work. Multiligament and dislocation cohorts (including military and professional-sport series) provide the best available outcome data.
Practice variation. Surgeons increasingly favour anatomic two-graft reconstruction (after LaPrade) over older single-graft (Larson) techniques and over primary repair, reflecting Stannard's finding of higher failure with repair. Timing is convergent internationally: acute injuries are best addressed within roughly 2-3 weeks while primary repair/augmented repair remains feasible, with reconstruction reserved for chronic deficiency.
Australian context. LCL and PLC injuries are common in Australian contact sports (AFL, Rugby League, Rugby Union), typically from a medial-sided tackle producing a varus moment. Most complex PLC reconstructions are performed in the private sector at major sports-medicine centres in Melbourne, Sydney and Brisbane. Sports Medicine Australia publishes return-to-play position statements, and Australian surgeons generally follow ESSKA and AOSSM algorithms; rehabilitation is led by sports physiotherapists experienced in post-ligament-reconstruction protocols.
LCL INJURIES
Clinical summary
Key Numbers
- •30° flexion - optimal angle for varus stress testing (isolates LCL)
- •Under 5mm opening = Grade I, 5-10mm = Grade II, over 10mm = Grade III
- •Dial test: over 10° asymmetry at 30° = PLC injury; both 30° and 90° = PLC + PCL
- •Isolated LCL injury is uncommon - most lateral injuries involve the PLC
- •Peroneal nerve injury ~25% in knee dislocation with PLC disruption (Niall 2005)
Critical Concepts
- •Isolated LCL injury is RARE - always assess PLC
- •Varus opening at 0° = combined LCL + cruciate injury
- •Peroneal nerve documentation BEFORE any intervention is mandatory
- •Untreated PLC is #1 cause of ACL/PCL reconstruction failure
- •Acute repair/reconstruction (under 3 weeks) has better outcomes
Must-Know Anatomy
- •LCL: Lateral epicondyle to fibular head (extra-articular)
- •PLC triad: LCL + popliteus + popliteofibular ligament
- •Peroneal nerve: 10mm posterior to biceps tendon at fibular neck
- •Arcuate sign: Fibular styloid avulsion = PLC injury
Management Principles
- •Grade I-II isolated: Non-operative (brace, PT)
- •Grade III isolated: Trial bracing, surgery if fails
- •Combined LCL + PLC: Surgical reconstruction required
- •Combined + cruciate: Address all structures, PLC protects graft
- •Chronic instability + varus: HTO before or with reconstruction
Viva Pearls
- •Always examine BOTH 0° and 30° for varus stress
- •Dial test at 30° AND 90° differentiates PLC vs PLC+PCL
- •Check peroneal nerve before doing ANYTHING
- •Failed cruciate reconstruction - think missed PLC injury
- •Chronic varus thrust needs alignment correction first