Snowboarder Fracture | Subtalar Joint | ORIF vs Excision
McCRORY-BLADIN CLASSIFICATION
Critical Must-Knows
- Snowboarder fracture = dorsiflexion + inversion (often with axial load); now the commonest cause of this once-rare injury
- Often missed initially - radiographically occult, mimics a lateral ankle sprain; low threshold for CT (mortise view + CT)
- Displacement threshold: greater than 2mm articular step-off is the operative trigger to protect the subtalar joint
- ORIF for displaced, reconstructable fragments - mini/lag screws preserve the posterior facet
- Excision for small comminuted / non-reconstructable fragments - better than a painful malunion
- Look for concomitant injuries - peroneal tendon dislocation, calcaneal chondral lesions, subtalar subluxation are common
Clinical Pearls
- "Snowboarder fracture = dorsiflexion + inversion mechanism, classic snowboarding injury
- "Often missed initially - high index of suspicion needed, CT if X-ray negative but clinical suspicion
- "Displacement greater than 2mm requires ORIF to protect the subtalar joint
- "ORIF for reconstructable fragments, excision for small comminuted fragments
- "McCrory-Bladin (not Hawkins) is the classification - Hawkins is for talar NECK
Critical Lateral Process Talus Fracture Exam Points
Often Missed
Lateral process talus fractures are often missed initially - Look carefully on ankle mortise view. CT recommended if suspected clinically but X-ray negative. High index of suspicion needed, especially in snowboarders.
Displacement Threshold
Articular step-off greater than 2mm is the operative trigger - protects the subtalar joint. Truly non-displaced fractures are treated conservatively. ORIF for reconstructable fragments, excision for small comminuted ones.
Subtalar Arthritis Risk
Malunion or a missed fracture leads to subtalar osteoarthritis - the lateral process forms the lateral part of the posterior facet. Anatomic reduction is essential. Even well-treated displaced fractures carry meaningful late OA risk (von Knoch: 45% radiographic subtalar OA at 3.5 years).
Snowboarder Fracture
Classic snowboarding injury - Dorsiflexion + inversion mechanism. Snowboarders bindings prevent ankle motion, force transmitted to talus. High index of suspicion in snowboarders with lateral ankle pain.
McCrory-Bladin Classification - Quick Decision Guide
| Type | Description | Default Treatment | Notes |
|---|---|---|---|
| Type I | Large single fragment (subtalar + talofibular) | ORIF if displaced over 2mm | Reconstructable; lag/mini screws |
| Type II | Comminuted / multifragmentary | ORIF if reconstructable, else excise | Worst pattern for subtalar OA |
| Type III | Small chip / avulsion (anteroinferior, often extra-articular) | Conservative; late excision if symptomatic | Most common; easiest to miss as 'sprain' |
Classification trap
The lateral process fracture classification is McCrory-Bladin (1996). Do not confuse it with the Hawkins / Hawkins-Canale classification, which describes talar neck fractures. Earlier versions of this page used "Hawkins" - that was an error. The Tinner-Sommer (2018) modification subdivides the comminuted type into reconstructable versus non-reconstructable subtypes to guide ORIF versus excision.
SIDELateral Process Fracture Features
| S | Snowboarder Classic snowboarding injury |
| I | Inversion Dorsiflexion + inversion mechanism |
| D | Displacement Greater than 2mm requires ORIF |
| E | Excision For small comminuted fragments |
| S | Snowboarder Classic snowboarding injury | D | Displacement Greater than 2mm requires ORIF |
| I | Inversion Dorsiflexion + inversion mechanism | E | Excision For small comminuted fragments |
Hook:SIDE: Snowboarder, Inversion, Displacement threshold, Excision for small fragments!
LARGETreatment Decision
| L | Large fragment ORIF preferred |
| A | Arthritis prevention Anatomic reduction essential |
| R | Reconstructible ORIF if possible |
| G | Greater than 2mm Displacement threshold |
| E | Excision For small comminuted fragments |
| L | Large fragment ORIF preferred | G | Greater than 2mm Displacement threshold |
| A | Arthritis prevention Anatomic reduction essential | E | Excision For small comminuted fragments |
| R | Reconstructible ORIF if possible |
Hook:LARGE: Large fragment ORIF, Arthritis prevention, Reconstructible, Greater than 2mm threshold, Excision for small!
MISSComplications
| M | Missed diagnosis Often missed initially |
| I | Inadequate treatment Leads to subtalar arthritis |
| S | Subtalar arthritis Most common complication |
| S | Surgical complications Wound issues, nonunion |
| M | Missed diagnosis Often missed initially | S | Subtalar arthritis Most common complication |
| I | Inadequate treatment Leads to subtalar arthritis | S | Surgical complications Wound issues, nonunion |
Hook:MISS: Missed diagnosis, Inadequate treatment, Subtalar arthritis, Surgical complications!
Overview and Epidemiology
Lateral process talus fractures are uncommon but important injuries, classically associated with snowboarding. They involve the lateral process of the talus, which forms part of the subtalar joint. These fractures are often missed initially and can lead to subtalar arthritis if not properly treated.
Definition
Lateral process talus fracture: Fracture of the lateral process of the talus, which:
- Forms part of the subtalar joint (articulates with calcaneus)
- Provides lateral stability to the subtalar joint
- Can cause subtalar arthritis if malunited
Snowboarder fracture: Classic mechanism in snowboarders due to:
- Bindings prevent ankle motion
- Force transmitted to talus
- Dorsiflexion + inversion mechanism
Epidemiology
- Frequency: the lateral process is the second most commonly fractured part of the talus after the neck; historically rare but markedly more common with the rise of snowboarding ("snowboarder's ankle")
- Age: peak in young, active adults (snowboarding, falls, sport)
- Mechanism: dorsiflexion + inversion, often with axial loading; also high-energy falls and road trauma (it is NOT snowboard-exclusive)
- Diagnostic delay: a substantial proportion are missed at first presentation and labelled "ankle sprain" because the fracture is frequently radiographically occult
- Concomitant injuries (common, drive surgical decisions): peroneal tendon dislocation (~46%), calcaneal/subtalar chondral lesions (~48%), subtalar subluxation (~7%) — figures from the Hörterer review
Snowboarder Fracture
Lateral process talus fracture is the classic snowboarder fracture - Dorsiflexion + inversion mechanism. Snowboard bindings prevent ankle motion, so force is transmitted to talus. High index of suspicion in snowboarders with lateral ankle pain after fall.
Anatomy and Pathophysiology
Lateral Process Anatomy
Lateral process of talus:
- Location: Lateral aspect of talus body
- Function: Forms part of subtalar joint (articulates with calcaneus)
- Size: Variable, typically 1-2cm
- Blood supply: Branches from tarsal sinus artery
Subtalar joint:
- Articulation: Talus and calcaneus
- Lateral process: Part of posterior facet
- Function: Inversion/eversion, stability
Pathophysiology
Injury mechanism:
- Dorsiflexion + inversion: Classic snowboarding mechanism
- Force transmission: Through lateral process to calcaneus
- Fracture pattern: Varies from simple to comminuted
Why often missed:
- Subtle on X-ray: May be obscured by overlapping structures
- Misdiagnosed as sprain: Similar symptoms to ankle sprain
- CT needed: Often requires CT for diagnosis
Why displacement matters:
- Subtalar joint: Lateral process is part of subtalar joint
- Articular surface: Displacement causes joint incongruity
- Arthritis risk: Malunion leads to subtalar arthritis
Classification Systems
McCrory-Bladin Classification (1996)
The standard classification for lateral process fractures - based on fracture morphology, not displacement alone.
Type I — Large single fragment
- Single large fragment involving BOTH the subtalar (posterior facet) and talofibular articular surfaces
- Usually reconstructable
- Treatment: ORIF if displaced (greater than 2mm); cast if truly undisplaced
Type II — Comminuted fragment
- Multifragmentary involving subtalar and talofibular surfaces
- Worst pattern for late subtalar arthritis
- Treatment: ORIF if reconstructable, excision if not
Type III — Chip / avulsion fracture
- Small anteroinferior chip; frequently extra-articular
- Most common type, most easily missed as a "sprain"
- Treatment: conservative; late excision if it becomes a painful nonunion
Tinner-Sommer modification (2018) subdivides the comminuted type into reconstructable versus non-reconstructable (IIIc) to formalise the ORIF-versus-excision decision.
Clinical Assessment
History
Symptoms:
- Lateral ankle pain: Pain on lateral side of ankle
- Swelling: Localised to lateral ankle
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: Fall with dorsiflexion + inversion (snowboarding, sports)
Risk factors:
- Snowboarding (classic mechanism)
- High-energy trauma
- Sports with inversion injuries
Physical Examination
Inspection:
- Swelling on lateral ankle
- Ecchymosis (may be delayed)
- Deformity (rare, usually subtle)
Palpation:
- Tenderness over lateral process (anterior to lateral malleolus)
- Subtalar joint tenderness
- Ankle joint usually not tender
Range of Motion:
- Subtalar ROM limited and painful
- Ankle ROM may be limited
- Inversion/eversion painful
Special tests:
- Subtalar joint stress: Pain with inversion/eversion
- Ankle stability: Usually stable (not ankle sprain)
Clinical Examination Key Point
High index of suspicion needed - Lateral process fractures are often missed initially. Look carefully on ankle mortise view. CT recommended if suspected clinically but X-ray negative. Classic in snowboarders with lateral ankle pain.
Differential Diagnosis
The single biggest pitfall is calling this a "lateral ankle sprain." Point of maximum tenderness and imaging distinguish the differentials.
Differential Diagnosis of Lateral Hindfoot Pain After Inversion Injury
| Diagnosis | Key feature | Best test | Discriminator |
|---|---|---|---|
| Lateral process talus fracture | Tenderness ~1cm below/anterior to tip of lateral malleolus | Mortise radiograph + CT | Bony tenderness over the process; fracture on CT |
| Lateral ankle (ATFL) sprain | Tenderness over ATFL anterior to malleolus, no bony point tenderness | Clinical; stress films if unstable | No fracture; soft-tissue swelling only |
| Calcaneal anterior process fracture | Tenderness at sinus tarsi / anterior calcaneus | Oblique radiograph + CT | Fracture on calcaneus, not talus |
| Os trigonum / posterolateral process (Shepherd) fracture | Posterolateral pain, worse on plantarflexion | Lateral radiograph + CT | Posterior, not lateral, process |
| Subtalar dislocation/subluxation | Gross deformity or instability | Radiograph + post-reduction CT | Joint malalignment; often coexists |
| Peroneal tendon dislocation | Snapping behind lateral malleolus, retromalleolar tenderness | Dynamic US / MRI | Tendon subluxation; common concomitant injury |
Investigations
Standard X-ray Protocol
Ankle mortise view (best view):
- Shows lateral process
- Look carefully - often subtle
- May be obscured by overlapping structures
Lateral view:
- May show fracture
- Less reliable than mortise view
AP view:
- May show fracture
- Less reliable than mortise view
Key point: Often missed on initial X-rays - high index of suspicion needed.

Management Algorithm
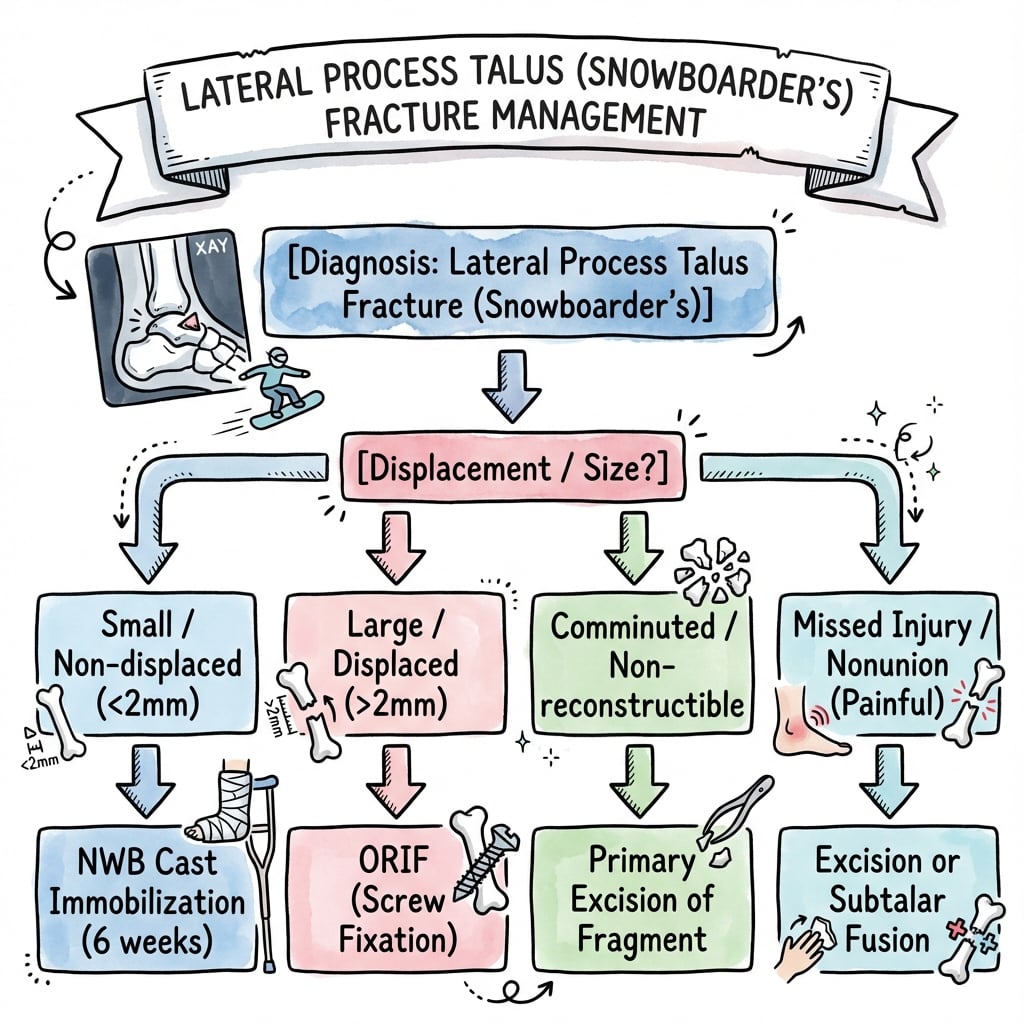
Management Pathway
Lateral Process Talus Fracture Management
Often missed initially - look carefully on ankle mortise view. CT recommended if suspected clinically but X-ray negative. Classic in snowboarders with lateral ankle pain.
If genuinely non-displaced (under 2mm) and especially small/extra-articular, cast and non-weight bearing for about 6 weeks with serial radiographs.
If displaced (over 2mm) with a large or reconstructable fragment, anatomic ORIF with mini/lag screws to restore the posterior facet and protect the subtalar joint.
If small, comminuted or non-reconstructable, excise the fragment - better than a painful malunion. Check subtalar stability afterwards.
Surgical Technique
ORIF Technique (Preferred for Large Fragments)
Indications:
- Large fragment (over 25% of process)
- Displaced (greater than 2mm)
- Reconstructible
Approach:
- Anterolateral or direct lateral approach
- Expose lateral process
- Protect peroneal tendons
Technique:
- Exposure: Anterolateral approach, expose lateral process
- Reduction: Anatomic reduction of articular surface
- Fixation: Lag screws (2.0-2.7mm) or mini-fragment screws
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Preserves subtalar joint
- Prevents arthritis
- Better outcomes than excision for large fragments
ORIF preferred for large fragments to preserve joint.
Complications
| Complication | Frequency / evidence | Risk Factors | Prevention / Management |
|---|---|---|---|
| Subtalar osteoarthritis | Key long-term complication; radiographic OA ~45% at 3.5y in displaced/operative cases (von Knoch) | Malunion, comminution, missed fracture, concomitant chondral injury | Anatomic reduction, early treatment; subtalar fusion if severe |
| Missed diagnosis / delayed treatment | Common - frequently mislabelled as 'sprain'; leads to late surgery (Perera) | Radiographically occult fracture | High index of suspicion, low threshold for CT |
| Nonunion | Reported in late-presenting / inadequately treated fractures | Missed fracture, inadequate fixation | Rigid fixation; excise small symptomatic nonunions |
| Concomitant injuries | Peroneal dislocation ~46%, calcaneal chondral ~48%, subtalar subluxation ~7% (Horterer) | High-energy mechanism | Active search on CT/MRI; address at surgery |
| Wound complications | Thin lateral soft-tissue envelope | Swelling, comorbidity | Careful soft-tissue handling, delay surgery until swelling settles |
Subtalar Osteoarthritis
The defining long-term complication. The lateral process forms the lateral part of the posterior subtalar facet, so any residual articular incongruity drives degeneration.
- Cause: malunion, comminution, missed fracture, associated chondral injury
- Prevention: anatomic reduction and early appropriate treatment
- Management: activity modification, orthoses, and subtalar (talocalcaneal) arthrodesis for established symptomatic arthritis
Missed Diagnosis
The commonest avoidable problem - the fracture is frequently radiographically occult and mimics a lateral ankle sprain.
- Cause: subtle on plain films, clinically resembles a sprain
- Prevention: high index of suspicion, bony point tenderness over the process, low threshold for CT
- Consequence: delayed treatment, nonunion and a higher need for late surgery (Perera)
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Subtalar ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- Cast removal
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
Outcome data come from small series, so quote ranges and the named studies rather than precise figures.
- Early diagnosis is the strongest determinant of a good result - favourable outcomes when diagnosed early and treated appropriately (von Knoch; McCrory-Bladin).
- Minimally displaced, correctly treated fractures do well: in the von Knoch cohort the non-operative minimally-displaced group scored higher (mean AOFAS 98) than the operative displaced/unstable group (93).
- Operatively treated displaced fractures still achieve good function in most patients (Wijers: median AOFAS 75 at 5.5 years; 78% operated), but late subtalar OA is common.
- Return to sport is achieved by most but not all (von Knoch: 35% did not regain their pre-injury level).
Long-Term Prognosis
- Subtalar osteoarthritis is the dominant late issue - radiographic OA in roughly 45% of displaced/operative cases at 3.5 years (von Knoch), concentrated in fractures with comminution, associated injuries, or delayed/missed treatment.
- Key risk factors: displacement, comminution, concomitant chondral/peroneal injury, and missed or delayed diagnosis.
- Salvage: established symptomatic subtalar arthritis is managed by subtalar arthrodesis.
Controversies and Areas of Uncertainty
The evidence base is low-level - small retrospective series and case reports, no randomised trials. Treatment recommendations are expert consensus, so a candidate should frame answers as principles rather than fixed rules.
ORIF vs excision for comminuted fragments
The Perera review favoured excision for comminuted (type II) fractures, whereas more recent series (Tinner-Sommer, Wijers) argue for reconstructing comminuted fragments that are technically fixable and reserving excision for the genuinely non-reconstructable. The honest exam answer: reconstruct if you can achieve a congruent posterior facet; excise if you cannot.
The 2mm threshold
The "greater than 2mm" articular step-off trigger is widely quoted but not derived from comparative trials. It is extrapolated from intra-articular fracture principles. Fragment size, comminution and intra-articular involvement matter as much as the absolute step-off.
Role of conservative treatment
Some series report acceptable results with casting of minimally displaced fractures, but Wijers restricts non-operative care to non-displaced, small, extra-articular fractures only. Outcomes of conservative treatment of displaced fractures remain unclear (Hörterer).
Concomitant injuries drive surgery
A growing theme is that associated peroneal tendon dislocation, calcaneal chondral lesions and subtalar subluxation - present in a large proportion of operative cases - may be the dominant determinant of outcome and a primary surgical indication, independent of the talar fragment itself.
Evidence Base
First description of the snowboarder's fracture
- Mimics a lateral ankle sprain; easily missed on plain films
- Displaced/comminuted fractures cause long-term disability
McCrory-Bladin classification (the standard system)
- Mechanism = dorsiflexion + inversion
- Three subtypes guide differential management
- Risk of subtalar OA justifies early aggressive treatment
Outcomes in snowboarders + concomitant injury burden
- Mean AOFAS 94; minimally-displaced scored higher than displaced
- 88% of operative cases had concomitant hindfoot injury
- Radiographic subtalar OA in 45% at 3.5 years
Management algorithm by fracture type
- Type I (large) to ORIF; Type II (comminuted) to excision; Type III (chip) to cast
- Missed diagnosis frequently leads to delayed surgery
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Snowboarder with Lateral Ankle Pain
"A 25-year-old snowboarder presents with lateral ankle pain after fall. Initial X-rays were read as normal, but he has persistent pain 2 weeks later. Clinical examination shows tenderness over lateral process. Repeat X-rays show subtle fracture of lateral process of talus. CT shows 3mm displacement."
Scenario 2: Small Comminuted Fragment
"A 30-year-old athlete presents with lateral process talus fracture. CT shows small comminuted fragment (under 25% of process) with 4mm displacement. The fragment is not reconstructible."
Scenario 3: Missed Fracture Presenting Late
"A 28-year-old presents 4 months after a snowboarding fall that was diagnosed and treated as a lateral ankle sprain. He has persistent lateral hindfoot pain, pain on subtalar motion and difficulty on uneven ground. Repeat radiographs and CT show an un-united, displaced lateral process fragment with early subtalar joint changes. How do you manage this?"
MCQ Practice Points
Snowboarder Fracture
Q: What is the classic mechanism of lateral process talus fracture? A: Dorsiflexion + inversion - Classic snowboarder fracture. Snowboard bindings prevent ankle motion, so force is transmitted to talus. High index of suspicion in snowboarders with lateral ankle pain.
Displacement Threshold
Q: What is the displacement threshold for surgical treatment of lateral process talus fractures? A: Greater than 2mm step-off - Displacement greater than 2mm requires ORIF to prevent subtalar arthritis. Non-displaced fractures (less than 2mm) can be treated conservatively with good results (85-90%).
ORIF vs Excision
Q: When is ORIF preferred over excision for lateral process talus fractures? A: Large fragments (over 25% of process) that are reconstructible - ORIF preserves subtalar joint and prevents arthritis (80-90% good results). Excision is acceptable for small comminuted fragments (under 25%) that are not reconstructible (75-85% good results).
Missed Diagnosis
Q: Why are lateral process talus fractures often missed initially? A: Subtle on X-ray, often misdiagnosed as ankle sprain - 30-40% are missed initially. High index of suspicion needed, especially in snowboarders. CT recommended if suspected clinically but X-ray negative.
Subtalar Arthritis
Q: What is the most common complication of untreated lateral process talus fractures? A: Subtalar arthritis - Malunion or missed fracture leads to subtalar arthritis in 20-30% of cases. Anatomic reduction with ORIF prevents arthritis (10-15% with proper treatment vs 20-30% without treatment).
Guidelines, Registries & Global Practice
Global epidemiology. Lateral process fractures are the second most common talar fracture after neck fractures, but remain uncommon overall (talar fractures are under 1% of all fractures). Incidence tracks snowboarding participation, so it is concentrated in alpine regions and winter-sports seasons; outside that context it follows high-energy falls and road trauma worldwide. There is no implant registry for this fracture - the evidence is pooled small series, so practice is consensus-driven everywhere.
Side-by-side guidance
How major bodies frame lateral process fracture management
| Body / Source | Diagnosis emphasis | Operative trigger | Distinctive point |
|---|---|---|---|
| AO Foundation | CT for any intra-articular hindfoot fracture | Displaced (over 2mm) intra-articular to anatomic ORIF | Mini-fragment/lag screw fixation, anterolateral approach |
| BOA / BOAST (open & hindfoot principles) | Soft-tissue assessment, CT planning | Displaced intra-articular fracture | Senior-led decision making; manage swelling before surgery |
| AAOS / North American texts | High suspicion in 'snowboarder's ankle' | Displaced/large fragment to ORIF; comminuted to excise | Strong emphasis on missed-diagnosis avoidance |
| EFORT / European series (von Knoch, Tinner-Sommer) | CT + MRI for concomitant injuries | Displaced fractures; reconstruct comminution if possible | Modified classification; address peroneal/chondral injuries |
High- vs limited-resource practice
High-resource settings
Routine CT (and often MRI) to characterise the fragment and detect concomitant peroneal/chondral injury; image-guided ORIF with mini-fragment instrumentation; early structured rehabilitation.
Limited-resource settings
Diagnosis may rest on a careful mortise radiograph and clinical suspicion where CT is scarce; the priority is simply not to miss it. Non-displaced fractures are cast; displaced fractures are referred for fixation or, where reconstruction is not feasible, fragment excision - a low-cost, durable option.
Orthopaedic Exam Relevance
Lateral process talus fractures are a common viva topic. Know that the snowboarder's fracture = dorsiflexion + inversion mechanism, is frequently missed (mimics a sprain), is classified by McCrory-Bladin (NOT Hawkins, which is talar neck), and that articular step-off greater than 2mm is the operative trigger. ORIF reconstructs displaced fixable fragments; excision is for small/comminuted non-reconstructable fragments; subtalar osteoarthritis is the main long-term complication. Be ready to discuss the mechanism, the classification trap, and the ORIF-versus-excision decision.
LATERAL PROCESS TALUS FRACTURES
Clinical summary
Key Concepts
- •Snowboarder fracture = dorsiflexion + inversion mechanism
- •Lateral process = lateral part of the posterior subtalar facet + talofibular surface
- •Frequently missed (mimics a sprain, often radiographically occult)
- •Articular step-off greater than 2mm is the operative trigger
Classification (McCrory-Bladin)
- •Type I: Large single fragment (subtalar + talofibular) - ORIF if displaced
- •Type II: Comminuted - ORIF if reconstructable, else excision
- •Type III: Small chip/avulsion (often extra-articular) - cast; late excision if symptomatic
- •NOT Hawkins - Hawkins is for the talar NECK
Treatment
- •Non-displaced/extra-articular: Conservative (cast, NWB ~6 weeks)
- •Displaced reconstructable fragment: ORIF (mini/lag screws, anterolateral approach)
- •Comminuted/non-reconstructable: Excision (better than malunion)
- •Operative trigger: articular step-off greater than 2mm or intra-articular displacement
Surgical Technique
- •ORIF: Anterolateral approach, anatomic reduction, lag/mini-fragment screws (2.0-2.7mm)
- •Excision: Same approach, remove fragment, smooth edges, check subtalar stability
- •Protect peroneal tendons; look for peroneal dislocation
- •Verify reduction fluoroscopically
Complications
- •Subtalar osteoarthritis (key long-term complication; ~45% radiographic at 3.5y in displaced/operative cases)
- •Missed diagnosis to nonunion and late surgery
- •Concomitant peroneal dislocation / calcaneal chondral lesion
- •Wound issues over thin lateral soft tissue