Posterior-Axillary-Fold Injury of Athletes
- LATISSIMUS DORSI (and TERES MAJOR) RUPTURES are UNCOMMON injuries of the tendons at/near their humeral insertion - these muscles form the POSTERIOR AXILLARY FOLD and act as extensors, adductors and internal rotators of the arm - and the injury spans a spectrum from strain/partial tear to COMPLETE AVULSION (the tendons may tear together or separately).
- They occur in THROWING/OVERHEAD and high-demand ATHLETES (classically baseball PITCHERS) and, characteristically, in WATER-SKIERS, through a sudden ECCENTRIC/violent load on the contracting muscle with the arm in abduction/external rotation.
- The PRESENTATION is ACUTE POSTERIOR-AXILLARY pain with BRUISING/ecchymosis, a palpable DEFECT or asymmetry of the posterior axillary fold, and WEAKNESS of shoulder extension, adduction and internal rotation; in athletes the functional complaint is loss of throwing/overhead POWER and velocity.
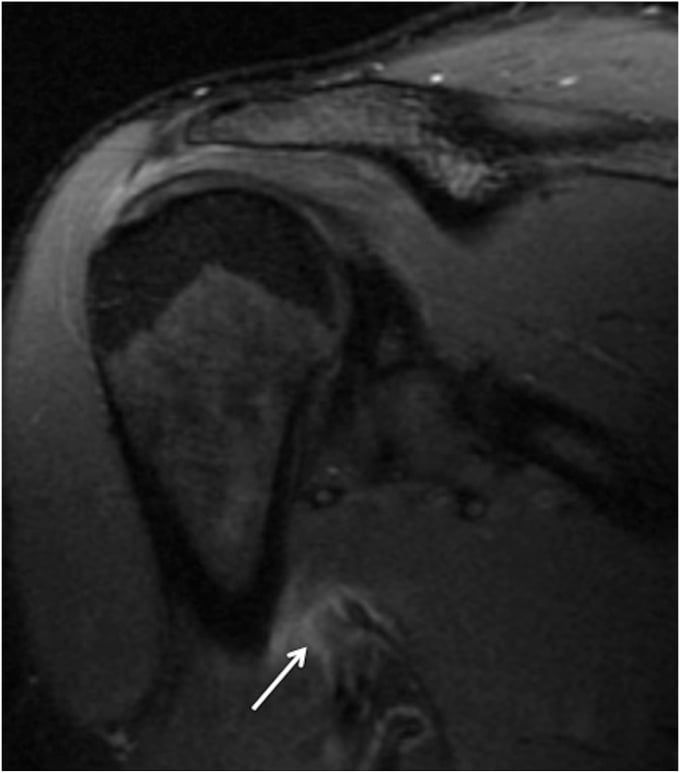
- DIAGNOSIS is clinical (the posterior-axillary defect/bruise and the sporting mechanism) confirmed by MRI, which characterises the tear, whether the latissimus and/or teres major is involved, and the degree of RETRACTION (informing treatment).
- THE COHORT EVIDENCE CUTS AGAINST 'REPAIR THE HIGH-DEMAND THROWER'. In the only series of PROFESSIONAL BASEBALL PITCHERS - 16 players treated between 2002 and 2008, INCLUDING 6 TENDON AVULSIONS as well as 10 strains - ALL were managed NON-OPERATIVELY, and 15 OF 16 (94 PERCENT) returned to the SAME OR HIGHER level of play. Mean time to throwing was 35.6 days and to pitching 61.9 days. So a complete avulsion in an elite thrower is NOT by itself an indication to operate: non-operative treatment has the better-documented track record in exactly that population.
- KNOW THE PROGNOSTIC NUMBERS FROM THAT SERIES. NINE OF 16 (56 PERCENT) of these injuries were SEASON-ENDING even though almost all players eventually returned, mean total time lost for those returning within the same season was 82.4 days, and 2 OF 16 (13 PERCENT) sustained a RECURRENCE. Strikingly, 75 PERCENT (12 of 16) had a PRIOR shoulder or elbow injury - so this is often a tendon failing in an already-damaged throwing shoulder rather than an isolated event.
- SURGICAL REPAIR IS AN OPTION WITH GOOD RESULTS, NOT A DEMAND-DRIVEN NECESSITY. In a series of 11 repairs (7 professional and 1 collegiate pitchers), ALL professional pitchers returned to the same level with NO significant change in any performance metric, an ASES score of 100 and a KJOC score of 89. Notably the mean time from injury to repair was 389 DAYS and only 36 PERCENT were repaired within 6 weeks - so the common assertion that these tears must be repaired EARLY, before retraction and fatty atrophy, is NOT borne out by that series.
- “Latissimus dorsi (+/- teres major) rupture = uncommon POSTERIOR-AXILLARY-FOLD tendon injury in throwing/overhead and high-demand athletes (and water-skiers). These muscles extend/adduct/internally rotate the arm.
- “Presentation: acute posterior-axillary pain + bruise + palpable defect/asymmetry + weakness of extension/adduction/IR; athletes lose throwing power. MRI confirms tear/retraction and which muscle(s) involved.
- “Management: the cohort evidence favours NON-OPERATIVE treatment even in elite throwers - 16 professional pitchers including 6 AVULSIONS, all managed non-operatively, 94% back to the same or higher level (35.6 days to throwing, 61.9 to pitching). But 56% were season-ending, 13% recurred, and 75% had a prior shoulder/elbow injury.
- “REPAIR is a good option rather than a demand-driven necessity: in 11 repairs all professional pitchers returned to the same level with unchanged performance metrics - achieved despite a mean 389 days from injury to surgery, so the 'repair early before retraction' rule is borrowed from cuff/pectoralis surgery and unproven here.
Throwing/overhead athlete (or water-skier) with acute posterior-axillary pain + bruising + a palpable defect and weakness of extension/adduction/internal rotation. MRI confirms.
In 16 professional pitchers including 6 avulsions, all treated non-operatively, 94 percent returned to the same or higher level. Repair also does well when chosen, but a complete avulsion is not by itself an operative indication.
Anatomy: Two Insertions, Two Nerves, and the Neurovascular Danger
- Origins and the fold. The latissimus dorsi has a broad origin (thoracolumbar fascia and spinous processes from about T7 down, the iliac crest, the lower ribs, and the inferior angle of the scapula); the teres major arises from the inferior angle and lower lateral border of the scapula. Their tendons together form the posterior axillary fold.
- Two distinct humeral insertions. The latissimus dorsi tendon inserts into the floor of the intertubercular (bicipital) groove; the teres major inserts onto the medial lip (crest of the lesser tubercle) just medial to it. The latissimus tendon lies anterior/deep and spirals around the inferior border of teres major - which is why the two can tear together or separately, and why MRI is used to say which is involved.
- Nerve supply. Latissimus dorsi = thoracodorsal nerve (C6-8, from the posterior cord); teres major = lower subscapular nerve (C5-6, posterior cord).
- Actions and the neurovascular danger. Both extend, adduct and internally rotate the humerus (latissimus is also the "handcuff/crutch" muscle, depressing the raised arm). The axillary approach for repair passes near the radial nerve, the axillary nerve and posterior circumflex humeral vessels, and the thoracodorsal pedicle - the "technical expertise/neurovascular risk" the evidence flags.
Q: Describe the insertions and nerve supply of latissimus dorsi and teres major.
A: Both form the posterior axillary fold. The latissimus dorsi inserts into the floor of the intertubercular (bicipital) groove and is supplied by the thoracodorsal nerve (C6-8, posterior cord); the teres major inserts onto the medial lip/crest of the lesser tubercle and is supplied by the lower subscapular nerve (C5-6, posterior cord). The LD tendon lies anterior/deep and spirals around the inferior border of teres major. Both extend, adduct and internally rotate the arm; the axillary repair approach risks the radial and axillary nerves, the posterior circumflex humeral vessels and the thoracodorsal pedicle.
MRI and Why Retraction Drives the Decision
- MRI findings. MRI shows the tendon avulsed off its humeral footprint with fluid/oedema and haematoma at the posterior axilla, identifies whether the latissimus dorsi, the teres major or both are torn, and measures the retraction (the gap between the torn tendon end and the footprint - 6 cm in the cited case).
- How much retraction and completeness really drive the decision. They inform surgical planning, but they do not settle treatment: in the professional-pitcher series, 6 avulsions were treated non-operatively and the group returned at 94 percent. The reasoning that repair must be done early, before retraction, scarring and fatty atrophy, is imported from rotator-cuff and pectoralis-major surgery and is not supported here - in the published repair series the mean interval from injury to surgery was 389 days, only 36 percent were operated within 6 weeks, and all professional pitchers still returned to the same level.
- Practical point. So the two things MRI must answer before deciding are which tendon(s) are involved and how far they have retracted; combined with the patient's demand, these determine whether and when to operate.
Q: What must MRI show in a latissimus dorsi / teres major rupture, and why does retraction matter?
A: MRI must show which tendon(s) are torn (LD, teres major or both), whether the tear is partial or a complete avulsion off the humeral footprint, and the degree of retraction (e.g. 6 cm in the cited case). Those findings guide surgical planning, but they do not settle treatment - 6 avulsions in the professional-pitcher series were managed non-operatively with a 94 percent return rate. The "repair early before retraction and fatty atrophy" rule is borrowed from cuff and pectoralis-major surgery: in the published repair series the mean interval to surgery was 389 days and only 36 percent were within 6 weeks, yet all professional pitchers returned to the same level.
What the Two Cohorts Show - and Why 'Repair the Elite Thrower' Overstates It
The intuitive rule is that a complete avulsion in a professional thrower must be repaired. The only cohort of professional baseball pitchers with these injuries says otherwise. Sixteen pitchers treated between 2002 and 2008
- 6 with tendon avulsions and 10 with strains - were all managed non-operatively with rest, rehabilitation and a throwing programme, and 15 of 16 (94 percent) returned to the same or higher level of play, at a mean of 35.6 days to throwing and 61.9 days to pitching. A complete avulsion is therefore not in itself an operative indication, and a candidate who says so without qualification is quoting a plausible principle rather than the data.
- Non-operative (Nagda, n=16 professional pitchers)
- 6 avulsions, 10 strains - all treated non-operatively
- Repair (Erickson, n=11; 7 professional pitchers)
- Complete tears selected for repair
- Non-operative (Nagda, n=16 professional pitchers)
- 15 of 16 (94 percent) same or higher
- Repair (Erickson, n=11; 7 professional pitchers)
- All professional pitchers returned to same level
- Non-operative (Nagda, n=16 professional pitchers)
- Not formally measured
- Repair (Erickson, n=11; 7 professional pitchers)
- No significant change in any pitching metric
- Non-operative (Nagda, n=16 professional pitchers)
- Mean 35.6 days to throwing, 61.9 to pitching
- Repair (Erickson, n=11; 7 professional pitchers)
- Mean 389 days from injury to repair; only 36 percent within 6 weeks
- Non-operative (Nagda, n=16 professional pitchers)
- 56 percent season-ending; 13 percent recurrence; 75 percent had prior shoulder or elbow injury
- Repair (Erickson, n=11; 7 professional pitchers)
- ASES 100, KJOC 89, VAS 0 in professional pitchers
Q: Is a delayed latissimus dorsi repair compromised by retraction and fatty atrophy, as in the rotator cuff?
A: That reasoning is borrowed from cuff and pectoralis-major repair and is not supported by the published repair series here. In those 11 repairs the mean interval from injury to surgery was 389 days, with only 36 percent operated within 6 weeks, and yet all professional pitchers returned to the same level with an ASES of 100, a KJOC of 89 and no significant change in any performance metric. Both series are small, retrospective and without a comparison group, so neither settles the operative-versus-non-operative question - but the honest position is that non-operative treatment has the better-documented record in elite throwers, repair produces good results when chosen, and urgency has not been demonstrated.
Features & Management
Latissimus dorsi (and teres major) ruptures are uncommon tendon injuries at/near the humeral insertion - the muscles of the posterior axillary fold, which extend, adduct and internally rotate the arm. They occur in throwing/overhead and high-demand athletes (classically baseball pitchers) and water-skiers, via a sudden eccentric load. Presentation is acute posterior-axillary pain, bruising, a palpable defect/ asymmetry, and weakness of extension/adduction/internal rotation, with loss of throwing power. MRI confirms the tear, the muscle(s) involved and the retraction. Management is debated, but the cohort evidence favours non-operative treatment even in elite throwers: 16 professional pitchers, including 6 avulsions, were all managed non-operatively and 94 percent returned to the same or higher level. Surgical repair also produces good results when chosen - all professional pitchers in a repair series returned with unchanged performance metrics - so it is an option, not a demand-driven necessity.
The management of latissimus dorsi and teres major ruptures is genuinely individualised, and the central judgement is the patient's functional demand set against the tear pattern. Many of these injuries - partial tears and tears in recreational athletes - do well with non-operative treatment: rest, a structured rehabilitation programme and a graded return to activity, often with good functional recovery despite some residual deficit. By contrast, a complete avulsion is not by itself an operative indication: in the only series of professional pitchers, six avulsions were among the sixteen players treated entirely non-operatively, and 94 percent of that group returned to the same or higher level. Surgical repair (re-attachment of the avulsed tendon, for example through a single-incision axillary approach with suture anchors) also produces good results when chosen, with all professional pitchers in a repair series returning to the same level and no measurable change in performance. MRI is important not only to confirm the diagnosis but to define which of the two tendons is involved and the degree of retraction, which informs both the decision and the surgical planning. The key is shared decision-making with the athlete rather than a one-size-fits-all approach.
The related injuries and principles sit on neighbouring pages. The analogous tendon rupture at the front of the axilla is pectoralis major rupture; the loading that produces this injury is set out in throwing biomechanics; the biology behind the repair-timing argument is in tendon healing; and the framework for clearing an athlete afterwards is return-to-sport criteria.

Mnemonics & Memory Aids
LATS
Hook:LATS: Latissimus (posterior axillary fold), Athletes (throwers/water-skiers), Tell-tale pain/bruise/defect (MRI), Start non-operative (94% of pro pitchers returned) - Surgery is an option.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A baseball pitcher develops sudden posterior axillary pain and bruising with weakness, and MRI shows a latissimus dorsi tendon avulsion. How do you decide management?”
What it is
- Uncommon rupture of latissimus dorsi (+/- teres major) tendon at the humeral insertion
- Posterior-axillary-fold muscles: extend, adduct, internally rotate the arm
- Spectrum: strain -> partial tear -> complete avulsion
Who & presentation
- Throwing/overhead and high-demand athletes; classically water-skiers (eccentric load)
- Acute posterior-axillary pain + bruising + palpable defect/asymmetry
- Weakness of extension/adduction/internal rotation; loss of throwing power
Diagnosis & management
- MRI: confirms tear, which tendon(s), degree of retraction
- Non-operative did well even in professionals: 16 pitchers, 6 avulsions, 94 percent same-or-higher level
- 56 percent season-ending; 13 percent recurrence; 75 percent had a prior shoulder or elbow injury
- Repair also gives good results (all pro pitchers returned, performance unchanged) despite mean 389 days to surgery - an option, not a necessity
Evidence & Key Studies
Latissimus dorsi tendon rupture repair in a high-demand athlete (single-incision axillary approach)
- Latissimus dorsi tendon rupture (with associated teres major partial tearing) occurred in a high-demand competitive athlete, causing shoulder weakness and impaired athletic/professional performance, with imaging confirming a complete rupture and retraction.
- Surgical repair (single-incision axillary approach with an all-suture-anchor tension-slide technique) achieved near-complete return to pre-injury function by 7 months.
- Surgical repair is an effective option for complete latissimus dorsi tendon ruptures in high-demand athletes, though it requires technical expertise (neurovascular risk).
Management and outcomes of latissimus dorsi and teres major injuries in professional baseball pitchers
- Retrospective case series of 16 professional baseball pitchers treated for a latissimus dorsi or teres major tear between 2002 and 2008, mean age 28.1 years, MRI-confirmed in all. The injuries comprised 6 tendon avulsions and 10 strains, and all 16 were treated non-operatively with rest, rehabilitation and a throwing programme.
- 15 of 16 (94 percent) returned to the same or higher level of play, at a mean of 35.6 days to throwing and 61.9 days to pitching. Nine of 16 (56 percent) were season-ending, and mean total time lost for those returning within the same season was 82.4 days.
- Two of 16 (13 percent) sustained a recurrence, and 75 percent (12 of 16) had a prior shoulder or elbow injury. The authors conclude that non-operative treatment is successful in allowing a return to high-level pitching - including in the avulsions. It is a small retrospective series with no operative comparison group.
Performance and return to sport in elite baseball players and recreational athletes following repair of the latissimus dorsi and teres major
- Eleven patients (mean age 29.9 years) undergoing latissimus dorsi and/or teres major repair with more than 12 months of follow-up; 73 percent were pitchers, of whom 7 were professional and 1 collegiate, and 86 percent underwent surgery on the dominant side.
- At final follow-up the mean visual analogue pain score was 0.7, the ASES score 100 and the KJOC score 93. Among professional pitchers, pain was 0, ASES 100 and KJOC 89; all returned to the same level of play, and no preoperative-to-postoperative performance metric differed significantly.
- Mean time from injury to repair was 389 days, with only 36 percent repaired within 6 weeks - so these good results were obtained despite substantial delay, which does not support an imperative to repair early. Eleven patients, retrospective, with no non-operative comparison group.
Latissimus dorsi tendon rupture (with teres major involvement) in a high-demand athlete causing weakness and impaired performance, and the effectiveness of surgical repair (single-incision axillary, suture-anchor) with good return to function, come from the cited Zogby report. The posterior-axillary-fold anatomy and function (extension/adduction/internal rotation), the throwing/overhead and water-skier mechanisms, the clinical presentation (pain/bruise/defect/weakness) and the role of MRI are standard, well-established teaching. The non-operative outcomes, the season-ending and recurrence proportions and the prior-injury figure come from the Nagda series of 16 professional pitchers; the repair outcomes and the 389-day mean interval to surgery from the Erickson series of 11 repairs. Both are small, retrospective and have no comparison group, so neither settles operative against non-operative treatment - and no randomised or comparative study exists. There is likewise no published incidence for this injury, no validated grading system despite the "grade IIIA" terminology used in some reports, no retraction threshold that mandates repair, and no evidence-based return-to-throwing protocol, so none is quoted here.