The Phases of Throwing & the Kinetic Chain
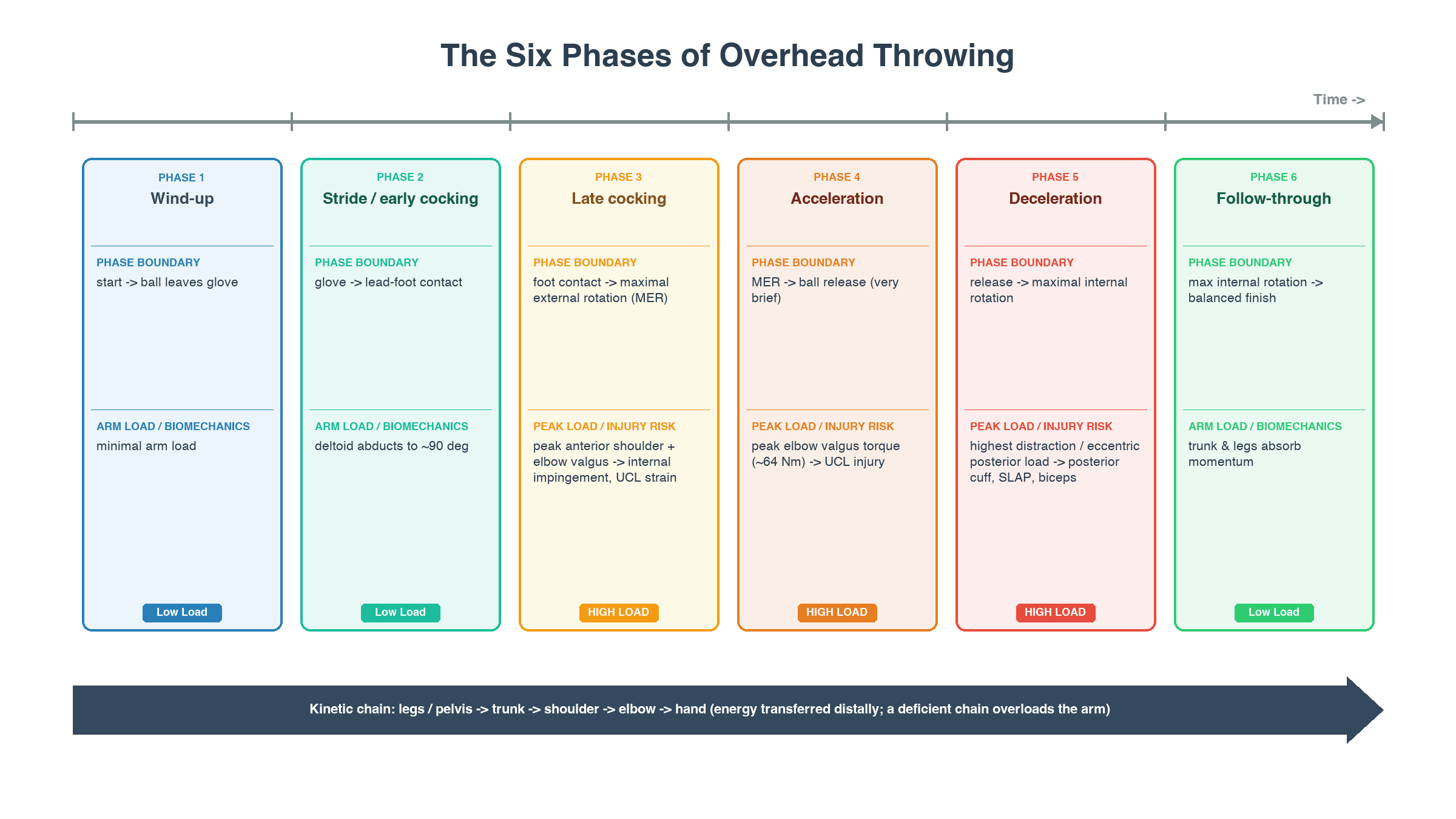
- Overhead THROWING (the pitching cycle) is divided into SIX PHASES: (1) WIND-UP, (2) STRIDE/EARLY COCKING, (3) LATE COCKING, (4) ACCELERATION, (5) DECELERATION, and (6) FOLLOW-THROUGH; understanding these phases explains WHEN and WHY specific injuries occur.
- Throwing is a KINETIC-CHAIN activity: energy/momentum is generated in the LEGS and PELVIS, transferred through the TRUNK, and delivered to the SHOULDER, ELBOW and HAND - so efficient, well-timed transfer from the lower body protects the arm, while a deficient kinetic chain forces the arm to 'make up' the energy and increases its load/injury risk.
- The PEAK LOADS occur at LATE COCKING and ACCELERATION: at late cocking the shoulder reaches maximal ABDUCTION and EXTERNAL ROTATION (the arm 'laid back'), generating large anterior shoulder forces and a high ELBOW VALGUS load; at acceleration there is explosive internal rotation with PEAK ELBOW VALGUS TORQUE and shoulder distraction - these are the phases that injure the UCL and the rotator cuff/labrum.
- DECELERATION generates the highest DISTRACTION and eccentric loads as the posterior cuff and scapular stabilisers violently slow the arm - the phase associated with posterior cuff/labral and SLAP pathology; FOLLOW-THROUGH dissipates the remaining energy.
- This biomechanical loading EXPLAINS the THROWING INJURIES: ULNAR COLLATERAL LIGAMENT (UCL) injury (medial elbow, from valgus torque), INTERNAL (posterosuperior) IMPINGEMENT and SLAP/labral tears, GLENOHUMERAL INTERNAL ROTATION DEFICIT (GIRD) and the associated 'thrower's shoulder', and biceps/posterior-cuff pathology - each maps to the phase and load that produces it.
- MECHANICS relate to INJURY RISK and PREVENTION: Altering throwing mechanics (for example stride length, which changes pelvic-trunk separation and the timing of peak trunk rotation) changes the load on the shoulder and elbow and the injury risk - so optimising the KINETIC CHAIN, PELVIC-TRUNK SEPARATION/timing and conditioning (and managing workload) is central to reducing throwing injuries.
- “Six phases of throwing: wind-up -> stride/early cocking -> late cocking -> acceleration -> deceleration -> follow-through. Throwing is a KINETIC CHAIN (legs/pelvis -> trunk -> shoulder -> elbow -> hand).
- “Peak loads: LATE COCKING (max shoulder abduction + EXTERNAL ROTATION; high anterior shoulder + elbow valgus load) and ACCELERATION (peak elbow VALGUS torque + shoulder distraction). DECELERATION = highest distraction/eccentric loads (posterior cuff/labrum/SLAP).
- “Explains injuries: UCL (valgus), internal impingement/SLAP, GIRD ('thrower's shoulder'), biceps/posterior cuff. A deficient kinetic chain forces the arm to overload. Prevent via mechanics (pelvic-trunk separation/timing), conditioning + workload management.
Late cocking (max shoulder external rotation; anterior shoulder + elbow valgus load) and acceleration (peak elbow valgus torque); deceleration = highest distraction/eccentric loads.
UCL (valgus), internal impingement/SLAP and GIRD (thrower's shoulder), posterior cuff/biceps. A deficient kinetic chain forces the arm to overload.
The Phases, the Kinetic Chain & the Injuries
Overhead throwing has six phases: wind-up, stride/early cocking, late cocking, acceleration, deceleration, follow-through. It is a kinetic chain - energy generated in the legs/pelvis, transferred through the trunk to the shoulder, elbow and hand - so a deficient chain forces the arm to overload. The peak loads are at late cocking (maximal shoulder abduction/external rotation, high anterior-shoulder and elbow valgus load) and acceleration (peak elbow valgus torque, shoulder distraction); deceleration generates the highest distraction/eccentric loads on the posterior cuff/labrum. This explains the throwing injuries - UCL (valgus), internal impingement/SLAP, GIRD and posterior cuff/biceps pathology - each mapping to the loading phase that produces it.
- Peak load
- Max shoulder external rotation; anterior shoulder + elbow valgus
- Associated injury
- Internal impingement, UCL strain, anterior instability
- Peak load
- Peak elbow valgus torque; shoulder distraction/IR
- Associated injury
- UCL injury; rotator cuff/labral load
- Peak load
- Highest distraction + posterior eccentric load
- Associated injury
- Posterior cuff/labral tears, SLAP, biceps
- Peak load
- Energy transfer legs/trunk -> arm
- Associated injury
- Deficient chain -> arm overload/injury
Defining the Phases: Boundaries and Muscle Activity
Each phase is defined by a specific event boundary, and the dominant muscle activity explains where the loads arise - examiners expect the precise definitions, not just the names.
- Starts / ends
- Initiation to the ball leaving the glove (lead knee at peak height)
- Dominant muscle activity
- Minimal arm activity; balance and positioning
- Starts / ends
- Ball out of glove to lead-foot contact
- Dominant muscle activity
- Deltoid abducts to about 90 degrees, then the cuff begins external rotation; the lower body strides
- Starts / ends
- Foot contact to MAXIMAL shoulder external rotation (MER)
- Dominant muscle activity
- Subscapularis, pectoralis major and latissimus contract ECCENTRICALLY to control external rotation; scapular retractors stabilise - peak anterior-shoulder and elbow-valgus load
- Starts / ends
- MER to ball release (very brief - tens of milliseconds)
- Dominant muscle activity
- Explosive CONCENTRIC internal rotation (subscapularis, pectoralis major, latissimus) and elbow extension - peak elbow valgus torque
- Starts / ends
- Ball release to maximal internal rotation
- Dominant muscle activity
- Violent ECCENTRIC posterior cuff (infraspinatus/teres minor), posterior deltoid and scapular stabilisers slow the arm - highest distraction loads
- Starts / ends
- Maximal internal rotation to a balanced finish
- Dominant muscle activity
- Trunk and legs absorb the remaining momentum
Proximal-to-distal sequencing: the segments accelerate and then decelerate in sequence (legs/pelvis, then trunk, then arm, then hand), each transferring momentum distally like a whip (the "summation of speed" principle); well-timed sequencing lets the small, fast distal segments reach high velocity without excess joint load, whereas mistimed sequencing (poor pelvic-trunk separation) makes the arm "catch up" and overload.
The Numbers: How Much Load Throwing Generates
The qualitative "peak loads" become memorable - and explain UCL failure - once quantified (established pitching-biomechanics figures).
- Maximal external rotation at late cocking is around 170-180 degrees (apparent external rotation, including the scapulothoracic and trunk contribution).
- Internal-rotation angular velocity near release reaches roughly 7000 degrees per second - among the fastest of all human joint motions.
- Distraction force at deceleration is around 1 to 1.5 times body weight, resisted eccentrically by the posterior cuff.
- Peak elbow valgus torque in late cocking/acceleration is approximately 64 Nm.
- This is roughly double the in-vitro failure strength of the ulnar collateral ligament (around 30-35 Nm), and the UCL supplies only about half of the valgus restraint.
- So the UCL cannot withstand a single maximal pitch on its own - the dynamic stabilisers (the flexor-pronator mass), the bony articulation and an efficient kinetic chain must share the load; when that sharing fails, the UCL is overloaded and injured. Note that the acute fatigue version of this - a within-game rise in measured joint load - was not confirmed when Escamilla and colleagues measured it; the established association is with cumulative volume. (UCL injury and valgus extension overload are developed in their own topics.)
How the Load Becomes the Lesion
Naming the phase that overloads a structure is only half the answer; examiners then ask by what mechanism the load produces the lesion. Three chains are worth being able to recite.
Repetitive eccentric deceleration loads the posteroinferior capsule and cuff, which respond with contracture. The result is glenohumeral internal rotation deficit (GIRD) - conventionally a loss of more than 20 degrees of internal rotation compared with the non-throwing side, measured at 90 degrees of abduction with the scapula stabilised. The trap is that the deficit alone does not distinguish adaptation from disease: the thrown shoulder also gains external rotation through bony humeral retroversion, so what matters is the total rotational motion (internal plus external). Preserved total motion suggests physiologic adaptation; lost total motion suggests pathologic posterior tightness.
A contracted posteroinferior capsule shifts the glenohumeral contact point posterosuperiorly and allows the scapula and humerus to hyperangulate in late cocking. The articular (undersurface) side of the supraspinatus and infraspinatus is then pinched between the greater tuberosity and the posterosuperior glenoid - internal (posterosuperior) impingement, producing undersurface partial cuff tears and posterosuperior labral fraying in the abducted, externally rotated arm.
In the same laid-back position the long head of biceps vector rotates posteriorly and vertically, twisting at its base and peeling the posterosuperior labrum off the glenoid rim - the peel-back mechanism, the biomechanical explanation for the type II SLAP lesion of the thrower (and the basis of the arthroscopic peel-back test, in which the labrum is seen to displace medially over the glenoid neck when the abducted arm is externally rotated).
Measurement technique, imaging and management for each are developed separately in GIRD, internal impingement, SLAP tears, scapular dyskinesis and UCL injury of the elbow.
Injury Risk & Prevention
- Kinetic chain: optimise lower-body and core conditioning so energy is generated and transferred efficiently (a deficient chain overloads the arm).
- Mechanics: pelvic-trunk SEPARATION and the TIMING of peak trunk rotation (and parameters such as stride length) influence the shoulder/elbow load and injury risk - coaching mechanics matters.
- Restore deficits: address GIRD/posterior capsular tightness (stretching), scapular dyskinesis and cuff strength in the thrower.
- Workload: volume and fatigue - not pitch type - are the dominant modifiable risks. Age-based pitch counts with mandatory rest days (the USA Baseball / MLB Pitch Smart limits: roughly 95 pitches a day at 13-14 years, with rest days scaling with the day's count, and no more than about 100 innings in a year) are the practical expression of this. The age-specific tables and rest-day rules are set out in full in our Little League Shoulder topic.
Pitching more than 100 innings in a single year raised the risk of serious injury (surgery or a career-ending injury) 3.5-fold in a 10-year prospective follow-up of 481 youth pitchers, whose cumulative serious-injury rate was 5.0 percent - and the same study could not demonstrate that throwing curveballs before age 13 increased risk. An earlier season-long cohort of 476 pitchers aged 9-14 did associate the curveball with a 52 percent increase in shoulder pain and the slider with an 86 percent increase in elbow pain, alongside pitch counts per game and per season. The defensible position is therefore that cumulative volume is the established risk and pitch type is contested - not that breaking balls are safe.
The unifying biomechanical principle of throwing is the kinetic chain: power is generated in the legs and pelvis and transferred through the trunk to the arm, and the timing of that transfer - particularly the separation between pelvis and trunk rotation - determines how much load reaches the shoulder and elbow. When the lower body and trunk do not generate or transfer energy efficiently (poor conditioning, faulty mechanics, mistimed pelvic- trunk separation), the arm has to 'catch up' and make up the energy, and the shoulder and elbow are subjected to higher rotational and valgus loads, increasing the risk of injury. This is why the peak loads at late cocking (maximal external rotation) and acceleration (peak elbow valgus torque), and the high distraction of deceleration, translate into the characteristic throwing injuries - ulnar collateral ligament tears, internal impingement and SLAP/labral lesions, GIRD and posterior cuff pathology. Prevention therefore targets the whole chain: lower-body and core conditioning, correct throwing mechanics, restoration of any glenohumeral internal-rotation deficit and scapular control, and disciplined workload management.
Mnemonics & Memory Aids
THROW
Hook:THROW: Transfer (kinetic chain), Hyper-external rotation (late cocking), Rapid acceleration (valgus), Off-load (deceleration), Workload/mechanics (prevention).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the phases of throwing and explain why throwers injure the elbow UCL and the shoulder labrum.”
The six phases
- Wind-up; stride/early cocking; late cocking
- Acceleration; deceleration; follow-through
- Kinetic chain: legs/pelvis -> trunk -> shoulder/elbow/hand
Peak loads
- Late cocking: max shoulder abduction + external rotation; anterior shoulder + elbow valgus
- Acceleration: peak elbow valgus torque; shoulder distraction/internal rotation
- Deceleration: highest distraction + posterior eccentric load
Resulting injuries
- UCL injury (valgus, late cocking/acceleration)
- Internal impingement / SLAP / labral tears; GIRD ('thrower's shoulder')
- Posterior cuff / biceps pathology (deceleration)
Prevention
- Optimise kinetic chain (lower-body/core conditioning)
- Mechanics: pelvic-trunk separation/timing (stride length)
- Restore GIRD (loss of more than 20 deg IR; judge by TOTAL rotational motion) and scapular control
- Workload is the established risk: more than 100 innings a year raised serious injury 3.5-fold; pitch type contested
- Approaching fatigue over 105-135 pitches did NOT raise measured joint kinetics (small study) - do not assert it
Evidence & Key Studies
Stride length influences pelvic-trunk separation and pitching biomechanics (and arm stress)
- Pelvis and trunk counter-rotation transfer energy/momentum from the lower extremities through the trunk during the pitching cycle, affecting throwing-arm kinematics.
- Altering stride length changed the timing within the pitching cycle and the pelvic-trunk separation and peak trunk angular velocity; shorter strides reduced separation and increased the proximal plyometric (trunk-relative) contribution.
- Greater trunk angular velocity relative to the pelvis late in the cycle makes the throwing arm 'catch up' from greater arm lag, increasing shoulder and elbow tensile stress and injury risk - linking mechanics to arm load.
Approaching muscular fatigue did NOT raise shoulder or elbow loads over a simulated game
- Controlled laboratory study: 10 collegiate pitchers threw 15 pitches an inning for 7-9 innings (105-135 pitches) until they subjectively could not continue; 20 kinematic and 11 kinetic variables were measured by 200 Hz three-dimensional motion capture.
- Compared with the first two innings, the only significant changes in the last two were a fall in BALL VELOCITY and a more VERTICAL TRUNK; no other kinematic or kinetic variable differed.
- The study did NOT support the widely taught idea that shoulder and elbow forces and torques rise as a pitcher fatigues - mechanics stayed remarkably similar.
- Small single-session sample (n = 10) using subjective fatigue as the endpoint, so it is underpowered for modest changes; the authors note that a longer-sustained fatigued state might still alter mechanics.
It is intuitive - and commonly taught - that a fatigued thrower's arm sees higher valgus and distraction loads. Measured over a single simulated game that did not happen: velocity dropped and the trunk straightened, but the joint kinetics did not rise. Fatigue and volume remain firmly associated with INJURY in the epidemiological studies; what is not established is that the pathway runs through an acute within-game rise in measured joint load. A safer answer in the viva is that cumulative loading, tissue recovery and mechanics all contribute, rather than asserting a within-game kinetic surge as fact.
The kinetic-chain transfer of energy from the lower extremities through the trunk to the throwing arm, the influence of mechanics (stride length, pelvic-trunk separation and timing) on the load reaching the shoulder and elbow, and the link between a mistimed chain (arm 'catch-up'/lag) and increased shoulder/elbow tensile stress/injury risk come from the cited Ramsey study. The six phases of throwing, the specific peak loads (late cocking external rotation, acceleration elbow valgus torque, deceleration distraction), and the resulting injury patterns (UCL, internal impingement/SLAP, GIRD, posterior cuff/biceps) with prevention via mechanics/ conditioning/workload are standard, well-established teaching. The finding that approaching muscular fatigue over 105-135 pitches did not raise measured shoulder or elbow kinetics comes from the cited Escamilla study, which is small and single-session. The GIRD threshold of more than 20 degrees, the primacy of total rotational motion, and the peel-back and hyperangulation mechanisms are taken in substance from our GIRD, internal impingement and SLAP tears topics; the Pitch Smart limits and the pitch-type findings (Olsen 2006; Fleisig 2011) are taken from our Little League Shoulder topic, where the full age-specific tables sit. Peak elbow valgus torque of about 64 Nm against an in-vitro ulnar collateral ligament failure strength of roughly 30-35 Nm is established pitching-biomechanics teaching. No published safe upper limit of valgus torque for an individual thrower exists, so none is quoted here. See also our UCL injury of the elbow and scapular dyskinesis topics.