Plantar Fibromatosis | Benign Fibroproliferative Disorder of the Plantar Aponeurosis
- Myofibroblast is the pathological cell - same biology as Dupuytren's and Peyronie's
- Nodules sit on the medial central band of the plantar aponeurosis (instep, not the weight-bearing heel)
- Toe contractures are rare - a key difference from Dupuytren's disease of the hand
- Conservative management first; surgery only for failed conservative care
- Wide (subtotal/total) fasciectomy beats local excision because partial excision recurs frequently
- “Part of the superficial fibromatoses (Dupuytren, Peyronie, knuckle pads)
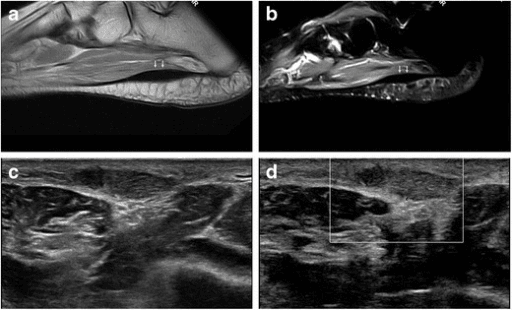
- “Ultrasound is first-line; MRI shows low T1/T2 signal (collagen) for aggressive lesions
- “Main differential is a malignant soft-tissue sarcoma - biopsy if atypical
- “Recurrence is the rule, not the exception, after inadequate excision
Benign fibroproliferative disorder of the plantar aponeurosis. The pathological cell is the myofibroblast, which lays down excess collagen and generates contractile force. It is one of the superficial fibromatoses, grouped with Dupuytren's (palm) and Peyronie's (penis).
Nodules grow on the medial part of the central band of the plantar fascia - the non-weight-bearing instep. Because they are off the main weight-bearing heel pad, they may be tolerated for years before becoming painful with footwear or walking.
Unlike Dupuytren's, toe contractures are rare. The disease tends to stay nodular rather than forming aggressive contracting cords. This is a classic exam discriminator between palmar and plantar fibromatosis.
Conservative first (orthotics, padding, activity change). Surgery only for failed conservative care, and when operating, wide fasciectomy beats local excision - local nodule excision has the highest recurrence. Always exclude a sarcoma before treating an atypical lesion.
FEET DABLederhose Associations & Risk Factors
Hook:The FEET DAB factors cluster with plantar fibromatosis - but remember the strongest clue is fibromatosis somewhere else (the hand or penis).
SOLEPlantar vs Palmar Fibromatosis
Hook:Think SOLE: the plantar version stays in the SOLE as a nodule, rarely contracts toes, and recurs if you only take the lump.
WIDESurgical Decision Principles
Hook:If conservative care fails, go WIDE: a generous fasciectomy, not a local lumpectomy, is the durable operation.
Overview & Definitions
What is Lederhose Disease?
Lederhose disease, also called plantar fibromatosis or Morbus Ledderhose, is a benign but locally infiltrative fibroproliferative disorder of the plantar aponeurosis. Firm, slow-growing nodules form within the fascia, most often along the medial border of the central band. It is named after Georg Ledderhose, the German surgeon who described it in the late 19th century. According to PubMed, recent reviews emphasise that it is rare, benign, and often difficult to treat because of its tendency to recur after surgery.
It is one of the superficial fibromatoses, a family that also includes:
- Dupuytren's disease - palmar and digital fascia of the hand
- Peyronie's disease - tunica albuginea of the penis
- Knuckle pads (Garrod's nodes) - dorsal PIP joints
Because the underlying biology (myofibroblast proliferation, excess collagen) is shared, these conditions frequently coexist. The presence of one should prompt examination for the others.
Key Terminology
The thick fibrous band running from the calcaneal tuberosity to the toes, with central, medial, and lateral components. Lederhose nodules characteristically affect the central band, on its medial side.
A benign fibrous proliferation that grows slowly and infiltrates locally but does not metastasise. Contrasts with deep fibromatoses (desmoid tumours), which are larger and more aggressive.
The pathological cell - a fibroblast that has acquired contractile alpha-smooth muscle actin. It produces collagen and generates the contractile force that, in the hand, causes finger contractures.
Reappearance of nodular disease in or adjacent to the operated field. Because the fascia is diffusely abnormal, inadequate excision predictably recurs, which drives the preference for wide fasciectomy.
Epidemiology (Global)
Plantar fibromatosis is uncommon and its true incidence is poorly defined. According to PubMed, a Dutch population study estimated only about 1.2 operations for plantar fibromatosis per 100,000 people per year, underlining how rarely it reaches surgery. It is generally reported in middle-aged and older adults, with a male predominance, and bilateral involvement occurs in a significant minority. A strong link with Dupuytren's disease is consistently reported across case series and reviews.
Pathophysiology & Anatomy
The Disease Process
The core abnormality is uncontrolled proliferation of myofibroblasts within the plantar aponeurosis, with deposition of disorganised collagen. As in Dupuytren's disease, the process is often described in three overlapping phases:
Myofibroblasts proliferate within the fascia, forming a firm, sometimes tender nodule. This is the most cellular and biologically active stage.
Cells align along lines of tension and collagen accumulates; nodules become denser and more fibrous. In the hand this is when cords form, but in the foot contracture is uncommon.
The lesion becomes acellular and collagen-rich. This mature collagen explains the characteristic low signal on MRI and the firm clinical feel.
Why the Foot Behaves Differently from the Hand
A high-yield exam concept is that, although the biology is shared with Dupuytren's, the clinical behaviour differs:
- Plantar disease tends to remain nodular, whereas palmar disease forms contracting cords.
- Toe contractures are rare because the digital extensions of the plantar fascia and the toe anatomy resist the same contracting deformity seen in fingers.
- Nodules sit on the non-weight-bearing instep, so they may be present a long time before they hurt.
Relevant Anatomy
Central band (thickest, from medial calcaneal tuberosity to the toes), medial band (thin, over abductor hallucis), and lateral band (over abductor digiti minimi). Lederhose disease targets the medial side of the central band.
The instep is not the primary weight-bearing surface; the heel pad and metatarsal heads are. Nodules therefore cause symptoms mainly with direct shoe pressure and during push-off rather than constant standing pain.
The medial and lateral plantar nerves and vessels run deep to the fascia. During fasciectomy these are at risk, and a painful plantar scar can itself be disabling - hence the emphasis on careful incision planning.
According to PubMed, pedobarography in painful Lederhose disease shows patients offload the midfoot and shift load toward the heel and toes during walking - an adaptive antalgic gait.
Classification
Pattern-Based Grouping
There is no single universally accepted classification, but lesions are usefully grouped by extent, which guides how aggressive surgery needs to be:
- Description
- Single discrete nodule
- Skin / Deep Attachment
- None
- Surgical Strategy
- Conservative first; local recurrence if simply shelled out
- Description
- Several nodules, one band
- Skin / Deep Attachment
- Usually none
- Surgical Strategy
- Conservative; subtotal fasciectomy if symptomatic
- Description
- Nodule tethered to dermis
- Skin / Deep Attachment
- Dermal attachment
- Surgical Strategy
- Wide excision, may need skin coverage
- Description
- Multiple bands, deep extension
- Skin / Deep Attachment
- Deep and/or dermal
- Surgical Strategy
- Total plantar fasciectomy
The more diffuse and attached the disease, the wider the excision needed and the higher the recurrence risk.
Clinical Presentation
History
Patients typically describe a firm lump in the instep of the foot, often present for months to years. Pain is variable and frequently provoked by:
- Direct pressure from shoes
- Prolonged standing and the push-off phase of gait
- Walking on hard surfaces
A history of fibromatosis elsewhere (Dupuytren's in particular) is an important clue and should be actively sought, along with risk associations such as diabetes, alcohol use, anticonvulsant therapy, and liver disease.
Examination
Visible fullness over the medial arch in larger lesions. Skin is usually intact; check for dimpling or tethering that suggests dermal involvement.
One or more firm, fixed nodules within the plantar fascia, classically on the medial central band. They move with the fascia, not the skin, unless tethered.
Assess for toe contracture - usually absent in plantar disease. Significant fixed toe deformity is unusual and should prompt reassessment of the diagnosis.
Examine the palms for Dupuytren's nodules or cords - the strongest associated finding and a frequent exam point.
On a foot-and-ankle clinical case, the examiner wants you to (1) localise a firm medial instep nodule within the plantar fascia, (2) confirm toes are not contracted, and (3) turn the hands over to look for associated Dupuytren's disease. Doing all three signals you understand it is a systemic fibromatosis.


Investigations
Imaging Pathway
According to PubMed, ultrasound is the first-line investigation and is usually sufficient to confirm the diagnosis, while MRI is reserved for aggressive, recurrent, or atypical lesions and to exclude a sarcoma.
- 1
Clinical assessment
Firm medial instep nodule, check toes, examine hands for Dupuytren's
- 2
Ultrasound (first-line)
Well-defined, iso- to hypoechoic nodule arising from the plantar fascia; confirms most cases
- 3
MRI (selected cases)
Aggressive, recurrent, large, or atypical lesions; low T1 and characteristically low T2 signal from dense collagen
- 4
Plain radiograph
Usually normal; excludes bony pathology and rare calcification
- 5
Biopsy / excision histology
If features are atypical or malignancy cannot be excluded confidently
Imaging Features
- Typical Finding
- Well-demarcated, iso/hypoechoic nodule in the fascia, fusiform
- Role
- First-line, confirms most cases
- Typical Finding
- Low to intermediate signal
- Role
- Defines extent for surgery
- Typical Finding
- Characteristically LOW signal (dense collagen)
- Role
- Helps distinguish from cystic/cellular masses
- Typical Finding
- Usually normal soft-tissue mass; no bony change
- Role
- Excludes bone pathology
Most plantar masses are benign, but a rapidly enlarging, deep, painful, or atypical lesion must be treated as a possible soft-tissue sarcoma. According to PubMed, MR features of fibromatosis overlap with other soft-tissue tumours; when in doubt, image with MRI and obtain histological confirmation rather than assuming a benign fibroma.
Histology
Excised tissue shows bland fibroblastic and myofibroblastic proliferation with abundant collagen and a low mitotic rate. There is no cellular atypia or necrosis, confirming the benign nature and distinguishing it from sarcoma.
Management
Principles
The two governing principles are: start conservatively, and if you must operate, excise widely. Most patients never need surgery, and surgery itself carries a meaningful recurrence and wound-complication burden.
- 1
Confirm diagnosis
Clinical + ultrasound; MRI/biopsy if atypical
- 2
Conservative care (first-line)
Orthotics with nodule relief, soft padding, footwear modification, activity change, stretching
- 3
Adjuncts for refractory cases
Intralesional corticosteroid; consider radiotherapy or other agents in selected centres
- 4
Surgery if conservative care fails
Wide subtotal or total plantar fasciectomy, not local nodule excision
- 5
Rehabilitation and surveillance
Wound care, gradual loading, monitor for recurrence
Conservative Management (First-Line)
Custom insoles with a relief (cut-out) around the nodule redistribute pressure away from the lesion. This is the mainstay and helps most symptomatic patients avoid surgery.
Soft, wide, cushioned shoes and activity modification reduce direct nodule loading. Simple measures are effective for many.
Plantar fascia and calf stretching may help symptoms. According to PubMed, conservative regimens combining orthoses, medication, and physical therapy can control symptoms effectively.
Intralesional corticosteroid is used for painful nodules. Reviews also describe collagenase, verapamil, tamoxifen, imatinib, and shockwave therapy, but evidence is limited and these are not standard first-line care.
Radiotherapy
According to PubMed, low-dose radiotherapy can reduce the recurrence rate after surgery for plantar fibromatosis, but it is associated with significant functional side effects and should be used very selectively. It is sometimes offered for early or recurrent disease in specialised centres rather than as routine treatment.
Complications
Disease-Related
Symptomatic nodules cause pressure pain and altered gait, offloading the midfoot during walking.
Nodules may enlarge or multiply; aggressive forms can rarely cause toe contracture or fascial shrinkage, though this is uncommon.
Treatment-Related
- Cause / Context
- Incomplete excision of diffusely abnormal fascia
- Mitigation
- Wide subtotal/total fasciectomy; selective radiotherapy
- Cause / Context
- Scar on a loaded surface
- Mitigation
- Careful incision placement, off weight-bearing line
- Cause / Context
- Thin plantar flaps, tension
- Mitigation
- Atraumatic technique, plan skin coverage if tethered
- Cause / Context
- Medial/lateral plantar nerve branches
- Mitigation
- Careful deep dissection
- Cause / Context
- Soft-tissue/skin effects
- Mitigation
- Use very selectively; counsel on side effects
Clinical Relevance & Exam Focus
Why Examiners Like This Topic
Lederhose disease is a favourite discriminator topic because it tests whether you understand the superficial fibromatosis family as a whole. A strong candidate links it to Dupuytren's and Peyronie's, knows the medial central band location, states that toe contractures are rare, applies a conservative-first philosophy, and explains why wide excision is needed when surgery is unavoidable.
Practical Take-Home Points
Always examine the hands (and ask about Peyronie's) - it reframes the case as a systemic fibromatosis.
Orthotics with nodule relief and footwear changes solve most symptomatic cases; do not rush to operate.
Local nodule excision recurs; wide fasciectomy is the durable operation. Plan the incision to avoid a painful plantar scar.
Atypical, deep, or rapidly growing masses need MRI and histology - never assume benign.
Guidelines, Registries & Global Practice
Evidence and Practice Synthesis
There are no large randomised trials or dedicated international guidelines for plantar fibromatosis given its rarity; practice is guided by case series, narrative reviews, and extrapolation from Dupuytren's disease. The globally consistent themes are summarised below.
- Consensus Position
- Conservative (orthotics, padding, footwear, activity)
- Evidence Basis
- Reviews; most patients avoid surgery
- Consensus Position
- Ultrasound first-line; MRI for atypical/aggressive lesions
- Evidence Basis
- Imaging reviews
- Consensus Position
- Wide subtotal or total fasciectomy, not local excision
- Evidence Basis
- Case series show lowest recurrence with wider excision
- Consensus Position
- Effective at reducing recurrence but selective use due to morbidity
- Evidence Basis
- Surgical/radiotherapy series
- Consensus Position
- Atypical masses imaged with MRI and confirmed histologically
- Evidence Basis
- Imaging overlap with soft-tissue tumours
Global Epidemiology Notes
- Population data are sparse; a Netherlands study estimated roughly 1.2 plantar fibromatosis operations per 100,000 people per year, reflecting how rarely the condition reaches surgery.
- The condition is reported worldwide across all regions, predominantly in middle-aged and older adults with a male predominance and a strong association with Dupuytren's disease.
Resource-Setting Variation
In settings with ready access to orthotic services, the conservative-first pathway is straightforward. Where custom orthoses are less accessible, simple footwear modification and padding remain effective and low-cost. Radiotherapy and sarcoma multidisciplinary pathways are concentrated in specialist centres, so referral may be required for aggressive, recurrent, or atypical disease.
Why the MRI Signal Varies with Disease Phase
The topic teaches low T2 signal as the rule and separately describes the proliferative-involutional-residual phases, but never links the MRI signal to the phase - which is why an early nodule can look worrying.
- Mature (residual) lesions are dark. A collagen-rich, hypocellular nodule is low signal on both T1 and T2 and enhances little - the 'classic' fibrous appearance.
- Early (proliferative) lesions are brighter. A cellular, actively proliferating nodule has more cells and water, so it shows higher T2 signal and avid contrast enhancement - and can mimic a more aggressive soft-tissue tumour.
- Why it matters. The signal therefore tracks the disease phase, and this overlap with sarcoma on early cellular lesions is exactly why an atypical mass needs histological confirmation rather than being assumed benign.
Q: Why does the MRI signal of plantar fibromatosis vary, and what does it reflect?
A: It tracks the disease phase / cellularity. A mature, collagen-rich (residual) nodule is low on both T1 and T2 with little enhancement - the 'classic' fibrous look. An early, cellular (proliferative) nodule has more cells and water, so it is higher on T2 with avid enhancement and can mimic a soft-tissue sarcoma. That overlap is why an atypical or cellular-looking lesion needs histological confirmation, not assumption.
Why Radiotherapy and the Medical Agents Work
The management lists radiotherapy, collagenase, verapamil, tamoxifen, imatinib and shockwave but never explains why they work or why the disease phase matters.
- Radiotherapy targets proliferating cells. Low-dose radiotherapy damages the actively proliferating (myo)fibroblasts of the early/proliferative phase, so it is used for early or recurrent disease and as a post-operative adjuvant to lower recurrence; it does little for a mature, acellular residual nodule and carries skin/functional morbidity - hence selective use.
- The medical agents hit the same biology. Collagenase enzymatically lyses collagen; verapamil reduces collagen synthesis and increases collagenase; tamoxifen lowers TGF-beta-driven myofibroblast activity; imatinib inhibits fibroblast tyrosine-kinase signalling; and intralesional corticosteroid is anti-proliferative - but the evidence for all is limited, so they remain adjuncts.
- The unifying principle. All of these work best on active, proliferative disease; once the nodule is mature collagen, only excision removes it - which is why treatment is staged from conservative and biological measures early to wide fasciectomy for established, refractory disease.
Q: Why does radiotherapy work in plantar fibromatosis, and when is it used?
A: Low-dose radiotherapy damages the actively proliferating (myo)fibroblasts of the early/proliferative phase - so it is used for early or recurrent disease and as a post-operative adjuvant to reduce recurrence; it does little for a mature acellular residual nodule and has skin/functional morbidity (selective use). The medical adjuncts (collagenase, verapamil, tamoxifen, imatinib, steroid, shockwave) likewise target the myofibroblast/collagen biology and work best on active disease - once the nodule is mature collagen, only excision removes it.
MCQ Practice Points
Q: Where do plantar fibromatosis nodules characteristically arise? A: On the medial part of the central band of the plantar aponeurosis - the non-weight-bearing instep. They are not centred under the heel pad, which is why pain is often related to footwear pressure and push-off.
Q: How does plantar fibromatosis differ clinically from Dupuytren's disease? A: Plantar disease tends to remain nodular and rarely causes toe contractures, whereas Dupuytren's forms contracting cords that flex the fingers. Both share myofibroblast biology and frequently coexist.
Q: Why is wide fasciectomy preferred over local nodule excision? A: Because the entire plantar fascia is diffusely abnormal, leaving fascia behind predictably recurs. According to PubMed, plantar fasciectomy is the operation of choice and wider excision gives the lowest recurrence, though it carries more wound morbidity.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with a firm, slowly growing lump in the arch of his right foot, painful when wearing dress shoes. He has Dupuytren's nodules in both palms. How would you assess and manage this patient?”
“A 48-year-old woman had a plantar nodule excised two years ago and now has multiple recurrent nodules along the same fascia with significant pain. She has a strong family history of Dupuytren's disease. How do you proceed?”
“A 40-year-old man presents with a deep, firm, mildly painful plantar mass that he says has grown noticeably over three months. Ultrasound shows an ill-defined lesion. How do you approach this?”
Core Concept
- Benign fibroproliferative disorder of the plantar aponeurosis
- Pathological cell = myofibroblast producing excess collagen
- One of the superficial fibromatoses (with Dupuytren's, Peyronie's)
- Nodules on the MEDIAL CENTRAL BAND (instep, not heel)
- Toe contractures are RARE (key difference from the hand)
Associations (FEET DAB)
- Fibromatoses elsewhere (Dupuytren's, Peyronie's) - strongest clue
- Epilepsy medication (anticonvulsants)
- Ethanol (alcohol)
- Trauma / repetitive vibration
- Diabetes mellitus
- Aging; and liver disease
Clinical Assessment
- Firm fixed nodule in the plantar fascia, painful with shoe pressure
- Confirm toes are NOT contracted
- ALWAYS examine the hands for Dupuytren's disease
- Antalgic gait offloads the midfoot (pedobarography)
Investigations
- Ultrasound = first-line, confirms most cases
- MRI for aggressive/atypical lesions; low T1 and characteristically LOW T2 signal (collagen)
- Radiograph usually normal
- Biopsy/histology if malignancy cannot be excluded
Management Ladder
- 1. Conservative FIRST: orthotic with nodule relief, padding, footwear, activity change
- 2. Adjuncts: intralesional steroid; other agents have limited evidence
- 3. Surgery only if conservative care fails
- 4. Operation of choice = WIDE subtotal/total fasciectomy (NOT local excision)
- 5. Radiotherapy reduces recurrence but is morbid - use selectively
Surgical Pearls
- Local nodule excision = highest recurrence (avoid)
- Wider excision = lower recurrence but more wound morbidity
- Plan incision off the weight-bearing line to avoid painful scar
- Protect medial/lateral plantar nerves and vessels
- Counsel that recurrence is common
Do Not Miss
- Rapidly growing, deep, ill-defined mass = exclude SARCOMA
- Use MRI + histology before definitive surgery if atypical
- Refer atypical lesions through a sarcoma MDT
- Never assume a plantar mass is a benign fibroma
Evidence & Key Studies
- Comprehensive review framing plantar fibromatosis within the superficial fibromatosis family alongside Dupuytren's and Peyronie's disease
- Associations described include trauma, diabetes mellitus, anticonvulsant use, alcohol consumption, and liver disease
- Ultrasound confirms diagnosis; MRI reserved for aggressive and advanced lesions
- Wide range of conservative options reported (steroids, verapamil, imatinib, radiotherapy, shockwave, tamoxifen, collagenase); surgery reserved for failed conservative care, with expected recurrence
- Population estimate of about 1.2 operations for plantar fibromatosis per 100,000 people per year in the Netherlands
- Plantar fasciectomy associated with the lowest recurrence rate of the surgical options studied
- Microscopically incomplete excision or excision of early recurrence alone led to recurrence in essentially all cases
- Adjuvant radiotherapy reduced recurrence but caused significantly impaired functional outcome in some patients
- Classifies fibromatoses into superficial (including plantar) and deep groups with shared histology
- MRI shows prominent low to intermediate signal with bands of low signal reflecting highly collagenised tissue
- Less collagenous, more cellular lesions can show non-specific high T2 signal, overlapping with other tumours
- Local recurrence after surgical resection is frequent due to infiltrative growth
- Pedobarography in 41 patients with painful Ledderhose disease versus 41 controls
- Patients shifted plantar load toward the heel, hallux, and toes
- Patients offloaded the medial and lateral midfoot regions during walking
- Force-time integral changes were most prominent at heel, medial midfoot, hallux, and toes
- Patient with concomitant Dupuytren's disease and plantar fibromatosis who failed all conservative measures
- Treated with subtotal fasciectomy via a carefully planned plantar incision
- Prompt and complete symptom relief with no recurrence at 2-year follow-up
- Emphasises incision choice to avoid painful scarring, skin necrosis, and shoe-wearing difficulty