Idiopathic AVN | Ages 4-8 | Containment Principle | Remodeling Potential
HERRING LATERAL PILLAR CLASSIFICATION
Critical Must-Knows
- Idiopathic AVN of the femoral head in children aged 4-8 years
- Containment principle: maintain femoral head within acetabulum during remodeling
- Herring lateral pillar is most reliable prognostic classification
- Age at onset is the most important prognostic factor (worse if older than 8)
- Natural history: necrosis → fragmentation → reossification → remodeling (2-4 years)
Clinical Pearls
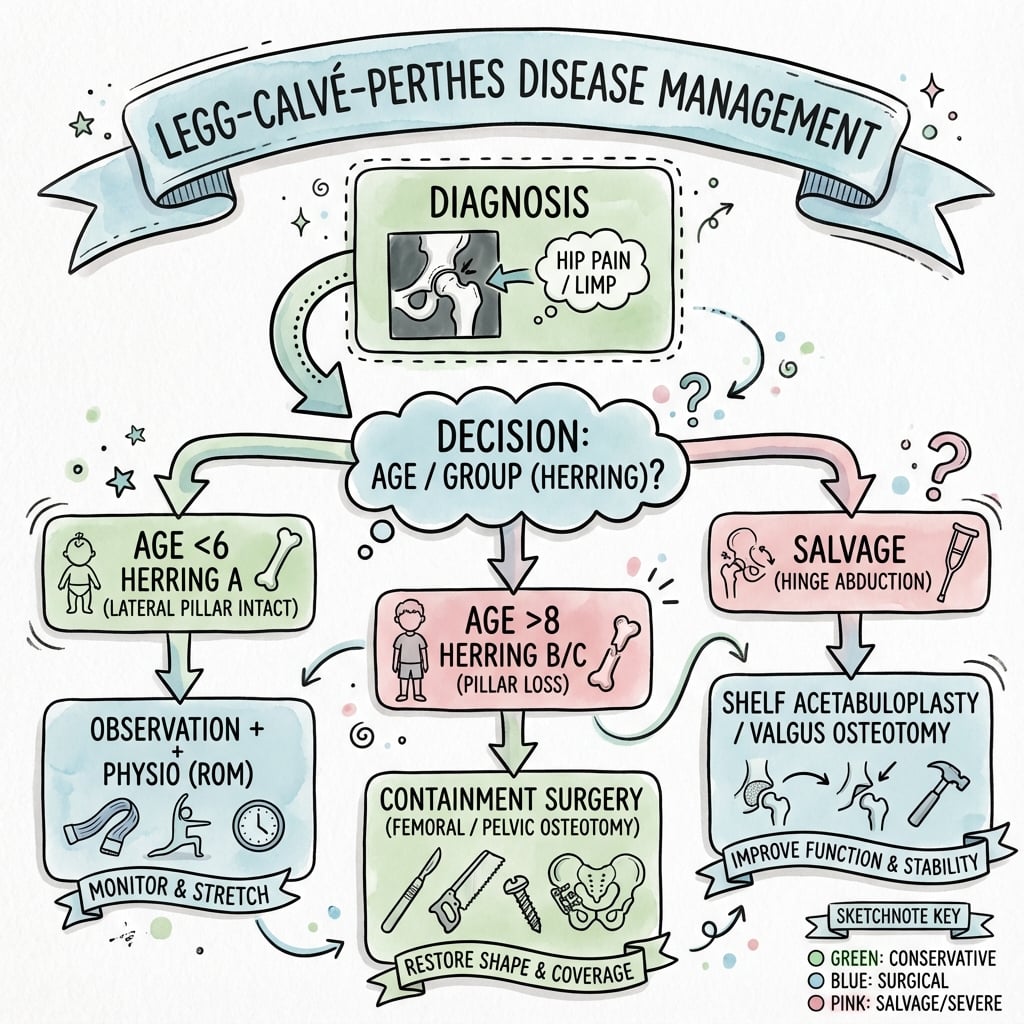
- "Legg-Calvé-Perthes disease is self-limiting but outcome depends on containment
- "Herring B at age under 8 = observation; age over 8 = containment surgery
- "Goal is spherical femoral head at skeletal maturity to prevent early arthritis
- "Containment options: varus osteotomy, Salter osteotomy, or shelf procedure
Clinical Imaging
Imaging Gallery




Critical Perthes Disease Exam Points
Containment Principle
The goal is to maintain the soft, fragmented femoral head within the acetabulum during reossification. This allows the acetabulum to act as a mold, promoting a spherical femoral head. Loss of containment leads to extrusion and permanent deformity.
Prognostic Factors
Age at onset is most important - children under 6 have excellent prognosis, over 8 have poor outcomes. Herring C (more than 50% lateral pillar collapse), B/C border (borderline B), and female gender are poor prognostic signs.
Herring Classification
The Herring lateral pillar classification is the most reliable system. Measured at maximal fragmentation stage. Group A = intact lateral pillar, B = less than 50% height loss, B/C = exactly 50%, C = more than 50% collapse.
Treatment by Age
Under age 6: observation regardless of classification. Ages 6-8: Herring B/C and C may benefit from containment. Over age 8: even Herring B may need surgery. Natural history is 2-4 years from onset to healing.
Quick Decision Guide - Treatment by Age and Herring Group
| Age | Herring Group | Treatment | Key Pearl |
|---|---|---|---|
| Under 6 years | Any (A, B, C) | Observation, ROM exercises | Excellent prognosis - remodeling potential high |
| 6-8 years | A or B | Observation, ROM exercises | Good prognosis with careful monitoring |
| 6-8 years | B/C or C | Containment surgery (femoral or pelvic osteotomy) | Critical age - intervention may improve outcome |
| Over 8 years | B | Consider containment surgery | Limited remodeling - may need surgery even for B |
| Over 8 years | B/C or C | Salvage procedures (valgus osteotomy, shelf) or arthroplasty long-term | Poor prognosis - focus on pain relief and function |
PERTHESPERTHES - The Disease Process
| P | Peak age 4-8 years Most common presentation age |
| E | Epiphyseal AVN Idiopathic avascular necrosis of femoral head |
| R | Revascularization occurs Natural healing over 2-4 years |
| T | Time dependent outcome Age at onset critical prognostic factor |
| H | Head must stay contained Containment principle |
| E | Extrusion is bad Loss of containment = poor outcome |
| S | Spherical head = good result Goal at skeletal maturity |
| P | Peak age 4-8 years Most common presentation age | T | Time dependent outcome Age at onset critical prognostic factor | S | Spherical head = good result Goal at skeletal maturity |
| E | Epiphyseal AVN Idiopathic avascular necrosis of femoral head | H | Head must stay contained Containment principle | ||
| R | Revascularization occurs Natural healing over 2-4 years | E | Extrusion is bad Loss of containment = poor outcome |
Hook:PERTHES reminds you this is a TIME-dependent disease where CONTAINMENT during revascularization determines outcome
NFRRSTAGES - Natural History of Perthes
| N | Necrosis (initial stage) Avascular necrosis, minimal X-ray changes |
| F | Fragmentation (3-12 months) Collapse and fragmentation visible, most deformity occurs |
| R | Reossification (12-36 months) New bone formation, revascularization |
| R | Remodeling (residual stage) Final shape determined, continues to skeletal maturity |
| N | Necrosis (initial stage) Avascular necrosis, minimal X-ray changes | R | Reossification (12-36 months) New bone formation, revascularization |
| F | Fragmentation (3-12 months) Collapse and fragmentation visible, most deformity occurs | R | Remodeling (residual stage) Final shape determined, continues to skeletal maturity |
Hook:NFRR = Natural Four-stage Revascularization and Remodeling
LATELATE - Poor Prognostic Features
| L | Lateral pillar collapse Herring C (more than 50% collapse) |
| A | Age over 8 years Most important poor prognostic factor |
| T | Total head involvement Catterall IV, complete head necrosis |
| E | Extrusion of head Loss of containment, uncovered laterally |
| L | Lateral pillar collapse Herring C (more than 50% collapse) | T | Total head involvement Catterall IV, complete head necrosis |
| A | Age over 8 years Most important poor prognostic factor | E | Extrusion of head Loss of containment, uncovered laterally |
Hook:LATE presentation = LATE poor outcome
GLEAMHEAD AT RISK Signs (Catterall)
| G | Gage sign V-shaped lucency at lateral epiphysis |
| L | Lateral calcification Calcification lateral to epiphysis |
| E | Epiphyseal extrusion Lateral subluxation of head |
| A | Abnormal metaphysis Metaphyseal cysts or irregularity |
| M | Metaphyseal rarefaction Diffuse osteopenia |
| G | Gage sign V-shaped lucency at lateral epiphysis | A | Abnormal metaphysis Metaphyseal cysts or irregularity |
| L | Lateral calcification Calcification lateral to epiphysis | M | Metaphyseal rarefaction Diffuse osteopenia |
| E | Epiphyseal extrusion Lateral subluxation of head |
Hook:GLEAM = signs that make the prognosis less bright (poor outcome predictors)
COVERContainment Treatment Principle
| C | Contain head in socket Treatment principle |
| O | Osteotomy options Femoral or pelvic |
| V | Varus femoral osteotomy Redirects head into socket |
| E | Extend coverage Pelvic osteotomy adds coverage |
| R | Remodel as spherical Goal of treatment |
| C | Contain head in socket Treatment principle | E | Extend coverage Pelvic osteotomy adds coverage |
| O | Osteotomy options Femoral or pelvic | R | Remodel as spherical Goal of treatment |
| V | Varus femoral osteotomy Redirects head into socket |
Hook:COVER the head for containment - the key treatment principle!
Overview and Epidemiology
Legg-Calvé-Perthes disease (also called Perthes disease or coxa plana) is idiopathic avascular necrosis of the femoral head in children. It is a self-limiting condition characterized by interruption of blood supply to the femoral epiphysis, followed by necrosis, fragmentation, revascularization, and remodeling.
Key features:
- Idiopathic AVN - cause unknown (unlike traumatic or sickle cell AVN)
- Self-limiting - natural history is 2-4 years from onset to healing
- Outcome depends on containment - maintaining head within acetabulum during healing
- Remodeling potential - younger children have excellent potential for recovery
Why 'Idiopathic'?
Unlike other causes of AVN in children (trauma, sickle cell, steroid use), Perthes disease has no identifiable cause. Theories include repetitive trauma, coagulopathy, or anatomical vascular watershed area, but none are proven.
Epidemiology:
Demographics
- Age: 4-8 years (peak 5-6 years)
- Gender: boys predominate, roughly 3-5:1 (3.1:1 in Swedish national data, Johansson 2016)
- Race: higher in those of Nordic/Caucasian and Asian background; lower in African ancestry
- Stature: often shorter, delayed bone age
Associations
- Low birth weight (below 2.5 kg)
- Delayed skeletal maturation (bone age)
- Lower socioeconomic status
- Second-hand smoke exposure
- NOT associated with activity level
Pathophysiology and Natural History
Blood supply to the femoral head:
The pediatric femoral head receives blood from:
- Lateral epiphyseal vessels (branches of medial femoral circumflex) - primary supply
- Foveal vessels (from ligamentum teres) - minimal in young children
- Metaphyseal vessels - blocked by growth plate
Vascular Anatomy in Children
Unlike adults, children have no metaphyseal contribution across the growth plate. The lateral epiphyseal vessels are the only significant blood supply to the femoral head before age 7-8. This makes the pediatric femoral head vulnerable to ischemia if these vessels are interrupted.
Pathophysiology theories:
- Vascular occlusion - thrombosis of lateral epiphyseal vessels (? coagulopathy)
- Repetitive microtrauma - mechanical stress on vulnerable vessels
- Anatomical watershed - terminal vessels predisposed to ischemia
- Venous outflow obstruction - increased intraosseous pressure
Natural history - four stages:
Waldenström Stages
Initial ischemic event. Minimal X-ray changes. Child develops limp and pain.
- Dense femoral head on X-ray (dead bone more dense)
- Widened joint space (synovitis, cartilage thickening)
Fragmentation and collapse. Most deformity occurs during this stage. This is when classification systems are applied.
- Subchondral fracture (crescent sign)
- Collapse and fragmentation of epiphysis
- Herring classification applied at maximal fragmentation
Revascularization and new bone formation. Head begins to reform shape.
- New bone replaces necrotic bone
- Gradual restoration of density
- Containment critical during this phase
Final remodeling. Shape at end of this stage determines long-term outcome.
- Acetabulum and femoral head remodel together
- Final sphericity determined
- Goal: spherical congruent head at skeletal maturity
Fragmentation Stage Critical
The fragmentation stage (stage II) is when the femoral head is most vulnerable. This is when:
- Most collapse and deformity occur
- Classification systems are applied (Herring at maximal fragmentation)
- Loss of containment leads to extrusion
- Containment treatment must be initiated if indicated
The Containment Principle:
The biological rationale for containment:
- The femoral head is soft and moldable during reossification
- The acetabulum acts as a mold to shape the reossifying head
- If the head extrudes laterally (loses containment), it reossifies in a non-spherical, mushroom shape
- Maintained containment → spherical head → good long-term outcome
- Lost containment → aspherical head → early osteoarthritis
Classification Systems
Multiple classification systems exist, but Herring lateral pillar is most reliable for prognosis and treatment decisions.
Herring Lateral Pillar Classification
Most commonly used and most reliable prognostic system. Applied at maximal fragmentation stage.
| Group | Lateral Pillar Height | Prognosis | Treatment (age dependent) |
|---|---|---|---|
| A | No loss of height (100%) | Excellent | Observation at all ages |
| B | Less than 50% height loss | Good if under 8; guarded if over 8 | Observation under 8; consider containment over 8 |
| B/C Border | Exactly 50% height loss (borderline) | Intermediate (acts like C in practice) | Containment recommended age over 6 |
| C | More than 50% height loss or total collapse | Poor | Salvage procedures or palliative treatment |
How to Measure Lateral Pillar
Lateral pillar is the lateral 15-30% of the epiphysis on AP X-ray. Compare affected to normal side. Measure at maximal fragmentation (peak of stage II). If borderline between B and C (exactly 50%), classify as B/C border - treat as high-risk.
Clinical Presentation and Assessment
Typical presentation:
History
- Age: 4-8 years (peak 5-6)
- Chief complaint: painless limp or mild hip/thigh/knee pain
- Onset: insidious over weeks to months
- Activity: pain worse with activity, better with rest
- Duration: symptoms present for weeks before presentation
Examination
- Gait: antalgic limp (painful gait)
- ROM: limited abduction and internal rotation (early sign)
- Trendelenburg: positive (abductor weakness from pain)
- Leg length: may have apparent shortening
- Muscle atrophy: thigh atrophy (chronic presentation)
Physical examination findings:
Key findings in order of sensitivity:
- Limited abduction - most sensitive early sign
- Limited internal rotation - especially in flexion
- Muscle spasm - protective spasm in hip flexors, adductors
- Leg length discrepancy - apparent shortening from muscle spasm
- Trendelenburg gait - abductor dysfunction
Irritable Hip vs Perthes
Transient synovitis (irritable hip) is the main differential. Key distinguishing features:
- Synovitis: acute onset (days), full ROM recovery in 1-2 weeks, normal X-rays
- Perthes: insidious onset (weeks), persistent ROM loss, X-ray changes within 4-8 weeks
- Rule: If X-ray normal but ROM restriction persists more than 3 weeks, repeat X-ray or get MRI
Differential diagnosis:
Differential Diagnosis of Limping Child with Hip Pain
| Condition | Age | Key Features | X-ray Findings |
|---|---|---|---|
| Perthes disease | 4-8 years | Insidious onset, persistent ROM loss | Sclerotic femoral head, crescent sign |
| Transient synovitis | 2-10 years | Acute onset, resolves in 1-2 weeks | Normal or widened joint space |
| Septic arthritis | Any age | Acute, fever, refuses weight-bearing, toxic | Widened joint space, effusion |
| SCFE | 10-14 years (adolescent) | Acute or chronic, obligate external rotation | Posterior-inferior slip on frog lateral |
| DDH (residual dysplasia) | Toddler to child | Waddling gait, Trendelenburg | Shallow acetabulum, subluxation |
Investigations
Imaging Protocol
AP pelvis and frog-leg lateral of both hips.
- AP pelvis: assess symmetry, lateral pillar height, extrusion
- Frog-leg lateral: crescent sign, extent of involvement
- Both hips: 10-15% bilateral, need to identify
Gold standard for early diagnosis before X-ray changes visible.
- T1: low signal in necrotic epiphysis
- T2: variable signal, may show hyperemia
- Gadolinium: lack of enhancement in necrotic area
- Indications: normal X-ray but persisting symptoms beyond 3 weeks
Historically used for early diagnosis. Now largely replaced by MRI.
- Shows photopenic area (cold spot) in femoral head
- Less anatomical detail than MRI
Intraoperative arthrography to assess containment if considering surgery.
- Shows cartilaginous head contour
- Assesses whether head contained in abduction-internal rotation

Radiographic signs by stage:
| Stage | AP Radiograph | Frog-Leg Lateral |
|---|---|---|
| Necrosis (I) | Dense (sclerotic) femoral head, widened joint space | Subtle density change |
| Fragmentation (II) | Collapsed epiphysis, lateral pillar assessment, extrusion | Crescent sign (subchondral fracture), fragmentation |
| Reossification (III) | Mixed sclerosis and lucency, gradual increase in density | Improving contour |
| Remodeling (IV) | Final head shape visible, coxa magna, short neck | Final congruence assessment |
Crescent Sign
The crescent sign is a subchondral lucency on frog-leg lateral representing fracture through the necrotic epiphysis. It appears early, often before fragmentation visible on AP. It is a Salter-Thompson classification feature and indicates significant involvement.
Key radiographic measurements:
- Lateral pillar height: compare affected to normal side (Herring classification)
- Extrusion index: percentage of femoral head lateral to Perkin's line (normal less than 20%)
- Epiphyseal quotient: width of affected epiphysis / normal side (measures coxa magna)
Management Algorithm
Treatment depends on age at onset and extent of involvement (Herring classification).
General principles:
- Goal: spherical, congruent femoral head at skeletal maturity
- Containment: maintain head within acetabulum during reossification
- ROM: maintain hip ROM to prevent stiffness
- Natural history: disease lasts 2-4 years regardless of treatment
Management: Observation
Children under 6 have excellent prognosis regardless of classification due to high remodeling potential.
Treatment Protocol
- Reassure family: excellent prognosis at this age
- Activity: normal activity as tolerated, avoid high impact initially
- Analgesia: NSAIDs for pain (ibuprofen)
- Goal: maintain abduction and internal rotation
- Method: physical therapy, swimming, cycling
- Avoid: prolonged immobilization (causes stiffness)
- X-rays: every 3-4 months until reossification complete
- Watch for: progression to Herring C, increasing extrusion
- Duration: follow for 2-4 years through all stages
- Most achieve Stulberg I-II (excellent)
- Even Herring C at age under 6 often remodels well
Why Observation Under 6?
Children under 6 have tremendous remodeling potential. Even with significant collapse (Herring C), the acetabulum and femoral head remodel together over years, achieving sphericity by skeletal maturity. Surgery does not improve outcomes at this age.

Surgical Techniques
Proximal Femoral Varus Osteotomy
Most common containment procedure for Perthes disease.
Goal: Redirect femoral head into acetabulum by creating varus angulation.
Surgical Steps
- Arthrogram: confirm head contained in abduction-internal rotation
- Template: plan degree of varus (typically 10-15 degrees)
- Calculate: amount of varus, derotation needed
- Position: supine on radiolucent table
- Approach: lateral approach to proximal femur
- Expose subtrochanteric region
- Level: subtrochanteric (below lesser trochanter)
- Cut: transverse or oblique based on plan
- Correction: 10-15 degrees varus, +/- derotation
- Check: intraoperative X-ray to confirm containment
- Implant: pediatric blade plate or locking plate
- Stability: ensure stable fixation for early motion
- Irrigate, close in layers
- Spica cast 4-6 weeks (some surgeons)
- Protected weight-bearing 6-8 weeks
- ROM exercises immediately
- Monitor for reossification on serial X-rays
Advantages:
- Redirects femoral head into acetabulum
- Allows early ROM
- Good containment if well-planned
Disadvantages:
- Leg length discrepancy (shortening)
- Trendelenburg gait if excessive varus
- Hardware removal often needed
- Risk of AVN from surgical trauma
How Much Varus?
Typical varus is 10-15 degrees. More varus improves containment but increases Trendelenburg risk. Use intraoperative arthrogram to confirm head contained in planned position before fixation. Avoid excessive varus (more than 20 degrees) due to abductor dysfunction.
Complications
Complications of Perthes Disease and Treatment
| Complication | Incidence/Risk | Prevention/Management |
|---|---|---|
| Poor final head shape (coxa plana) | Common with Herring C, age over 8, inadequate containment | Containment surgery in appropriate candidates, accept and plan for arthroplasty |
| Early osteoarthritis (Stulberg IV-V) | High risk if aspherical head at maturity, often before age 50 | Optimize final head shape with containment, THA when symptomatic |
| Leg length discrepancy | Common (overgrowth from hyperemia or shortening from collapse) | Monitor, shoe lift if more than 2cm, consider epiphysiodesis |
| Hip stiffness (loss of ROM) | Common if prolonged immobilization or severe disease | Early ROM exercises, avoid prolonged casting |
| Hinge abduction | Aspherical head impinges on lateral acetabulum | Recognize on exam (pain in abduction), valgus osteotomy if symptomatic |
| Trendelenburg gait | Abductor dysfunction from excessive varus osteotomy or coxa vara | Avoid excessive varus (more than 20 degrees), strengthen abductors |
| Premature physeal closure | Rare, from ischemic injury to growth plate | Monitor growth, may need contralateral epiphysiodesis |
Long-term outcomes:
- Stulberg I-II: excellent long-term function, low risk of OA
- Stulberg III: moderate risk of OA, typically after age 50-60
- Stulberg IV-V: high risk of early OA, often requiring THA by age 40-50
Perthes is a Pediatric Diagnosis with Adult Consequences
The goal of treatment is not to cure Perthes (it is self-limiting), but to optimize the final head shape at skeletal maturity. An aspherical head (Stulberg IV-V) will lead to early osteoarthritis in the 4th-5th decade. Containment during active disease aims to prevent this outcome.
Postoperative Care and Rehabilitation
Post-surgical protocol varies by procedure type:
Post-Operative Timeline
- Immobilization: Spica cast or hip brace depending on surgeon preference
- Pain management: Multimodal analgesia (paracetamol, NSAIDs, opioids PRN)
- DVT prophylaxis: Usually not needed in pediatric patients
- Wound care: Drain removal at 24-48 hours, suture removal at 2 weeks
- Monitoring: Neurovascular checks (especially sciatic nerve)
- Weight-bearing: Non-weight-bearing or toe-touch weight-bearing
- Mobilization: Wheelchair or crutches
- ROM exercises: Begin gentle hip ROM if not in spica cast
- Radiographs: Check at 6 weeks for osteotomy healing
- Cast: If spica cast used, typically 4-6 weeks total
- Weight-bearing: Progressive from partial to full (based on X-ray healing)
- Physical therapy: Active ROM exercises, gentle strengthening
- Monitor: Serial X-rays to assess osteotomy healing and containment
- Return to school: Typically week 8-10 with activity restrictions
- Full weight-bearing: By 12 weeks typically
- Strengthening: Progressive hip and core strengthening
- Activity: Low-impact activities (swimming, cycling) from 3 months
- Sports: Return to contact sports at 6 months if healed
- Consideration: Blade plate removal typically at 12-18 months
- Timing: After osteotomy fully healed and reossification complete
- Not urgent: Can leave in situ if asymptomatic
Key Rehabilitation Principles:
ROM is Critical
Maintain hip ROM throughout treatment. Stiffness is common complication. Early ROM exercises prevent contractures and optimize final outcome. Focus on abduction and internal rotation.
Patient Compliance
Family education essential. Disease lasts 2-4 years. Parents must understand importance of activity modification, ROM exercises, and regular follow-up. Non-compliance worsens outcome.
Follow-up Schedule:
- Surgical cases: 2 weeks (wound), 6 weeks (healing), 3 months, 6 months, then every 6 months until reossification complete
- Non-operative cases: Every 3-4 months until reossification complete
- Long-term: Annually until skeletal maturity (assess final Stulberg classification)
- Transition: To adult services for ongoing OA risk monitoring
Rehabilitation Goals
The goal of post-operative rehabilitation (or observation protocol) is to:
- Maintain ROM - prevent stiffness
- Monitor containment - ensure head stays in acetabulum
- Optimize reossification - promote spherical head shape
- Return to function - age-appropriate activities The disease duration is the same whether treated or not (2-4 years) - treatment affects final head shape, not disease duration.
Outcomes and Prognosis
Prognostic factors:
Favorable (good prognosis):
- Age at onset under 6 years (most important)
- Herring A or B classification
- Less than 50% lateral pillar collapse
- Minimal extrusion (less than 20%)
- Male gender
- Maintained ROM
Unfavorable (poor prognosis):
- Age at onset over 8 years (most important)
- Herring B/C or C classification
- More than 50% lateral pillar collapse
- Significant extrusion (more than 20%)
- Female gender (worse at same age/classification)
- Restricted ROM, especially abduction
Outcomes by Age and Classification
| Age Group | Herring Classification | Typical Final Outcome (Stulberg) | Notes |
|---|---|---|---|
| Under 6 | Any (A, B, C) | Stulberg I-II (excellent) | High remodeling potential |
| 6-8 years | A or B | Stulberg I-III (good to moderate) | Containment may improve outcome for B |
| 6-8 years | B/C or C | Stulberg III-IV (moderate to poor) | Containment recommended |
| Over 8 | B | Stulberg III-IV (moderate to poor) | Limited remodeling even with treatment |
| Over 8 | C | Stulberg IV-V (poor) | Will likely need THA by age 40-50 |
Natural history without treatment:
- Under 6: most achieve good outcome (Stulberg I-III) even without surgery
- 6-8: variable, depends on extent (B/C and C often progress to Stulberg IV-V)
- Over 8: poor outcome common, especially Herring B/C or C
Effect of containment surgery:
- May improve outcome by 1 Stulberg class (IV → III) if done appropriately
- Most beneficial in age 6-8 with Herring B/C or C
- Limited benefit if too young (under 6) or too old (over 10)
Evidence Base and Key Studies
Herring IPSG Part II - Effect of Treatment on Outcome (Landmark)
- Prospective multicentre study: 438 patients (451 hips), all aged 6.0-12.0 years at onset; 345 hips followed to skeletal maturity
- Lateral pillar classification and age at onset were both strong independent prognostic factors (both p less than 0.001)
- In children over 8 years at onset with lateral pillar B or B/C border hips, surgical treatment (femoral or innominate osteotomy) gave significantly better outcomes than non-operative care (p of 0.05 or less)
- Group B hips in children 8 years or younger did equally well with operative and non-operative treatment; group C hips did poorly in all ages regardless of treatment
- Female patients did significantly worse than males if over 8 years at onset (p of 0.004)
Herring - Original Lateral Pillar Classification (Landmark)
- 93 hips in 86 brace-treated patients followed to maturity; original three-group system (A, B, C) applied in the fragmentation stage
- Group A had a uniformly good outcome (100% Stulberg I-II)
- Group B did well if under 9 years at onset (92% Stulberg I-II) but worse if over 9; group C became aspherical in the majority across both age groups
- Inter-observer agreement was 78%; the classification group was a stronger predictor of final outcome than age at onset
- Group C hips also had a longer duration of the fragmentation and reossification stages
Wiig Norwegian National Prospective Study (Landmark)
- Nationwide prospective study, 28 Norwegian hospitals, 425 children reported; 368 unilateral cases with 5-year follow-up
- Strongest predictor of outcome was femoral head involvement of more or less than 50% (OR 7.76), then age at diagnosis and lateral pillar classification
- In children over 6 years at diagnosis with more than 50% head necrosis, proximal femoral varus osteotomy gave significantly better outcomes than orthosis (p of 0.001) or physiotherapy (p of 0.001)
- No difference between physiotherapy and abduction orthosis; the authors recommended abandoning the orthosis
- No treatment effect was seen in children under 6 years at diagnosis
Stulberg - Natural History and Final-Outcome Classification (Landmark)
- Two cohorts (88 and 68 patients) followed an average of 40 and 30 years respectively; five classes of hip deformity defined at maturity
- Spherical congruency (classes I-II): osteoarthritis does not develop
- Aspherical congruency (classes III-IV): mild-to-moderate arthritis develops in late adulthood
- Aspherical incongruency (class V): severe arthritis develops before the age of 50
Yoo - Valgus Femoral Osteotomy for Hinge Abduction
- 31 hips with hinge abduction treated by valgus femoral osteotomy and followed to skeletal maturity
- Iowa Hip Score improved from 71 to 92; hip abduction, internal and external rotation all increased
- Final Stulberg grades were II in 4, III in 21 and IV in 6 hips - function improved more reliably than head sphericity
- Greater femoral-head remodelling was associated with younger age (under 10) and earlier disease stage (fragmentation/early reossification) at surgery
Larson - IPSG 20-Year Outcomes of Non-operative Treatment
- 56 patients (58 hips) from the prospective multicentre cohort, examined at a mean of 20 years after non-operative (range-of-motion or brace) treatment
- Only 26% of hips had no osteoarthritis; 30% had mild and 44% moderate-to-severe radiographic OA (Tonnis grade 2-3)
- Stulberg classification was the only factor independently associated with the Nonarthritic Hip Score (p of 0.003)
- Clinical signs of femoroacetabular impingement were associated with pain and poorer hip scores
Nakamura - Flexion Varus Osteotomy vs Brace in Late-onset Disease
- Historical-control study of late-onset disease (onset at 8 years or older): 33 brace-treated vs 21 flexion varus osteotomy hips
- Good radiographic outcome (Stulberg I-II) in 76% of the osteotomy group versus 36% of the brace group (odds ratio 5.6)
- 18% of brace-treated hips required subsequent femoral varus osteotomy for progressive collapse and hinge abduction
- All osteotomy patients required a second procedure for implant removal
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Presentation (Standard, 2-3 min)
"A 6-year-old boy presents with a 4-week history of painless limp. Parents noticed he limps after playing. Examination shows limited hip abduction and internal rotation. X-ray shows dense femoral head with crescent sign on frog-leg lateral. The lateral pillar appears to have 40% height loss compared to the normal side. What is your assessment and management?"
Scenario 2: Surgical Decision-Making (Challenging, 3-4 min)
"A 7.5-year-old girl presents with 2 months of hip pain and limp. X-ray shows fragmentation of the femoral head with more than 50% lateral pillar collapse (Herring C). Extrusion index is 30%. She has 25 degrees of abduction and limited internal rotation. Parents ask if surgery will help. What is your assessment and what do you tell the family?"
Scenario 3: Late Presentation and Differential Diagnosis (Critical, 2-3 min)
"A 5-year-old boy presents with 6 weeks of hip pain and refusal to bear weight. He has been treated for 'irritable hip' twice in the past 3 months with temporary improvement. Examination shows limited ROM in all planes. ESR and CRP are mildly elevated (ESR 25, CRP 15). Temperature is normal. X-ray shows subtle increased density of the femoral head. What is your differential and management?"
MCQ Practice Points
Natural History Question
Q: What is the typical duration of Legg-Calvé-Perthes disease from onset to complete healing? A: 2-4 years. The disease progresses through four stages (necrosis, fragmentation, reossification, remodeling) over this timeframe, regardless of treatment. Treatment does not shorten the disease course but aims to optimize the final head shape.
Classification Question
Q: At what stage should the Herring lateral pillar classification be applied? A: At maximal fragmentation stage (stage II). This is when the lateral pillar height loss is most evident and classification is most reliable. Classifying too early (necrosis stage) or too late (reossification stage) reduces accuracy.
Prognosis Question
Q: What is the single most important prognostic factor in Legg-Calvé-Perthes disease? A: Age at onset. Children under 6 have excellent prognosis regardless of classification. Children over 8 have poor prognosis even with treatment. Age is more important than classification, extent of involvement, or treatment type.
Treatment Question
Q: A 7-year-old boy with Perthes disease has Herring C classification. Intraoperatively, you notice that when you abduct the hip, the femoral head impinges on the lateral acetabulum causing pain. What is this called and what should you do? A: This is hinge abduction, where the aspherical head impinges on the lateral acetabulum. It is a contraindication to varus osteotomy (which would worsen impingement). Instead, consider valgus osteotomy to redirect the head away from the impinging position and reduce pain.
Anatomy Question
Q: Why is the pediatric femoral head particularly vulnerable to avascular necrosis? A: The lateral epiphyseal vessels (from medial femoral circumflex artery) are the only significant blood supply to the femoral head in children under 7-8 years. Unlike adults, there is no metaphyseal contribution across the growth plate, and the foveal vessels (ligamentum teres) are minimal. This single vascular supply makes the head vulnerable if these vessels are interrupted.
Imaging Question
Q: What is the crescent sign in Perthes disease? A: A subchondral lucency on frog-leg lateral radiograph representing a fracture through the necrotic subchondral bone. It appears early in the disease (transition from necrosis to fragmentation stage) and indicates significant epiphyseal involvement. It is a key feature of the Salter-Thompson classification.
Guidelines, Registries & Global Practice
Perthes disease has no single international clinical-practice guideline; management is guided by the prospective cohort evidence above and by paediatric-orthopaedic registries. The picture below is deliberately global rather than tied to any one health system.
Global epidemiology (population-based):
Reported Incidence and Demographics by Population
| Source population | Reported incidence (per 100,000 0-14 yrs) | Key finding |
|---|---|---|
| Sweden, born 1973-1993 (Johansson 2016) | 9.3 | Boy:girl ratio 3.1:1; higher with lower parental socioeconomic status and Nordic lineage |
| UK, 1990-2008 (Perry 2012) | 12.2 falling to 5.7 over the period | Strong North-South gradient; incidence tracks childhood deprivation, suggesting an environmental determinant |
| Merseyside UK register, 1976-2009 (Perry 2011) | 14.2 falling to 7.7 in Liverpool | Most deprived quintile had over 3 times the incidence of the most affluent (11.5 vs 3.8) |
Reported incidence therefore varies several-fold worldwide (single figures to mid-teens per 100,000), with a consistent male predominance (roughly 3-5:1) and a robust association with socioeconomic deprivation. A Swedish national-register study also found increased rates of obesity, hypertension and other osteochondroses in affected children, supporting a possible systemic component (Hailer 2018, DOI).
Where management genuinely differs (and where it agrees):
Practice Positions and Their Evidence
| Question | Predominant position | Evidence base / level |
|---|---|---|
| Under 8 yrs (or skeletal age 6 or less) | Symptomatic / non-operative care, maintain range of motion | Herring IPSG: no treatment benefit in this group (Level 2) |
| Over 8 yrs, lateral pillar B or B/C border | Containment osteotomy favoured over non-operative care | Herring IPSG Part II: surgery significantly better (Level 2) |
| Over 6 yrs with more than 50% head necrosis | Proximal femoral varus osteotomy preferred; abduction bracing not supported | Wiig Norwegian national study (Level 2) |
| Abduction orthosis / bracing | Largely abandoned as a containment method | Herring IPSG and Wiig: no benefit over physiotherapy (Level 2) |
| Lateral pillar C (any age) and non-containable hips | Poor prognosis; symptom-directed and salvage (valgus osteotomy for hinge abduction) | Yoo, Nakamura (Level 3-4) |
Registry evidence: Several national paediatric-orthopaedic registries now capture Perthes prospectively, notably the Swedish Paediatric Orthopaedic Quality register (SPOQ) Perthes' register, which has been used to study comorbidity and outcome (Morlin 2021, DOI). Unlike arthroplasty, there is no implant-survival registry relevant here; registries instead inform incidence, risk factors and natural history rather than device performance.
Global practice variation: In high-resource settings the debate centres on which containment operation (femoral versus pelvic versus combined) and patient selection, supported by MRI/arthrography. In lower-resource settings, late presentation is more common, MRI access is limited, and management leans on plain radiographs with a higher proportion of salvage rather than early containment. Long-term surveillance to skeletal maturity, with transition to adult services for femoroacetabular impingement and early-osteoarthritis monitoring, is recommended everywhere.
Exam Context
For any orthopaedic board, be ready to discuss:
- Age-based treatment algorithm (observe under 8; containment for over-8 lateral pillar B/B-C border; salvage for group C)
- The two landmark cohorts - Herring IPSG and Wiig - and exactly what each showed about who benefits from surgery
- Why bracing was abandoned as a containment strategy
- Containment principle and the choice between femoral varus, Salter and combined osteotomy
- Hinge abduction as a contraindication to varus (use valgus instead)
- Differential diagnosis, especially septic arthritis versus early Perthes
LEGG-CALVÉ-PERTHES DISEASE
Clinical summary
THE ESSENTIALS
- •Idiopathic AVN of femoral head, age 4-8 years
- •Self-limiting 2-4 years, goal = spherical head at maturity
- •Age at onset is most important prognostic factor
- •Containment principle: maintain head in acetabulum during reossification
HERRING CLASSIFICATION
- •Applied at maximal fragmentation stage
- •A = no lateral pillar collapse (excellent)
- •B = less than 50% collapse (good if under 8)
- •B/C = exactly 50% (borderline, treat as high risk)
- •C = more than 50% collapse (poor)
TREATMENT BY AGE
- •Under 6: observation all groups (excellent remodeling)
- •6-8 years: Herring A/B observe; B/C or C = containment surgery
- •Over 8: Herring B consider surgery; C = salvage/palliation
- •Containment options: femoral varus, Salter, shelf procedure
SURGICAL PEARLS
- •Varus osteotomy: 10-15 degrees, causes shortening
- •Salter: rotates acetabulum, no shortening, needs graft
- •Assess hinge abduction before varus (contraindication)
- •Intraoperative arthrogram confirms containment achievable
POOR PROGNOSTIC FEATURES (LATE)
- •L = Lateral pillar collapse (Herring C)
- •A = Age over 8 years (most important)
- •T = Total head involvement (Catterall IV)
- •E = Extrusion (more than 20%)
KEY EVIDENCE AND OUTCOMES
- •Stulberg I-II = good long-term (no early OA)
- •Stulberg IV-V = early OA by age 40-50, need THA
- •Herring study: age most important factor
- •Wiig RCT: containment benefit uncertain for all patients