Malignant Smooth-Muscle Sarcoma | Spindle Cells with Blunt-Ended Nuclei | Grade and Size Drive Outcome
- Leiomyosarcoma is a malignant tumour of smooth muscle and is one of the commonest adult soft tissue sarcomas
- Histology shows intersecting fascicles of spindle cells with blunt-ended (cigar-shaped) nuclei and eosinophilic cytoplasm
- Immunohistochemistry is positive for smooth-muscle markers - desmin, smooth muscle actin (SMA) and h-caldesmon
- Tumour grade (FNCLCC) and size are the dominant independent predictors of survival and distant recurrence
- Wide local excision is the curative treatment; chemotherapy is reserved for advanced or selected high-risk disease, not routine adjuvant use
- “Soft tissue leiomyosarcoma is biologically different from GIST - it is NOT KIT/CD117 driven and does not respond to imatinib
- “Retroperitoneal location carries a worse prognosis than extremity disease, largely because of size and margin difficulty
- “Lung is the dominant site of distant metastasis for extremity tumours; liver is important for retroperitoneal and vascular tumours
- “Adjuvant chemotherapy did NOT improve survival in the EORTC 62931 randomised trial of resected soft tissue sarcoma
Leiomyosarcoma is a malignant smooth-muscle tumour. Diagnosis rests on spindle cells with blunt-ended nuclei plus a smooth-muscle immunoprofile (desmin, SMA, h-caldesmon positive). It is NOT a GIST and does not respond to imatinib.
FNCLCC grade and tumour size are the dominant independent predictors of survival and distant recurrence. Site (retroperitoneal versus extremity) matters mostly because retroperitoneal tumours are large and hard to resect with clear margins.
Wide local excision with negative margins is the only reliable curative treatment. Radiotherapy improves local control for deep or larger extremity tumours. Chemotherapy is not routine adjuvant therapy.
Image-guided core needle biopsy, planned with the definitive surgeon, comes before any excision. Never shell out (marginal excise) an undiagnosed deep soft tissue mass - it compromises later limb-salvage surgery.
SMOOTHLeiomyosarcoma Core Features
Hook:SMOOTH muscle gone bad - SMOOTH captures origin, markers, demographics, prognosis, sites and spread.
BEEFHistology Clues for Leiomyosarcoma
Hook:Think BEEF - smooth muscle is meat: blunt nuclei, eosinophilic cytoplasm, intersecting fascicles, fibrillary cytoplasm.
GRIMSAdverse Prognostic Factors
Hook:A GRIMS picture means a worse outcome - Grade, Retroperitoneal, Incomplete margins, Measurement large, Spread.
Overview and Epidemiology

Leiomyosarcoma is a malignant tumour that shows differentiation toward smooth muscle. It is one of the more common adult soft tissue sarcomas. In soft tissue, it arises wherever smooth muscle exists - in the walls of blood vessels, in the dermal arrector pili muscles, and from poorly differentiated mesenchymal cells. The three clinically important groups are somatic soft tissue tumours of the extremity and trunk, retroperitoneal and abdominal tumours, and tumours of large vessels such as the inferior vena cava.
Do not confuse soft tissue leiomyosarcoma with gastrointestinal stromal tumour (GIST). Historically many gut "leiomyosarcomas" were reclassified as GISTs once KIT/CD117 and DOG1 testing became available. True leiomyosarcoma is KIT-negative, is driven by smooth-muscle biology rather than KIT/PDGFRA mutations, and does not respond to imatinib. Modern leiomyosarcoma series deliberately exclude GISTs.
- Age: Most patients are middle-aged to older adults (typically 50-70 years)
- Gender: Slight overall female predominance (strong in uterine disease)
- Share of sarcomas: Roughly 10-20% of adult soft tissue sarcomas
- Young patients: Uncommon but possible; consider in any persistent deep mass
- Extremity / trunk: Common somatic soft tissue site, often deep
- Retroperitoneum / abdomen: Frequent and prognostically poor (large, hard margins)
- Vascular (IVC and other vessels): Distinct group arising from the vessel wall
- Cutaneous / subcutaneous: Smaller, better prognosis when superficial
Outcome by Site (MSKCC Primary Leiomyosarcoma Series)
- Approximate Share
- About half of primary cases
- Recurrence Pattern
- Distant recurrence around one third
- Prognostic Note
- Best access to wide margins; favourable group
- Approximate Share
- About 40%
- Recurrence Pattern
- Recurrence around half; late recurrence after 5 years
- Prognostic Note
- Worse disease-specific survival, driven by size and margins
- Approximate Share
- About 1 in 10
- Recurrence Pattern
- Recurrence around one quarter
- Prognostic Note
- Intermediate behaviour
The "vascular" group is a distinct, examinable entity: leiomyosarcoma is the commonest primary malignant tumour of the inferior vena cava (IVC), arising from the vessel-wall smooth muscle, with a marked female predominance. It is classified by the level of caval involvement, which dictates presentation and reconstruction:
- Level I (lower / infrarenal): below the renal veins. Often presents with leg swelling; the abundant collaterals that develop may allow ligation without reconstruction.
- Level II (middle / renal-to-hepatic): between the renal and hepatic veins - the commonest level. Renal vein involvement matters; reconstruction (graft) is often needed to preserve renal outflow.
- Level III (upper / suprahepatic): at/above the hepatic veins, up to the right atrium - presents with Budd-Chiari syndrome (hepatic venous outflow obstruction); technically the hardest, may need cardiopulmonary bypass.
Management is en bloc resection of the involved caval segment with reconstruction (ring-reinforced PTFE/graft) or ligation depending on level and collateral development; prognosis is worse than extremity disease and the liver and lung are the metastatic sites.
Exam point: leiomyosarcoma is the commonest primary IVC tumour (female predominance) - classify by level (I infrarenal / II renal-hepatic / III suprahepatic = Budd-Chiari), and resect en bloc with graft reconstruction or ligation guided by level and collaterals.
Pathophysiology and Molecular Biology
Cellular Origin and Genetics
Leiomyosarcoma differentiates toward smooth muscle. Unlike synovial sarcoma or Ewing sarcoma, it has no single recurrent translocation. Instead it shows a complex karyotype with widespread chromosomal gains and losses and frequent inactivation of tumour-suppressor pathways. This genomic complexity is typical of the "non-translocation" pleomorphic sarcomas and explains why no targeted driver therapy (such as imatinib for GIST) exists.
Complex, unstable genome:
- No pathognomonic fusion gene (contrast synovial sarcoma)
- Frequent loss of tumour-suppressor function (e.g. RB1 and TP53 pathways)
- Numerous copy-number changes and chromosomal rearrangements
- Heterogeneous biology between uterine and non-uterine tumours
Smooth-muscle markers establish the line of differentiation:
- Desmin: Commonly positive
- Smooth muscle actin (SMA): Commonly positive
- h-caldesmon: More specific smooth-muscle marker
- May show focal keratin or EMA - a recognised diagnostic trap
There is no single confirmatory molecular test for leiomyosarcoma. Diagnosis combines characteristic histology (intersecting fascicles, blunt-ended nuclei, eosinophilic cytoplasm) with a smooth-muscle immunoprofile (desmin, SMA, h-caldesmon). Always exclude GIST (KIT/DOG1) for visceral lesions and exclude dedifferentiated liposarcoma with smooth-muscle areas in the retroperitoneum.
Tumour Biology and Behaviour
- Description
- Enlarging deep mass, often painless until large
- Clinical Implication
- Diagnostic delay common; any deep mass over 5cm needs urgent imaging
- Description
- Infiltrative; pushes and invades along fascial planes
- Clinical Implication
- Wide margins essential to control local recurrence
- Description
- Predominantly haematogenous, lymph-node spread uncommon
- Clinical Implication
- Stage the lungs (and liver for retroperitoneal/vascular tumours)
- Description
- Recurrence can occur beyond 5 years, especially retroperitoneal
- Clinical Implication
- Long-term surveillance is mandatory
Classification and Grading
Histological Diagnosis
Classic Histology
Leiomyosarcoma is built from intersecting fascicles of spindle cells that cross at roughly right angles.
- Blunt-ended (cigar-shaped) nuclei - the classic clue
- Brightly eosinophilic, fibrillary cytoplasm
- Perinuclear vacuoles may be seen
- Mitoses present; atypia varies with grade
- Long sweeping fascicles intersecting at 90 degrees
- Higher-grade tumours show pleomorphism and necrosis
- Pleomorphic / dedifferentiated areas in high-grade tumours
- Coagulative tumour necrosis contributes to grade
The combination of blunt-ended nuclei and eosinophilic cytoplasm in intersecting fascicles is the textbook appearance.
FNCLCC Histological Grading
Grade is the single most important histopathological prognostic factor in soft tissue sarcoma. The FNCLCC (French Federation of Cancer Centres) system assigns a grade from a score built on three components.
- What Is Scored
- How closely the tumour resembles normal adult mesenchymal tissue
- Score Range
- 1 to 3
- What Is Scored
- Mitoses per 10 high-power fields
- Score Range
- 1 to 3
- What Is Scored
- Extent of coagulative necrosis
- Score Range
- 0 to 2
- What Is Scored
- Sum of the three scores maps to grade
- Score Range
- Grade 1, 2 or 3
The total FNCLCC score (differentiation plus mitotic count plus necrosis) maps to grade 1, 2 or 3. High grade (grade 3) is independently associated with distant recurrence and death. In leiomyosarcoma specifically, grade and size are the dominant predictors of disease-specific survival.
AJCC Staging (Soft Tissue Sarcoma)
- Grade
- Low (G1)
- Size / Spread
- 5cm or less
- General Outlook
- Favourable
- Grade
- Low (G1)
- Size / Spread
- Greater than 5cm
- General Outlook
- Favourable
- Grade
- High (G2-3)
- Size / Spread
- 5cm or less
- General Outlook
- Intermediate
- Grade
- High (G2-3)
- Size / Spread
- Greater than 5cm (size bands)
- General Outlook
- Higher risk of distant relapse
- Grade
- Any
- Size / Spread
- Nodal or distant metastasis
- General Outlook
- Poor
Retroperitoneal sarcomas use a separate AJCC size-banded staging scheme. Most clinically significant leiomyosarcomas are intermediate to high grade.
Clinical Presentation
History
- Extremity/trunk: Enlarging, often painless deep mass
- Retroperitoneal: Vague abdominal fullness, pain, mass effect
- Vascular (IVC): Leg swelling, Budd-Chiari features, abdominal pain
- Cutaneous: Small firm dermal/subcutaneous nodule
- Size greater than 5cm
- Deep to fascia
- Increasing in size
- New pain in a previously painless lump
Any soft tissue mass that is larger than 5cm, deep to fascia, or enlarging should be regarded as a sarcoma until proven otherwise and referred to a specialist sarcoma service. Reassuring slow growth does not exclude leiomyosarcoma.
Examination Approach
Clinical Assessment
- Mass size and relation to surface anatomy
- Skin changes (uncommon unless cutaneous or fungating)
- Limb swelling or venous engorgement (vascular tumours)
- Firm, often fixed deep mass
- Relation to neurovascular bundle
- Tenderness if large or nerve-involving
- Joint range of motion if periarticular
- Distal neurovascular status
- Muscle power in the affected compartment
- Regional nodes (metastasis uncommon but recorded)
- Respiratory assessment (lung is the dominant metastatic site)
A complete baseline supports later treatment planning.
Investigations and Imaging
Imaging Protocol
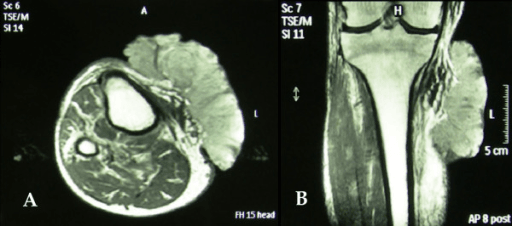
MRI (Gold Standard for Local Staging)
MRI of the whole anatomical region defines the tumour and its relations.
Protocol and findings:
- T1-weighted: anatomy and tumour extent
- T2-weighted with fat suppression: heterogeneous high signal
- Post-contrast T1 with fat suppression: heterogeneous enhancement, may show necrosis
- Define relation to neurovascular bundle, bone and compartment boundaries
MRI is essential before biopsy and surgery to plan margins and the biopsy tract.
Biopsy
Core principles for any suspected soft tissue sarcoma:
- Image-guided core needle biopsy is the standard
- Plan the biopsy tract with the definitive surgeon so it can be excised en bloc
- Refer to a sarcoma centre before biopsy wherever possible
- Never perform an unplanned marginal ("shell-out") excision of an undiagnosed deep mass - it seeds tumour and jeopardises limb salvage
- Send tissue for full immunohistochemistry (desmin, SMA, h-caldesmon, plus KIT/DOG1 and MDM2/CDK4 where relevant)
Management
Core Principles
Wide local excision with negative margins is the only reliable curative treatment for localised leiomyosarcoma. Radiotherapy improves local control for deep or larger extremity tumours. Unlike synovial sarcoma, chemotherapy is not standard adjuvant therapy and is reserved for advanced or selected high-risk disease decided at a multidisciplinary meeting.
Treatment fundamentals:
- Surgery: wide excision with a cuff of normal tissue, biopsy tract excised en bloc
- Radiotherapy: pre- or post-operative for deep/larger extremity tumours or close margins
- Systemic therapy: doxorubicin-based regimens for advanced disease; not routine adjuvant
These principles apply across leiomyosarcoma sites, modified by anatomy.
Systemic Agents in Advanced Leiomyosarcoma
- Agent(s)
- Doxorubicin (anthracycline) based
- Evidence Summary
- Standard backbone for metastatic soft tissue sarcoma
- Agent(s)
- Trabectedin
- Evidence Summary
- Phase III: improved progression-free survival versus dacarbazine in leiomyosarcoma/liposarcoma
- Agent(s)
- Eribulin
- Evidence Summary
- Phase III: improved overall survival versus dacarbazine in this pooled leiomyosarcoma/liposarcoma population
- Agent(s)
- Adjuvant doxorubicin/ifosfamide
- Evidence Summary
- EORTC 62931: no relapse-free or overall survival benefit - not routine
Surgical Technique
Preoperative Planning
Preparation Steps
- Review MRI/CT with radiology and the sarcoma MDT
- Define tumour extent and neurovascular relations
- Confirm diagnosis and grade on core biopsy
- Plan resection margins and reconstruction
- Mark the biopsy tract for en bloc excision
- Plan a longitudinal, extensile incision
- Treat drain sites as contaminated
- Anticipate the soft tissue defect
- Arrange flap or graft coverage if needed
- Plan vascular reconstruction for vessel-based tumours
Good planning underpins both oncological clearance and function.
Complications
Disease and Treatment Complications
- Driver
- Positive margins, high grade, large size
- Management
- Re-resection where feasible; radiotherapy
- Driver
- High grade, large size (lung dominant; liver for retroperitoneal/vascular)
- Management
- Systemic therapy; metastasectomy for resectable oligometastatic lung disease
- Driver
- Pre-operative radiotherapy, poor soft tissue coverage
- Management
- Wound care, negative-pressure therapy, flap coverage
- Driver
- Tumour proximity or deliberate sacrifice
- Management
- Reconstruction, physiotherapy, orthotics
- Driver
- Anthracycline (cardiotoxicity), ifosfamide
- Management
- Cumulative-dose limits, cardiac monitoring, supportive care
Prognosis and Outcomes
Prognostic Factors
- Favourable
- Low grade (G1)
- Unfavourable
- High grade (G3)
- Favourable
- 5cm or less
- Unfavourable
- Greater than 5cm
- Favourable
- Extremity / superficial
- Unfavourable
- Retroperitoneal / deep
- Favourable
- Negative
- Unfavourable
- Positive
- Favourable
- Localised
- Unfavourable
- Metastatic at presentation
In primary leiomyosarcoma, multivariate analysis shows that grade and size are the dominant independent predictors of disease-specific survival and distant recurrence, while margin status drives local recurrence. Although retroperitoneal tumours do worse than extremity tumours, much of that difference is explained by their larger size and the difficulty of obtaining clear margins.
Superficial leiomyosarcoma is not one entity - the depth relative to the dermis splits it into two prognostically very different tumours, a classic examiner discriminator:
- Cutaneous (dermal) leiomyosarcoma: arises from the arrector pili (pilar) smooth muscle in the dermis. It is essentially non-metastasising - the concern is local recurrence only - so it has an excellent prognosis and wide local excision is curative; intensive systemic staging/surveillance is largely unnecessary.
- Subcutaneous leiomyosarcoma: arises from vessel-wall smooth muscle in the subcutis. It behaves like a deep soft tissue sarcoma and DOES metastasise (lung), so it needs wide margins plus staging and long-term surveillance like other deep tumours.
- The teaching point: the dermis is the dividing line - a tumour confined to the dermis is benignly-behaving for metastasis, whereas one that involves or sits beneath the subcutis carries true metastatic risk. This dichotomy drives the extent of staging, follow-up and counselling.
Exam point: dermal (cutaneous) leiomyosarcoma essentially does not metastasise (wide excision cures, recurrence is local), whereas subcutaneous leiomyosarcoma metastasises and must be staged and followed like a deep soft tissue sarcoma - depth relative to the dermis is the key prognostic divider.
Surveillance
Follow-up Strategy
Surveillance Schedule
- Clinical review every 3-4 months
- Chest CT for lung metastases
- Local MRI for high-grade or marginal-resection tumours
- Clinical review every 6 months
- Periodic chest imaging
- Local imaging guided by symptoms and risk
- Annual review
- Continue chest (and abdominal for retroperitoneal/vascular) imaging
- Late recurrence is recognised, especially in retroperitoneal disease
Leiomyosarcoma can recur late - distant or local recurrence beyond 5 years is well described, particularly for abdominal and retroperitoneal tumours. A written long-term surveillance plan is essential.
Guidelines, Registries & Global Practice
Global Epidemiology
- Share of sarcomas: Roughly 10-20% of adult soft tissue sarcomas worldwide
- Age: Predominantly middle-aged and older adults (typically 50-70 years)
- Sex: Slight overall female predominance, strongest in uterine disease
- Reclassification effect: True leiomyosarcoma figures rose in clarity once GISTs were separated out
- Drivers: Grade and size dominate survival; margins drive local recurrence
- Site: Retroperitoneal disease does worse than extremity disease
- Spread: Haematogenous (lung dominant; liver for retroperitoneal/vascular); nodes rare
- Late recurrence: Recognised beyond 5 years, especially retroperitoneal
Side-by-Side Guidance from Major Societies
- Diagnosis
- Refer to sarcoma centre before biopsy; core biopsy with immunohistochemistry
- Local Treatment
- Wide excision plus radiotherapy for deep/larger extremity tumours
- Systemic Therapy
- Anthracycline-based for advanced disease; adjuvant individualised, not routine
- Diagnosis
- Image-guided core biopsy at a sarcoma centre; multidisciplinary review
- Local Treatment
- Limb-sparing wide excision with radiotherapy; re-excision for positive margins
- Systemic Therapy
- Doxorubicin first line; trabectedin and eribulin in later lines
- Diagnosis
- Mandatory specialist sarcoma MDT before definitive treatment
- Local Treatment
- Centralised surgery and radiotherapy at designated centres
- Systemic Therapy
- Chemotherapy reserved for selected high-risk or advanced cases
- Diagnosis
- Multidisciplinary diagnosis; exclude dedifferentiated liposarcoma
- Local Treatment
- En bloc resection of involved organs at high-volume centres
- Systemic Therapy
- Radiotherapy and chemotherapy individualised
Every major society agrees on three points regardless of region: any suspicious deep or enlarging soft tissue mass should be referred to a specialist sarcoma centre before biopsy, diagnosis should be made by planned core biopsy with immunohistochemistry, and definitive management should be set by a multidisciplinary sarcoma team. The main areas of disagreement are the thresholds for radiotherapy and for any systemic therapy.
High- vs Limited-Resource Practice Variation
- Routine immunohistochemistry (desmin, SMA, h-caldesmon) and exclusion of GIST/dedifferentiated liposarcoma
- Centralised sarcoma MDTs, limb salvage with reconstruction, and specialist radiotherapy
- Access to MRI staging, PET-CT and histology-specific agents (trabectedin, eribulin)
- Pulmonary metastasectomy programmes for selected oligometastatic disease
- Diagnosis may rest on morphology and a limited immunohistochemistry panel
- Later presentation with larger tumours; higher amputation rates
- Restricted radiotherapy and systemic-therapy access
- Telepathology and regional referral networks help bridge expertise gaps
Applicable in any health system:
- Document the investigation pathway for any persistent or deep soft tissue mass (mitigates delayed diagnosis)
- Confirm pre-biopsy staging and that the biopsy was planned with the definitive surgeon
- Record exclusion of GIST and, in the retroperitoneum, of dedifferentiated liposarcoma
- Evidence of sarcoma MDT discussion before definitive treatment
- Informed consent covering recurrence and metastatic risk, possible organ or limb sacrifice
- A written long-term surveillance plan, given recognised late recurrence
Controversies and Areas of Uncertainty
The benefit of adjuvant chemotherapy in resected soft tissue sarcoma remains unproven. The EORTC 62931 randomised trial of doxorubicin plus ifosfamide showed no relapse-free or overall survival benefit, so chemotherapy is not routine and is reserved for selected high-risk cases at MDT discretion.
Trabectedin and eribulin have specific activity in leiomyosarcoma and liposarcoma, supporting a move toward histology-specific second-line therapy rather than one-size-fits-all chemotherapy. The optimal sequencing of agents is still debated.
Radiotherapy is well established for deep extremity sarcoma but its role in the retroperitoneum is contested, with trial data showing limited benefit. Use is selective and individualised.
Resection of resectable, oligometastatic lung disease is widely practised and associated with longer survival in selected patients, but no randomised trial confirms a survival benefit. Patient selection is decisive.
MCQ Practice Points
Q: Which immunohistochemical profile confirms leiomyosarcoma? A: Positive for smooth-muscle markers - desmin, smooth muscle actin (SMA) and h-caldesmon - with characteristic spindle cells showing blunt-ended (cigar-shaped) nuclei. KIT/CD117 is negative, which helps exclude GIST.
Q: What are the dominant independent predictors of survival in primary soft tissue leiomyosarcoma? A: FNCLCC grade and tumour size. Margin status is the key driver of local recurrence. Retroperitoneal site is associated with worse outcome largely because of larger size and margin difficulty.
Q: Is adjuvant chemotherapy standard after resection of localised leiomyosarcoma? A: No. The EORTC 62931 randomised trial of doxorubicin plus ifosfamide showed no relapse-free or overall survival benefit. Chemotherapy is reserved for advanced disease or individualised high-risk cases.
Q: How does soft tissue leiomyosarcoma differ from GIST? A: Leiomyosarcoma is a true smooth-muscle tumour that is KIT-negative and does NOT respond to imatinib. GIST is KIT/DOG1 positive and is treated with imatinib. Many old gut "leiomyosarcomas" were reclassified as GISTs.
Q: What are the dominant metastatic sites in leiomyosarcoma? A: Lung for extremity tumours; liver is also important for retroperitoneal and vascular tumours. Spread is predominantly haematogenous and lymph-node metastasis is uncommon.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man has a 7cm deep, firm, painless mass in the posterior thigh that has been slowly enlarging over six months. How would you investigate and manage him?”
“A 58-year-old woman has a 14cm retroperitoneal mass on CT. Core biopsy reports a high-grade spindle-cell tumour. How do you confirm the diagnosis and plan treatment, and how does this differ from an extremity tumour?”
“A 55-year-old man treated two years ago for a high-grade extremity leiomyosarcoma now has three FDG-avid nodules confined to the right lung on surveillance CT. How do you proceed, and what systemic options exist if surgery is not appropriate?”
Key Epidemiology
- Malignant smooth-muscle sarcoma; roughly 10-20% of adult soft tissue sarcomas
- Typical age 50-70 years, slight overall female predominance
- Three groups: extremity/trunk, retroperitoneal/abdominal, and vascular (e.g. IVC)
- Distinct from GIST - true leiomyosarcoma is KIT-negative
Diagnosis (Morphology plus IHC)
- Intersecting fascicles of spindle cells with blunt-ended (cigar-shaped) nuclei
- Brightly eosinophilic, fibrillary cytoplasm
- Positive: desmin, smooth muscle actin (SMA), h-caldesmon
- Negative KIT/DOG1 excludes GIST; check MDM2/CDK4 in retroperitoneum to exclude dedifferentiated liposarcoma
Grading and Staging
- FNCLCC grade = differentiation + mitotic count + necrosis, mapped to grade 1-3
- Grade is the most important histopathological prognostic factor
- AJCC staging by grade, size and metastasis (separate scheme for retroperitoneum)
- Most clinically significant tumours are intermediate to high grade
Investigation and Biopsy
- MRI is the gold standard for local staging of the mass
- CT chest for lung metastases; CT abdomen/pelvis (and liver) for retroperitoneal/vascular tumours
- Image-guided core biopsy with tract planned by the definitive surgeon
- Never shell out an undiagnosed deep mass - refer to a sarcoma centre first
Treatment
- Wide local excision with negative margins is the curative backbone
- Radiotherapy improves local control for deep or larger extremity tumours
- Adjuvant chemotherapy is NOT routine - EORTC 62931 showed no survival benefit
- Advanced disease: doxorubicin first line, then trabectedin and eribulin
- Metastasectomy for selected resectable oligometastatic lung disease
Adverse Prognostic Factors (GRIMS)
- Grade high (FNCLCC 3)
- Retroperitoneal / deep site
- Incomplete (positive) margins
- Measurement large (size over 5cm)
- Spread (metastatic at presentation)
Prognosis and Surveillance
- Grade and size are the dominant independent predictors of survival
- Margin status drives local recurrence
- Spread is haematogenous (lung; liver for retroperitoneal/vascular); nodes rare
- Late recurrence beyond 5 years is recognised - long-term surveillance is mandatory
Evidence Base and Key Studies
Predictors of Survival and Recurrence in Primary Leiomyosarcoma
- 353 patients with primary resectable leiomyosarcoma (GISTs excluded) from a prospective database, 1982-2006
- Distribution: 48% extremity, 41% abdominal/retroperitoneal, 11% truncal; 75% high grade, median size 6.0cm
- On multivariate analysis only high grade and size were independent predictors of disease-specific survival
- Late recurrence beyond 5 years occurred in 9% of abdominal/retroperitoneal and 4% of extremity tumours
Prognostic Factors in 1,041 Localised Extremity Soft Tissue Sarcomas
- 1,041 adults with localised extremity soft tissue sarcoma treated at a single institution, prospective data
- 5-year survival 76%; high grade, large size and deep location were adverse for disease-specific survival
- Leiomyosarcoma histology was an independent adverse factor for both distant recurrence and disease-specific survival
- Microscopically positive margins independently predicted local recurrence and tumour-related death
Histological Grading of Soft Tissue Sarcomas (FNCLCC and MIB-1)
- Reviews histological grading as the most important histopathological prognostic factor in soft tissue sarcoma
- Describes the FNCLCC system based on differentiation, mitotic count and tumour necrosis
- Discusses the MIB-1 (Ki-67) proliferation index as an adjunct to grading
- Highlights pitfalls in grade assessment and its relationship to other clinicopathological factors