Hammer Toe | Claw Toe | Mallet Toe | Flexor-Extensor Imbalance
Classification by Joint Involvement
Critical Must-Knows
- Flexible vs rigid deformities determine surgical approach - flexible responds to soft tissue, rigid needs bony correction
- Hammer toe affects PIPJ primarily; claw toe involves all three joints with MTPJ hyperextension
- Mallet toe is isolated DIPJ flexion (often traumatic FDL rupture or footwear-related)
- Flexor to extensor transfer (Girdlestone-Taylor) corrects dynamic claw deformity by rebalancing forces
- PIPJ fusion is gold standard for fixed hammer/claw toe - provides stable, pain-free toe in functional position
Clinical Pearls
- "Distinguish flexible (passively correctable) from rigid (fixed) deformities - dictates treatment
- "Claw toe commonly seen in cavus foot, CMT, or diabetes - always examine foot posture and neurology
- "MTPJ synovitis and plantar plate insufficiency cause crossover toe and require MTPJ-level intervention
- "Flexor to extensor transfer only works if MTPJ is passively reducible - otherwise add MTPJ capsule release
Critical Lesser Toe Deformity Exam Points
Deformity Classification
Master the joint involvement pattern. Hammer toe equals PIPJ flexion. Claw toe equals MTPJ hyperextension plus PIPJ and DIPJ flexion. Mallet toe equals isolated DIPJ flexion. Crossover toe equals MTPJ instability with deviation.
Flexible vs Rigid Assessment
Passive correction test is critical. Flexible deformities correct with passive dorsiflexion of the ankle or manipulation. Rigid deformities have fixed contractures requiring bony surgery. This dictates entire treatment algorithm.
Flexor to Extensor Transfer
Girdlestone-Taylor procedure mechanism. Transfer FDL to extensor hood to plantarflex MTPJ and extend IP joints. Only works if MTPJ passively reduces. Indicated for flexible claw toe in dynamic imbalance.
PIPJ Fusion Principles
Gold standard for fixed deformity. Fuse PIPJ in 15-25 degrees flexion for functional toe position. Remove cartilage, achieve bony apposition, fix with K-wire or screw. Avoid excessive shortening.
Quick Decision Guide - Lesser Toe Deformities
| Clinical Scenario | Deformity Type | Flexibility | Treatment |
|---|---|---|---|
| Second toe PIPJ flexion, passively correctable, painful corn over PIPJ | Hammer toe - flexible | Corrects with manipulation | Flexor tenotomy + extensor lengthening |
| Second toe PIPJ flexion, rigid, painful corn, shoe intolerance | Hammer toe - rigid | Fixed contracture | PIPJ resection arthroplasty or fusion |
| Multiple toes with MTPJ dorsiflexion + PIPJ/DIPJ flexion, cavus foot | Claw toe - flexible | Reduces with ankle dorsiflexion | Flexor to extensor transfer + address cavus |
| Claw toe with MTPJ fixed dorsiflexion, metatarsalgia, clawed posture | Claw toe - rigid | MTPJ and IP joints fixed | PIPJ fusion + MTPJ release or shortening osteotomy |
| Isolated DIPJ flexion, tip of toe painful, nail dystrophy | Mallet toe | Usually flexible early | FDL tenotomy or DIPJ fusion if rigid |
| Second toe crossing over hallux, painful MTPJ, plantar plate tear | Crossover toe | MTPJ instability | MTPJ capsule repair + flexor transfer or arthroplasty |
HCMLesser Toe Deformity Pattern Recognition
| H | Hammer toe PIPJ flexion deformity only (DIPJ neutral or extended) |
| C | Claw toe MTPJ hyperextension + PIPJ flexion + DIPJ flexion (all three joints) |
| M | Mallet toe DIPJ flexion only (PIPJ and MTPJ normal) |
| H | Hammer toe PIPJ flexion deformity only (DIPJ neutral or extended) |
| C | Claw toe MTPJ hyperextension + PIPJ flexion + DIPJ flexion (all three joints) |
| M | Mallet toe DIPJ flexion only (PIPJ and MTPJ normal) |
Hook:HCM - ascending complexity: Hammer affects one joint, Claw affects all three, Mallet is isolated to tip!
FREDFlexor to Extensor Transfer Indication
| F | Flexible deformity Must passively correct - rigid deformities need bony surgery |
| R | Reducible MTPJ MTPJ must reduce to neutral - otherwise transfer fails |
| E | Extensor imbalance Dynamic imbalance favoring extension over flexion |
| D | Dynamic claw toe Deformity worsens with ankle plantarflexion (positive Silverskiold) |
| F | Flexible deformity Must passively correct - rigid deformities need bony surgery | E | Extensor imbalance Dynamic imbalance favoring extension over flexion |
| R | Reducible MTPJ MTPJ must reduce to neutral - otherwise transfer fails | D | Dynamic claw toe Deformity worsens with ankle plantarflexion (positive Silverskiold) |
Hook:FRED the transfer - Flexible and Reducible are Essential for Dynamic correction!
CAPSPIPJ Fusion Technical Points
| C | Cartilage removal Complete cartilage removal from PIPJ - achieve raw bone surfaces |
| A | Alignment 15-25 degrees flexion - functional toe position |
| P | Pin or screw fixation Intramedullary K-wire 6-8 weeks or buried headless screw |
| S | Shortening avoidance Minimal bone resection - avoid floppy, short toe |
| C | Cartilage removal Complete cartilage removal from PIPJ - achieve raw bone surfaces | P | Pin or screw fixation Intramedullary K-wire 6-8 weeks or buried headless screw |
| A | Alignment 15-25 degrees flexion - functional toe position | S | Shortening avoidance Minimal bone resection - avoid floppy, short toe |
Hook:Put a CAP on the joint - arthrodese in proper position with solid fixation!
SLIPCrossover Toe Pathoanatomy
| S | Synovitis MTPJ synovitis - initiating pathology in most cases |
| L | Ligament failure Plantar plate and collateral ligaments stretch/tear |
| I | Instability MTPJ instability with dorsal subluxation/dislocation |
| P | Positional deviation Toe deviates medially (usually) crossing over adjacent toe |
| S | Synovitis MTPJ synovitis - initiating pathology in most cases | I | Instability MTPJ instability with dorsal subluxation/dislocation |
| L | Ligament failure Plantar plate and collateral ligaments stretch/tear | P | Positional deviation Toe deviates medially (usually) crossing over adjacent toe |
Hook:The toe SLIPS out of position - starts with synovitis, ends with deviation!
Overview and Epidemiology
Clinical Significance
Lesser toe deformities are common acquired foot problems causing pain, skin breakdown, and functional limitation. The spectrum ranges from flexible dynamic deformities (amenable to soft tissue procedures) to fixed rigid contractures (requiring bony surgery). Understanding the biomechanics and joint-specific involvement is critical for selecting appropriate surgical intervention and achieving durable correction.
Demographics and Risk Factors
- Gender: 80% female (footwear, ligament laxity)
- Age: Typically 30-60 years (progressive deformity)
- Footwear: High heels, narrow toe box, short shoes
- Heredity: Family history in 60-70% of cases
- Foot type: Cavus foot predisposes to claw toes
- Systemic: Rheumatoid arthritis, diabetes, neurological disease
Understanding the underlying cause guides treatment - address footwear, treat cavus deformity, manage inflammatory arthritis.
Pathophysiology Spectrum
- Intrinsic muscle weakness: Lumbricals/interossei fail, allowing long flexors to dominate
- Extrinsic muscle imbalance: EDL overpowers intrinsics, creating MTPJ hyperextension
- Chronic footwear pressure: Tight shoes force toes into flexed posture
- MTPJ synovitis: Inflammatory synovitis weakens plantar plate
- Progressive contracture: Capsular and tendinous contractures become fixed
The natural history is progression from flexible to rigid deformity - early intervention preserves joint motion.
Pathophysiology and Mechanisms
Critical Intrinsic Muscle Function
Lumbricals and interossei are key stabilizers. These intrinsic muscles insert into the extensor hood and produce MTPJ flexion with IP extension (opposite of extrinsic muscles). When intrinsics weaken (cavus foot, neuropathy, chronic overload), the long flexors (FDL, FDB) and extensors (EDL) dominate, creating the classic claw deformity pattern with MTPJ hyperextension and IP flexion.
Normal Toe Biomechanics
Extrinsic Muscles
Flexors:
- FDL: Flexes DIPJ primarily, PIPJ secondarily
- FDB: Flexes PIPJ, inserts on middle phalanx
- Both cross plantar to MTPJ - can hyperextend MTPJ if unopposed
Extensors:
- EDL: Extends all three joints, inserts into extensor hood
- Dominance causes MTPJ hyperextension, stretches plantar plate
Balance between flexors and extensors maintains neutral alignment.
Intrinsic Muscles
Lumbricals:
- Originate from FDL tendons
- Insert into extensor hood lateral band
- Flex MTPJ, extend PIPJ and DIPJ
Interossei (plantar and dorsal):
- Similar insertion to lumbricals
- Flex MTPJ, extend IP joints
- Provide mediolateral stability
Intrinsics prevent claw deformity - when they fail, extrinsics dominate and deformity develops.
Joint Deformity Patterns and Muscle Imbalance
| Deformity | MTPJ Position | PIPJ Position | DIPJ Position | Primary Imbalance |
|---|---|---|---|---|
| Normal | Neutral (0-10° extension) | Neutral (0-10° flexion) | Neutral | Balanced intrinsic/extrinsic |
| Hammer Toe | Normal or slight hyperextension | Flexed 30-90° | Neutral or extended | FDB/FDL dominance over intrinsics |
| Claw Toe | Hyperextended 30-60° | Flexed 45-90° | Flexed 30-60° | EDL + FDL dominate, intrinsics absent |
| Mallet Toe | Normal | Normal | Flexed 30-90° | FDL tightness or rupture |
Classification Systems
Classification by Joint Involvement
| Type | MTPJ | PIPJ | DIPJ | Clinical Features |
|---|---|---|---|---|
| Hammer Toe | Normal/mild hyperextension | Flexed (main deformity) | Neutral or extended | Dorsal PIPJ corn, tip may contact ground |
| Claw Toe | Hyperextended | Flexed | Flexed | Dorsal corns at PIPJ, metatarsalgia, elevated toes |
| Mallet Toe | Normal | Normal | Flexed | Tip corn, nail dystrophy, often traumatic |
| Crossover Toe | Dorsal subluxation | Variable flexion | Variable | Medial deviation, overlaps adjacent toe |
Key Distinction for Examiners
Hammer toe versus claw toe: Hammer toe has MTPJ relatively neutral with isolated PIPJ flexion. Claw toe has MTPJ hyperextension (key differentiator) plus flexion at both IP joints. Claw toes often bilateral and associated with cavus foot or neuromuscular disease. Examiners will show images or clinical photos - identify MTPJ position first.
Clinical Assessment
History
- Pain location: Dorsal corn over PIPJ, tip pain, metatarsalgia
- Footwear: Tight shoes, high heels, chronic pressure
- Progression: Acute versus chronic, flexible versus rigid
- Functional impact: Walking limitation, shoe intolerance
- Associated symptoms: Numbness (neuropathy), systemic arthritis
- Medical history: Diabetes, rheumatoid arthritis, Charcot-Marie-Tooth
History reveals the underlying etiology and progression pattern - guides treatment selection.
Examination
- Inspect standing: Deformity pattern, MTPJ position, skin changes
- Flexibility test: Passive correction with manipulation
- Silverskiold test: Claw deformity reduces with ankle DF
- MTPJ stability: Dorsal drawer test for plantar plate integrity
- Neurovascular: Sensation, pulses, capillary refill
- Global foot: Cavus deformity, hindfoot alignment, ankle ROM
Systematic examination identifies the primary deformity, flexibility, and associated pathology.
Beware the Neurological Claw Toe
Bilateral claw toes in young patient suggest underlying neuromuscular disease. Look for pes cavus, clawed hallux, weak intrinsic muscles, and sensory changes. Common causes include Charcot-Marie-Tooth disease, polio sequelae, spinal dysraphism, or hereditary motor-sensory neuropathy. MRI spine and EMG/nerve conduction studies are indicated. Addressing the underlying cavus and muscle imbalance is essential - isolated toe correction will fail without treating the driving pathology.
Physical Examination Tests
Key Clinical Tests
| Test | Technique | Positive Finding | Interpretation |
|---|---|---|---|
| Passive Correction Test | Manually straighten the toe with MTPJ, PIPJ, DIPJ neutral | Deformity fully corrects | Flexible deformity - soft tissue procedure appropriate |
| Passive Correction Test | Attempt to straighten the toe passively | Deformity persists despite force | Rigid contracture - requires bony surgery |
| Silverskiold Test (Modified) | Passively dorsiflex ankle and observe toe position | Claw deformity reduces with ankle DF | Gastrocnemius tightness driving flexor pull - tendon release indicated |
| MTPJ Dorsal Drawer | Stabilize metatarsal head, translate proximal phalanx dorsally | Excessive dorsal translation (more than 2mm) | Plantar plate insufficiency - crossover toe developing |
| Metatarsal Head Palpation | Palpate plantar aspect of metatarsal heads during stance | Prominent, painful metatarsal head | Metatarsalgia from MTPJ hyperextension - address in surgery |
Differential Diagnosis
Why Differential Diagnosis Matters
Not every flexed or painful lesser toe is a primary structural deformity. Distinguish a true hammer/claw/mallet toe from conditions that mimic or drive forefoot pain - getting this wrong leads to operating on the wrong structure (e.g. resecting a PIPJ when the real problem is an interdigital neuroma or MTPJ synovitis).
Differential Diagnosis of the Painful or Deformed Lesser Toe
| Condition | Key Distinguishing Features | Investigation | Management Pointer |
|---|---|---|---|
| Hammer / claw / mallet toe | Fixed joint posture (PIPJ, all-joint, or DIPJ); dorsal or tip corn | Weight-bearing radiographs; clinical flexibility test | Soft tissue vs bony correction by flexibility |
| Plantar plate tear / crossover toe | MTPJ pain, dorsal drawer positive, deviation/overlap, V-sign | MRI or ultrasound of plantar plate | Plantar plate repair plus or minus Weil osteotomy |
| Interdigital (Morton) neuroma | Burning interspace pain, Mulder click, no fixed joint deformity | Ultrasound or MRI; diagnostic injection | Footwear, injection, excision - not toe surgery |
| Freiberg infraction | Localised MTP head pain, often 2nd ray, adolescent/young adult | Radiograph - flattening/sclerosis of metatarsal head | Offloading; joint debridement or osteotomy if advanced |
| Inflammatory arthropathy (RA, psoriatic) | Polyarticular, synovitis, MTPJ erosions, bilateral | Inflammatory markers, autoantibodies, radiographs | Medical control first; reconstruction when quiescent |
| Neuromuscular cavus (CMT, dysraphism) | Bilateral claw toes, pes cavus, weak intrinsics, sensory change | EMG/NCS, MRI spine, genetic testing | Treat cavus and imbalance, not just the toes |
| Subungual / soft tissue lesion or infection | Focal swelling, nail change, erythema, no joint contracture | Examination, swab/imaging if infection suspected | Treat the lesion or infection directly |
Investigations
Imaging Protocol
Standard views: AP, lateral, oblique of entire foot.
What to assess:
- MTPJ alignment and subluxation
- IP joint arthritis or deformity
- Metatarsal parabola and relative lengths
- Pes cavus or planus deformity
- Hallux valgus or rigidus
Weight-bearing films show the true functional deformity and metatarsal load distribution.
Indications: Suspected plantar plate tear, MTPJ synovitis, soft tissue mass.
What to assess:
- Plantar plate integrity (T2 hyperintensity, discontinuity)
- MTPJ synovitis and effusion
- Collateral ligament injury
- Flexor tendon pathology
MRI delineates plantar plate tears in crossover toe - guides repair versus reconstruction.
EMG/Nerve Conduction Studies: Identify peripheral neuropathy pattern.
MRI Spine: Rule out spinal dysraphism, tethered cord, syrinx.
Genetics: Consider CMT genetic testing if family history and progressive cavovarus.
Identifying neurological cause prevents surgical failure and guides comprehensive treatment.
Radiographic Findings
Weight-bearing AP foot radiograph shows the key pathology. Look for MTPJ subluxation (proximal phalanx dorsal to metatarsal head), PIPJ flexion deformity creating a "V" or "Z" shape, and relative metatarsal lengths. A long second metatarsal (Morton's foot) increases risk of second toe hammer and crossover deformity. Lateral radiograph shows the degree of PIPJ and DIPJ flexion and confirms MTPJ dorsiflexion angle.
Imaging Gallery



Management Algorithm
Conservative Treatment Principles
Indications:
- Asymptomatic or mildly symptomatic deformities
- Flexible deformities without significant pain
- Patient unwilling or unfit for surgery
- Early-stage crossover toe (Grade 0-I)
Conservative Measures
- Wide toe box shoes: Accommodate deformity, reduce pressure
- Low heel height: Reduce forefoot pressure and FDL pull
- Soft uppers: Minimize dorsal corn irritation
- Adequate length: Prevent toe jamming and flexion posture
Proper footwear is the foundation of conservative care - 70% of mild cases improve with shoe modification alone.
- Dorsal pads: Protect PIPJ corns from shoe pressure
- Toe sleeves: Silicone or gel sleeves cushion deformity
- Toe spacers: Separate toes, reduce interdigital corns
- Metatarsal pads: Offload metatarsal heads in metatarsalgia
- Arch supports: Support medial longitudinal arch in flexible flatfoot
Padding provides symptomatic relief but does not correct underlying deformity.
- Buddy taping: Tape affected toe to adjacent normal toe
- Dorsal splinting: Night splints maintain IP extension
- Plantar flexion taping: Pull MTPJ into plantarflexion
Taping works only for flexible deformities and requires patient compliance - limited long-term efficacy.
- Avoid prolonged walking or standing
- Swimming and cycling instead of impact activities
- Rest and ice for acute flares
- NSAIDs for inflammatory pain (MTPJ synovitis)
Activity modification reduces symptoms but does not alter natural history of progression to rigid deformity.
Limitations of Non-Operative Treatment
Conservative management is palliative, not curative. Flexible deformities may stabilize with footwear and padding, but rigid contractures will not reverse. The natural history is progression from flexible to rigid over years to decades. Once fixed contracture develops, only surgical correction can restore alignment. Patient expectations must be realistic - conservative care buys time and reduces symptoms, but most symptomatic rigid deformities eventually require surgery.
Non-operative management is the first line for all deformities, but surgical intervention is indicated when conservative measures fail.
Surgical Technique
Girdlestone-Taylor Procedure for Flexible Claw Toe
Indication: Flexible claw toe with dynamic imbalance, passively reducible MTPJ, no fixed PIPJ contracture.
Principle: Harvest FDL, reroute it dorsally through the proximal phalanx, and suture to extensor hood. This converts the deforming flexor force into a correcting force that plantarflexes the MTPJ and extends the IP joints.
Surgical Steps
- Incision: 2cm longitudinal plantar incision at level of MTPJ crease
- Dissection: Identify FDL tendon running deep to FDB
- Harvest: Transect FDL as far distally as possible (DIPJ level preferred)
- Deliver: Pull tendon proximally into wound with hemostat
Distal transection ensures adequate tendon length for transfer and avoids tethering.
- Dorsal incision: Longitudinal 2cm incision over proximal phalanx
- Expose bone: Retract EDL and extensor hood laterally
- Drill holes: Two parallel 2.0mm drill holes from plantar-lateral to dorsal-medial
- Trajectory: Aim toward extensor hood insertion, avoid fracturing thin cortex
Drill holes allow tendon passage from plantar to dorsal, creating the mechanical advantage.
- Pass tendon: Thread FDL through drill holes using suture passer or wire loop
- Emerge dorsally: Tendon exits on dorsal aspect of proximal phalanx
- Tension: Hold MTPJ in 10-15° plantarflexion, IP joints in neutral extension
- Suture: Weave tendon through extensor hood and suture to itself with non-absorbable suture (2-0 Ethibond)
Proper tensioning is critical - too tight creates MTPJ plantarflexion deformity, too loose allows recurrent claw.
- Assess MTPJ: If MTPJ does not reduce to neutral after transfer, release dorsal capsule
- Release: Incise dorsal MTPJ capsule transversely
- Reduce: Manually plantarflex MTPJ to neutral alignment
- Avoid over-release: Excessive release risks MTPJ instability
MTPJ must be passively reducible pre-operatively or the transfer will fail - add capsule release for borderline cases.
- Skin closure: 4-0 nylon interrupted sutures
- Dressing: Non-adherent gauze, gauze padding between toes
- Splint: Buddy tape to adjacent toe, or plantar-flexion strap
- No K-wire: Transfer provides dynamic correction, K-wire not typically needed
Post-op splinting maintains correction during tendon healing (6 weeks).
Technical Pearls
- Drill hole trajectory: Aim for extensor hood insertion site (mid-proximal phalanx dorsum)
- Tendon length: Harvest FDL as distally as possible for adequate length
- Tensioning test: After suturing, passively flex ankle - toe should extend without excessive MTPJ plantarflexion
- Multiple toes: Can transfer multiple toes simultaneously in bilateral claw
Successful transfer requires precise tensioning and adequate tendon length.
Pitfalls to Avoid
- Over-tensioning: Creates MTPJ plantarflexion deformity (cock-up toe)
- Under-tensioning: Recurrent claw deformity
- Inadequate FDL release: Tethering prevents full correction
- Operating on rigid MTPJ: Transfer fails if MTPJ does not reduce passively - add capsule release or choose fusion
Pre-operative flexibility assessment is critical - do not transfer on rigid deformity.
When to Add PIPJ Fusion to Transfer
If the PIPJ is rigid (does not passively extend), the flexor to extensor transfer alone will fail. In this case, add PIPJ resection arthroplasty or fusion to straighten the toe. The transfer corrects the MTPJ hyperextension and dynamic imbalance; the PIPJ fusion addresses the fixed contracture. Combined procedures are common in moderate-to-severe claw toes with mixed flexible and rigid components.
Flexor to extensor transfer is a powerful procedure for dynamic claw toe but requires careful patient selection (flexible MTPJ).
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Recurrent deformity | 10-20% | Inadequate soft tissue release, untreated MTPJ hyperextension, progressive neuromuscular disease | Revision surgery - add missing component (fusion if did arthroplasty, transfer if inadequate balancing) |
| Nonunion (PIPJ fusion) | 5-10% | Inadequate cartilage removal, smoking, poor bone quality, unstable fixation | Revision fusion with better fixation (screw instead of K-wire), bone graft if defect |
| Malunion (PIPJ fusion) | 5-15% | Improper alignment at surgery, K-wire migration, inadequate fixation | If symptomatic: revision osteotomy and re-fusion; if asymptomatic: observe |
| Floppy toe (over-resection) | 10-15% | Excessive bone resection at arthroplasty, loss of structural support | Difficult to treat - revision fusion if severe, otherwise conservative management |
| Infection (superficial) | 2-5% | Diabetes, neuropathy, smoking, poor hygiene, K-wire left protruding | Oral antibiotics, pin removal if around K-wire; most resolve without sequelae |
| Infection (deep/osteomyelitis) | Under 2% | Diabetes with neuropathy, vascular disease, open wound | IV antibiotics, surgical debridement, possible amputation if severe |
| Neurovascular injury | Under 1% | Excessive dissection, blind retraction, anatomical variation | Digital nerve or artery injury - sensory loss or ischemia; if toe viable, observe; if ischemic, may require amputation |
| Stiffness (adjacent joints) | 5-10% | Prolonged immobilization, excessive scar tissue, K-wire across multiple joints | Physical therapy, passive ROM exercises; usually improves over 3-6 months |
| Transfer failure (FDL to extensor) | 10-20% | Under- or over-tensioning, operating on rigid MTPJ, inadequate FDL release | Revision with proper tensioning or convert to MTPJ fusion if joint damage |
| Metatarsalgia (transfer of pressure) | 5-15% | Over-correction with toe plantarflexion, unaddressed long metatarsal, adjacent metatarsal overload | Orthotic metatarsal padding, if severe: Weil osteotomy of adjacent metatarsal |
Vascular Complications in Diabetic or PAD Patients
Assess vascular status pre-operatively in all diabetic or elderly patients. Obtain palpable pulses, ankle-brachial index (ABI), and transcutaneous oxygen pressure (TcPO2) if concern for PAD. Lesser toe surgery has higher complication rates in vascular compromise - wound dehiscence, infection, and toe necrosis occur in 10-20% of diabetic neuropathy patients versus under 5% in healthy patients. Consider toe amputation instead of reconstruction if vascular supply marginal (ABI under 0.5, TcPO2 under 30 mmHg).
Postoperative Care and Rehabilitation
Typical Rehabilitation Timeline
Recovery Milestones
- Analgesia: Multimodal pain control (oral opioids, NSAIDs, ice, elevation)
- Dressing: Bulky dressing with gauze padding between toes
- Immobilization: Post-op shoe or sandal, buddy taping
- Weight-bearing: Heel weight-bearing only, non-weight-bearing on forefoot
- Elevation: Keep foot elevated above heart 23 hours/day for 48 hours
Strict elevation and rest reduce swelling and promote early healing.
- Wound check: Inspect incision at 7-10 days, remove sutures at 10-14 days
- Dressing change: Weekly dressing changes, maintain buddy taping
- Weight-bearing: Gradual increase to full weight-bearing in post-op shoe
- ROM: Gentle passive ROM of unfused joints (MTPJ, non-operated PIPJ)
- Pin care: If K-wire present, daily cleaning with alcohol swab
Early mobilization prevents stiffness while protecting surgical repair.
- Pin removal: Remove K-wire at 4-6 weeks in clinic (no anesthesia needed)
- Footwear transition: Transition to wide, stiff-soled athletic shoe
- Buddy taping: Continue buddy taping for additional 2-4 weeks after pin removal
- Physiotherapy: Active ROM exercises, toe flexion/extension, marble pickups
- Return to work: Sedentary work at 2-3 weeks, standing work at 6 weeks
Progressive mobilization and protection as soft tissues and bone heal.
- Radiographs: If fusion performed, X-rays at 6 weeks to confirm healing
- Footwear: Regular shoes with wide toe box, avoid high heels and narrow shoes
- Activity: Walking, swimming, cycling allowed; avoid running and jumping
- Strengthening: Towel curls, resistance band exercises for foot intrinsics
Strengthening and return to normal activities as tolerated.
- Full activity: Return to sports and impact activities at 3 months
- Footwear education: Permanent change to supportive, wide toe box shoes
- Surveillance: Monitor for recurrent deformity, adjacent toe problems
- Final assessment: Expect 85-90% of final outcome by 6 months
Full recovery takes 6-12 months - swelling can persist for up to 1 year.
Post-Op Expectations
Set realistic expectations pre-operatively. Lesser toe surgery provides pain relief and functional improvement in 80-90% of cases, but cosmetic results may be imperfect. Expect mild swelling for 6-12 months, slight toe shortening, and some stiffness. Perfect alignment and completely normal appearance are unrealistic goals. Patients seeking cosmetic perfection may be dissatisfied despite good functional outcomes. Goal is a pain-free, functional toe that fits in shoes.
Rehabilitation is gradual and emphasizes protection during healing followed by progressive mobilization.
Outcomes and Prognosis
Outcomes by Procedure Type
| Procedure | Success Rate | Recurrence | Patient Satisfaction | Key Outcome |
|---|---|---|---|---|
| Flexor tenotomy (flexible hammer toe) | 75-85% | 15-25% | Good | Simple, quick recovery, but higher recurrence than fusion |
| PIPJ resection arthroplasty | 70-80% | 20-30% | Moderate | Potential for floppy toe, less durable than fusion |
| PIPJ fusion | 85-95% | 5-10% | Excellent | Gold standard - high fusion rate, low recurrence, durable |
| Flexor to extensor transfer (flexible claw) | 70-85% | 15-30% | Good-Excellent | Effective for dynamic deformity, requires precise tensioning |
| Crossover toe repair (Grade I-II) | 60-75% | 25-40% | Moderate-Good | Complex pathology, multi-level surgery, moderate outcomes |
| Crossover toe MTPJ arthroplasty (Grade III) | 70-80% | 10-20% | Moderate | Salvage procedure, sacrifices MTPJ but relieves pain |
Predictors of Poor Outcome
Factors associated with higher failure and recurrence rates:
- Inadequate initial correction - incomplete soft tissue release or inadequate bony correction
- Untreated underlying pathology - cavus foot, neuromuscular disease, hallux valgus
- Smoking - impairs bone and soft tissue healing, increases nonunion and infection
- Diabetes with neuropathy - wound healing problems, infection, Charcot risk
- Unrealistic expectations - patients seeking cosmetic perfection versus functional improvement
- Operating on rigid deformity with soft tissue procedure - flexor transfer on non-reducible MTPJ fails
- Failure to address adjacent pathology - untreated metatarsalgia, long metatarsal, MTPJ instability
Addressing these factors pre-operatively and selecting appropriate procedures improves outcomes.
Long-Term Prognosis
Favorable Prognosis Factors
- Isolated flexible deformity in healthy patient
- Proper procedure selection matching deformity and flexibility
- Adequate initial correction with complete releases and stable fixation
- Post-op compliance with protected weight-bearing and footwear
- Normal neurovascular status and no underlying systemic disease
These patients achieve 85-95% good-to-excellent outcomes with low recurrence.
Guarded Prognosis Factors
- Multiple rigid toes requiring simultaneous corrections
- Revision surgery for failed prior procedure
- Diabetic neuropathy or peripheral vascular disease
- Progressive neuromuscular disease (CMT, polio)
- Severe MTPJ instability with plantar plate rupture
These patients have 60-70% success rates and higher complication and recurrence rates.
Controversies and Areas of Uncertainty
Fusion vs Resection Arthroplasty for PIPJ
Resection arthroplasty is quicker and preserves some length, but fibrous (not bony) union is common and floppy-toe risk exists with over-resection. Arthrodesis gives a more rigid, predictable result. Head-to-head high-level data are limited - choice remains surgeon- and patient-specific (age, demand, revision setting).
Intramedullary Implant vs K-wire
Implants may improve radiographic union and avoid pin-track issues and a second visit for removal, but two systematic reviews found no functional or satisfaction advantage over K-wire despite far higher cost. The standard of care is not settled and RCTs are awaited.
Plantar Plate Repair Technique and Approach
Dorsal (with Weil osteotomy) versus direct plantar approach, suture-anchor versus suture-only, and the role of the flexor-to-extensor transfer as an adjunct are all debated. Higher-grade tears give less reliable stability whichever technique is used.
Prophylactic Surgery in the Neuropathic Foot
Flexor tenotomy to offload clawed toe tips can prevent or heal apical ulcers in diabetic/neuropathic feet, but timing, patient selection and durability versus offloading alone remain uncertain - balanced against the higher wound and infection risk of operating on an at-risk foot.
How to Handle Controversy in a Viva
When asked about a controversial choice (fusion vs arthroplasty, implant vs K-wire), do not pick dogmatically. State that the evidence is largely Level III-IV, summarise the trade-offs, and frame your answer around the individual patient - flexibility of the deformity, age and demand, bone quality, vascular status, cost/access, and whether it is a primary or revision case. Examiners reward balanced, evidence-aware reasoning over a memorised single answer.
Evidence Base and Key Studies
Correction of Clawtoes by the Girdlestone-Taylor Flexor-Extensor Transfer
- Case series of 39 feet in 31 patients (mean age 57.5 years) treated with the Girdlestone-Taylor flexor-to-extensor transfer; mean follow-up 38 months
- Wide variation in aetiology and severity; reduction of metatarsalgia and callosities with improved toe shape achieved in most cases
- Procedure relied on subjective satisfaction, pain relief and recurrence of callosities as outcome measures
- Authors recommended the transfer even in elderly patients, avoiding radical resection or amputation
Operative Repair of the Fixed Hammertoe Deformity
- 63 patients (118 toes) evaluated at mean 61-month follow-up after PIPJ resection arthroplasty with intramedullary K-wire for fixed hammertoe
- Bony fusion of the PIPJ occurred in 81% of toes; the remaining 19% formed a stable fibrous union
- Pain relieved in 92% and subjective satisfaction reported by 84%; mean postoperative AOFAS score 83
- Malalignment and numbness were the principal factors associated with an unsatisfactory result; minor complications in 5%
Prospective Protocol for Surgical Treatment of Lesser MTP Joint Plantar Plate Tears
- 68 patients (100 MTP joints) prospectively graded by an anatomical plantar plate tear classification and treated by a grade-based protocol
- Grade 0-I: radiofrequency shrinkage; Grade II-III: direct plantar plate reinsertion; Grade IV: flexor-to-extensor transfer; all combined with a Weil osteotomy
- Significant improvement in AOFAS, VAS, stability and toe purchase across all grades (P less than .0001)
- Grades I, III and IV had inferior stability and toe purchase versus grades 0 and II; Grade IV achieved only a fair mean AOFAS (72)
Implants for PIPJ Arthrodesis of the Lesser Toes: A Systematic Review
- Systematic review of 12 studies comparing 12 intramedullary implants in 797 patients (1118 toes) for hammer or claw toe PIPJ arthrodesis
- Reported fusion rates ranged widely from 22.2% to 96% depending on implant and study
- Four studies comparing an implant directly with K-wire showed improved union rates with the implant (P less than 0.05)
- Function, pain relief, satisfaction and quality of life all improved but were equivocal between implants and K-wire; all studies were high or critical risk of bias
Ideal Implant Choice for PIPJ Arthrodesis in Hammer/Claw Toe Correction
- Systematic review of 5 studies (1 RCT, 4 case-controlled) comparing K-wires with novel internal fixation devices for PIPJ arthrodesis
- Novel intramedullary devices showed promising union rates compared with K-wires
- No advantage of internal devices over K-wires in pain, patient satisfaction, foot function or complication rates
- Internal devices avoid pin-track issues and the need for later removal but at higher cost
Hammer Toe Correction Using an Absorbable Intramedullary Pin
- 48 PIPJ arthrodeses in 35 patients for fixed rigid hammertoe using a 2-mm absorbable intramedullary pin; mean follow-up 38.5 months
- Procedure described as simple and safe with high patient satisfaction and minimal complications
- No pin-track management or hardware removal required, unlike percutaneous K-wires
- Indicated when the MTPJ is stable, skin is intact and the proximal phalanx canal is 2.0 mm or less; also useful in metal allergy
High Heritability and Prevalence of Lesser Toe Deformities (Framingham Foot Study)
- Population-based study of 1,370 adults (mean age 66 years, 57% women) from the Framingham Foot Study using a validated examination
- Prevalence of lesser toe deformities 29.6% and hallux valgus 31% in this older community-dwelling cohort
- Significant heritability of lesser toe deformity (0.49-0.90 depending on age and sex); 0.65 in those over 70 years
- First demonstration that common forefoot deformities are strongly heritable, not solely footwear-driven
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Flexible Hammer Toe Classification and Management (2-3 min)
"A 52-year-old woman presents with painful second toe deformity. She has a dorsal corn over the PIPJ that prevents her from wearing closed-toe shoes. On examination, the PIPJ is flexed 45 degrees, the MTPJ is in neutral, and the DIPJ is extended. The deformity passively corrects with manipulation. Weight-bearing foot radiographs show PIPJ flexion with no arthritis. What is your diagnosis and management plan?"
Scenario 2: Claw Toe Surgical Technique (3-4 min)
"A 38-year-old man with Charcot-Marie-Tooth disease presents with bilateral claw toes affecting the second through fifth toes. He has pes cavus and metatarsalgia. On examination, the MTPJ is hyperextended 40 degrees, the PIPJ is flexed 60 degrees, and the DIPJ is flexed 30 degrees. The deformity reduces when you passively dorsiflex the ankle (positive Silverskiold test). Walk me through your surgical approach for the flexible claw toe deformity."
Scenario 3: Crossover Toe Complication Management (2-3 min)
"A 60-year-old woman underwent plantar plate repair and flexor to extensor transfer for Grade II crossover toe 3 months ago. She returns with recurrent medial deviation of the second toe and persistent metatarsalgia. On examination, the second toe is crossing over the hallux again, and there is tenderness at the second MTPJ with positive dorsal drawer test. What has happened and how do you manage this?"
MCQ Practice Points
Anatomy Question
Q: Which muscle transfer is performed in the Girdlestone-Taylor procedure for flexible claw toe? A: Flexor digitorum longus (FDL) to the extensor hood. The FDL is harvested from its insertion at the distal phalanx, passed through drill holes in the proximal phalanx, and sutured to the extensor hood on the dorsal side. This converts the deforming flexor force into a correcting force that plantarflexes the MTPJ and extends the IP joints. The procedure only works if the MTPJ is passively reducible; rigid MTPJ requires capsule release or bony correction.
Classification Question
Q: What is the key clinical difference between hammer toe and claw toe? A: MTPJ position. Hammer toe has MTPJ in neutral or mild hyperextension with primary deformity at the PIPJ (flexion). Claw toe has MTPJ hyperextension (key distinguishing feature) plus flexion at both PIPJ and DIPJ. Mallet toe is isolated DIPJ flexion. Knowing this distinction guides treatment - hammer toe needs PIPJ correction, claw toe requires MTPJ and IP joint correction.
Treatment Question
Q: What is the gold standard surgical treatment for rigid hammer toe? A: PIPJ fusion (arthrodesis). Fusion provides the most durable and predictable correction for rigid hammer toe, with fusion rates of 85-95% and patient satisfaction over 90%. The PIPJ is fused in 15-25 degrees of flexion using intramedullary K-wire or headless screw. Resection arthroplasty (DuVries procedure) is simpler but has higher recurrence rates and risk of floppy toe from over-resection. For young, active patients, fusion is preferred.
Complication Question
Q: What is the most common cause of floppy toe deformity after hammer toe surgery? A: Excessive bone resection during PIPJ resection arthroplasty. Over-resection of the proximal phalanx head removes structural support, creating a short, unstable toe with loss of ground contact and poor function. The appropriate amount to resect is 3-5mm (the head only). Floppy toe is difficult to treat - prevention is key by performing meticulous arthroplasty or choosing fusion instead for more predictable length preservation.
Biomechanics Question
Q: What is the Silverskiold test in the context of claw toe assessment? A: Passive ankle dorsiflexion test to assess if claw deformity reduces. If the claw toe deformity corrects when the ankle is passively dorsiflexed, it indicates that gastrocnemius tightness and extrinsic flexor (FDL/FDB) pull are driving the deformity - this is a flexible, dynamic deformity amenable to flexor release or transfer. If the deformity persists regardless of ankle position, the contracture is fixed at the joint level and requires bony correction (fusion or arthroplasty). This test guides procedure selection.
Evidence Question
Q: What is the recurrence rate of lesser toe deformities after surgical correction? A: 10-20% over 5-10 years for most procedures. Recurrence is higher with resection arthroplasty (20-30%) versus fusion (5-10%). Flexor to extensor transfer has 15-30% recurrence if tensioning is suboptimal or if underlying cavus deformity is not addressed. Crossover toe repair has the highest failure rate (25-40%) due to complex multi-factorial pathology. Patient factors (diabetes, smoking, neuromuscular disease) and inadequate initial correction increase recurrence risk.
Guidelines, Registries & Global Practice
Global Epidemiology
- Prevalence: Lesser toe deformities affect roughly 30% of community-dwelling older adults (Framingham Foot Study - 29.6%)
- Sex: Female predominance (footwear, ligamentous laxity, hormonal factors)
- Heritability: Strong genetic contribution (0.49-0.90), highest after age 70 - not purely footwear-driven
- Associations: Hallux valgus, pes cavus, inflammatory arthritis, diabetic and neuromuscular disease
- Resource setting: Higher symptomatic burden where constrictive footwear is common; neuromuscular causes (leprosy, polio sequelae, untreated CMT) remain relevant in limited-resource regions
Deformity is common, heritable and frequently coexists with hallux valgus - screen the whole forefoot, not just the symptomatic toe.
Registry & Evidence Notes
- No dedicated lesser toe registry: Unlike arthroplasty (NJR, AJRR, AOANJRR), forefoot reconstruction is not captured in implant registries
- Evidence base: Predominantly Level III-IV case series and small systematic reviews; few randomised trials
- Implant data: Intramedullary PIPJ devices show variable union (22-96%) with no proven functional gain over K-wire (Arumugam 2025; Wei 2020)
- PROMs: AOFAS lesser MTP-IP and MOXFQ scores increasingly used to standardise outcome reporting
Quote the evidence honestly in vivas - lesser toe surgery is reliable for pain but lacks high-level comparative data.
Side-by-Side Guideline & Society Positions
| Body / Region | Emphasis | Key Practice Point |
|---|---|---|
| AAOS / AOFAS (US) | Stepwise care; flexibility-based algorithm | Conservative trial first; PIPJ arthrodesis favoured for rigid deformity; plantar plate grading guides MTPJ surgery |
| BOA / BOFAS (UK) | Shared decision-making, PROMs | Document MOXFQ; reserve surgery for failed non-operative care; K-wire remains standard, implants not routinely funded |
| AO Foundation | Fixation principles | Stable arthrodesis with adequate cartilage resection and compression; K-wire or intramedullary device acceptable |
| EFORT / European consensus | Forefoot reconstruction as a unit | Address coexisting hallux valgus and metatarsal length (Weil osteotomy) at the index procedure to reduce recurrence |
| IWGDF (diabetic foot) | Risk stratification, offloading | Treat clawed toes as ulcer risk; flexor tenotomy to offload tips in neuropathic feet; vascular assessment mandatory |
High-Resource Practice
- MRI and ultrasound to grade plantar plate tears pre-operatively
- Choice of intramedullary implants, headless screws and suture anchors available
- Day-case surgery with regional ankle block and structured PROM follow-up
- Multidisciplinary diabetic foot pathways for offloading and prophylactic surgery
Imaging and implant choice are abundant - the constraint is appropriate selection, not access.
Limited-Resource Practice
- Diagnosis is clinical; plain radiographs guide most decisions
- K-wire fixation and percutaneous flexor tenotomy are mainstay (low cost, reliable)
- Neuromuscular causes (leprosy, polio, untreated CMT) over-represented - treat the driver
- Footwear modification and education are the most cost-effective interventions
Simple, durable techniques (K-wire, tenotomy) and footwear advice deliver most of the benefit at minimal cost.
Consent and Risk Communication (Globally Relevant)
Counsel and document before surgery:
- Realistic expectations: Functional pain relief is reliable; cosmetic perfection and a completely normal-looking toe are not - swelling may persist 6-12 months
- Recurrence: 10-20% over 5-10 years (higher with resection arthroplasty than fusion)
- Specific risks: Floppy/short toe from over-resection, nonunion, malunion, stiffness, numbness, infection
- Conservative trial: Confirm an adequate trial of footwear modification and padding (3-6 months)
- Higher-risk feet: Vascular assessment (pulses, ABI, TcPO2) in diabetic or PAD patients; correct site marking for the right toe
Honest expectation-setting and a documented conservative trial are the strongest protections against dissatisfaction and dispute, regardless of health system.
LESSER TOE DEFORMITIES
Clinical summary
Classification (Joint Involvement)
- •Hammer toe = PIPJ flexion (MTPJ normal, DIPJ neutral/extended)
- •Claw toe = MTPJ hyperextension + PIPJ flexion + DIPJ flexion (all three joints)
- •Mallet toe = DIPJ flexion only (MTPJ and PIPJ normal)
- •Crossover toe = MTPJ instability with medial/lateral deviation (plantar plate tear)
Flexibility Assessment (Critical for Treatment)
- •Flexible = passively correctable, soft tissue procedure (tenotomy, transfer, lengthening)
- •Rigid = fixed contracture, bony procedure (fusion, arthroplasty, osteotomy)
- •Silverskiold test = ankle dorsiflexion reduces claw = flexible, gastrocnemius-driven
- •MTPJ dorsal drawer = excessive translation = plantar plate insufficiency (crossover toe developing)
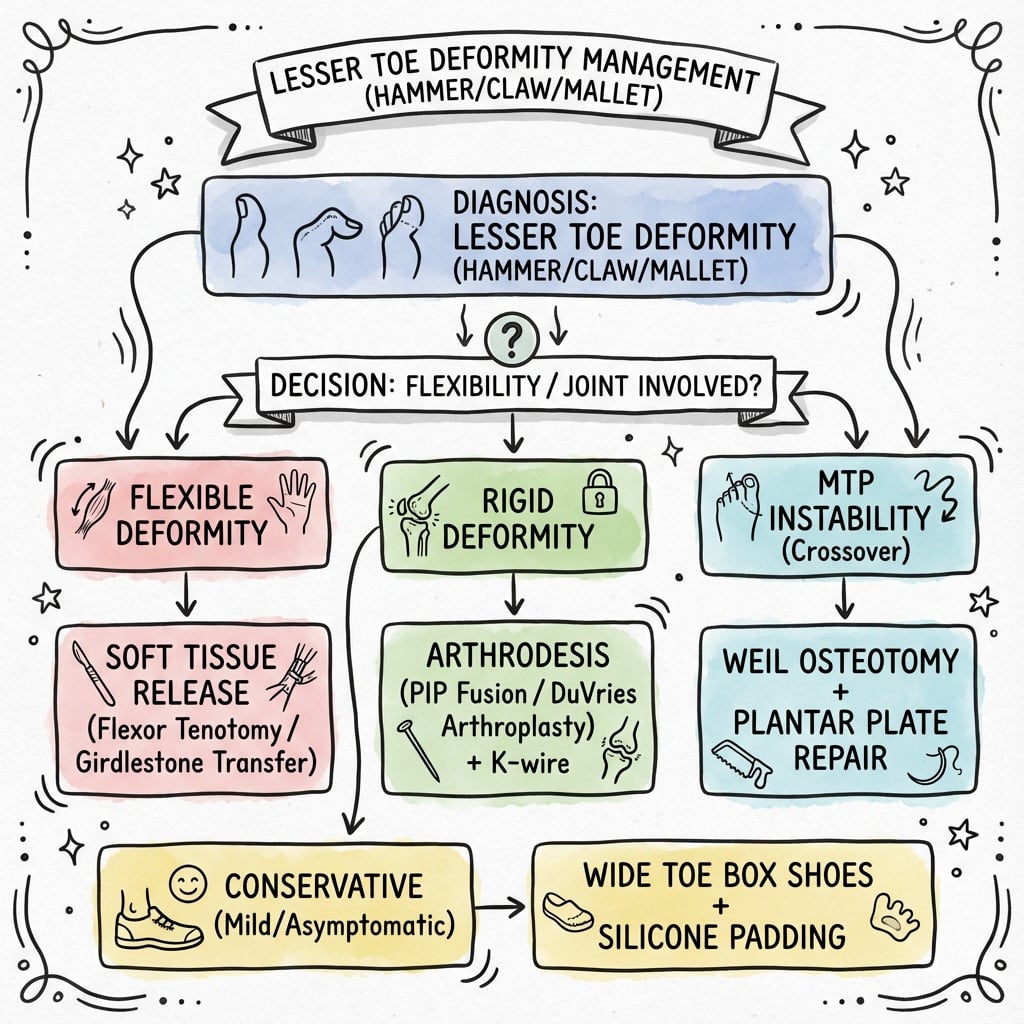
Treatment Algorithm
- •Flexible hammer toe = flexor tenotomy + extensor lengthening
- •Rigid hammer toe = PIPJ fusion (gold standard) or resection arthroplasty
- •Flexible claw toe = flexor to extensor transfer (Girdlestone-Taylor) + address cavus
- •Rigid claw toe = PIPJ fusion + MTPJ capsule release or shortening osteotomy
- •Mallet toe (flexible) = FDL tenotomy; (rigid) = DIPJ fusion
- •Crossover toe Grade I-II = plantar plate repair + flexor transfer; Grade III = MTPJ arthroplasty/fusion
Surgical Pearls
- •PIPJ fusion: 15-25° flexion, K-wire 6-8 weeks or headless screw (permanent), 85-95% fusion rate
- •Flexor to extensor transfer: harvest FDL distally, drill proximal phalanx, tension with MTPJ 10-15° plantarflexion
- •Transfer only works if MTPJ passively reduces - if rigid, add capsule release or choose fusion
- •Resection arthroplasty: resect only 3-5mm (head of proximal phalanx) - over-resection creates floppy toe
Complications and Management
- •Recurrence 10-20% over 5-10 years (higher with arthroplasty vs fusion, higher if underlying pathology not addressed)
- •Floppy toe from over-resection (difficult to treat - prevention key)
- •Nonunion 5-10% (inadequate cartilage removal, smoking, poor fixation) - revision with screw or graft
- •Transfer failure (under/over-tensioning, operating on rigid MTPJ) - revision or convert to fusion
- •Infection higher in diabetes/PAD (8-12% vs 2-5%) - check vascular status pre-op (ABI, TcPO2)
Key Evidence and Outcomes
- •PIPJ resection arthroplasty for fixed hammertoe: 81% bony union, 92% pain relief, 84% satisfaction (Coughlin, Dorris & Polk 2000)
- •Girdlestone-Taylor flexor-to-extensor transfer: reliable relief of metatarsalgia/callosity in flexible deformity, including the elderly (Barbari & Brevig 1984)
- •Plantar plate tears - grade-based protocol with Weil osteotomy improves all grades but higher grades give less stable joints (Nery, Coughlin & Baumfeld 2014)
- •Intramedullary implants for PIPJ fusion may improve union over K-wire but functional outcomes are equivocal (Arumugam 2025; Wei 2020)
- •Lesser toe deformities affect ~30% of older adults and are strongly heritable (Framingham Foot Study 2013)