The Great Orthopaedic Mimic in Children
- Leukaemia - especially ACUTE LYMPHOBLASTIC LEUKAEMIA (ALL), the commonest childhood malignancy - frequently involves the marrow and bone, and a substantial minority of children (around a fifth to a third) present with MUSCULOSKELETAL symptoms (bone/joint pain, limp, refusal to weight-bear, arthralgia or arthritis), which may be the FIRST or even the ONLY presenting feature, BEFORE any obvious haematological abnormality.
- This makes leukaemia a classic ORTHOPAEDIC/RHEUMATOLOGICAL MIMIC: it is misdiagnosed as juvenile idiopathic arthritis, SEPTIC ARTHRITIS, OSTEOMYELITIS, chronic recurrent multifocal osteomyelitis (CRMO), transient synovitis, 'growing pains' or even non-accidental injury - leading to DELAYED diagnosis (studies show diagnosis takes far longer when there are no haematological symptoms).
- RED FLAGS that should prompt a leukaemia work-up: bone pain that is SEVERE, NOCTURNAL or DISPROPORTIONATE to examination, pain that is METAPHYSEAL rather than localising to a joint, systemic features (fever, fatigue, weight loss, pallor), hepatosplenomegaly or lymphadenopathy, and laboratory clues - CYTOPENIAS (anaemia, thrombocytopenia, or a low/normal white-cell count with low platelets), a raised LDH and urate, and an ESR raised out of proportion.
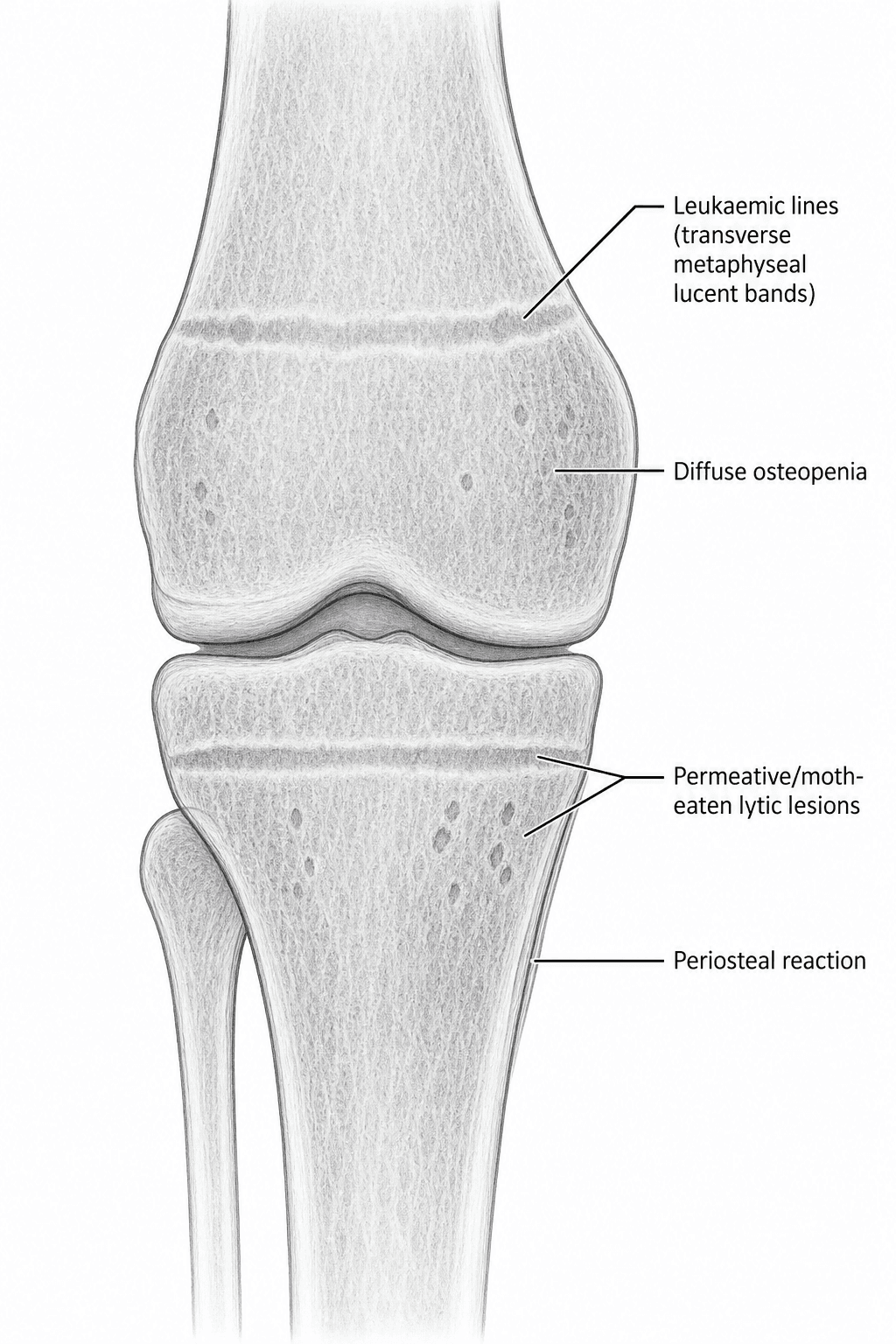
- Characteristic RADIOGRAPHIC features include 'LEUKAEMIC LINES' - transverse RADIOLUCENT METAPHYSEAL BANDS (classic in children but non-specific) - together with diffuse OSTEOPENIA, PERMEATIVE/moth-eaten lytic lesions, periosteal reaction, osteolytic lesions and occasionally vertebral compression fractures; MRI shows diffuse marrow replacement (low T1 signal), and FDG-PET shows multiple bone foci/systemic marrow uptake.
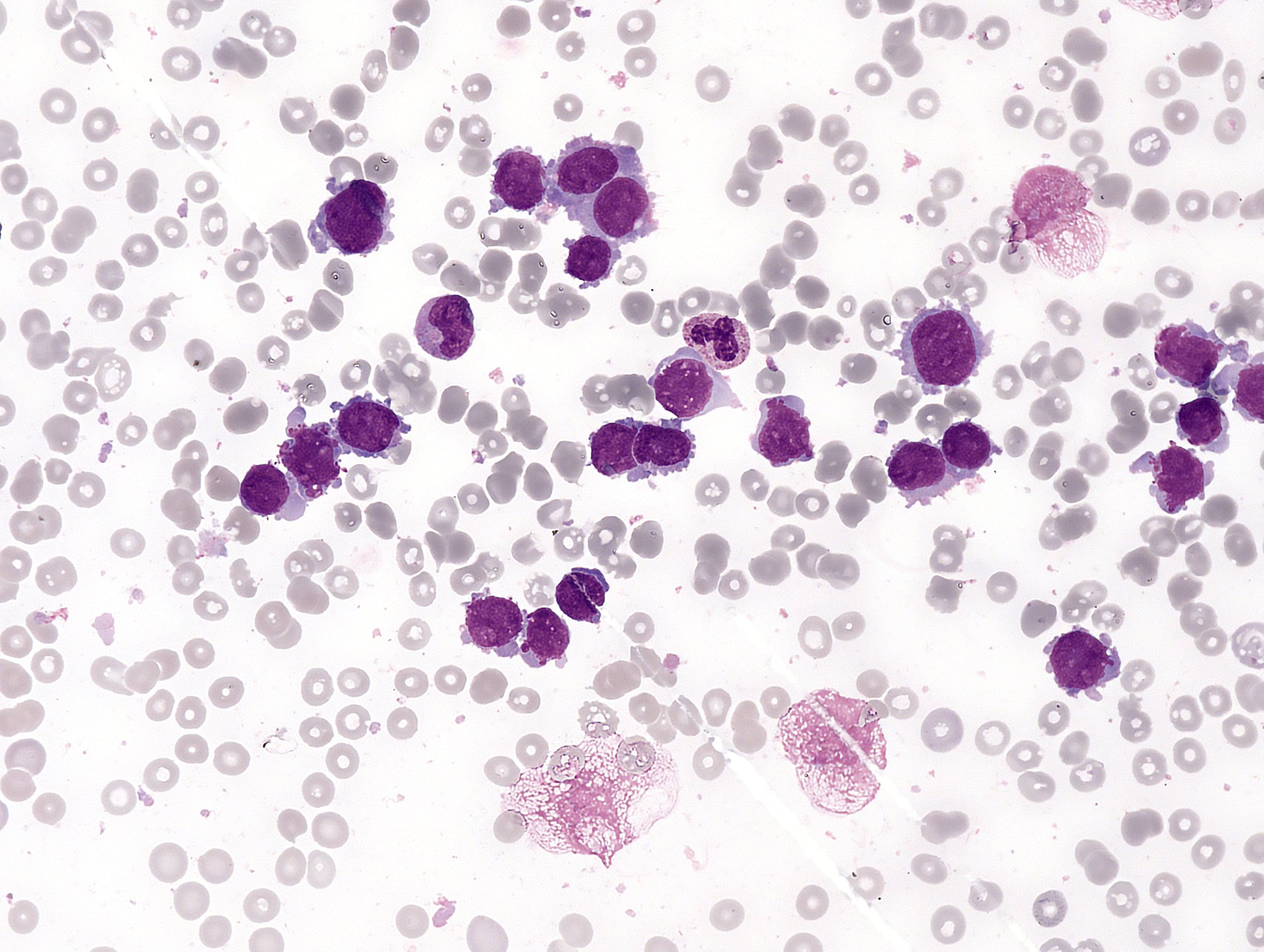
- DIAGNOSIS rests on the FULL BLOOD COUNT and BLOOD FILM (cytopenias, circulating blasts), supported by LDH/urate, and is CONFIRMED by BONE MARROW aspirate/biopsy showing blasts - so any child with unexplained bone/joint pain plus a red flag or abnormal counts must have these BEFORE the pain is attributed to a benign orthopaedic cause.
- The ORTHOPAEDIC ROLE is principally RECOGNITION and prompt referral to paediatric haematology-oncology (treatment is chemotherapy-led); the surgeon must AVOID inappropriate surgery (e.g. washing out a 'septic joint' or biopsying a 'bone lesion' that is actually leukaemia), manage pathological fractures, and be aware of treatment-related complications such as STEROID-INDUCED OSTEONECROSIS.
- “Childhood ALL often presents with musculoskeletal/bone pain - a classic mimic of JIA, septic arthritis, osteomyelitis and CRMO; diagnosis is frequently delayed.
- “Red flags: night/disproportionate/metaphyseal bone pain, systemic features, hepatosplenomegaly, CYTOPENIAS (esp low platelets), high LDH/urate, ESR out of proportion.
- “Radiographs: LEUKAEMIC LINES (metaphyseal lucent bands) + osteopenia + permeative lesions. Diagnose with FBC/film + bone marrow; recognise & refer (don't operate inappropriately).
Childhood ALL can present as bone/joint pain mimicking JIA, septic arthritis, osteomyelitis or CRMO - often before haematological signs, causing delayed diagnosis.
Check an FBC and blood film (cytopenias/blasts), LDH/urate, and have a low threshold for bone marrow examination before treating a benign orthopaedic diagnosis.
Presentation & the Orthopaedic Mimic
A significant minority of children with ALL present with musculoskeletal symptoms - bone or joint pain, a limp, refusal to weight-bear, or an arthritis - and in some this is the first or only feature, with the blood film initially looking unremarkable. Because of this, leukaemia is repeatedly misdiagnosed as juvenile idiopathic arthritis, septic arthritis, osteomyelitis, CRMO, transient synovitis or 'growing pains', and the diagnosis is delayed - one series found diagnosis took nearly three times as long in children presenting with musculoskeletal pain without haematological symptoms. The clinician must therefore keep leukaemia in mind whenever a child has unexplained, persistent or atypical bone/joint pain.
Red Flags, Imaging & Diagnosis
- Clinical red flags: severe, nocturnal or disproportionate bone pain; pain that is metaphyseal and non-articular; systemic features (fever, fatigue, weight loss, pallor); hepatosplenomegaly or lymphadenopathy.
- Laboratory red flags: cytopenias (anaemia, thrombocytopenia, or a low/normal white-cell count with low platelets - a 'cytopenia in more than one line'), raised LDH and urate, and an ESR raised out of proportion to a presumed benign cause.
- Imaging: radiographs show leukaemic lines (metaphyseal lucent bands), osteopenia, permeative/moth-eaten lesions, periosteal reaction and sometimes vertebral compression; MRI shows diffuse marrow replacement; FDG-PET shows multifocal bone/marrow uptake.
- Confirm: FBC + blood film then BONE MARROW aspirate/biopsy (blasts) - diagnostic. Always think of leukaemia BEFORE labelling a child's bone/joint pain benign.
"Diffuse marrow replacement" needs a rule you can apply at the viewing station, because a child's marrow is red and therefore dark anyway. The usable test is a comparison, not an absolute: on T1-weighted images, normal marrow - including the normal red marrow of a child - is BRIGHTER than adjacent skeletal muscle. Marrow that is darker than muscle on T1 is abnormal, and in this context that is the sign of blast infiltration. The distribution then does the rest of the work: leukaemic replacement is diffuse, symmetrical and confluent, involving the marrow of both sides in continuity, whereas a primary bone tumour or an osteomyelitis produces a focal lesion with a margin. Fat-suppressed T2/STIR adds sensitivity but is far less specific - red marrow, oedema and infiltration are all bright - so the T1-versus-muscle comparison remains the anchor. (The full approach, including red-marrow reconversion and its age pattern, is in MRI Bone Marrow Signal.)
A caveat worth carrying into a viva: diffuse marrow change on MRI is not by itself a diagnosis of leukaemia. Red marrow reconversion from any cause of chronic anaemia or marrow stress, and marrow stimulated by growth factors, produce the same appearance. MRI raises the suspicion and directs where to look; the marrow aspirate proves it.
The Orthopaedic Role
- Recognition and referral: the key orthopaedic responsibility is to suspect leukaemia and refer promptly to paediatric haematology-oncology; treatment is chemotherapy-led.
- Avoid inappropriate surgery: do NOT wash out a presumed 'septic joint' or biopsy a 'bone lesion' that is in fact leukaemia without first considering and excluding it (check the FBC/film); an unnecessary operation delays diagnosis and adds morbidity.
- Manage skeletal complications: pathological fractures, vertebral collapse, and the late steroid-induced OSTEONECROSIS (especially of the femoral head) that complicates ALL treatment.
- If a bone biopsy is performed for a suspicious lesion, ensure samples reach haematopathology and culture so leukaemia/myeloid sarcoma (chloroma) is not missed.
The single most useful screen in a child with worrying bone pain is the full blood count and film: a cytopenia affecting more than one cell line (e.g. anaemia plus thrombocytopenia), circulating blasts, or a white-cell count that is unexpectedly low or very high should trigger an urgent leukaemia work-up and referral. A normal initial film does NOT exclude leukaemia (the marrow can be involved before the peripheral blood), so persistent or escalating symptoms with red flags warrant bone marrow examination. Do not let a child with leukaemia undergo an arthrotomy for 'septic arthritis' or an osteotomy/biopsy mislabelled as a primary bone tumour.
Telling Leukaemia from Septic Arthritis (the Kocher Trap)
The single most dangerous error is taking a leukaemic child to theatre for an arthrotomy/washout of a presumed septic arthritis. The widely-used Kocher predictors of a paediatric septic hip - inability to weight-bear, fever, a raised ESR/CRP and a raised peripheral white-cell count - can all be mimicked by leukaemia, so a child can score highly on a septic-arthritis pathway yet have leukaemia. Several features pull the diagnosis back towards leukaemia and should be sought before any operation:
- The blood count, read line-by-line. Septic arthritis usually produces a reactive thrombocytosis and a neutrophilia; leukaemia characteristically gives LOW or low-normal platelets, often with anaemia, i.e. a cytopenia in more than one cell line. A 'high inflammatory picture' with a normal or low white-cell count, or with low platelets, is a strong leukaemia clue. Circulating blasts on the film are diagnostic of the trap.
- The pain pattern. Septic arthritis localises to one joint with marked joint-line tenderness and resistance to any movement; leukaemic pain is more often metaphyseal/non-articular, nocturnal, disproportionate and frequently multifocal or migratory rather than confined to a single joint.
- Other labs and examination. A markedly raised LDH and urate, an ESR raised out of proportion to the clinical picture, and hepatosplenomegaly or lymphadenopathy point to leukaemia, not sepsis.
- The rule. In a child being worked up for a septic joint, review the full blood count and film (and have a low threshold for marrow) before arthrotomy - a normal initial film does not exclude leukaemia, so persistent red-flag symptoms still warrant marrow examination. (The criteria themselves and their validation are covered in Kocher Criteria; the management of true paediatric septic arthritis in Septic Arthritis of the Paediatric Hip.)
Leukaemia can satisfy a Kocher septic-arthritis pathway. The discriminators are in the full blood count read by line - sepsis tends to raise platelets (reactive thrombocytosis), leukaemia lowers them and involves more than one line - plus disproportionate/nocturnal/metaphyseal/multifocal pain, very high LDH/urate and organomegaly. Check the FBC/film before you wash out a 'septic joint'.
The Three Numbers That Separate ALL from JIA
Telling a child with leukaemia from a child with juvenile idiopathic arthritis is the version of this problem that reaches a clinic rather than an emergency department, and it has a quantified answer. A multicentre case-control study of 277 children first seen in paediatric rheumatology clinics - 71 who turned out to have ALL and 206 who turned out to have JIA - tested which findings at that first visit actually predicted leukaemia:
- Threshold
- Less than 4 x 10^9/L
- Why it discriminates
- The opposite of the reactive leucocytosis expected in sepsis or active inflammatory arthritis - marrow crowded by blasts fails to release mature cells
- Threshold
- 150-250 x 10^9/L - inside the normal range
- Why it discriminates
- The counter-intuitive one: the platelets do not have to be low. An inflamed child should have a reactive thrombocytosis, so a merely unremarkable platelet count is itself the abnormality
- Threshold
- Pain that wakes the child from sleep
- Why it discriminates
- Marrow-pressure pain does not settle with rest, unlike mechanical or synovitic pain
- Threshold
- Sensitivity 100%, specificity 85%
- Why it discriminates
- No child with all three was ultimately JIA in this cohort - the combination, not any single item, is what carries the weight
- Threshold
- Not discriminating
- Why it discriminates
- Occurred at similar rates in both groups - a child with a genuinely swollen joint and a positive ANA can still have leukaemia
Three-quarters of the children with ALL had no blasts on the peripheral film at that visit. That single figure is why "the film was normal" cannot be allowed to close the question, and why the marrow, not the film, is the test that settles it.
The platelet row inverts the usual instinct, and is worth reading twice. Frank thrombocytopenia and a two-line cytopenia are the late and easy findings; by then the diagnosis is rarely missed. The child who gets missed has a blood count that a quick glance calls normal, and the discriminating observation is a relative one - platelets that ought to be reactively high in a child who is systemically unwell, and are instead sitting quietly in the lower half of the reference range.
What Not to Do Before the Diagnosis Is Made
Three actions taken in good faith before the marrow is examined each cause specific, avoidable harm.
- Why it is taken
- The child scores on a septic-arthritis pathway
- The harm
- Anaesthesia and surgery in a child who may be thrombocytopenic and neutropenic; the diagnosis is delayed, and the joint fluid does not give the answer
- Why it is taken
- A permeative lytic lesion with periosteal reaction looks like Ewing sarcoma
- The harm
- A marrow aspirate would have been quicker, safer and diagnostic. If a lesion is biopsied anyway, tissue must reach haematopathology as well as histopathology and microbiology
- Why it is taken
- The joints are swollen, the child is unwell, and steroids reliably relieve both
- The harm
- The most damaging of the three - see below
Why a trial of steroids is the worst of the three. Glucocorticoids are themselves lymphotoxic - they are a component of ALL induction. Given empirically they will partially treat the leukaemia, so the child improves, which is read as confirmation that the diagnosis was inflammatory. Meanwhile the blasts are cleared from the marrow and the peripheral blood, so a marrow examination performed afterwards can be non-diagnostic or falsely reassuring, delaying diagnosis further and making accurate immunophenotyping and cytogenetic risk stratification - which determine the intensity of the treatment the child will receive - unreliable. Rapid cytoreduction in an undiagnosed child also risks tumour lysis without the prophylaxis that would have been given had anyone known. Take the blood count and film, and if there is any doubt the marrow, before the first dose - not after it.
The Rest of the Differential - and the One Other Malignancy That Presents This Way
- What points to it
- Night pain, metaphyseal and multifocal, low WCC with low-normal platelets, high LDH and urate, organomegaly
- What settles it
- Blood film then BONE MARROW aspirate
- What points to it
- Under 5 years old, often unwell and irritable; abdominal or thoracic mass; periorbital ecchymosis and proptosis from skull/orbital deposits; can also infiltrate marrow and cause cytopenias
- What settles it
- Urinary catecholamines (VMA/HVA), cross-sectional imaging of abdomen and chest, MIBG scintigraphy, marrow examination
- What points to it
- Usually a single diaphyseal lesion with a lamellated periosteal reaction and a soft-tissue mass; may have fever and raised inflammatory markers
- What settles it
- Biopsy through a planned approach, after staging - never before leukaemia has been excluded on the blood count
- What points to it
- Multifocal, symmetrical, metaphyseal, relapsing over months; clavicle involvement is characteristic; cultures sterile
- What settles it
- Diagnosis of exclusion - whole-body MRI, and leukaemia must be excluded first
- What points to it
- Single focus, rapidly progressive, marked local signs, neutrophilia and reactive thrombocytosis
- What settles it
- Aspiration and culture, MRI
- What points to it
- Morning stiffness improving with movement, true synovitis, no night pain, normal or reactive counts
- What settles it
- Clinical, after leukaemia is excluded - and before any steroid is given
- What points to it
- Multiple fractures of differing ages, inconsistent history
- What settles it
- Skeletal survey, safeguarding pathway
Neuroblastoma deserves particular attention because it is the one other malignancy that reproduces almost every feature relied on above. It occurs in a younger child, typically under five; it metastasises to bone with periosteal reaction and permeative lysis; and because it infiltrates marrow it can produce exactly the same cytopenias, so a low count does not distinguish the two. The features that do are extra-skeletal: periorbital ecchymosis with proptosis from orbital deposits, an abdominal mass crossing the midline, hypertension, and in some children opsoclonus-myoclonus. Urinary vanillylmandelic and homovanillic acid are the screening test. The practical point is that the marrow examination arranged for suspected leukaemia will often reveal it, which is another reason the marrow - not a bone biopsy - is the right first invasive investigation in a child with multifocal bone lesions and abnormal counts.
Skeletal Complications of Leukaemia & Its Treatment
- At diagnosis (marrow infiltration): diffuse osteopenia, vertebral compression fractures (back pain and loss of height can be a presenting feature), and pathological long-bone fractures through weakened, infiltrated bone - reflecting both direct blast infiltration and disordered bone turnover.
- Corticosteroid osteonecrosis: high-dose glucocorticoids are central to ALL induction/maintenance, and osteonecrosis is a well-recognised complication, classically of the femoral and humeral heads and often multifocal and bilateral. Two variables dominate the risk, and both are quantified below - age at treatment and which steroid was used. (The pathophysiology and staging of osteonecrosis are covered in Avascular Necrosis of the Hip; the bone effects of steroids in Corticosteroids in Orthopaedics.)
- Glucocorticoid-induced osteoporosis: prolonged steroids reduce bone density and add fragility/vertebral fractures on top of the disease-related osteopenia.
- Methotrexate osteopathy: chronic methotrexate can cause an osteopathy with bone pain, metaphyseal lucent bands and insufficiency fractures (especially distal lower limb), which can itself mimic relapse.
- Growth disturbance: chemotherapy, steroids and (historically) radiotherapy can affect the physis and growth.
- Orthopaedic management: surveillance and joint-preserving measures for early osteonecrosis (activity modification, protected weight-bearing, and core decompression in selected hips) with arthroplasty for collapsed joints in older patients; bone-health optimisation (calcium/vitamin D, weight-bearing) for steroid bone loss; and fracture care coordinated with the oncology team, since timing must respect the chemotherapy schedule and marrow suppression.
How much does age matter? More than almost any other risk factor in orthopaedic oncology. In 1,095 children treated on three consecutive Japanese protocols, symptomatic osteonecrosis on the dexamethasone-era protocol occurred in 0.42% of those treated under the age of 10 and 15.6% of those aged 10 or over - a roughly thirty-fold difference, and the reason surveillance and counselling are pitched at adolescents rather than at all children on treatment. Girls fared worse than boys on the same protocol (6.7% versus 1.3%).
The choice of steroid matters too. Across the same three protocols, osteonecrosis occurred in 0.76% and 0.35% when prednisolone was the only steroid, and rose to 3.6% once dexamethasone partly replaced it. A separate prospective Dutch cohort of 466 children aged 4-18 on a dexamethasone-based protocol found symptomatic osteonecrosis in 6.4%. Dexamethasone gives better central nervous system penetration and better leukaemia control; the osteonecrosis is the price, which is why the trade-off is a live one in protocol design rather than a settled question.
That same Dutch cohort answers a question the exam likes: bone density before treatment did not predict who developed osteonecrosis, so a baseline DXA does not identify the at-risk child. Bone density then fell faster in those who developed osteonecrosis than in those who did not - the osteonecrosis drives the bone loss, partly through the enforced restriction of weight-bearing, rather than low bone density causing the osteonecrosis. The practical consequence is that protected weight-bearing, which the joint needs, works against the skeleton, and bone-health measures should be intensified at the moment osteonecrosis is diagnosed rather than left until a fragility fracture appears.
Split the skeletal complications into disease (osteopenia, vertebral compression, pathological fractures from marrow infiltration) and treatment (corticosteroid osteonecrosis - classically femoral/humeral head, multifocal, commoner in adolescents; glucocorticoid-induced osteoporosis; methotrexate osteopathy with metaphyseal bands/insufficiency fractures). Orthopaedic care is osteonecrosis surveillance/joint preservation vs arthroplasty, bone-health optimisation, and fracture care coordinated with oncology.
Mnemonics & Memory Aids
LEUKAEMIA
Hook:LEUKAEMIA - think of it in any child with atypical bone pain.
RED FLAGS
Hook:RED FLAGS push you to a blood film and marrow.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child presents with bone and joint pain and a possible septic/inflammatory joint. Why must you consider leukaemia, and how would you investigate?”
“What are the radiographic features of leukaemic bone involvement, and what is the orthopaedic surgeon's role?”
“A 6-year-old has had six weeks of joint pain and swelling. The rheumatology registrar has diagnosed juvenile idiopathic arthritis and wants to start prednisolone today. The white cell count is 3.8, the platelets 190, the haemoglobin 108, and the film shows no blasts. What do you say?”
Presentation
- Childhood ALL often presents with MSK pain (bone/joint pain, limp, arthritis)
- Mimics JIA, septic arthritis, osteomyelitis, CRMO -> delayed diagnosis
- May precede haematological signs
Red flags
- Night/severe/disproportionate metaphyseal (non-articular) bone pain
- Systemic: fever, weight loss, fatigue, pallor; hepatosplenomegaly/lymphadenopathy
- Cytopenias (esp more than one line, low platelets), high LDH/urate, ESR out of proportion
The three numbers (ALL vs JIA)
- WCC under 4 x 10^9/L + platelets 150-250 (LOW-NORMAL, not low) + night pain
- All three: sensitivity 100%, specificity 85%. ANA/rash/arthritis do NOT discriminate
- 75% have NO circulating blasts at rheumatology assessment - a clean film excludes nothing
Do NOT, before the marrow
- Wash out a 'septic joint' - and do not biopsy a 'bone tumour'; the marrow is quicker and diagnostic
- Give a steroid: partially treats ALL, clears the marrow, wrecks risk stratification, risks tumour lysis
- MRI rule: marrow DARKER than muscle on T1 is abnormal; leukaemia is diffuse/symmetrical, tumour is focal
Imaging & diagnosis
- Radiographs: leukaemic lines (metaphyseal lucent bands), osteopenia, permeative lesions
- MRI: diffuse marrow replacement; FDG-PET: multifocal bone/marrow uptake
- Confirm: FBC + blood film -> BONE MARROW (blasts)
Orthopaedic role
- Recognise & refer to paediatric haematology-oncology (chemo-led treatment)
- Avoid inappropriate surgery (septic-joint washout/biopsy without checking FBC)
- Manage pathological fractures; aware of steroid-induced osteonecrosis; consider chloroma (AML)
Evidence & Key Studies
Pediatric ALL presenting with musculoskeletal pain without haematological symptoms (utility of FDG-PET)
- Of 58 children with ALL, 12 presented with prominent musculoskeletal pain WITHOUT haematological symptoms; diagnosis took much longer (48.5 vs 17.1 days).
- Three of these were initially misdiagnosed as CRMO, fracture or septic osteomyelitis because of localised imaging and unremarkable blood tests.
- FDG-PET revealed multiple bone foci or systemic marrow uptake in all cases, helping diagnose leukaemia when blood tests were unremarkable.
Predictive factors distinguishing childhood leukaemia from juvenile rheumatoid arthritis (multicentre case-control)
- 277 children first seen in paediatric rheumatology clinics - 71 ultimately ALL, 206 ultimately JRA - compared on findings present at that first visit.
- 75% of the children with ALL had NO blasts on the peripheral blood film at the time of rheumatology evaluation.
- The three predictive factors were a low white cell count (under 4 x 10^9/L), a LOW-NORMAL platelet count (150-250 x 10^9/L) and a history of night-time pain; with all three, sensitivity 100% and specificity 85%.
- Antinuclear antibody, rash and objective signs of arthritis did NOT discriminate - they occurred at similar rates in both groups.
Corticosteroid-induced osteonecrosis in children treated for ALL: age and steroid choice (Japanese CCLSG)
- 1,095 children across three consecutive protocols; osteonecrosis in 16, of whom 15 were symptomatic.
- Cumulative incidence 0.76% and 0.35% on prednisolone-only protocols, rising to 3.6% once dexamethasone partly replaced prednisolone (P less than 0.01).
- Within the dexamethasone-era protocol, age dominated: 0.42% under age 10 versus 15.6% at age 10 or over (P less than 0.0001); girls 6.7% versus boys 1.3%.
Bone density decline following symptomatic osteonecrosis in childhood ALL (prospective national cohort)
- 466 children aged 4-18 on a dexamethasone-based protocol; symptomatic osteonecrosis in 6.4%.
- Bone density at diagnosis did NOT differ between those who did and did not go on to develop osteonecrosis - a baseline DXA does not identify the at-risk child.
- Bone density declined more steeply after osteonecrosis was diagnosed, implicating restricted weight-bearing and architectural destruction rather than pre-existing low density.
Acute lymphoblastic leukaemia presenting as chronic recurrent multifocal osteomyelitis
- A child with months of fever, migratory joint swelling and limb pain was initially diagnosed as osteomyelitis/systemic JIA and then CRMO, with an initial normal bone marrow.
- Only later, with pancytopenia and hepatosplenomegaly, did repeat marrow confirm ALL.
- Reinforces vigilance for leukaemia in children with musculoskeletal symptoms, as a normal initial marrow does not exclude it.
The frequency of musculoskeletal-only presentation of childhood ALL, the resulting diagnostic delay and misdiagnosis (as CRMO/fracture/osteomyelitis), and the utility of FDG-PET come from the cited Ikawa series, and the example of ALL mimicking CRMO (with an initially normal marrow) from the cited Singh case. The three predictive factors distinguishing ALL from juvenile arthritis - the white-cell and low-normal platelet thresholds, night pain, and the finding that three-quarters had no circulating blasts - come from the cited Jones multicentre case-control study. The osteonecrosis figures by age and by steroid come from the cited Hyakuna series, and the 6.4% symptomatic rate with the bone-density findings from the cited den Hoed prospective cohort. The T1-versus-muscle marrow rule is taken from MRI Bone Marrow Signal. The red flags, the radiographic 'leukaemic lines' and the diagnosis by blood film/bone marrow are standard, well-established paediatric teaching. (See also Septic Arthritis of the Paediatric Hip, Chronic Recurrent Multifocal Osteomyelitis and Kocher Criteria.)