Levine-Edwards Classification of Hangman Fractures
- Calling a displaced injury "Type I" because the patient is neurologically intact. Most hangman fractures are neurologically intact (Levine & Edwards: only 4 of 52 had a deficit) — neurology does NOT determine the type. Translation, angulation and the disc/facet status do.
- Applying cervical traction to a Type IIA. The single highest-yield trap: a flexion-distraction Type IIA is over-distracted by traction and can be made neurologically worse. Severe angulation with minimal translation = remove the traction.
- Skipping MRI before non-operative care. A "Type I" with an occult C2-C3 disc disruption is a misclassified Type II that will fail a collar — image the disc and posterior ligaments first.
- Forgetting the rest of the cervical spine and the vertebral arteries. About 1 in 4 have a second cervical injury; foramen transversarium involvement and Type III injuries raise vertebral artery injury risk — add CTA/MRA.
- Over-trusting the halo in adults. High complication rates (pin-site, loosening, non-union, restricted chest expansion, especially over 60) — say you would counsel surgery for unstable types.
Background & the bilateral pars concept
A "hangman fracture" is a bilateral fracture of the pars interarticularis (or pedicle) of C2 with traumatic spondylolisthesis of C2 on C3. The name comes from judicial hanging, but the modern injury is typically a high-energy motor vehicle collision or axial-load diving injury rather than hyperextension-traction.
The Effendi classification (1981) grouped these injuries by morphology and mechanism; Levine and Edwards (1985) modified Effendi into the four-type, morphology-and-stability-based system used worldwide today. A fifth variant — Type IA (Coric) — was later added for the atypical, often comminuted, oblique/coronal pattern that does not behave like a Type I. The system matters because morphology predicts stability and dictates treatment: a stable Type I needs only an orthosis, an unstable Type II needs halo or surgery, and a flexion-distraction Type IIA is made worse by the very traction used for other cervical injuries.
A Type IIA hangman can look like a Type II on a single lateral film because the disc is still partially hinged, but applying cervical traction over-distracts the disrupted C2-C3 disc and can cause neurological injury. If angulation is severe but translation is minimal, the injury is flexion-distraction (Type IIA) — skip the traction and go straight to surgical fixation.
Examiners frequently ask "what did Levine and Edwards modify?", so know the Effendi classification (1981) it is built on:
- Effendi Type I — a fracture with no or minimal displacement (translation up to ~3 mm) and no angulation; the C2-C3 disc is normal. Stable.
- Effendi Type II — a displaced fracture (significant translation and/or angulation) with an abnormal C2-C3 disc; the body of C2 is displaced and angulated. Unstable.
- Effendi Type III — a displaced fracture plus C2-C3 facet (apophyseal) joint dislocation — the C2-C3 facets are subluxed/locked while the body fragment lies in flexion. Severely unstable.
What Levine and Edwards (1985) added — they kept the broad three-group framework but subdivided the displaced Effendi Type II into a translation-predominant Type II (hyperextension-axial load then flexion, disc disrupted) and a separate angulation-predominant Type IIA (flexion-distraction, minimal translation), the crucial addition because Type IIA is over-distracted by the traction used to reduce a Type II. They also tied each type to a specific mechanism and to a stability-based treatment rule — which is why the modern eponym is "Levine-Edwards" even though Effendi described the original groups.
The four Levine-Edwards types
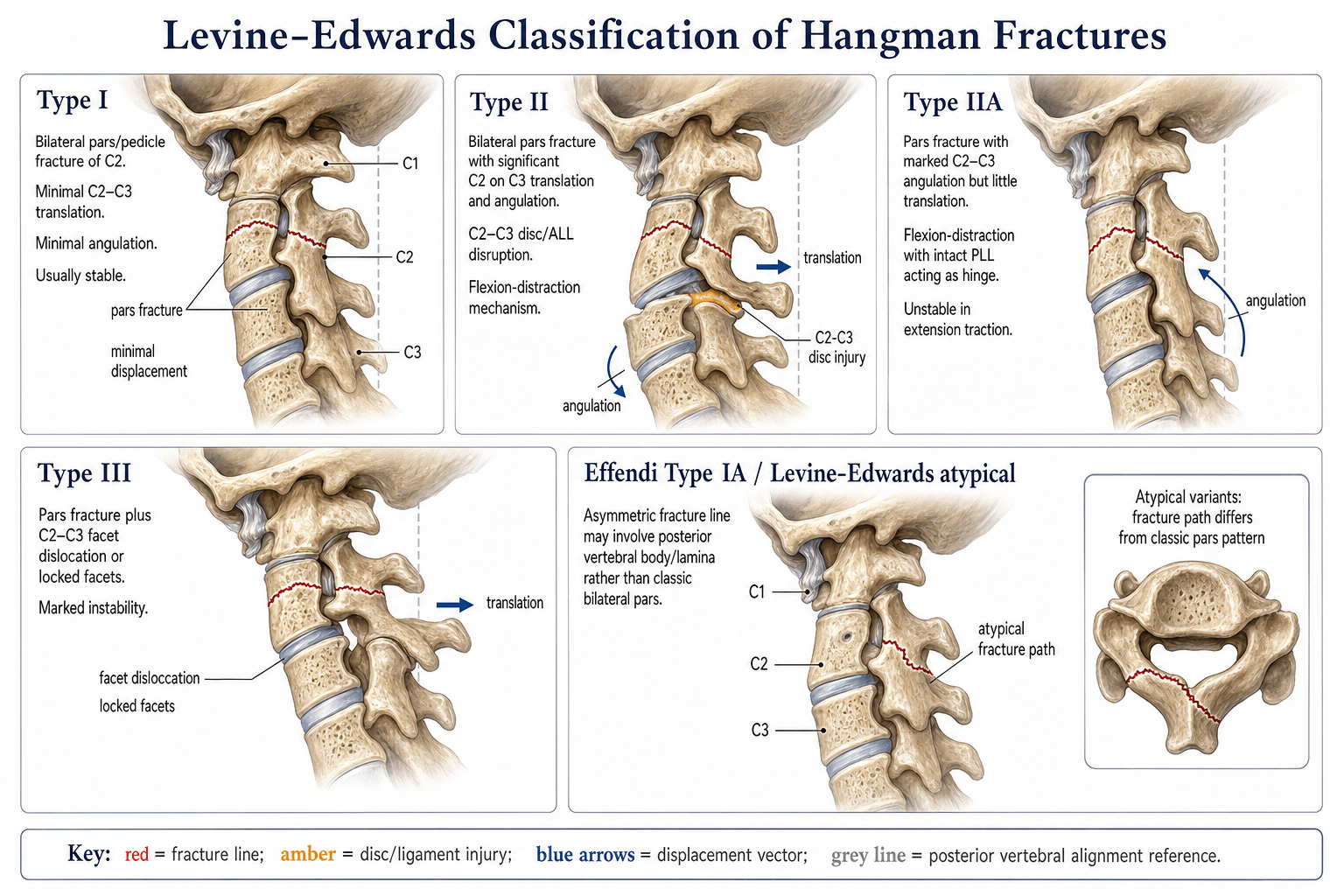


Each type is defined by the translation of C2 on C3, the angulation across C2-C3, and the integrity of the disc and facet complex (lateral plain film plus CT with sagittal reconstruction; MRI for the disc and posterior ligaments).
- Translation
- Less than 3 mm
- Angulation
- Minimal (under 10°)
- Disc & facet
- Disc intact, facets intact
- Stability / mechanism
- Stable; hyperextension-axial load
- Translation
- Often minimal
- Angulation
- Mild
- Disc & facet
- Comminuted pars, oblique/coronal fracture line
- Stability / mechanism
- Usually stable but distinct; lateral bending/asymmetric load
- Translation
- More than 3 mm
- Angulation
- More than 10°
- Disc & facet
- Disc disrupted, ALL/PLL often torn
- Stability / mechanism
- Unstable; hyperextension-axial load then severe flexion
- Translation
- Minimal (under 3 mm)
- Angulation
- Severe (over 10°)
- Disc & facet
- Disc and PLL disrupted, facets perched (PLL hinge)
- Stability / mechanism
- Highly unstable; FLEXION-DISTRACTION
- Translation
- Gross
- Angulation
- Severe
- Disc & facet
- Unilateral or bilateral C2-C3 facet dislocation
- Stability / mechanism
- Severely unstable; flexion-compression; high neuro risk
Angulation is measured at the C2-C3 disc (the angle between the inferior endplate of C2 and the superior endplate of C3), and translation is the anteroposterior step between the posterior cortices of C2 and C3 on a true lateral. Inconsistent measurement technique is a common source of disagreement between observers — use the same method every time.
I–II–IIA–IIIThe four types in order
Hook:As you move I → II → IIA → III, instability and surgical urgency both rise; IIA is the one where traction is forbidden.
Mechanism, imaging & pattern recognition
- Mechanism
- Hyperextension-axial load; rebound to neutral
- Key imaging clue
- Bilateral pars fracture, under 3 mm shift, facets aligned
- Pitfall
- Mistaking a comminuted IA pattern for a benign Type I
- Mechanism
- Lateral bending / asymmetric axial load, coronal fracture line
- Key imaging clue
- Coronal/oblique orientation, comminution of the posterior C2 body
- Pitfall
- Underestimating instability if treated as Type I
- Mechanism
- Hyperextension-axial load THEN severe flexion (rebound)
- Key imaging clue
- Over 3 mm slip and over 10° angulation, disc disrupted on MRI
- Pitfall
- Missing PLL/disc injury — MRI before conservative care
- Mechanism
- Flexion-distraction
- Key imaging clue
- Severe angulation, minimal translation, perched/hinged joints
- Pitfall
- Applying traction — it over-distracts
- Mechanism
- Flexion-compression with facet dislocation
- Key imaging clue
- Locked or perched C2-C3 facets, gross displacement
- Pitfall
- Attempting closed reduction without surgical backup
MRI is mandatory before deciding on non-operative treatment for a Type I and for any patient with a neurological deficit. The Levine-Edwards type is morphological; it does not capture disc disruption, posterior ligamentous injury, or cord signal change. A "Type I" with an unseen disc injury is a misclassified Type II and will fail conservative management.
A classic viva follow-up: "this C2 is grossly displaced — why is the patient walking and talking?" Only 4 of Levine and Edwards' 52 patients had a cord deficit, and the reason is anatomical, not luck:
- The bilateral pars fracture decompresses the canal. Because the fracture separates the posterior arch (laminae, spinous process) from the vertebral body bilaterally, when the body translates forward the posterior elements are left behind — so the injury effectively vents/widens the spinal canal at C2 rather than narrowing it. This auto-decompression spares the cord even with large translation.
- The upper cervical canal is capacious. The canal is widest at C1-C2 (Steel's "rule of thirds" — at this level roughly one-third cord, one-third dens, one-third free space), giving the cord substantial reserve.
- When a hangman fracture DOES injure the cord, suspect a Type III (a true facet dislocation narrows the canal) or an associated injury — which is why Type III carries the highest neurological risk and why the whole cervical spine and the vertebral arteries must be imaged.
The corollary for the exam: a neurological deficit in a "simple" hangman fracture is a red flag for a higher-grade pattern, a missed second injury, or a vascular injury — not a reason to over-call the fracture type itself.
Management by type
- 1Classify on CT + MRICT (sagittal recon) defines the fracture; MRI defines the C2-C3 disc and posterior ligaments. Measure translation and angulation consistently. Image the whole cervical spine.
- 2Type I → rigid orthosisPhiladelphia collar, Minerva or halo for 6–12 weeks — but only after MRI confirms the disc and PLL are intact (otherwise it is a Type II).
- 3Type II → halo or surgeryReduce (light traction, watching the disc space) then halo vest, OR surgical fixation. In adults, surgery (anterior C2-C3 discectomy and fusion, or posterior C2-C3 instrumentation) is increasingly chosen to avoid halo morbidity.
- 4Type IIA / III → surgeryIIA: surgical fixation, NO traction (over-distracts the disc). III: open reduction of the dislocated facets and fusion, often combined anterior-posterior; check the vertebral arteries.
- First-line
- Rigid cervical orthosis 6–12 weeks
- Operative indication
- Persistent pain, non-union, or re-displacement on serial imaging
- Critical caveat
- Confirm disc/PLL intact on MRI first
- First-line
- Rigid orthosis with close CT follow-up
- Operative indication
- Comminution, non-union, persistent instability
- Critical caveat
- Distinguish from Type I to set the right follow-up intensity
- First-line
- Halo vest (12 weeks) OR surgical fixation
- Operative indication
- Disc disruption, neuro deficit, severe displacement, or patient factors
- Critical caveat
- Halo is high-morbidity in adults — discuss surgery
- First-line
- Surgical fixation (anterior C2-C3 fusion or posterior C2-C3 instrumentation)
- Operative indication
- Non-operative care is rarely successful
- Critical caveat
- Traction is CONTRAINDICATED — over-distracts the disc
- First-line
- Open reduction and fusion (often combined anterior-posterior)
- Operative indication
- Conservative care is not appropriate
- Critical caveat
- Address the facet dislocation; check for vertebral artery injury
For an unstable hangman (Type II/IIA/III): anterior C2-C3 discectomy and fusion is the workhorse when the disc is disrupted (it treats the actual pathological segment); posterior C2-C3 instrumented fusion (C3 lateral mass screws + C2 pars/pedicle screws) is the alternative; and a direct pars (Judet) lag screw is elegant when both sides are reducible and the fragments will hold — but it does not address a disrupted disc, so most surgeons add anterior fusion or use a combined construct. The C2 pars/pedicle trajectory is unforgiving — pre-operative CT is mandatory to check the vertebral artery foramen and the medial wall.
Traction is acceptable for Type II, contraindicated for Type IIA, and rarely indicated for Type III. In a Type II, start with light weight (~2–3 kg), obtain a lateral film, and stop if the disc space opens — any further angulation or distraction means you are actually dealing with a Type IIA pattern.
Limitations & modern context
- The type is not the only decision driver — MRI findings (disc disruption, PLC injury, cord oedema) and patient factors (halo tolerance, body habitus, comorbidities) often push a "stable Type I" toward surgery.
- Halo vest complications are common in adults — pin-site infection, loosening, restricted chest expansion, non-union — especially over age 60; a Philadelphia collar or Minerva is often used, and many centres now prefer early surgical fixation in unstable types.
- The Type IA (Coric) variant is increasingly recognised as distinct and possibly less benign than originally thought — some centres follow it as effectively a Type II biologically.
- The classification is morphological, not mechanistic — two Type II injuries from different mechanisms can behave differently, which is why MRI supplements the type.
- Associated injuries are common — up to ~1 in 4 patients with a hangman fracture has another cervical injury (often C1 or lower cervical); always image the whole cervical spine.
- Vertebral artery injury is more likely with foramen transversarium involvement and with high-grade (Type III) injuries — consider CTA/MRA.
Viva practice
- I (under 3 mm, minimal angulation, disc intact → orthosis); II (over 3 mm + over 10°, disc disrupted → halo/surgery); IIA (severe angulation, minimal translation, flexion-distraction → surgery, NO traction); III (facet dislocation → open reduction + fusion).
- The Type IIA trap: traction over-distracts the disrupted disc — collar/extension and proceed to surgery.
- MRI before any non-operative decision — a "Type I" with a disc injury is a misclassified Type II.
- Image the whole cervical spine (~1 in 4 have a second injury); check the vertebral arteries in high-grade injuries.
- Operative options: anterior C2-C3 discectomy/fusion (disc disrupted), posterior C2-C3 instrumentation, or a direct pars (Judet) screw when reducible.
- Halo is high-morbidity in adults — many centres now fix unstable types surgically.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 34-year-old driver is brought in after a high-speed MVA. He is GCS 15, no neurological deficit, and a CT shows a bilateral pars fracture of C2 with 6 mm of anterior translation of C2 on C3 and about 15° of angulation. How do you classify and manage this?”
“A 27-year-old front-seat passenger is immobilised at the scene. Imaging shows severe angulation at C2-C3 with less than 2 mm of translation, perched C2-C3 facets, and a hyperintense C2-C3 disc on STIR MRI. The trauma team has set up cervical traction. What is your classification and what do you do?”
Exam cheat sheet
The four types (+ IA)
- Type I: under 3 mm translation, under 10° angulation, disc intact — stable, rigid orthosis
- Type IA (Coric): comminuted, oblique/coronal fracture line — distinct, potentially less benign
- Type II: over 3 mm and over 10°, disc disrupted — unstable, halo or surgery
- Type IIA: severe angulation, minimal translation, flexion-distraction — traction contraindicated, surgery
- Type III: facet dislocation — severely unstable, open reduction and fusion
Measurement & imaging rules
- Translation = AP step between the posterior cortices of C2 and C3 on a true lateral
- Angulation = angle between the inferior endplate of C2 and the superior endplate of C3
- CT (sagittal recon) defines the fracture; MRI defines the disc and posterior ligaments
- Image the whole cervical spine — about 1 in 4 have a second injury
- CTA/MRA if vertebral artery injury suspected (foramen involvement, Type III)
Management & traps
- Type I: rigid orthosis 6–12 weeks (confirm MRI quiet first)
- Type II: halo vest OR surgery (anterior C2-C3 fusion or posterior instrumentation)
- Type IIA: surgery; NO traction (over-distracts the disc)
- Type III: open reduction and fusion, often combined anterior-posterior
- MRI before non-operative care; halo is high-morbidity in adults
Evidence
The management of traumatic spondylolisthesis of the axis
- Series of 52 patients (15 Type I, 29 Type II, 3 Type IIa, 5 Type III) modifying the Effendi classification into the four-type Levine-Edwards system.
- Type I was stable and treated in a collar; Type II reduced in halo traction then halo vest; Type IIA showed INCREASED displacement in traction and was reduced by gentle extension/compression; Type III was grossly unstable and required surgery.
- Correlated each type with mechanism: I hyperextension-axial load; II hyperextension-axial load then severe flexion; IIa flexion-distraction; III flexion-compression.
Early halo immobilization of displaced traumatic spondylolisthesis of the axis
- Retrospective review of 27 Type II and 4 Type IIA hangman fractures treated with early halo immobilisation after traction reduction.
- 21 of 27 Type II fractures united with early halo; 6 required re-application of traction for displacement, and all 4 Type IIA fractures united.
- The discriminating factor for failure was the initial angulation — patients needing re-traction had an initial angulation of 12° or more.
A systematic review of the management of hangman's fractures
- Systematic review of the literature (1966–2004); the Effendi classification modified by Levine-Edwards was used most widely.
- Most hangman fractures — including Effendi I/II and Levine-Edwards Type II — were managed successfully with traction and external (often rigid) immobilisation.
- Levine-Edwards Type IIa and III needed rigid immobilisation, and surgical stabilisation was recommended for unstable IIa/III with significant dislocation.
Hangman's fracture: a clinical review based on surgical treatment of 15 cases
- Retrospective surgical series of 15 hangman fractures over 5 years.
- Proposed a novel classification grouping patients by the presence of atlantoaxial and/or C2-C3 instability, which guided the surgical strategy.
- All cases achieved solid bony fusion at a mean follow-up of 26 months, with only marginal restriction of neck movement.
According to PubMed, the classification and the Type-IIA-worsens-with-traction principle come from Levine & Edwards 1985 (PMID 3968113); the early-halo data and the 12°-angulation failure threshold from Vaccaro et al. 2002 (DOI 10.1097/00007632-200210150-00009); the systematic review favouring conservative care for most fractures and surgery for unstable IIa/III from Li et al. 2006 (DOI 10.1007/s00586-005-0918-2); and a modern surgical series with an instability-based classification from Goel et al. 2022 (DOI 10.1007/s10143-021-01556-8).