Structure | Composition | Biomechanics | Healing | Graft Incorporation
Hierarchical Organization
Critical Must-Knows
- Type I collagen (70-80% dry weight) in hierarchical organization provides tensile strength
- Enthesis has 4 zones: ligament → fibrocartilage → mineralized FC → bone (graded transition)
- Crimping pattern creates toe region of stress-strain curve (0-3% strain, low stiffness)
- Healing phases: inflammatory (0-7d), proliferative (7d-6wk), remodeling (6wk-24mo)
- ACL grafts never achieve full native strength - plateau at 50-70% after 12-24 months
- Intra-articular ligaments (ACL) heal poorly; extra-articular (MCL) heal better
Clinical Pearls
- "Insertion (enthesis) does not regenerate after surgical reconstruction
- "Midsubstance healing stronger than bone-ligament junction in first 8-12 weeks
- "Graft weakening phase occurs at 3-4 months during revascularization
- "Immobilization causes rapid strength loss; controlled motion promotes alignment
- "Bony avulsions heal better than midsubstance tears (preserve enthesis)
Clinical Imaging
Imaging Gallery

Critical Ligament Biology Exam Points
Type I Collagen Dominance
70-80% of ligament dry weight is Type I collagen providing tensile strength. Type III collagen increases during healing (up to 30%) but should decrease with remodeling. Elastin content less than 5% except in elastic ligaments (ligamentum flavum 70% elastin).
Crimping and Toe Region
Wavy crimping pattern (20-100 micrometers period) allows initial low-stiffness loading. Explains toe region of stress-strain curve (0-3% strain). As load increases, crimps straighten, then collagen fibers resist tension directly - linear region begins (3-8% strain).
Four-Zone Enthesis
Insertion has graded transition minimizing stress concentration. Zone 1: ligament (Type I collagen). Zone 2: fibrocartilage (Type II increases). Zone 3: mineralized fibrocartilage (tidemark). Zone 4: bone (Sharpey fibers). Does not regenerate after surgery.
Healing Never Complete
Healed ligaments reach only 50-70% native strength after 12-24 months. Scar tissue has disorganized collagen, increased Type III, reduced crimp, fewer cross-links. Explains persistent laxity risk after injuries. Graft weakening at 3-4 months is critical vulnerable period.
At a Glance
Ligaments derive tensile strength from Type I collagen (70-80% dry weight) organized in a hierarchical structure from tropocollagen through microfibrils, fibrils, and fascicles, with 60-80% water content providing viscoelastic properties. The characteristic wavy crimping pattern (20-100μm period) creates the toe region of the stress-strain curve, allowing initial low-stiffness loading at 0-3% strain before collagen fibers engage directly. The four-zone enthesis (ligament → fibrocartilage → mineralized fibrocartilage → bone) minimizes stress concentration at the bone-ligament interface but critically does not regenerate after surgical reconstruction. Ligament healing proceeds through inflammatory (0-7d), proliferative (7d-6wk), and remodeling phases (6wk-24mo), but healed tissue reaches only 50-70% native strength due to disorganized collagen and reduced cross-links. ACL grafts experience a vulnerable weakening phase at 3-4 months during revascularization—intra-articular ligaments heal poorly compared to extra-articular structures like the MCL.
COWPEGLigament Composition - COWPEG
| C | Collagen Type I (70-80% dry weight) - main structural protein providing tensile strength |
| O | Other proteins Proteoglycans, elastin, fibronectin, laminin - matrix organization |
| W | Water 60-80% total weight - provides viscoelasticity, nutrient transport |
| P | Proteoglycans Decorin, biglycan - organize collagen fibrils, resist compression |
| E | Elastin Less than 5% (except ligamentum flavum 70%) - allows recoil |
| G | Ground substance GAGs, hyaluronic acid - hydration, lubrication, spacing |
| C | Collagen Type I (70-80% dry weight) - main structural protein providing tensile strength | W | Water 60-80% total weight - provides viscoelasticity, nutrient transport | E | Elastin Less than 5% (except ligamentum flavum 70%) - allows recoil |
| O | Other proteins Proteoglycans, elastin, fibronectin, laminin - matrix organization | P | Proteoglycans Decorin, biglycan - organize collagen fibrils, resist compression | G | Ground substance GAGs, hyaluronic acid - hydration, lubrication, spacing |
Hook:COWPEG holds ligaments together - remember Collagen is king at 70-80%!
TMSFLHierarchical Organization - TMSFL
| T | Tropocollagen Triple helix - 3 alpha chains, 300nm long, 1.5nm diameter, basic unit |
| M | Microfibril 5 staggered tropocollagen molecules - 5nm diameter, 67nm banding |
| S | Subfibril Assembled microfibrils - 10-20nm diameter, cross-linking begins |
| F | Fibril Subfibril bundles - 50-500nm diameter, visible crimping pattern |
| L | Ligament Fascicles (fibril bundles) wrapped by endo/epiligament sheaths |
| T | Tropocollagen Triple helix - 3 alpha chains, 300nm long, 1.5nm diameter, basic unit | F | Fibril Subfibril bundles - 50-500nm diameter, visible crimping pattern |
| M | Microfibril 5 staggered tropocollagen molecules - 5nm diameter, 67nm banding | L | Ligament Fascicles (fibril bundles) wrapped by endo/epiligament sheaths |
| S | Subfibril Assembled microfibrils - 10-20nm diameter, cross-linking begins |
Hook:TMSFL - Tiny Molecules Stack to Form Ligaments from nano to macro!
IPRHealing Phases - IPR
| I | Inflammatory 0-7 days: Hematoma, neutrophils, macrophages, PDGF/TGF-β/VEGF release |
| P | Proliferative 7 days-6 weeks: Fibroblast proliferation, Type III collagen, neovascularization |
| R | Remodeling 6 weeks-12-24 months: Type I replacement, collagen alignment, cross-linking |
| I | Inflammatory 0-7 days: Hematoma, neutrophils, macrophages, PDGF/TGF-β/VEGF release |
| P | Proliferative 7 days-6 weeks: Fibroblast proliferation, Type III collagen, neovascularization |
| R | Remodeling 6 weeks-12-24 months: Type I replacement, collagen alignment, cross-linking |
Hook:IPR - Injury Provokes Repair but takes 12-24 months to complete!
LFMBFour Zones of Enthesis - LFMB
| L | Ligament Zone 1: Dense regular connective tissue, aligned Type I collagen fibers |
| F | Fibrocartilage Zone 2: Chondrocytes appear, Type II collagen increases, gradual transition |
| M | Mineralized FC Zone 3: Calcium phosphate deposition, tidemark visible, biomechanical gradient |
| B | Bone Zone 4: Subchondral and trabecular bone, Sharpey fibers anchor ligament |
| L | Ligament Zone 1: Dense regular connective tissue, aligned Type I collagen fibers | M | Mineralized FC Zone 3: Calcium phosphate deposition, tidemark visible, biomechanical gradient |
| F | Fibrocartilage Zone 2: Chondrocytes appear, Type II collagen increases, gradual transition | B | Bone Zone 4: Subchondral and trabecular bone, Sharpey fibers anchor ligament |
Hook:LFMB - Ligament Fades into Mineralized Bone through graded zones!
Overview and Fundamental Concepts
Ligaments are dense connective tissue structures that connect bone to bone, providing joint stability while permitting controlled physiological motion. Their unique hierarchical organization - from nanometer-scale tropocollagen molecules to centimeter-scale anatomical structures - provides exceptional tensile strength along the fiber axis while maintaining sufficient flexibility for joint movement.
Understanding ligament biology is fundamental for interpreting injury patterns, predicting healing capacity, optimizing surgical reconstruction techniques, and designing evidence-based rehabilitation protocols. The composition, biomechanical properties, and healing characteristics of ligaments directly influence clinical decision-making across all orthopaedic subspecialties.
Definition and Function
Ligaments are specialized collagenous bands that:
- Connect bone to bone (differ from tendons which connect muscle to bone)
- Provide passive mechanical restraint to joint motion
- Guide joint kinematics through arc of motion
- Contain mechanoreceptors providing proprioceptive feedback
- Exhibit viscoelastic behavior (rate-dependent mechanical properties)
Functional classification:
- Capsular ligaments: Thickenings of joint capsule (e.g., glenohumeral ligaments)
- Extracapsular ligaments: Distinct structures outside joint (e.g., MCL of knee)
- Intracapsular ligaments: Within joint but extrasynovial (e.g., ACL, PCL)
- Elastic ligaments: High elastin content allowing stretch (e.g., ligamentum flavum)
Clinical Significance of Ligament Biology
Ligament structure explains clinical observations: midsubstance tears heal poorly (dense, relatively avascular tissue), bony avulsions heal well (preserved enthesis, cancellous bone vascularity), ACL grafts require 12-24 months to remodel (slow biological ligamentization), and postoperative rehabilitation must protect healing during proliferative phase while providing controlled stress to promote collagen alignment during remodeling phase.
Concepts: Composition and Structure
Extracellular Matrix Components
Ligaments are composed of cells embedded within an abundant extracellular matrix. Understanding composition is essential for interpreting healing responses and graft behavior.
| Component | Percentage | Function | Clinical Note |
|---|---|---|---|
| Water | 60-80% total weight | Viscoelasticity, nutrient transport | Dehydration reduces stiffness |
| Type I collagen | 70-80% dry weight | Tensile strength, structural framework | Decreased in healing tissue |
| Type III collagen | Under 10% normal | Compliance, early healing | Increases to 30% in scar then decreases |
| Proteoglycans | 1-3% dry weight | Collagen organization, compression resistance | Decorin, biglycan regulate fibrillogenesis |
| Elastin | 1-5% (70% in LF) | Elastic recoil | Ligamentum flavum has unique high content |
| Other proteins | Under 5% | Cell adhesion, matrix organization | Fibronectin, laminin, fibrillin |
Type I Collagen:
- Triple helix of two alpha-1 chains and one alpha-2 chain
- Provides high tensile strength (weak in compression)
- Organized in hierarchical bundles with crimping pattern
- Cross-linked by lysyl oxidase creating pyridinoline links
- Synthesized by fibroblasts in response to mechanical loading
Type III Collagen:
- Present in small amounts in normal ligaments (under 10%)
- Increases significantly during healing (up to 30% at 6-8 weeks)
- More compliant, smaller diameter fibrils than Type I
- Should decrease during remodeling phase (incomplete in scar tissue)
- Persistent elevation indicates incomplete maturation
Proteoglycans:
- Small leucine-rich proteoglycans (SLRPs): decorin, biglycan
- Regulate collagen fibril diameter and spacing
- Resist compressive forces through osmotic swelling
- Increased in healing ligaments
- Age-related decrease may contribute to injury susceptibility
Cellular Components
Fibroblasts - Primary Cell Type
90-95% of ligament cells are fibroblasts:
- Synthesize collagen (Types I and III) and matrix proteins
- Respond to mechanical loading via mechanotransduction
- Aligned along primary stress lines in mature ligaments
- Increased cellularity during healing (peak at 2-3 weeks)
- Express receptors for growth factors (TGF-β, PDGF, IGF-1)
Other Cell Populations
Specialized cells (5-10%):
- Chondrocytes at fibrocartilaginous insertions (enthesis)
- Synovial cells in intra-articular ligaments (ACL, PCL)
- Vascular endothelial cells in epiligament and midsubstance
- Nerve endings and mechanoreceptors (proprioception)
- Mast cells and inflammatory cells (injury response)
Hierarchical Structure
Ligaments exhibit hierarchical organization spanning seven orders of magnitude (nanometers to centimeters), optimizing mechanical performance while allowing biological remodeling.
Level 1: Tropocollagen Molecule (1-10nm)
- Triple helix: 3 alpha chains in right-handed superhelix
- Dimensions: 300nm length, 1.5nm diameter
- Left-handed polyproline helix of each alpha chain
- Glycine at every third position allows tight packing
- Synthesized intracellularly, secreted as procollagen
Level 2: Microfibril (5-20nm)
- 5 tropocollagen molecules in staggered quarter-stagger arrangement
- Creates characteristic 67nm D-period banding pattern
- Gap and overlap regions visible on electron microscopy
- Initial enzymatic cross-linking occurs at this level
- Basic unit of fibril assembly
Level 3: Subfibril (10-20nm)
- Assembled microfibrils with increasing cross-links
- Diameter varies with collagen type and tissue
- Lateral fusion creates larger diameter structures
- Cross-linking density increases with maturation
Level 4: Fibril (50-500nm)
- Bundles of subfibrils visible on light microscopy
- Wavy crimping pattern (20-100 micrometer period)
- Diameter correlates with mechanical properties
- Cross-linking provides tensile strength
- Crimping allows initial low-stiffness loading
Level 5: Fascicle (50-300 micrometers)
- Bundles of fibrils wrapped by endoligament sheath
- Functional unit of ligament mechanics
- Contains blood vessels and nerves
- Allows gliding between fascicles
Level 6: Ligament (millimeter to centimeter)
- Multiple fascicles wrapped by epiligament
- Gross anatomical structure
- Vascular supply in epiligament and endoligament
- Mechanoreceptors provide proprioceptive feedback
Crimping Pattern - Biomechanical Significance
The crimping pattern (wavy appearance at rest with 20-100 micrometer period) is critical for ligament function. During initial loading, crimps straighten without stretching collagen molecules - this creates the toe region of the stress-strain curve (0-3% strain) with low stiffness allowing joint motion without high forces. Once crimps fully extend, the linear region begins (3-8% strain) where collagen fibers resist tension directly with high stiffness (elastic modulus 100-400 MPa). Loss of crimping in healing tissue explains reduced compliance.
Cross-Linking
Enzymatic cross-links:
- Lysyl oxidase converts lysine and hydroxylysine to reactive aldehydes
- Mature cross-links: Pyridinoline (PYD) and deoxypyridinoline (DPD)
- Provide mechanical stability and tensile strength
- Increase with age and tissue maturation
- Reduced in healing tissue (explains lower strength)
- Cannot reform once disrupted in injury
Non-enzymatic cross-links:
- Advanced glycation end-products (AGEs) increase with age
- Contribute to age-related stiffening and embrittlement
- Accelerated in diabetes (may predispose to injury)
Enthesis: The Ligament-Bone Interface
The insertion zone (enthesis) is a specialized transitional structure that minimizes stress concentration at the interface between compliant ligament and stiff bone. This graded transition occurs over less than 1mm distance.
Four-Zone Structure:
Zone 1 - Ligament:
- Dense regular connective tissue
- Aligned Type I collagen fibers parallel to loading direction
- High fibroblast density
- Continuous with ligament midsubstance
Zone 2 - Fibrocartilage (Uncalcified):
- Gradual transition zone
- Chondrocytes within lacunae appear
- Type II collagen increases alongside Type I
- Increased proteoglycan content
- Resists compressive forces from oblique loading
Zone 3 - Mineralized Fibrocartilage:
- Calcium phosphate deposition (hydroxyapatite crystals)
- Tidemark visible on histology (basophilic line)
- Sharp biomechanical gradient in elastic modulus
- Type X collagen present (marker of mineralization)
- Anchors collagen fibers to bone
Zone 4 - Bone:
- Subchondral and trabecular bone
- Sharpey fibers: Collagen fibers penetrating bone
- Provides mechanical anchorage
- Vascular supply for enthesis nutrition
Clinical Implications of Enthesis Structure
The enthesis does not regenerate after surgical reconstruction. Bone tunnel healing creates fibrovascular scar tissue, not the native four-zone enthesis. This explains why ligament-to-bone healing is the weakest link in ACL reconstruction during first 8-12 weeks. Bony avulsion fractures preserve the enthesis - they heal better than midsubstance tears because the biological insertion remains intact.
Mechanical Function of Enthesis:
- Gradual increase in elastic modulus from ligament (100-400 MPa) to bone (10-20 GPa)
- Factor of 50-100 difference occurs over less than 1mm
- Prevents stress concentration that would cause interface failure
- Fibrocartilage zones resist shear and compressive stresses
Clinical failure patterns:
- Young patients: Bony avulsion (bone weaker than enthesis)
- Adults: Midsubstance tear (age-related collagen weakening)
- Elderly: Enthesis failure may occur with degeneration
Mechanical Properties and Biomechanics
Ligaments exhibit characteristic non-linear stress-strain curves reflecting their hierarchical structure and crimping pattern.
Four Regions of the Curve:
1. Toe Region (0-3% strain):
- Low stiffness, non-linear behavior
- Crimps straightening without collagen stretching
- Physiological loading range for normal activities
- Allows joint motion without generating high resistance
- Protects against impact loading
2. Linear Region (3-8% strain):
- High stiffness, linear elastic behavior
- Crimps fully extended, collagen fibers bearing load
- Elastic modulus: 100-400 MPa depending on ligament
- Reversible deformation if load removed before yield point
- Most ligament function occurs in transition from toe to linear
3. Yield Point and Plastic Deformation (4-8% strain):
- Microstructural damage begins (interfibrillar sliding)
- Permanent deformation occurs (crimp pattern disrupted)
- Clinical "sprain" - subfailure injury
- Partial recovery possible but reduced mechanical properties
- May progress to complete failure if loading continues
4. Failure Region (greater than 8% strain):
- Macroscopic fiber failure
- Complete ligament rupture
- Ultimate tensile stress: 20-100 MPa depending on ligament
- Mode of failure: Midsubstance (adults), avulsion (children/elderly), enthesis (degeneration)
| Ligament | Failure Load (N) | Stiffness (N/mm) | Ultimate Stress (MPa) | Clinical Note |
|---|---|---|---|---|
| ACL | 2160 (young) | 242 | 38 | Weakest at age 50-60 years, drops to 658N |
| PCL | 2000 | 295 | 28 | Thicker cross-section than ACL |
| MCL | 3000 | 140 | 39 | Broad insertion distributes load |
| LCL | 1500 | 160 | 45 | More prone to bony avulsion |
| Patellar tendon | 2900 | 660 | 63 | Common ACL graft - high strength |
Viscoelastic Behavior
Ligaments are viscoelastic materials - their mechanical response depends on rate and duration of loading, not just magnitude.
Key Viscoelastic Phenomena:
Creep:
- Increasing deformation under constant load over time
- Explains joint laxity increase during prolonged static positioning
- Clinical relevance: Surgical positioning (joint opens with retraction)
- Recovers partially with rest (time-dependent)
Stress Relaxation:
- Decreasing stress under constant deformation over time
- Initial high stress gradually decreases at fixed elongation
- Mechanism: Fluid exudation and fiber reorientation
- Clinical relevance: Graft tensioning during ACL reconstruction
Hysteresis:
- Energy dissipation during loading-unloading cycles
- Loading and unloading curves do not overlap
- Represents energy absorbed (protective mechanism)
- Reduces with repetitive cycling (preconditioning)
Strain Rate Sensitivity:
- Faster loading produces higher apparent stiffness
- Slower loading allows more viscoelastic deformation
- Clinical relevance: Dynamic vs static testing, injury mechanism
- High-energy injuries may produce different patterns than low-energy
Clinical Application of Viscoelasticity
Warm-up reduces injury risk by preconditioning ligaments through repetitive low-load cycling, which reduces hysteresis and optimizes viscoelastic response. Cyclic loading during rehabilitation promotes optimal collagen fiber alignment along stress lines (mechanotransduction). Creep during surgery explains why joint distraction increases over time with constant retractor force.
Factors Affecting Mechanical Properties
Age:
- Strength peaks at 30-40 years
- Significant decline after 50 years (collagen cross-link changes)
- ACL failure load decreases from 2160N (age 22-35) to 658N (age 60-97)
- Increased stiffness but reduced ultimate strength with aging
Sex:
- Females have 10-15% lower tensile strength (hormonal influences)
- Increased ACL injury risk in females (neuromuscular factors also contribute)
- Menstrual cycle phase may affect collagen synthesis
Physical Conditioning:
- Exercise increases collagen synthesis and cross-sectional area
- Training increases failure load by 10-20%
- Immobilization rapidly decreases strength (50% reduction by 8 weeks)
Skeletal Maturity:
- Pediatric: Bone weaker than ligament (avulsion fractures common)
- Adult: Ligament weaker than bone (midsubstance tears)
- Elderly: Enthesis and bone may fail (osteoporosis)
Differential Diagnosis: Distinguishing Ligament Failure Patterns
When a ligamentous injury is suspected, the biological principles above explain why the failure pattern differs by age and loading - and which entities mimic a midsubstance tear.
| Entity | Typical patient / mechanism | Site of failure | Healing / management implication |
|---|---|---|---|
| Midsubstance ligament tear | Adult, tensile overload | Within ligament substance | Intra-articular (ACL) heals poorly; extra-articular (MCL) heals by scar |
| Bony avulsion fracture | Child/adolescent or elderly | Bone at the enthesis (enthesis preserved) | Heals well by bone healing; fix if displaced - near-normal strength |
| Enthesopathy / insertional degeneration | Older, chronic overload | Enthesis fibrocartilage (degenerative, not inflammatory) | Load management; degenerative process, limited self-repair |
| Enthesitis (spondyloarthropathy) | Younger, inflammatory, often HLA-B27 | Inflamed enthesis / synovio-entheseal complex | Rheumatological - DMARD/biologic therapy, not surgical |
| Ligamentous laxity / collagen disorder | Generalised hypermobility (e.g. Ehlers-Danlos) | Abnormal collagen / cross-linking diffusely | Higher recurrent instability and graft-stretch risk |
Clinical Relevance: Healing and Reconstruction
Ligament Healing and Remodeling
Three Phases of Healing
Ligament healing follows a predictable sequence but is prolonged and incomplete. Unlike bone, ligaments do not return to native structure or full strength.
Immediate response:
- Hematoma formation at injury site
- Platelet activation and degranulation
- Neutrophil infiltration (peak 24-48 hours)
- Macrophage recruitment (peak 48-96 hours)
Growth factor release:
- Platelet-derived growth factor (PDGF) - fibroblast chemotaxis
- Transforming growth factor-beta (TGF-β) - collagen synthesis
- Vascular endothelial growth factor (VEGF) - angiogenesis
- Interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α)
Tissue changes:
- Debridement of necrotic tissue by macrophages
- Granulation tissue formation begins
- Fibrin clot provides initial scaffold
- Mechanical strength very low (less than 10% normal)
Cellular response:
- Fibroblast proliferation and migration into injury site
- Cellularity peaks at 2-3 weeks (then gradually decreases)
- Myofibroblasts appear (wound contraction)
Matrix deposition:
- Abundant Type III collagen synthesis (disorganized)
- Type III may reach 30% of collagen (vs under 10% normal)
- Proteoglycan content increased
- Neovascularization from epiligament and bone
Mechanical properties:
- Strength gradually increases but remains low
- 10-30% of native strength by 6 weeks
- Stiffness much lower than normal
- Vulnerable to re-injury if overstressed
Matrix maturation:
- Type III collagen gradually replaced by Type I
- Collagen fibers align along stress lines (mechanotransduction)
- Cross-linking increases (pyridinoline and deoxypyridinoline)
- Cellularity decreases toward normal levels
- Vascularity decreases
Mechanical recovery:
- Strength increases progressively (asymptotic curve)
- Plateaus at 50-70% of native tissue strength
- Stiffness increases but remains below normal
- Crimp pattern partially restored but irregular
Incomplete restoration:
- Collagen organization remains suboptimal (more random)
- Type III persists at higher levels than normal
- Cross-link density lower than native tissue
- Explains persistent laxity risk and re-injury susceptibility
Intra-Articular vs Extra-Articular Healing
Intra-articular ligaments (ACL, PCL) heal poorly due to synovial fluid environment:
- Synovial fluid dilutes hematoma and washes away fibrin clot
- Growth factors dispersed rather than concentrated at injury
- Synoviocytes release proteases that degrade matrix
- Mechanical stability inadequate to maintain apposition
Extra-articular ligaments (MCL, LCL) heal more reliably:
- Stable hematoma formation
- Preserved local growth factor milieu
- Less mechanical disruption
- Explains why MCL grade 1-2 injuries managed conservatively while ACL tears require reconstruction
ACL Graft Remodeling (Ligamentization)
Understanding the biological incorporation process is essential for postoperative rehabilitation planning and patient counseling.
Phase 1: Early Incorporation (0-8 weeks)
- Graft is initially avascular and acellular (especially allograft)
- Autograft hamstring/patellar tendon undergoes central necrosis
- Bone tunnel healing is the weakest link during this phase
- Fibrovascular interface forms (not native enthesis)
- Initial graft strength high but decreases with remodeling onset
- Avoid aggressive loading - protect bone-graft interface
Phase 2: Revascularization (8-12 weeks)
- Blood vessels grow from synovium and bone tunnels into graft
- Hypercellular synovial response (synovial cells migrate into graft)
- Inflammatory cell infiltration
- Graft weakening phase - mechanical properties transiently decrease
- Paradoxical vulnerability despite clinical appearance of recovery
Phase 3: Cellular Remodeling (3-12 months)
- Fibroblasts replace synovial cells
- Collagen turnover - old fibers degraded, new fibers synthesized
- Gradual realignment of collagen along stress lines
- Type I collagen proportion increases
- Cellularity decreases toward normal ligament levels
- Strength increases but remains below native ACL
Phase 4: Maturation (12-24 months)
- Histological appearance approaches native ligament
- Collagen crimp pattern partially restored
- Cross-linking increases
- Strength plateaus at 50-70% of intact ACL
- Neuromuscular recovery may be limiting factor for function
- Return to full pivoting sports: 9-12 months minimum
Bone Tunnel Healing:
- Initial fibrovascular scar (not four-zone enthesis)
- Sharpey-like fibers develop by 8-12 weeks
- Provides mechanical anchorage but weaker than native
- Tunnel widening common (biological remodeling response)
- Interference screw provides stability during early healing
- Suspensory fixation relies on graft-fixation strength
Autograft vs Allograft Remodeling
Autograft (hamstring, patellar tendon): Starts with viable cells peripherally but central necrosis. Earlier revascularization (8-10 weeks). Allograft: Completely acellular initially. Slower host cell repopulation (10-14 weeks). Fresh-frozen allografts incorporate faster than irradiated/processed grafts. Both plateau at similar final strength (50-70% native ACL) but autograft may reach plateau faster by 3-6 months. Clinical outcomes similar but autograft preferred in young, active patients.
Graft Biology and Surgical Considerations
Autograft Options
| Graft Type | Advantages | Disadvantages | Remodeling Timeline |
|---|---|---|---|
| Bone-Patellar Tendon-Bone | High strength (2900N), bone-bone healing (8-12wk), rigid fixation | Anterior knee pain (20-30%), patellar fracture risk, kneeling discomfort | Faster bone healing, plateau 12-18mo |
| Hamstring (4-strand) | Low donor morbidity, high strength (4000N), larger diameter | Slower bone-tendon healing, fixation challenges, hamstring weakness | Slower integration, plateau 18-24mo |
| Quadriceps Tendon | Large, strong graft, minimal morbidity, partial bone block option | Less studied, potential extensor lag if overharvested | Similar to patellar tendon, 12-18mo |
Allograft Considerations
Advantages:
- No donor site morbidity
- Shorter operative time
- Larger graft availability (multi-ligament reconstruction)
- Less postoperative pain
Disadvantages:
- Disease transmission risk (screened but not zero)
- Slower revascularization and incorporation
- Processing (irradiation, chemical) may weaken graft
- Higher failure rate in young, active patients (under 25 years)
- Immune response (low grade, does not cause rejection but slows healing)
Processing methods affect biology:
- Fresh-frozen: Minimal processing, fastest incorporation, standard choice
- Irradiated (greater than 2.5 Mrad): Weakens collagen, slower incorporation
- Chemically processed (proprietary): Variable effects on strength and biology
Synthetic Grafts
Permanent synthetic ligaments:
- Historical poor outcomes (wear debris, synovitis, failure)
- Lack biological integration
- Stress shielding prevents graft remodeling
- Generally abandoned except specialized cases
Synthetic scaffolds (investigational):
- Provide temporary mechanical support during healing
- Designed to degrade as native tissue regenerates
- Promote cell infiltration and matrix deposition
- Clinical efficacy not yet proven
Growth Factors and Biological Augmentation
Growth factors in ligament healing:
- PDGF: Fibroblast chemotaxis and proliferation
- TGF-β: Collagen synthesis, matrix production
- VEGF: Angiogenesis, vascular invasion
- IGF-1: Cell proliferation, matrix synthesis
- BMP-12/13: Tendon/ligament differentiation
Clinical applications (investigational):
- Platelet-rich plasma (PRP): Variable evidence, not standard of care
- Stem cell augmentation: Early research, not proven effective
- Growth factor injections: Risk of ectopic ossification with BMPs
Mechanical augmentation:
- Suture tape augmentation of ACL reconstruction
- Provides temporary mechanical support during graft remodeling
- May reduce early graft elongation
- Does not replace need for adequate graft and fixation
Evidence Base
Human Patellar Tendon Autograft Ligamentization (Landmark Biopsy Study)
- 23 patients biopsied 3 weeks to 6.5 years post-reconstruction - patellar tendon autograft is viable as early as 3 weeks (may not pass through a frankly necrotic stage)
- Stage of rapid remodelling over the first year: fibroblast count and neovascularity rise while the proportion of mature collagen falls (correlates with the graft weakening phase)
- Maturation stage over the subsequent 2 years with declining cellularity and maturing collagen matrix
- By 3 years grafts were ligamentous by all histological criteria, but full ligamentization takes as long as 3 years
Age-Related Changes in ACL Mechanical Properties (Landmark Cadaveric Study)
- 27 paired cadaver knees in three age bands - younger (22-35), middle (40-50) and older (60-97 years)
- Femur-ACL-tibia complex ultimate load and linear stiffness fell significantly with specimen age
- Younger specimens (anatomical orientation): linear stiffness 242 plus or minus 28 N/mm and ultimate load 2160 plus or minus 157 N - higher than previously reported baselines
- Structural properties were higher in the anatomical than tibial loading orientation, informing graft selection targets
MCL Heals by Scar Formation - Never Reaches Normal (Landmark Study)
- Complete midsubstance MCL gaps in a rabbit model heal by distinct bridging scar over time, not by true ligament regeneration
- Gap bridging is rapid, but subtle changes in the healing tissue continue for many months
- The ligament scar remains structurally, chemically and mechanically abnormal even at long-term follow-up
- Improvement plateaus, suggesting the scar may never approach normal ligament characteristics without treatment
Enthesis Structure-Function and Stress Dissipation (Landmark Review)
- Fibrocartilaginous entheses are sites of stress concentration where the graded soft-to-hard tissue transition dissipates load and limits fibre bending at the bone interface
- Enthesis fibrocartilage is normally avascular and adapts to mechanical load; the surrounding 'enthesis organ' (fat pad, bursa, adjacent bone) jointly dissipates stress
- Most insertional enthesopathies in sport are degenerative rather than inflammatory
- Entheses have limited intrinsic capacity for self-repair, relevant to surgical reattachment
Ligamentization of the Human ACL Graft (Systematic Review)
- Systematic review of human graft biopsy studies - a free tendon graft replacing the ruptured ACL undergoes a biological process termed 'ligamentization'
- The graft remains viable throughout; mature grafts may histologically resemble native ACL
- Ultrastructural differences in collagen fibril diameter distribution persist - the graft never fully replicates native ACL architecture
- No consensus exists on the precise time frame of the ligamentization stages in humans
Graft Choice in Revision ACL Reconstruction (MARS Cohort)
- Prospective multicentre cohort of 1205 revision ACL reconstructions (48% autograft, 49% allograft) followed to 2 years
- Autograft predicted superior 2-year IKDC and KOOS sport and quality-of-life subscale scores
- Graft rerupture occurred in 37 of 1112 patients (3.3%): autograft revision was 2.78 times less likely to rerupture than allograft (95% CI 1.01-7.69)
- No difference in rerupture between soft-tissue and bone-patellar tendon-bone grafts
Population Incidence of ACL Tears and Reconstruction (21-Year Study)
- Population-based study of 1841 new isolated ACL tears (1990-2010) - overall age- and sex-adjusted incidence 68.6 per 100,000 person-years
- Higher in males than females (81.7 versus 55.3 per 100,000)
- Peak incidence at 19-25 years in males (241.0 per 100,000) and at 14-18 years in females (227.6 per 100,000)
- Rate of ACL reconstruction increased significantly over time across all age groups
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Ligament Structure and Stress-Strain Curve
"Examiner presents a stress-strain curve for a ligament and asks: Explain the four regions of this curve and how they relate to the hierarchical structure of ligaments."
Scenario 2: ACL Graft Remodeling and Return to Sport
"A 22-year-old professional footballer had ACL reconstruction with hamstring autograft 4 months ago. He has regained full range of motion and muscle strength, and wants to know when he can return to competitive football. Explain the biological basis for the timeline you recommend."
Scenario 3: MCL vs ACL Healing and Treatment Decisions
"Examiner asks: Why do we typically manage isolated MCL injuries conservatively while ACL tears require surgical reconstruction? Explain the biological basis for this difference in treatment approach."
Scenario 4: Enthesis Structure and Clinical Implications
"Examiner shows a diagram of the ligament-bone insertion and asks: Describe the structure of the enthesis and explain why bony avulsion fractures heal better than midsubstance ligament tears."
MCQ Practice Points
Composition Question
Q: What percentage of ligament dry weight is Type I collagen?
A: 70-80%. Type I collagen provides tensile strength and is the predominant structural protein. Type III collagen is present in smaller amounts (under 10% in normal ligaments) and increases during healing (up to 30%) but should decrease with remodeling. Persistent Type III elevation indicates incomplete maturation of scar tissue.
Enthesis Question
Q: What are the four zones of the fibrocartilaginous enthesis from ligament to bone?
A: Ligament → Fibrocartilage → Mineralized Fibrocartilage → Bone (remember LFMB). This graded transition minimizes stress concentration at the insertion site. Zone 2 (fibrocartilage) resists compressive forces, Zone 3 (mineralized FC) provides biomechanical gradient, and Zone 4 (bone) anchors via Sharpey fibers.
Healing Strength Question
Q: What percentage of native ligament strength do healed ligaments typically achieve after complete remodeling?
A: 50-70% even after 12-24 months of remodeling. Scar tissue has disorganized collagen, increased Type III collagen, reduced crimp pattern, and fewer mature cross-links compared to native tissue. This incomplete restoration explains persistent laxity risk after ligament injuries and why grafts never achieve 100% native strength.
ACL vs MCL Healing Question
Q: Why does the MCL heal more reliably than the ACL after injury?
A: MCL is extra-articular - stable hematoma forms, growth factors concentrate at injury site, mechanical apposition can be maintained with bracing. ACL is intra-articular - synovial fluid dilutes hematoma, washes away growth factors, synoviocytes release proteases that degrade matrix, mechanical instability prevents apposition. This biological difference explains conservative MCL treatment versus surgical ACL reconstruction.
Stress-Strain Curve Question
Q: What causes the toe region of the ligament stress-strain curve?
A: Straightening of crimped collagen fibrils without stretching the collagen molecules themselves. The crimping pattern (wavy appearance with 20-100 micrometer period) allows initial loading at low stiffness (0-3% strain). Once crimps fully extend, the linear region begins (3-8% strain) where collagen fibers resist tension directly with high elastic modulus (100-400 MPa).
Graft Remodeling Question
Q: When does the graft weakening phase occur after ACL reconstruction?
A: 3-4 months post-reconstruction during the revascularization phase. As blood vessels grow into the graft from synovium and bone tunnels, there is hypercellular response and active collagen turnover. Mechanical properties transiently decrease during this phase despite clinical appearance of recovery. This is a critical vulnerable period requiring continued activity restrictions.
Guidelines, Registries & Global Practice
Global Epidemiology
Ligament injury - dominated clinically by ACL rupture - is a worldwide burden, and the figures below are population- or registry-derived rather than estimates.
| Metric | Figure | Population / Source |
|---|---|---|
| Isolated ACL tear incidence | 68.6 per 100,000 person-years | US population-based, Sanders 2016 (PMID 26920430) |
| Male vs female incidence | 81.7 vs 55.3 per 100,000 | Same cohort (PMID 26920430) |
| Peak age - males | 19-25 yrs (241.0 per 100,000) | Same cohort (PMID 26920430) |
| Peak age - females | 14-18 yrs (227.6 per 100,000) | Same cohort (PMID 26920430) |
| Australian ACLR volume | 160,353 over 2001-2020; up 82% (peak 10,011 in 2017) | Campbell 2024, privately-insured cohort (PMID 39135546) |
| Australian ACLR sex split | 64% male / 36% female | Same cohort (PMID 39135546) |
The female adolescent peak (14-18 yrs) and the rising surgical rate across all ages are consistent international findings, underpinning sex-specific neuromuscular prevention programmes and service planning.
Guideline & Registry Positions (Side-by-Side)
| Body / Registry | Position relevant to ligament biology & ACLR | Evidence basis |
|---|---|---|
| AAOS (USA) | Autograft favoured over allograft in young/active patients to reduce re-rupture; emphasises function- and time-based return to sport | Clinical practice guideline + cohort data |
| NICE / BOA (UK) | ACL reconstruction reserved for symptomatic instability or failed rehabilitation; structured rehabilitation first-line for many tears | Guideline / consensus (Level 1-2) |
| ESSKA / EFORT (Europe) | Graft remains ultrastructurally distinct after ligamentization; protect graft through maturation; individualise graft choice | Systematic review evidence, Claes 2011 (PMID 21515806) |
| MARS Group (revision registry) | Autograft 2.78x less re-rupture than allograft at revision; soft-tissue and BPTB equivalent | Prospective cohort, Level 2 (PMID 25274353) |
| National registries (e.g. Scandinavian, AOANJRR-linked data) | Track graft type, re-revision and patient-reported outcomes to monitor practice variation | Registry data |
Practice Variation
- Graft choice varies by region: hamstring autograft predominates in much of Europe and Australasia, while bone-patellar tendon-bone retains strong support in North America; allograft use is higher in older or revision populations and lower in young athletes owing to re-rupture risk.
- Operative vs non-operative thresholds differ: UK and Scandinavian practice apply a rehabilitation-first pathway for many ACL tears, whereas earlier reconstruction is more common in high-demand athletes and in systems with rapid access to surgery.
- Return-to-sport criteria are converging on a minimum of roughly 9-12 months plus objective functional and psychological testing, reflecting graft-maturation biology rather than symptom resolution alone.
Exam Relevance (FRACS / FRCS Tr & Orth)
- Ligament biology is a core basic-science viva topic: examiners probe hierarchical structure, the four-zone enthesis, stress-strain curve regions and the healing phases.
- High-yield testable points: Type I collagen dominance, crimping and the toe region, the graft weakening phase, and the intra-articular versus extra-articular healing distinction with its management consequences.
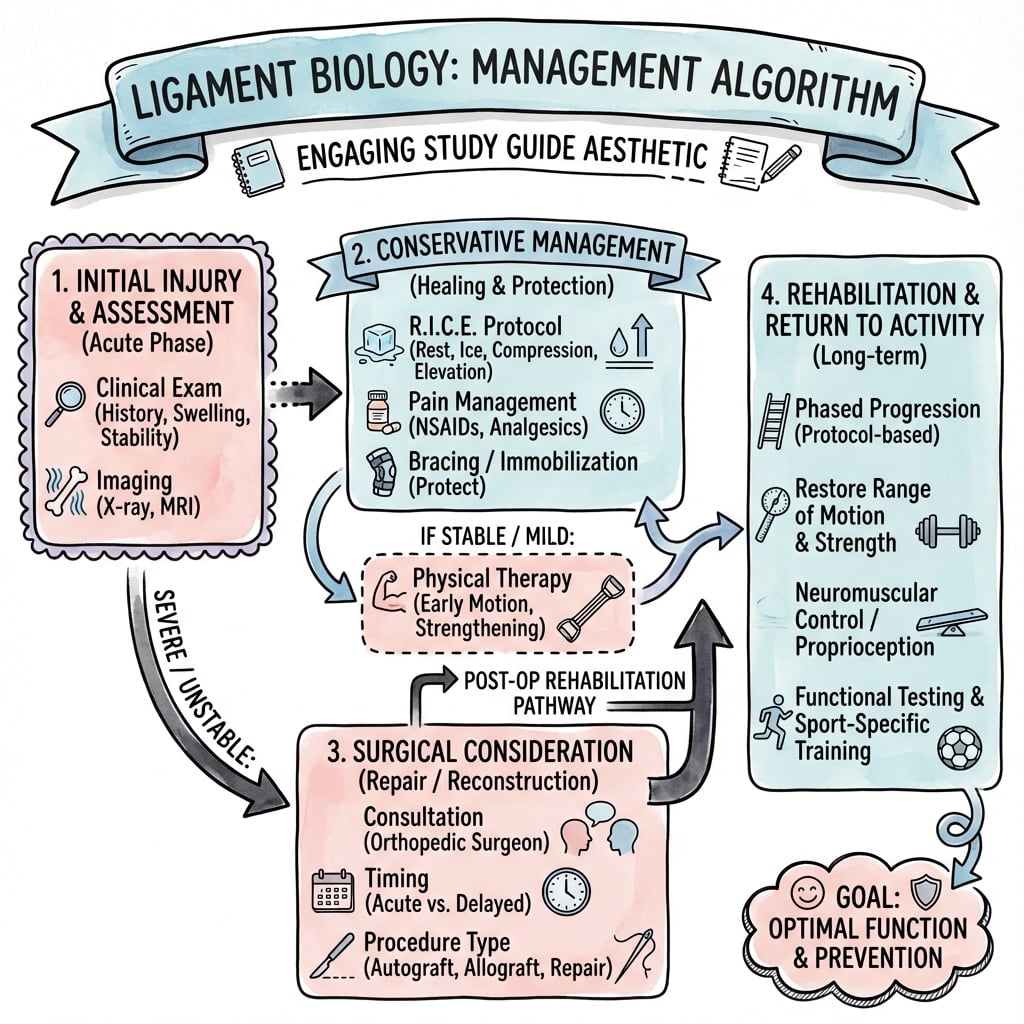
Management Algorithm
LIGAMENT BIOLOGY
Clinical summary
Composition
- •Type I collagen: 70-80% dry weight (main structural protein, tensile strength)
- •Type III collagen: under 10% normal (increases to 30% in healing, should decrease)
- •Water: 60-80% total weight (viscoelasticity, nutrient transport)
- •Proteoglycans: 1-3% (decorin, biglycan - organize fibrils, resist compression)
- •Elastin: 1-5% (70% in ligamentum flavum - unique elastic ligament)
- •Cells: 90-95% fibroblasts, 5-10% chondrocytes/synovial/vascular cells
Hierarchical Structure (TMSFL)
- •Tropocollagen: 300nm × 1.5nm triple helix (3 alpha chains, basic unit)
- •Microfibril: 5 staggered tropocollagen, 67nm D-period banding pattern
- •Subfibril: 10-20nm assembled microfibrils, cross-linking begins
- •Fibril: 50-500nm bundles with crimping pattern (20-100 micrometer period)
- •Fascicle: Fibril bundles + endoligament sheath (functional unit)
- •Ligament: Fascicle groups + epiligament (macroscopic structure)
Four-Zone Enthesis (LFMB)
- •Zone 1 - Ligament: Dense regular CT, aligned Type I collagen
- •Zone 2 - Fibrocartilage: Chondrocytes appear, Type II increases, resists compression
- •Zone 3 - Mineralized FC: Hydroxyapatite crystals, tidemark, Type X collagen
- •Zone 4 - Bone: Sharpey fibers anchor ligament, vascular supply
- •Function: Graded modulus (100-400 MPa → 10-20 GPa) minimizes stress concentration
- •Clinical: Does not regenerate after surgery, bony avulsions heal better
Stress-Strain Curve Regions
- •Toe (0-3% strain): Crimp straightening, low stiffness, physiological loading
- •Linear (3-8% strain): Collagen fibers resist directly, modulus 100-400 MPa
- •Yield (4-8% strain): Microstructural damage, permanent deformation, sprain
- •Failure (over 8% strain): Macroscopic rupture, UTS 20-100 MPa
Mechanical Properties
- •ACL: 2160N failure load (young), 242 N/mm stiffness, 38 MPa UTS
- •PCL: 2000N failure, 295 N/mm stiffness, thicker than ACL
- •MCL: 3000N failure, 140 N/mm stiffness, broad insertion distributes load
- •Patellar tendon: 2900N failure, 660 N/mm stiffness (common ACL graft)
- •Viscoelastic: Creep, stress relaxation, hysteresis, strain rate dependent
- •Age: Strength peaks 30-40 years, ACL drops 70% by age 60-97
Healing Timeline (IPR)
- •Inflammatory (0-7 days): Hematoma, neutrophils, macrophages, PDGF/TGF-β/VEGF
- •Proliferative (7d-6wk): Fibroblasts, Type III collagen (up to 30%), neovascularization, strength 10-30%
- •Remodeling (6wk-24mo): Type I replaces Type III, alignment, cross-linking, strength plateaus 50-70%
- •Incomplete restoration: Disorganized collagen, persistent Type III, reduced cross-links
ACL Graft Remodeling (4 Phases)
- •0-8 weeks: Avascular graft, bone tunnel weakest link, protect interface
- •8-12 weeks: Revascularization from synovium/bone tunnels, hypercellular response
- •3-4 months: GRAFT WEAKENING PHASE - critical vulnerable period despite clinical recovery
- •3-12 months: Cellular remodeling, collagen turnover, strength increases gradually
- •12-24 months: Maturation, histology approaches native, plateaus at 50-70% strength
- •Return to sport: Minimum 9-12 months based on biology, not subjective recovery
Intra-Articular vs Extra-Articular Healing
- •Intra-articular (ACL, PCL): Poor healing - synovial fluid dilutes hematoma, disperses growth factors, proteases degrade matrix, mechanical instability
- •Extra-articular (MCL, LCL): Better healing - stable hematoma, concentrated growth factors, vascular supply, mechanical protection possible
- •Clinical: MCL grades 1-2 conservative, ACL requires reconstruction
- •Bony avulsion: Excellent healing - preserves enthesis, cancellous bone vascularity
Key Exam Numbers
- •Type I collagen: 70-80% dry weight
- •Water content: 60-80% total weight
- •Healing strength: 50-70% native maximum
- •ACL young adult: 2160N failure (drops to 658N by age 60-97)
- •Graft weakening: 3-4 months post-reconstruction
- •Return to sport: 9-12 months minimum
- •Enthesis transition: Under 1mm distance, 50-100× modulus increase