Strain Classification | Satellite Cells | Regeneration vs Fibrosis | Return to Sport
- Satellite cells are muscle stem cells essential for regeneration
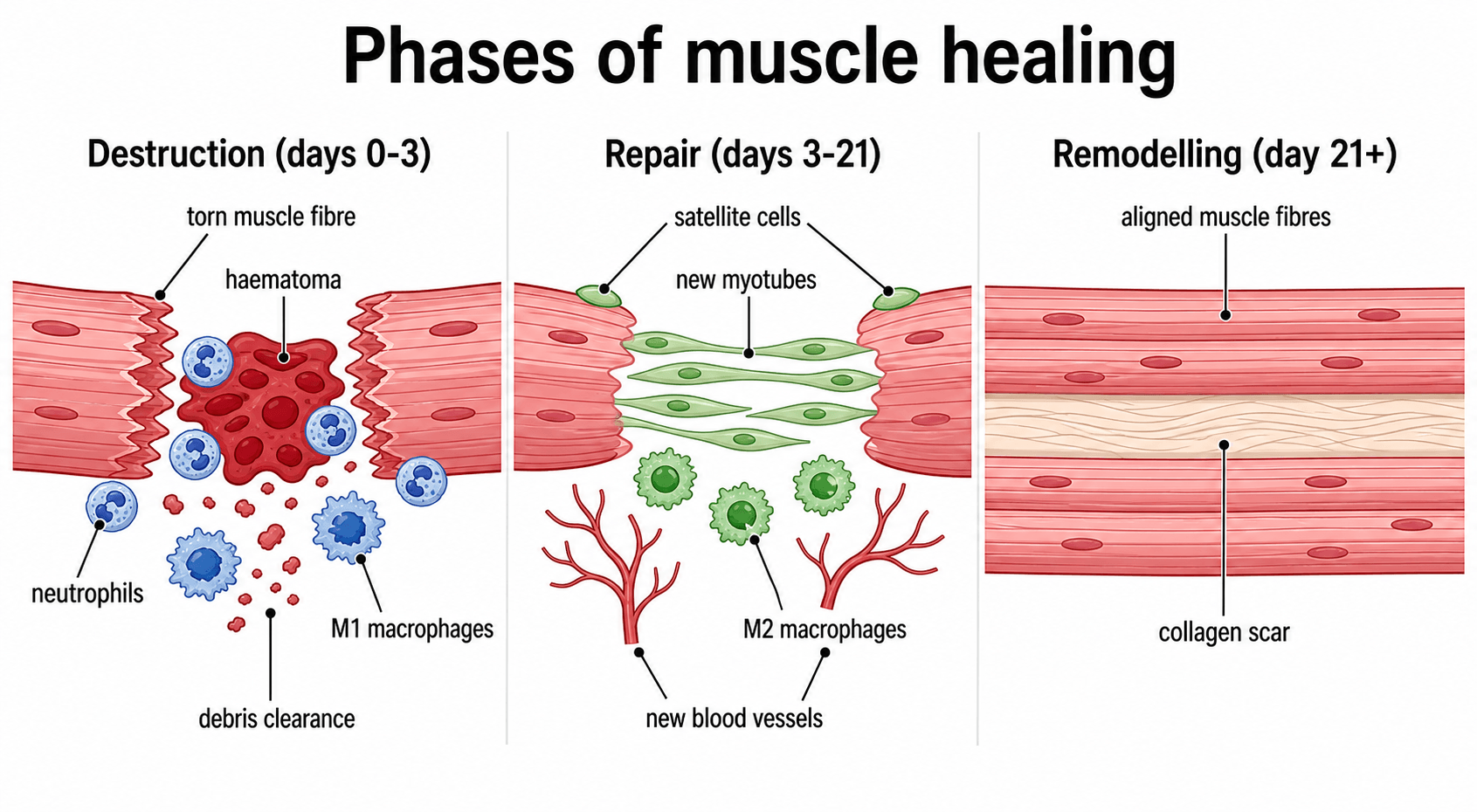
- Three healing phases: Destruction (0-3 days), Repair (3-21 days), Remodeling (21+ days)
- Myotendinous junction is most common injury site
- Early mobilization promotes regeneration over fibrosis
- Fibrosis occurs when regenerative capacity is overwhelmed
- “Satellite cells express Pax7 and are located beneath basal lamina
- “Type IIb fibers are most susceptible to strain injury
- “Eccentric contractions cause most muscle injuries
- “NSAIDs may impair early healing but reduce fibrosis
Muscle stem cells located between sarcolemma and basal lamina. Express Pax7 in quiescent state, MyoD when activated. Essential for regeneration - without them, only fibrosis occurs.
Most common injury site due to stress concentration. The interdigitating membrane folds provide 10-20x surface area but remain vulnerable during eccentric loading. Grade III injuries often avulse here.
Competition between healing pathways. Early mobilization, adequate blood supply, and satellite cell activation favor regeneration. Severe injury, immobilization, and poor vascularity favor fibrosis and scar.
Active lengthening causes most muscle strains. Fast-twitch Type IIb fibers spanning two joints (hamstrings, rectus femoris, gastrocnemius) are most vulnerable during the late swing phase.
- Grade I (Mild)
- Less than 5%
- Grade II (Moderate)
- 5-50%
- Grade III (Severe)
- More than 50% or complete
- Grade I (Mild)
- Localized tenderness
- Grade II (Moderate)
- Palpable defect, weakness
- Grade III (Severe)
- Complete loss of function
- Grade I (Mild)
- Minimal
- Grade II (Moderate)
- Moderate
- Grade III (Severe)
- Significant with hematoma
- Grade I (Mild)
- Able
- Grade II (Moderate)
- Antalgic gait
- Grade III (Severe)
- Unable
- Grade I (Mild)
- 1-2 weeks
- Grade II (Moderate)
- 3-6 weeks
- Grade III (Severe)
- 3-6 months
- Grade I (Mild)
- Often normal
- Grade II (Moderate)
- Partial tear on MRI
- Grade III (Severe)
- Complete disruption
- Grade I (Mild)
- RICE, early ROM
- Grade II (Moderate)
- Protected rehab
- Grade III (Severe)
- Surgery consideration
SATELLITESATELLITE - Muscle Stem Cells
Hook:SATELLITE cells orbit muscle fibers, waiting to repair damage like satellite dishes receiving signals
Overview / Introduction
Skeletal muscle injury is among the most common presentations in sports medicine and trauma, and skeletal muscle is one of the few adult tissues with a genuine capacity for scar-free regeneration through a dedicated stem-cell population. Understanding why injured muscle sometimes regenerates fully and sometimes heals by fibrosis is a core basic-science theme tested across orthopaedic fellowship examinations.
- It links basic science (satellite cells, myogenic regulatory factors, macrophage polarisation) to clinical management (classification, POLICE, eccentric rehabilitation, return to sport).
- It is a favourite vehicle for examiners to probe tissue healing principles that generalise to tendon, ligament and bone.
- The regeneration-versus-fibrosis balance is a recurring high-yield concept that explains re-injury, chronic stiffness and the rationale for early controlled loading.
muscle structure and fibre-type susceptibility, mechanisms of injury (strain, contusion, laceration), the three-phase healing cascade, the cellular and molecular control of regeneration, classification systems (clinical Grade I-III and the imaging-based Munich classification), assessment, evidence-based treatment, pharmacology, complications, and global guideline/registry context.
Muscle Structure and Biology
Skeletal muscle constitutes approximately 40% of body mass and is a highly organized tissue capable of both force generation and regeneration.
Hierarchical organization:
- Muscle fiber (myofiber): Multinucleated syncytium, 10-100 μm diameter
- Myofibril: Contractile unit containing sarcomeres
- Sarcomere: Z-line to Z-line, contains actin and myosin
- Fascicle: Bundle of fibers surrounded by perimysium
- Muscle belly: Multiple fascicles within epimysium
Fiber types and susceptibility:
- Metabolism
- Oxidative
- Contraction
- Slow
- Fatigue Resistance
- High
- Injury Risk
- Lower
- Metabolism
- Oxidative-Glycolytic
- Contraction
- Fast
- Fatigue Resistance
- Moderate
- Injury Risk
- Moderate
- Metabolism
- Glycolytic
- Contraction
- Fast
- Fatigue Resistance
- Low
- Injury Risk
- Highest
Type IIb fibers are most susceptible to strain injury because they generate high forces rapidly but fatigue quickly. Their low oxidative capacity means they rely on anaerobic metabolism and are more prone to metabolic failure during sustained eccentric loading.
Satellite cell biology:
- Location: Between sarcolemma and basal lamina
- Quiescent state: Express Pax7, remain dormant
- Activation: Injury releases HGF, FGF, triggers proliferation
- Differentiation: Express MyoD, Myf5, myogenin, MRF4
- Self-renewal: Asymmetric division maintains pool
Satellite cells are essential for postnatal muscle growth and regeneration. Without satellite cells, damaged muscle cannot regenerate and heals only by fibrosis.
Mechanisms of Muscle Injury
Strain Injuries (Most Common)
Definition: Injury from excessive tensile force during muscle contraction
- Eccentric contraction (active lengthening) is highest risk
- Force exceeds tensile strength at myotendinous junction
- Fast-twitch fibers fail first
- Late swing phase of running (hamstrings)
- Kicking motion (rectus femoris)
- Push-off phase (gastrocnemius)
- Previous injury (scar tissue reduces compliance)
- Muscle imbalance (weak hamstrings relative to quadriceps)
- Fatigue (reduced force absorption capacity)
- Poor flexibility (reduced extensibility)
- Inadequate warm-up
Strain injuries account for over 90% of sports-related muscle injuries.
Myotendinous junction vulnerability:
The myotendinous junction (MTJ) is the most common site of muscle strain injury. Features contributing to vulnerability include:
- Stress concentration: Transition from compliant muscle to stiff tendon
- Structural complexity: Interdigitating membrane folds
- Force transmission zone: All contractile force passes through MTJ
- Limited blood supply: Watershed region
The MTJ membrane folds increase surface area 10-20 fold for force transmission but remain the weak link in the muscle-tendon unit.
FASTFAST TWITCH - Injury Risk Factors
Hook:FAST twitch fibers fail first during eccentric loading
Modern Imaging-Based Classification (Munich and BAMIC)
The clinical Grade I-III system above is simple but imprecise. Elite sports medicine now uses imaging-based classifications that separate functional disorders from true structural tears and locate the injury, because site (especially intratendinous involvement) predicts return-to-play time better than size alone.
Munich consensus classification (Mueller-Wohlfahrt 2013):
- Type
- Type 1 — overexertion-related
- Description
- 1a fatigue-induced; 1b delayed-onset muscle soreness (DOMS)
- Type
- Type 2 — neuromuscular
- Description
- 2a spine-related; 2b muscle-related (neuromuscular control)
- Type
- Type 3 — partial tear
- Description
- 3a minor (< a fascicle/bundle); 3b moderate partial tear
- Type
- Type 4 — (sub)total tear / avulsion
- Description
- Subtotal or complete muscle tear or tendinous avulsion
British Athletics Muscle Injury Classification (BAMIC, Pollock 2014) — grades 0-4 for size combined with a site letter: a = myofascial, b = musculotendinous (at the MTJ), c = intratendinous (extends into the tendon). Grade 0 = MRI-negative (0a focal, 0b DOMS); grades 1-4 = increasing extent; grade 4 = complete tear.
In BAMIC, the "c" (intratendinous) injuries carry the worst prognosis and the longest return-to-play, even for a given grade, because the tendon is the slow-healing, load-bearing element. This is why modern classification records the site, not just the percentage of fibres torn — a key advance over the Grade I-III system.
Phases of Muscle Healing
Muscle Healing Timeline
- Fiber necrosis and rupture
- Hematoma formation
- Inflammatory cell infiltration (neutrophils, then macrophages)
- Phagocytosis of necrotic debris
- Release of growth factors (HGF, FGF, IGF-1)
- Neutrophils peak at 24 hours
- M1 macrophages (pro-inflammatory) dominate
- Satellite cells activated but not yet proliferating
- Satellite cell proliferation and differentiation
- Myoblast fusion to form myotubes
- New myofiber formation
- Revascularization (angiogenesis)
- Connective tissue scaffold formation
- M2 macrophages (anti-inflammatory) dominate
- Peak myoblast proliferation at day 5-7
- Myotubes visible by day 5
- New fibers express embryonic myosin
- Collagen III deposition
- Myofiber maturation and hypertrophy
- Collagen III replaced by Collagen I
- Scar tissue remodeling
- Fiber alignment with stress
- Neuromuscular junction reestablishment
- Mature myosin isoform expression
- Tensile strength increases progressively
- Complete remodeling may take 6-12 months
- Some scar tissue may persist permanently
Molecular regulation of healing:
- Key Factors
- TNF-α, IL-1β
- Role
- Pro-inflammatory signaling
- Key Factors
- HGF
- Role
- Satellite cell activation
- Key Factors
- FGF, IGF-1
- Role
- Myoblast proliferation
- Key Factors
- Myostatin
- Role
- Negative regulator (inhibits growth)
- Key Factors
- MyoD, Myogenin
- Role
- Myogenic differentiation
- Key Factors
- TGF-β
- Role
- Fibrosis (if excessive)
- Key Factors
- Mechanical loading
- Role
- Fiber alignment, hypertrophy
The transition from pro-inflammatory M1 macrophages to anti-inflammatory M2 macrophages around day 3-4 is critical for successful regeneration. M1 macrophages clear debris but also release factors that can impair regeneration if prolonged. M2 macrophages promote myoblast differentiation and angiogenesis.
DRRDRR - Healing Phases
Hook:DRR = Destroy, Repair, Remodel - the three phases of muscle healing
Regeneration vs Fibrosis
The critical balance:
Muscle healing represents a competition between regeneration (restoration of functional muscle) and fibrosis (scar formation). Understanding factors that influence this balance is essential.
- Satellite cell availability and activation
- Adequate blood supply
- Early controlled mobilization
- Preserved basal lamina scaffold
- Limited injury extent
- Young age
- Satellite cell depletion
- Poor vascularity
- Prolonged immobilization
- Extensive basal lamina disruption
- Large injury gap
- Repeated injury to same area
- Advanced age
- Regeneration
- Satellite cells, myoblasts
- Fibrosis
- Fibroblasts
- Regeneration
- New muscle fibers
- Fibrosis
- Collagen scar
- Regeneration
- Contractile, normal
- Fibrosis
- Non-contractile, stiff
- Regeneration
- Normal capillary bed
- Fibrosis
- Reduced vessels
- Regeneration
- MyoD, IGF-1
- Fibrosis
- TGF-β, CTGF
- Regeneration
- Weeks to months
- Fibrosis
- Forms within weeks
TGF-β: The fibrosis switch:
Transforming growth factor beta (TGF-β) plays a central role in determining regeneration vs fibrosis:
- Physiological levels: Promotes matrix production for scaffold
- Excessive levels: Induces fibroblast proliferation and collagen deposition
- Therapeutic target: TGF-β inhibition reduces fibrosis in animal models
Clinical implications:
- Early mobilization promotes satellite cell activity and reduces fibrosis
- Severe injuries with large gaps tend toward fibrosis
- Repeated injuries to same location create progressively more scar
- Complete ruptures may require surgical approximation to allow regeneration
Clinical Assessment
History:
- Mechanism of injury (eccentric loading, direct trauma)
- Precise location of pain
- Immediate vs delayed onset
- Audible pop or tearing sensation
- Functional limitations
- Previous injury to same muscle
Examination:
- Grade I
- Localized tenderness
- Grade II
- Diffuse tenderness
- Grade III
- Over defect
- Grade I
- No
- Grade II
- May be present
- Grade III
- Yes (palpable gap)
- Grade I
- Minimal
- Grade II
- Moderate
- Grade III
- Significant
- Grade I
- Delayed, minimal
- Grade II
- Moderate
- Grade III
- Extensive, early
- Grade I
- Nearly full
- Grade II
- Reduced, painful
- Grade III
- Absent or minimal
- Grade I
- Full but painful
- Grade II
- Reduced
- Grade III
- Unable
- Grade I
- Minor limitation
- Grade II
- Moderate limitation
- Grade III
- Unable to function
- First-line imaging for acute injuries
- Dynamic assessment possible
- Identifies hematoma, fiber disruption
- Operator dependent
- Gold standard for injury characterization
- Grades edema and fiber disruption
- Identifies extent and location
- Useful for surgical planning in Grade III
- Grade I: Edema, no fiber disruption (less than 5% cross-section)
- Grade II: Partial fiber disruption (5-50% cross-section)
- Grade III: Complete disruption or more than 50% involvement
The "felt a pop, sudden pain" presentation is not always a simple strain. Key alternatives must be excluded, especially in skeletally immature or older patients.
- Distinguishing features
- Eccentric mechanism, tender at myotendinous junction, pain on resisted contraction
- Key investigation
- MRI / ultrasound shows feathery edema at MTJ
- Distinguishing features
- Palpable gap, marked weakness, ecchymosis tracking distally
- Key investigation
- MRI shows tendon discontinuity and retraction
- Distinguishing features
- Skeletally immature, ischial or AIIS pain, bony fragment
- Key investigation
- Plain radiograph shows displaced apophysis
- Distinguishing features
- Calf swelling, no clear mechanism, risk factors present
- Key investigation
- Doppler ultrasound; do not aggressively mobilise
- Distinguishing features
- Pain out of proportion, pain on passive stretch, tense compartment
- Key investigation
- Clinical diagnosis; compartment pressures if unclear
- Distinguishing features
- Diffuse, bilateral, peaks 24-72h after unaccustomed exercise
- Key investigation
- Clinical; self-limiting, no focal defect
- Distinguishing features
- Firm, enlarging mass weeks after contusion, restricted ROM
- Key investigation
- Radiograph/CT shows peripheral zonal ossification
Treatment Principles
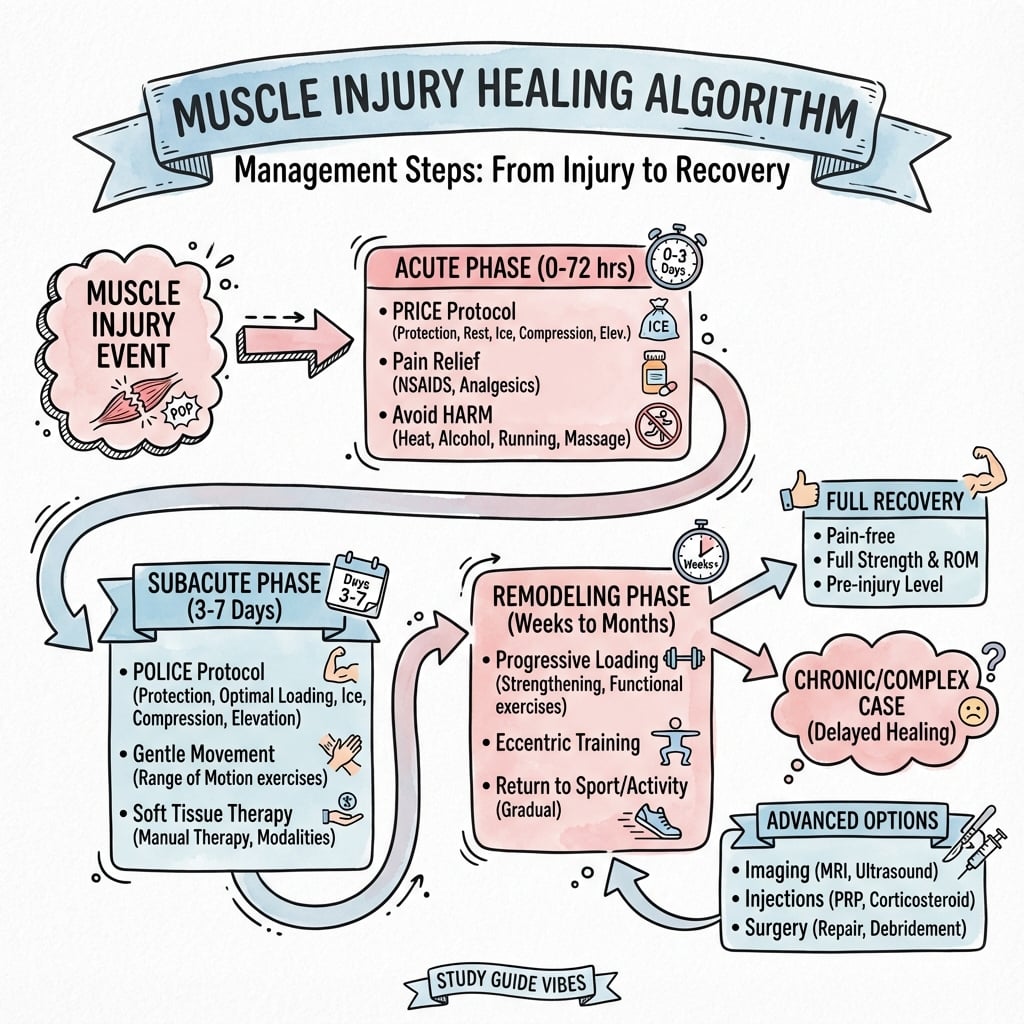
Acute Phase (Days 0-3)
- Avoid aggravating activities
- Consider crutches if weight bearing painful
- Compression bandaging
- Complete rest is NOT recommended
- Early protected movement within pain limits
- Isometric contractions when comfortable
- 15-20 minutes every 2-3 hours
- Reduces metabolic demand
- Limits secondary hypoxic injury
- Reduces hematoma expansion
- Limits edema formation
- Reduces venous pressure
- Promotes lymphatic drainage
Modern approach replaces RICE with POLICE (Protection, Optimal Loading, Ice, Compression, Elevation).
Surgical considerations (Grade III injuries):
- Surgery Indications
- Complete avulsion from ischium
- Technique
- Suture anchor repair
- Surgery Indications
- Complete distal rupture
- Technique
- End-to-end repair
- Surgery Indications
- Complete rupture off humerus
- Technique
- Suture anchor reattachment
- Surgery Indications
- Complete rupture (see dedicated topic)
- Technique
- End-to-end repair or augmentation
Pharmacological Considerations
NSAIDs - Controversial role:
- Evidence
- Effective in acute phase
- Evidence
- Reduces early inflammation
- Evidence
- May delay satellite cell activation
- Evidence
- May decrease scar formation
- Limit NSAID use to first 48-72 hours if needed for pain
- Avoid prolonged use during repair phase
- Paracetamol preferred for ongoing analgesia
- Generally contraindicated
- Risk of delayed healing
- Risk of tendon rupture (at MTJ)
- May be considered for specific indications (e.g., severe contusion with compartment concerns)
- Theoretical benefit from growth factors
- Mixed clinical evidence
- Not currently standard of care
- May have role in chronic non-healing injuries
- Growth factor therapy (IGF-1, HGF)
- Anti-TGF-β agents (reduce fibrosis)
- Stem cell therapies
- Gene therapy approaches
Most emerging therapies remain experimental.
Complications
- Bone formation within muscle tissue
- Most common after contusion injury
- Risk factors: Aggressive early treatment, repeat trauma, hematoma aspiration
- Prevention: Avoid aggressive stretching, heat in early phase
- Treatment: Observation, excision after maturation (6-12 months)
- Rare but serious complication
- Usually after severe contusion or crush injury
- Pain out of proportion, pain with passive stretch
- Urgent fasciotomy required
- Persistent weakness
- Reduced flexibility
- Re-injury susceptibility
- May result from excessive fibrosis
- Most common complication
- Previous injury is strongest risk factor
- Usually occurs in same location
- Prevention: Complete rehabilitation before return to sport
Five Ps (often late signs):
- Pain out of proportion
- Pain with passive stretch
- Paresthesias
- Pallor
- Pulselessness (very late)
Early sign: Increasing analgesic requirements
Maintain high index of suspicion after crush injuries or severe contusions.
Guidelines, Registries and Global Practice
Global epidemiology:
- Muscle injuries account for roughly 30% of all time-loss injuries in professional football, with thigh injuries alone representing about 25% of injuries in the UEFA Elite League cohort.
- Indirect (strain) injuries vastly outnumber direct (contusion) injuries (88% vs 12% of thigh injuries) and cause markedly longer absence (mean 18.5 vs 7 days).
- The hamstrings are the single most commonly injured muscle group in sprinting sports; rectus femoris and gastrocnemius follow. Recurrence rates of 12-30% make muscle injury one of the costliest problems in elite sport.
Side-by-side guidance and classification systems:
- Focus
- Terminology and classification
- Key recommendation
- Distinguishes functional disorders (types 1-2) from structural injuries (types 3-4); standardises language
- Focus
- MRI-based grading
- Key recommendation
- Grades 0-4 plus a/b/c by site (myofascial, musculotendinous, intratendinous); intratendinous (c) injuries have worse prognosis
- Focus
- Clinical plus imaging
- Key recommendation
- Combines mechanism and imaging to guide prognosis
- Focus
- Rehabilitation principles
- Key recommendation
- Early controlled loading and progressive eccentric exercise; functional return-to-sport criteria over fixed timelines
- Focus
- Tissue healing principles
- Key recommendation
- Protect, then progressively load; surgery reserved for complete avulsions/ruptures
Unlike arthroplasty, muscle injuries are not tracked in implant registries; the most authoritative population-level data come from prospective surveillance cohorts such as the UEFA Elite Club Injury Study, which functions as a de facto registry for elite-football soft-tissue injury and underpins much of the global epidemiology above.
- High-resource settings: Early MRI for grading and prognosis, individualised eccentric rehabilitation with objective strength/return-to-sport testing, and access to physiotherapy-led graded loading.
- Limited-resource settings: Clinical grading (Grade I-III) without routine MRI, with management centred on the universally available and evidence-supported core: relative rest, protection, progressive loading and graded return. The key message is that the highest-value interventions (early controlled loading and progressive eccentric rehabilitation) require no expensive technology.
Controversies and Areas of Uncertainty
Muscle-injury management contains several genuinely unresolved questions that examiners use to test depth of understanding. Acknowledging uncertainty (rather than overstating dogma) is a marker of consultant-level judgment.
Animal data suggest NSAIDs blunt the inflammatory signalling and satellite-cell activation needed for regeneration, yet human clinical trials are inconsistent and most show no clear functional harm with short courses. The pragmatic consensus is to limit NSAIDs to short-term analgesia in the acute phase and prefer paracetamol thereafter, but this is opinion-led, not high-level evidence.
Despite biological plausibility, the best evidence (Pas/Reurink 2015 meta-analysis) shows no benefit of PRP for acute hamstring injury. PRP, stem-cell and growth-factor therapies remain experimental for muscle, and routine clinical use is not supported.
The simple clinical Grade I-III system is easy but has poor prognostic value. Imaging-based systems (Munich, British Athletics, ISMuLT) add detail and prognostic discrimination but are less universally adopted and add cost. No single system is the agreed global standard.
Early controlled loading is favoured over immobilization, but the optimal timing, intensity and progression of eccentric loading, and the precise return-to-sport thresholds, remain debated. Most protocols are extrapolated from small studies and expert consensus.
MCQ Practice Points
Q: Which marker identifies a quiescent satellite cell? A: Pax7. Quiescent satellite cells reside beneath the basal lamina and express the transcription factor Pax7. On activation they upregulate MyoD and Myf5, then myogenin and MRF4 as they differentiate into myoblasts. A cell co-expressing Pax7 but not MyoD is quiescent; loss of Pax7 with gain of myogenin signals terminal differentiation.
Q: Which fibre type and contraction mode carry the highest strain risk? A: Fast-twitch Type IIb fibres during eccentric (active lengthening) contraction. Biarticular muscles with a high proportion of Type IIb fibres (hamstrings, rectus femoris, gastrocnemius) fail most often, typically at or near the myotendinous junction during the late swing phase of sprinting.
Q: What single cellular event best distinguishes regeneration from fibrosis? A: Satellite cell activation and myotube formation versus fibroblast-driven collagen deposition. When satellite cells are available and the basal lamina scaffold is preserved, new contractile fibres form. When satellite capacity is overwhelmed or the scaffold is destroyed, TGF-beta1-driven fibroblast activity lays down non-contractile collagen scar.
Q: For an acute hamstring strain, what intervention has the strongest evidence? A: Progressive lengthening (eccentric) rehabilitation exercises, not platelet-rich plasma. Meta-analysis (Pas/Reurink 2015) showed lengthening rehabilitation significantly shortened return to play (HR 3.22) while PRP showed no benefit over control.
Q: When does the macrophage phenotype switch occur and why does it matter? A: Around day 3-4, pro-inflammatory M1 macrophages give way to anti-inflammatory M2 macrophages. M1 cells phagocytose necrotic debris; M2 cells promote myoblast differentiation and angiogenesis. A failed or prolonged M1 phase impairs regeneration and favours fibrosis.
Rapid-fire high-yield facts:
- Satellite cells express Pax7 (quiescent) and MyoD (activated), located between sarcolemma and basal lamina
- Type IIb fast-twitch fibres are most susceptible to strain
- Myotendinous junction is the most common strain site
- Phases: Destruction (days 0-3), Repair (days 3-21), Remodeling (day 21 onwards)
- M1 macrophages are pro-inflammatory; M2 macrophages promote repair
- TGF-beta drives fibrosis; early controlled mobilization favours regeneration
- Myositis ossificans is the classic complication of quadriceps contusion
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A basic science examiner asks you to describe the phases of muscle healing following a Grade II hamstring strain.”
“A 25-year-old footballer presents with acute posterior thigh pain after sprinting. He felt a pop and has weakness with knee flexion. How do you classify and manage this injury?”
“Explain the role of satellite cells in muscle regeneration and what happens if they are depleted.”
Key Anatomy
- Satellite cells between sarcolemma and basal lamina
- Pax7+ quiescent, MyoD+ activated
- Type IIb fast-twitch most vulnerable
- MTJ is most common injury site
Healing Phases
- Destruction: Days 0-3, necrosis, M1 macrophages
- Repair: Days 3-21, satellite activation, M2 macrophages
- Remodeling: Day 21+, fiber maturation, collagen conversion
Strain Classification
- Grade I: Less than 5% fibers, return 1-2 weeks
- Grade II: 5-50%, partial tear, return 3-6 weeks
- Grade III: More than 50% or complete, return 3-6 months
Treatment Principles
- POLICE not RICE (Optimal Loading)
- Early mobilization promotes regeneration
- Progress: Isometrics to Isotonics to Eccentrics
- Return when less than 10% strength deficit
Regeneration vs Fibrosis
- Satellite cells = regeneration
- TGF-β excess = fibrosis
- Early mobilization favors regeneration
- Repeated injury increases scar
Complications
- Myositis ossificans after contusion
- Re-injury is most common complication
- Compartment syndrome rare but serious
- Previous injury is biggest risk factor
Evidence Base
Muscle injuries: biology and treatment
- Foundational narrative review defining the three-phase model: destruction, repair, remodeling
- Satellite cells (located beneath the basal lamina) are essential for true regeneration
- Brief immobilization to allow scar to gain strength, then early controlled mobilization, is superior to either prolonged rest or immediate aggressive loading
- Fibrosis (granulation tissue and scar) and regeneration progress in parallel and compete
Muscle injuries and repair: current trends in research
- TGF-beta1 is a central driver of post-injury fibrosis in skeletal muscle
- Antifibrotic agents (e.g. decorin, suramin, gamma-interferon) reduced scar in animal models
- Growth factors (IGF-1, bFGF, NGF) enhanced myoblast proliferation and muscle regeneration in vivo
- Combined antifibrosis plus growth-factor strategies improved functional recovery experimentally
Inflammatory processes in muscle injury and repair
- Neutrophils invade rapidly after injury and can promote further muscle damage via free radicals
- Pro-inflammatory (M1) macrophages clear debris; anti-inflammatory (M2) macrophages support repair, regeneration and growth
- Macrophage actions are coordinated with satellite cell activation, proliferation and differentiation
- Muscle-derived nitric oxide modulates inflammatory cell invasion, protecting healthy fibres