Needlestick and Sharps Injury
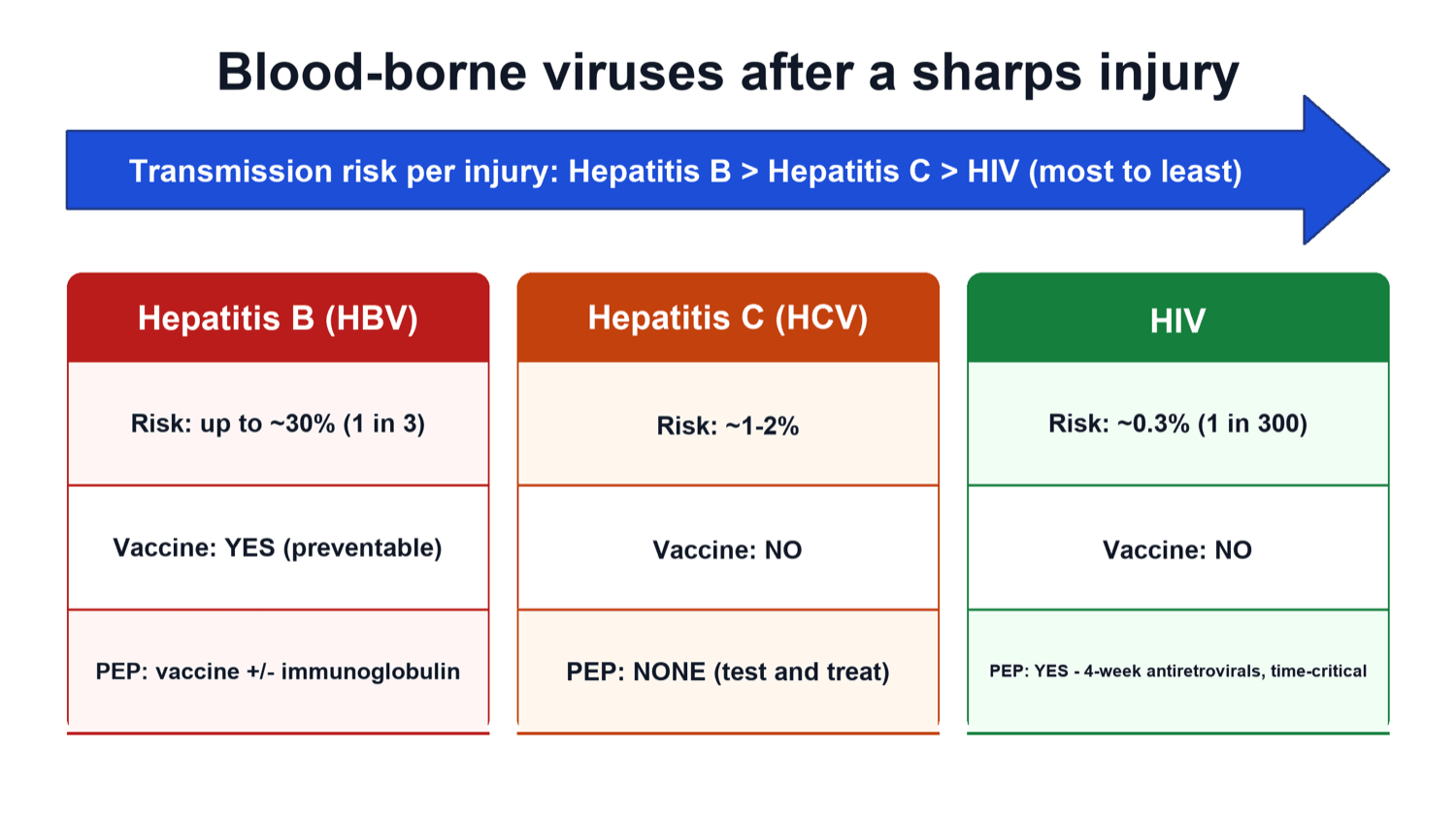
Per injury, transmission risk runs hepatitis B greater than hepatitis C greater than HIV. Untreated hepatitis B is the most transmissible; HIV is the least likely per stick but is the one with time-critical drug prophylaxis. Quoting this order confidently is a classic viva win.
Encourage bleeding, wash with soap and running water, irrigate splashed eyes or mouth with water/saline. Do NOT suck the wound, scrub it, or apply caustic agents - there is no evidence these help and they may worsen tissue damage.
For a significant exposure from an HIV-positive or high-risk source, start post-exposure prophylaxis as soon as possible (ideally within hours, and generally not beyond 72 hours), continue for 4 weeks, and arrange follow-up testing. Hesitating to assess and refer is the trap.
Deeper injury, a hollow blood-filled needle, visible blood on the device, a needle that was in the source's artery or vein, and a source with advanced/high-viral-load disease all raise the chance of transmission. These factors guide whether PEP is offered.
Overview
A needlestick or sharps injury is when a contaminated needle, blade, wire, drill bit, or bone fragment pierces the skin of a member of the surgical team. It is one of the most common occupational hazards in surgery and a favourite exam topic because it links microbiology (which viruses), risk assessment (how likely is transmission), and practical management (what you actually do at 2am when you are stuck).
The reason it matters is blood-borne viruses. A single percutaneous injury can transmit hepatitis B virus, hepatitis C virus, or HIV from an infected source patient into the injured worker. The chance of transmission from any one injury is generally low, but it is not zero, and it rises with deeper injuries, hollow blood-filled needles, and sources with high viral loads.
Orthopaedics is a high-risk specialty. We routinely handle sharp Kirschner wires, drill bits, oscillating saws, sharp-tipped suture needles, and jagged bone ends, often with reduced tactile feedback through gloves and in awkward positions. This means more sharps exposures than in many other fields. The whole topic reduces to two threads the examiner will test: prevent the injury (double gloving, blunt needles, no-touch technique, safe disposal, vaccination), and respond correctly when it happens (first aid, report, risk-assess, treat).
Principles: The Viruses and the Transmission Risk
Three blood-borne viruses dominate the risk assessment after a sharps injury. The order of transmission risk per injury is the single most testable fact: hepatitis B is the most transmissible, then hepatitis C, then HIV is the least transmissible per stick.
- Approximate risk per percutaneous injury (positive source)
- Highest of the three - can reach roughly one in three when the source is highly infectious (e antigen positive) and the worker is non-immune
- Key exam point
- Largely preventable by VACCINATION - a documented vaccine responder is well protected; an unvaccinated worker may need vaccine plus hepatitis B immunoglobulin
- Approximate risk per percutaneous injury (positive source)
- Intermediate - on the order of a few per cent (commonly quoted around 1 to 2 percent)
- Key exam point
- No vaccine and no effective drug prophylaxis after exposure - management is baseline testing, follow-up testing, and early antiviral treatment if seroconversion occurs
- Approximate risk per percutaneous injury (positive source)
- Lowest - on average about 0.3 percent (roughly 1 in 300) after a single percutaneous exposure from a positive source
- Key exam point
- The only one with time-critical drug PROPHYLAXIS (PEP). Risk is much lower if the source is on treatment with an undetectable viral load
Why the risk varies so much between viruses comes down to how much circulating virus there usually is and how the body defends against it. Hepatitis B is present in very high concentrations in infected blood and is highly infectious, which is why an unprotected worker is at greatest risk - and why vaccination, which gives most people lasting protection, is so powerful. HIV circulates at far lower levels and is less hardy, so the average per-injury risk is low, but because untreated infection is so serious we still act urgently with drug prophylaxis.
Lead with the risk order: "Per injury, hepatitis B is the most transmissible, then hepatitis C, then HIV." Then add the twist examiners love: HIV is the least likely to transmit per stick but is the only one with time-critical drug prophylaxis, while hepatitis B is the most transmissible but is largely preventable by vaccination.
What makes a single injury more dangerous
Not every stick carries the same risk. Transmission is more likely with:
- A deeper injury (more inoculum transferred)
- A hollow, blood-filled needle rather than a solid suture needle
- Visible blood on the device
- A needle that had just been in the source patient's artery or vein
- A source with advanced disease or a high viral load
These factors come straight from the landmark case-control work on HIV transmission and are used everywhere to decide whether the exposure is "significant" and whether PEP is offered.
Immediate Management After an Injury
This is the most heavily tested practical sequence. Have it ready as a structured answer: first aid, report, risk-assess the source and the injury, then treat and follow up.
For a skin injury, encourage the wound to bleed gently and wash with soap under running water. Do not suck, scrub, or apply caustic agents. For a splash to the eye, mouth, or nose, irrigate generously with water or saline. Remove contact lenses and irrigate again.
Step away from the field safely (a colleague takes over if you are scrubbed), and report promptly to occupational health or the emergency department per local policy. Prompt reporting is what unlocks timely risk assessment and PEP.
Establish the source patient's blood-borne virus status (and seek consent for testing if unknown). Grade the injury: deep, hollow blood-filled needle, visible blood, and vessel needle all raise risk. Together these decide whether the exposure is significant.
Offer HIV PEP if indicated, manage hepatitis B (booster or immunoglobulin depending on vaccination status and source), take baseline bloods from the worker, and arrange follow-up testing. There is no PEP for hepatitis C - it is baseline plus follow-up testing and early treatment if seroconversion occurs.
If the exposure looks significant and the source is HIV-positive or high-risk, start PEP as soon as possible (ideally within hours; it is generally not started beyond 72 hours) and review/stop it once source results are back. Waiting for every test result before starting can mean missing the window where prophylaxis works.
Managing each virus
- Hepatitis B: depends on the worker's vaccination/immune status. A documented vaccine responder is well protected and may need only a check or a booster. A non-responder or unvaccinated worker exposed to a hepatitis B source may need hepatitis B immunoglobulin plus an accelerated vaccine course.
- Hepatitis C: there is no vaccine and no post-exposure drug prophylaxis. Management is baseline testing, then follow-up testing; if the worker seroconverts, modern direct-acting antivirals are highly effective, so the emphasis is on detection and early treatment.
- HIV: a 4-week course of combination antiretroviral PEP for a significant exposure from a positive or high-risk source, started as early as possible, with counselling that PEP reduces but does not eliminate the risk, and with follow-up HIV testing.
Beyond "start PEP", know the specifics:
- The regimen: a 28-day course of combination antiretrovirals — typically a two-drug nucleoside backbone (tenofovir disoproxil plus emtricitabine) with a third agent, the modern preference being an integrase inhibitor (raltegravir or dolutegravir) for tolerability and few interactions.
- Baseline and follow-up testing: before starting, take baseline HIV (a fourth-generation antigen/antibody test), hepatitis B and C, plus renal/liver function and a pregnancy test; then follow-up HIV testing to around 12 weeks after exposure (the fourth-generation tests allow this shorter window), with hepatitis C antibody/RNA follow-up. Counsel on barrier precautions and not donating blood during the follow-up period.
- Exposure route matters: the average per-exposure HIV risk falls with the route — percutaneous (around 0.3%) is higher than a mucous-membrane splash (around 0.09%), which is higher than non-intact skin; intact skin carries no meaningful risk.
- Source unknown/untraceable: make an individual risk assessment from the clinical setting and local prevalence rather than reflexively giving or withholding PEP.
Prevention in the Operating Theatre
Prevention is the part examiners reward most, because the best management of a needlestick is never to have one. The measures stack: no single step is perfect, but together they substantially cut exposures.
The single most reliable measure. Two glove layers dramatically reduce the rate at which the inner glove (and therefore the skin) is breached, and a coloured indicator under-glove makes a perforation immediately visible so gloves can be changed. Strongly advised in orthopaedics.
Blunt-tipped needles pass through fascia and muscle but are far less likely to puncture skin. They markedly reduce sharps injuries during closure of deep layers where a sharp tip is not needed.
Use a neutral zone or hands-free transfer (a kidney dish or designated tray) so sharps are never passed hand to hand. The person using the sharp picks it up and puts it back - no two people hold it at once.
Dispose of sharps immediately into a puncture-proof container kept close to the point of use. Never resheath a needle by hand and never overfill the container - both are classic causes of injury.
Two more pillars sit around the operative measures:
- Hepatitis B vaccination of all staff, with confirmation of an antibody response. This converts the most transmissible virus into a largely preventable one and is the strongest single argument for a vaccinated workforce.
- A blame-free reporting culture and training. Underreporting of sticks is common among surgeons; a clear, fast, non-judgemental reporting pathway is what makes timely risk assessment and PEP actually happen.
If asked "how do you reduce sharps injuries in your theatre?", give a layered answer: double gloving with an indicator glove, blunt needles for deep closure, a hands-free no-touch passing technique, immediate safe disposal without resheathing, hepatitis B vaccination of staff, and a culture where everyone reports.
Clinical Relevance
Needlestick injury sits at the meeting point of personal safety, patient care, and medico-legal responsibility, which is why it appears so often in basic-science and clinical vivas. Every orthopaedic surgeon will be exposed at some point, so the examiner expects you to be calm and systematic: first aid, report, risk-assess, treat, follow up. The topic also tests whether you understand risk in proportion - that hepatitis B is the most transmissible but preventable, that HIV is the least transmissible per stick but the one needing urgent prophylaxis, and that a deep injury from a hollow blood-filled needle in a high-viral-load source is the worst-case scenario. Finally, it probes your professionalism: do you protect your team with double gloves, blunt needles, and a no-touch technique, and do you report honestly so the system can protect you? Getting all of this right is the practical core that recurs across the exam.
The topic so far is the worker being exposed; examiners also test the reverse — a blood-borne-virus-positive surgeon and the risk of transmitting to a patient. Much of orthopaedics is an exposure-prone procedure (EPP): the gloved fingertips work with sharp instruments, wires or sharp bone in a confined space or wound where they are not always fully visible, so a worker's blood could enter the patient. Workers who perform EPPs must know their status and have health clearance, and BBV-positive workers are governed by viral-load rules (the exact figures are jurisdiction-specific; UK/UKHSA values are given here as an example):
- Hepatitis B — an e-antigen-positive worker must not perform EPPs; an e-antigen-negative worker may, provided the HBV DNA viral load stays below a set threshold (around 200 IU/mL, or maintained low on antiviral treatment with monitoring).
- Hepatitis C — an HCV-RNA-positive worker must not perform EPPs until successfully treated and RNA-negative (cured), after which they may return.
- HIV — historically barred, but modern guidance permits EPPs if the worker is on effective antiretroviral therapy with an undetectable plasma viral load (below about 200 copies/mL) and is regularly monitored by occupational health.
The professional duties are to know your status, not self-diagnose or self-treat, and disclose to occupational health.
Guidelines, Registries and Global Practice
- A consistent global message runs through occupational-health guidance (for example US CDC/US Public Health Service guidance, UK guidance from UKHSA/Public Health bodies and the Royal College of Surgeons, and WHO occupational-safety standards): treat every sharps injury as a potential blood-borne virus exposure, give immediate first aid, report promptly, risk-assess the source, and offer time-critical HIV PEP for significant exposures.
- Hepatitis B vaccination of all healthcare workers with confirmation of an antibody response is recommended worldwide and is the cornerstone of protecting against the most transmissible of the three viruses.
- Engineering and practice controls are emphasised everywhere: double gloving (with an indicator glove), blunt suture needles, safety-engineered devices, hands-free transfer/neutral zones, and puncture-proof sharps containers with no resheathing.
- Underreporting is a recognised global problem, especially among surgeons. Guidance stresses a fast, blame-free reporting pathway, because timely reporting is what makes risk assessment and prophylaxis possible.
- Practice varies by setting: source HIV testing, PEP drug availability, and hepatitis B immunoglobulin access differ between high- and low-resource environments, but the assess-and-act framework is the same everywhere.
Memory aids
WASH UPImmediate Steps After a Stick
Hook:WASH UP the wound, then work UP the risk - first aid, report, assess the source, and treat if needed.
DEVICEWhat Makes an Injury High Risk
Hook:A risky DEVICE - deep, bloody, from a vessel, in an ill source, hollow, and ungloved - is the high-transmission stick.
GUARDPrevention in Theatre
Hook:GUARD the team - double gloves, blunt needles, no hand-passing, safe disposal, and hepatitis B vaccination.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are operating and a suture needle pierces your finger through a single glove. The source patient's blood-borne virus status is unknown. The examiner asks exactly what you do, in order.”
“The examiner asks you to rank the transmission risk of the three main blood-borne viruses, explain why orthopaedics is high risk, and justify the measures you use to prevent sharps injuries.”
The Three Viruses
- Risk per injury: hepatitis B greater than hepatitis C greater than HIV
- Hepatitis B: most transmissible but vaccine-preventable
- Hepatitis C: intermediate; no vaccine, no PEP - test and treat if seroconverts
- HIV: about 0.3 percent per stick; the one with time-critical PEP
Immediate Steps
- First aid: encourage bleeding, wash with soap and water, irrigate splashes
- Do NOT suck, scrub, or apply caustic agents
- Report promptly to occupational health / emergency department
- Risk-assess the injury AND the source
High-Risk Injury Features
- Deep injury, visible blood on the device
- Hollow blood-filled needle (not solid suture needle)
- Needle that was in the source's artery or vein
- Source with advanced disease / high viral load
Treatment and Prevention
- HIV PEP: start ASAP (within hours, not beyond 72h), 4-week course
- Hepatitis B: booster or immunoglobulin per vaccination status
- Prevent: double glove with indicator glove, blunt needles, no-touch technique
- Safe disposal, never resheath; vaccinate staff; report honestly
Evidence: Risk, Prophylaxis and Prevention
The evidence base is built on a small number of influential studies: a case-control study that defined HIV transmission risk and the value of prophylaxis, and randomised trials showing that extra glove layers protect the surgeon.
Every citation below has been checked against its source record in PubMed. The Cochrane review carries the pivotal case-control odds ratios that define a 'significant' exposure (deep injury, visible blood, vessel needle, terminal source) and the protective effect of prompt zidovudine PEP; the two randomised/controlled glove studies are the direct evidence that double gloving keeps the skin-facing inner glove intact.
Antiretroviral post-exposure prophylaxis (PEP) for occupational HIV exposure (Cochrane Review)
- Systematic review of occupational HIV post-exposure prophylaxis - no randomised trial exists (and one is neither ethical nor practical given the low seroconversion rate)
- The pivotal case-control study found HIV transmission was strongly associated with DEEP injury (odds ratio 15), VISIBLE BLOOD on the device (odds ratio 6.2), a needle that had been in the source's blood vessel (odds ratio 4.3), and a TERMINALLY ILL source (odds ratio 5.6)
- Workers who took zidovudine after exposure had markedly lower odds of seroconversion (odds ratio 0.19, an approximately 81 percent reduction in transmission)
- Three-drug regimens caused more adverse events than two-drug regimens, but discontinuation rates were similar
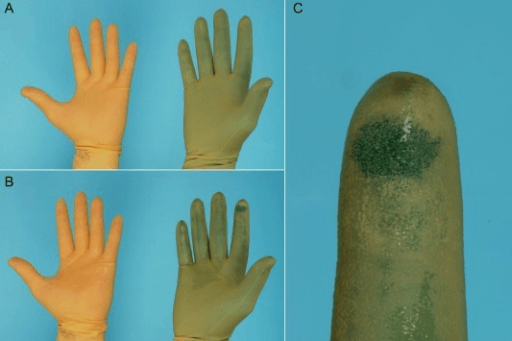
Double Gloving as Self-Protection in Surgery (Randomised Controlled Trial)
- Randomised controlled trial of 400 glove barriers worn by surgeons and assistants during consecutive abdominal operations
- Single gloves perforated in 20 percent of cases, but BOTH layers of a double-glove set were breached in only 4 percent (a fivefold reduction; p less than 0.001)
- Perforations were more common on the non-dominant hand, with longer operations, and with more senior operating roles
- Reducing inner-glove perforation directly reduces the episodes in which blood could pass between patient and surgeon
Efficacy of Double Gloving and Through-and-Through Perforation (Controlled Study)
- Controlled study of 1,536 surgical gloves (512 single, 1,024 double) tested for perforation by air-insufflation and water-leak methods
- Overall glove perforation rate was about 15 percent, highest among trainees and in deep general-surgery procedures, with the index finger most often involved
- Even when the outer glove of a double set was perforated, a through-and-through puncture reaching the inner glove occurred in only about 1 percent
- Double gloving provided greater than 98 percent protection against the inner glove being breached when the outer glove was punctured