Three-Layer Structure | Fiber Classification | Action Potential | Injury Grading | Wallerian Degeneration
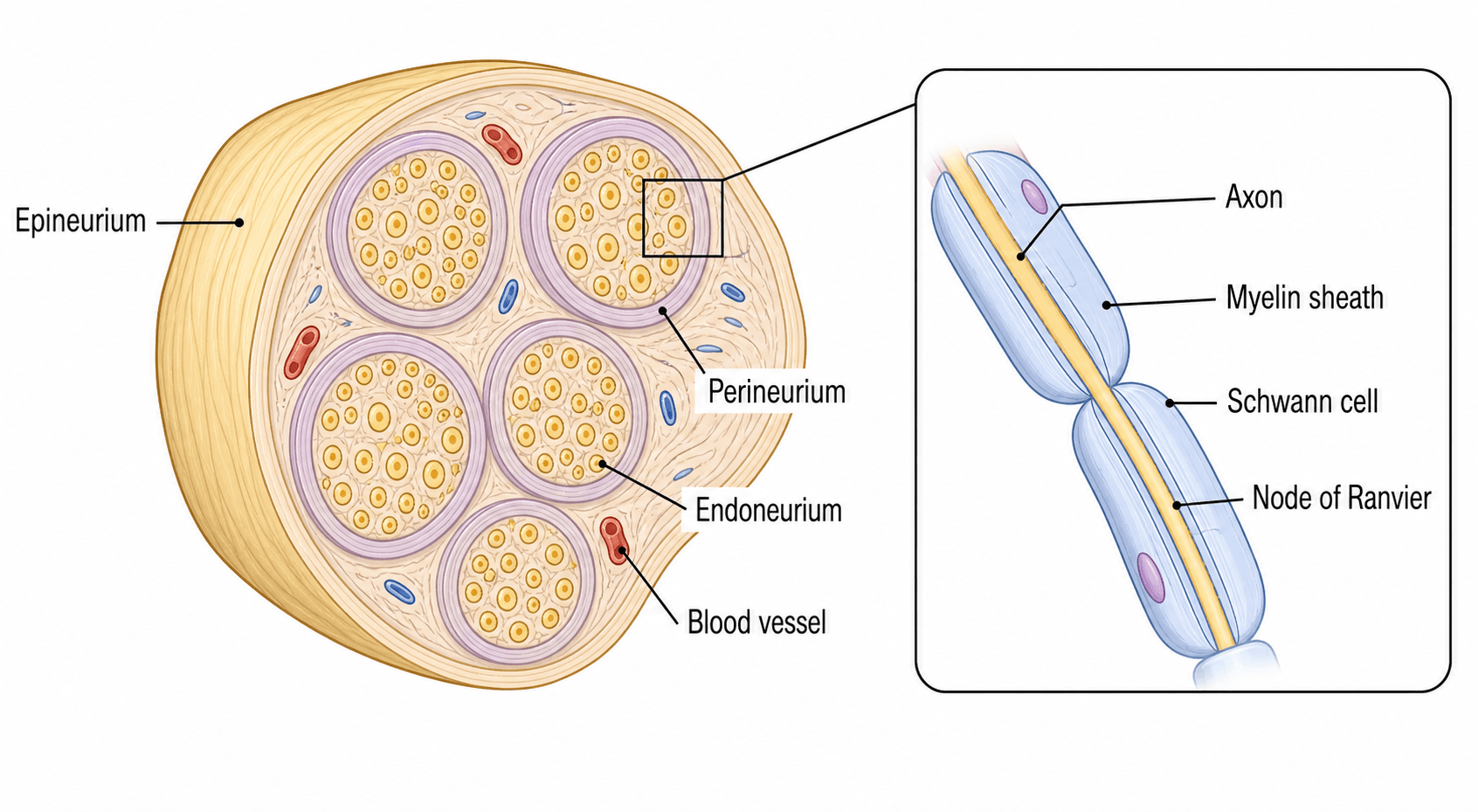
- Three-layer structure: Epineurium (outer), perineurium (surrounds fascicles), endoneurium (within fascicles)
- A-alpha fibers (largest, myelinated) conduct motor signals at 70-120 m/s; C fibers (unmyelinated) conduct pain at 0.5-2 m/s
- Action potential requires sodium influx (depolarization) then potassium efflux (repolarization); threshold is -55mV
- Wallerian degeneration occurs distal to injury within 24-48 hours; proximal stump regenerates at 1-3mm/day
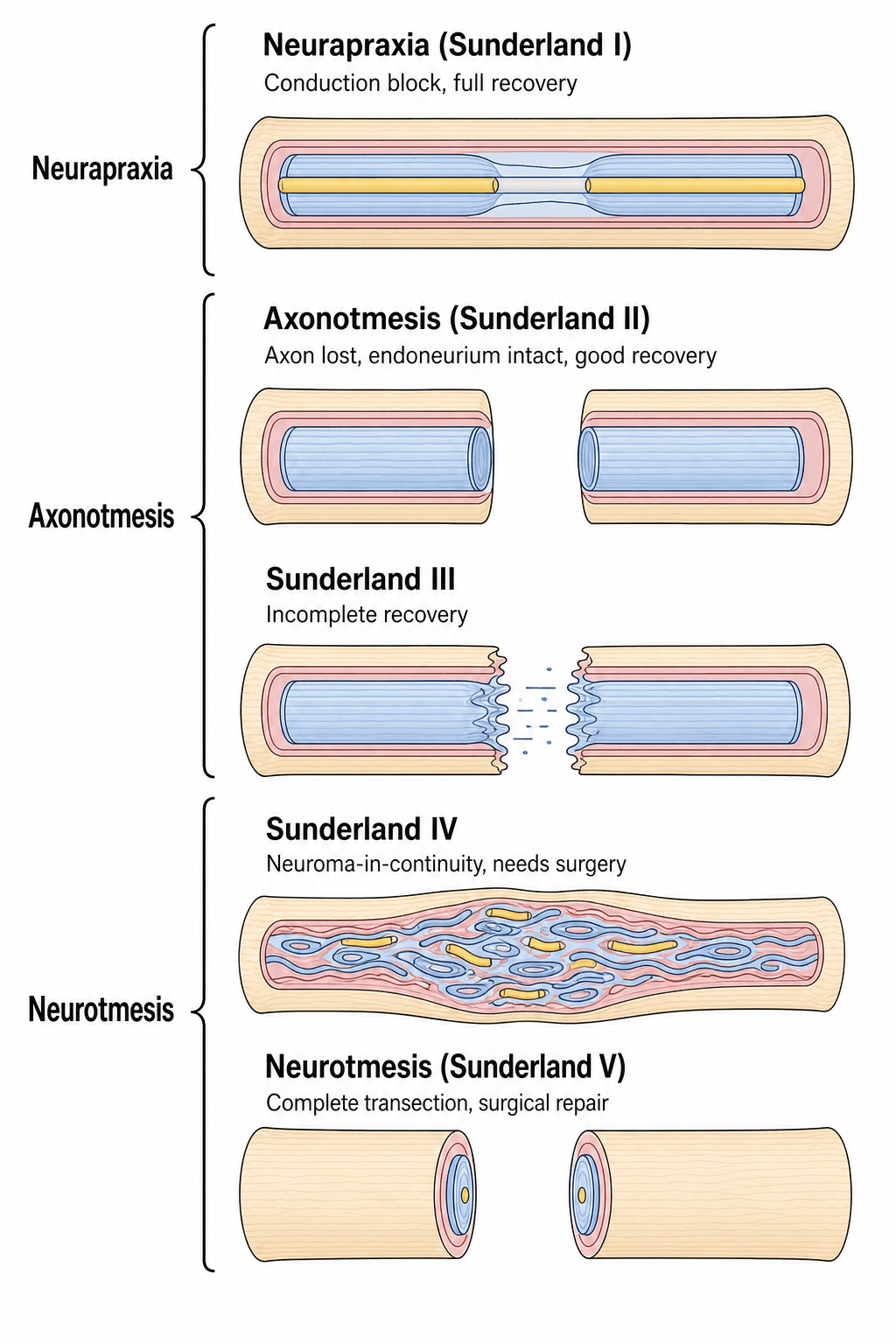
- Sunderland Grade III (endoneurial disruption) may not recover without surgery despite intact nerve sheath
- “Nerve fibers classified by diameter (Erlanger-Gasser: A, B, C) or function (Lloyd: Ia, Ib, II, III, IV)
- “Nodes of Ranvier allow saltatory conduction - 50x faster than continuous conduction
- “Tinel's sign progression tracks regenerating axons advancing at 1mm/day
- “Second-degree injury (axonotmesis) recovers spontaneously; third-degree may require neurolysis
Epineurium (outer connective tissue sheath), perineurium (surrounds each fascicle, blood-nerve barrier), endoneurium (within fascicles, surrounds individual axons). Perineurium is critical for regeneration - intact perineurium allows axons to reach targets.
A-alpha (motor, proprioception, 70-120 m/s), A-delta (sharp pain, temperature, 5-30 m/s), C fibers (dull pain, 0.5-2 m/s). Larger diameter = faster conduction. Myelination increases speed 50-fold via saltatory conduction.
Distal axon degenerates within 24-48 hours after injury. Schwann cells phagocytose myelin debris and proliferate to form Bands of Büngner (regeneration tubes). Macrophages clear debris. Process complete by 3-4 weeks.
Grade I (neuropraxia) - conduction block, full recovery. Grade II (axon loss, intact endoneurium) - recovers. Grade III (endoneurial loss) - incomplete recovery. Grade IV (perineurium lost) - no recovery. Grade V (transection) - requires surgery.
Overview and Introduction
Peripheral nerves are complex structures that transmit electrical signals between the central nervous system and peripheral tissues. Understanding nerve anatomy and physiology is fundamental to managing nerve injuries and understanding neurological deficits in orthopaedic surgery.
Clinical relevance: Peripheral nerve injury is an uncommon but disabling complication of limb trauma. In a large European trauma registry, an associated peripheral nerve injury was recorded in approximately 3.3% of severely injured patients with upper-extremity involvement, clustering in young men after high-energy mechanisms (notably motorcycle trauma) and with humeral or forearm fractures. Accurate classification using the Seddon and Sunderland systems guides prognosis, the decision to observe versus explore, and the timing of repair.
Concepts and Mechanisms
Connective Tissue Layers
- Location
- Outermost sheath around entire nerve
- Function
- Mechanical protection, contains vasa nervorum
- Clinical Significance
- Preserved in neurolysis; provides suture purchase
- Location
- Surrounds each fascicle
- Function
- Blood-nerve barrier, ionic regulation
- Clinical Significance
- CRITICAL for regeneration - intact = good recovery
- Location
- Within fascicles, surrounds axons
- Function
- Collagen tubes (Schwann cell basement membrane)
- Clinical Significance
- Forms Bands of Büngner during regeneration
Epineurium:
- Composition: Loose areolar connective tissue, type I and III collagen, fibroblasts
- Thickness: Comprises 30-75% of nerve cross-sectional area
- Vascularity: Contains vasa nervorum (longitudinal vessels) and lymphatics
- Function: Mechanical protection, allows gliding, nutrient supply
- Clinical: Provides strength for suturing during repair
Perineurium:
- Composition: 7-15 concentric layers of flattened cells with tight junctions
- Function: Blood-nerve barrier (selective permeability), maintains endoneurial microenvironment
- Pressure: Maintains endoneurial fluid pressure at 2-8 mmHg
- Clinical: Critical for regeneration - intact perineurium guides axons to correct targets (Sunderland I-II vs III)
- Resistance: High electrical resistance prevents current leakage
Endoneurium:
- Composition: Type III collagen fibrils, Schwann cells, capillaries
- Structure: Forms tubes around individual axons (diameter 0.4-14 micrometers)
- Function: Mechanical support for axons, ion regulation, regeneration scaffold
- Clinical: Intact endoneurial tubes (Bands of Büngner) are critical for successful regeneration
- Fluid: Contains endoneurial fluid (nutrient transport)
Intact perineurium (Sunderland I-II) allows spontaneous recovery because axons regenerate within intact tubes to reach correct targets. Disrupted perineurium (Sunderland III-IV) leads to misdirected regeneration, neuroma formation, and poor functional recovery even if the nerve is in continuity.
Understanding the three layers explains why injury severity affects prognosis.
Nerve Fiber Types and Classification
Classification by Diameter and Speed
- Diameter (μm)
- 12-20
- Conduction Velocity (m/s)
- 70-120
- Myelination
- Heavy
- Function
- Motor, proprioception (Ia, Ib afferents)
- Diameter (μm)
- 6-12
- Conduction Velocity (m/s)
- 35-75
- Myelination
- Heavy
- Function
- Touch, pressure (mechanoreceptors)
- Diameter (μm)
- 4-8
- Conduction Velocity (m/s)
- 15-40
- Myelination
- Medium
- Function
- Motor to muscle spindles (fusimotor)
- Diameter (μm)
- 1-5
- Conduction Velocity (m/s)
- 5-30
- Myelination
- Light
- Function
- Sharp pain, temperature, crude touch
- Diameter (μm)
- 1-3
- Conduction Velocity (m/s)
- 3-15
- Myelination
- Light
- Function
- Preganglionic autonomic
- Diameter (μm)
- 0.2-1.5
- Conduction Velocity (m/s)
- 0.5-2
- Myelination
- None
- Function
- Dull pain, temperature, postganglionic autonomic
Key principles:
- Diameter determines speed: Larger diameter = faster conduction (less resistance)
- Myelination increases speed: Saltatory conduction 50x faster than continuous
- Clinical testing: Large fibers (vibration, proprioception) lost first in compression; small fibers (pain) lost last
- Regeneration: Large myelinated fibers regenerate faster than small unmyelinated fibers
Compression at two sites along a nerve causes additive impairment. Example: Cervical radiculopathy plus carpal tunnel syndrome. The first compression reduces axoplasmic flow, making distal segments vulnerable. Clinically, treating one site may not fully resolve symptoms.
Fiber classification explains differential susceptibility to injury and recovery patterns.
The classification above is of nerve FIBRES; the sensory END-ORGANS they supply are a distinct, frequently-examined basic-science topic. Know the four mechanoreceptors by depth, adaptation and modality:
- Meissner corpuscles - superficial dermal papillae; fast-adapting, low-threshold; light/moving touch and flutter; dense in fingertips for fine discrimination.
- Merkel cells/discs - basal epidermis; slow-adapting, low-threshold; sustained pressure, fine spatial detail and texture; with Meissner corpuscles they are the main contributors to two-point discrimination in the hand.
- Pacinian corpuscles - deep dermis/subcutis (onion-skin lamellae); fast-adapting, large receptive field; high-frequency vibration and deep pressure.
- Ruffini endings - dermis; slow-adapting; skin stretch, sustained pressure and joint position.
- Free nerve endings - pain (nociception) and temperature (A-delta and C fibres) and crude touch.
fast-adapting receptors signal change/movement and fall silent during a sustained stimulus (so you stop feeling your clothes), whereas slow-adapting receptors fire throughout a maintained stimulus (so you keep sensing a constant grip).
two-point discrimination (Merkel plus Meissner) and vibration (Pacinian/Meissner) testing assess large-fibre/end-organ function after nerve injury; protective sensation recovers before fine discrimination. Exam point: Meissner/Merkel = superficial, fine touch and 2PD; Pacinian = deep, vibration; Ruffini = stretch; free nerve endings = pain/temperature.
Action Potential and Nerve Conduction
Membrane Potential at Rest
Resting membrane potential: -70 mV (inside negative relative to outside)
Ionic basis:
- Sodium (Na+): High outside (140 mM), low inside (10 mM)
- Potassium (K+): High inside (140 mM), low outside (5 mM)
- Chloride (Cl-): High outside (110 mM), low inside (10 mM)
- Intracellular anions: Negatively charged proteins trapped inside
Maintenance mechanisms:
- Na+/K+-ATPase pump: Actively transports 3 Na+ out, 2 K+ in (uses ATP)
- Selective permeability: Membrane more permeable to K+ than Na+ at rest
- Potassium leak channels: Allow K+ to exit, creating negative inside
- Equilibrium potentials: ENa = +60 mV, EK = -90 mV, resting is between
Nernst equation (equilibrium potential for ion):
- E = (RT/zF) times ln([ion outside]/[ion inside])
- At body temperature: E = 61 mV times log([outside]/[inside]) / z
- Predicts voltage where ion flux is zero
Goldman-Hodgkin-Katz equation (membrane potential):
- Accounts for permeability to multiple ions (primarily K+, Na+, Cl-)
- Resting state: dominated by K+ permeability (Em approaches EK = -90 mV)
Hyperkalemia (high extracellular K+) reduces the concentration gradient, making resting potential less negative (depolarized). This partially inactivates Na+ channels, paradoxically reducing excitability and causing weakness. Severe hyperkalemia can cause cardiac arrest.
Understanding resting potential is fundamental to action potential generation.
Nerve Injury Classification
Clinical Three-Grade System
- Pathology
- Conduction block, myelin injury, axon intact
- Recovery
- Complete (100%)
- Time to Recovery
- Hours to 12 weeks
- Treatment
- Observation, expectant
- Pathology
- Axon disrupted, endoneurium intact
- Recovery
- Good to excellent (80-90%)
- Time to Recovery
- Months (1mm/day)
- Treatment
- Observation, may need neurolysis
- Pathology
- Complete nerve transection
- Recovery
- None without surgery
- Time to Recovery
- No recovery
- Treatment
- Surgical repair required
Neuropraxia:
- Mechanism: Focal demyelination (compression, ischemia, mild traction)
- Pathology: Myelin damaged, axon continuity preserved
- Electrophysiology: Conduction block at injury site; normal distal to block
- Recovery: Remyelination over days to weeks (Schwann cells repair)
- Example: Saturday night palsy (radial nerve compression)
Axonotmesis:
- Mechanism: Severe crush or traction (axon torn, sheath intact)
- Pathology: Wallerian degeneration distal to injury; endoneurium preserved
- Electrophysiology: No conduction distal after 3-5 days (degeneration complete)
- Recovery: Axonal regeneration at 1-3 mm/day through intact endoneurial tubes
- Outcome: Good recovery if target not too distant (reinnervation before atrophy)
- Example: Closed humeral shaft fracture with radial nerve palsy
Neurotmesis:
- Mechanism: Laceration, severe traction, high-energy trauma
- Pathology: Complete disruption of axons and connective tissue sheaths
- Electrophysiology: No recovery potential without surgical intervention
- Recovery: None unless surgically repaired (primary or secondary repair)
- Outcome: Incomplete recovery even with repair (misdirected axons, target muscle atrophy)
- Example: Open fracture with nerve transection, iatrogenic nerve laceration
Seddon classification is clinical (based on examination and mechanism), not histological. After closed injury, distinguish neuropraxia (observe) from neurotmesis (explore) using serial examination, electromyography (denervation after 3 weeks), and Tinel's sign (advancing = axonotmesis; non-advancing = possible neurotmesis).
Seddon classification guides initial clinical management decisions.
Wallerian Degeneration and Regeneration
Distal Axon Degeneration After Injury
Wallerian Degeneration Timeline
Axon severed. Distal segment sealed. Proximal segment retracts. Initial Ca2+ influx triggers calpain activation and cytoskeletal breakdown in distal axon.
Distal axon fragments (granular disintegration). Myelin breaks down into ovoids. Schwann cells detect injury (lose axonal contact, upregulate c-Jun transcription factor). Macrophages recruited to injury site.
Schwann cells phagocytose myelin debris (lipid-laden Schwann cells). Macrophages infiltrate and clear remaining debris. Endoneurial tubes persist (basement membrane intact).
Schwann cells proliferate rapidly. Form Bands of Büngner (columns of Schwann cells within endoneurial tubes). Upregulate neurotrophic factors (NGF, BDNF, GDNF). Express adhesion molecules (N-CAM, L1) to guide regenerating axons.
Debris clearance complete. Endoneurial tubes contain Schwann cell columns ready to support regeneration. If no regenerating axon arrives, Schwann cells eventually atrophy and tubes collapse (after 12-18 months).
Molecular mechanisms:
- Calcium influx: Activates calpains (proteases) causing axonal breakdown
- Ubiquitin-proteasome system: Degrades cytoskeletal proteins (neurofilaments, tubulin)
- Schwann cell dedifferentiation: Lose myelin phenotype, acquire repair phenotype
- Upregulation of c-Jun: Master transcription factor in Schwann cells for repair program
- Neurotrophic factors: NGF, BDNF, GDNF support regenerating axons
Clinical significance:
- Electrical conduction preserved: Distal axon conducts for 24-48 hours (useful for intraoperative nerve stimulation)
- Denervation changes on EMG: Appear at 2-3 weeks (fibrillations, positive sharp waves)
- Window for repair: Schwann cell support optimal for 12-18 months; declines thereafter (endoneurial tubes collapse)
Fibrillation potentials and positive sharp waves (spontaneous muscle fiber activity) appear 2-3 weeks after denervation. This is the time required for Wallerian degeneration to be complete and muscle fiber membrane to become unstable (upregulation of acetylcholine receptors). Do not expect EMG changes in first week after nerve injury.
Understanding Wallerian degeneration explains the timing of nerve repair and recovery.
The painful neuroma is the clinical face of failed regeneration, and its modern management is high-yield. A neuroma is a disorganised tangle of regenerating axons, Schwann cells and fibrous tissue that forms when regrowing axons fail to enter a distal endoneurial tube.
- End (terminal) neuroma: at the cut end of a transected nerve with no distal target - the classic painful amputation-stump neuroma.
- Neuroma-in-continuity: a fusiform swelling within an injured but non-transected nerve (Sunderland III-IV) where intrafascicular scar blocks/misdirects axons - the lesion that needs intra-operative nerve action potentials to decide resect-and-graft versus neurolysis.
a tender, often Tinel-positive nodule with shooting/burning pain in the nerve distribution, hypersensitivity, and (in amputees) prosthesis intolerance.
- Primary prevention: a tension-free, well-aligned repair gives axons a distal target; at amputation, traction neurectomy lets the cut end retract into healthy soft tissue away from the wound and weight-bearing surfaces.
- Established treatment: excise the neuroma and transpose/bury the proximal stump into muscle or bone, away from scar and load.
- Modern reconstructive approaches: targeted muscle reinnervation (TMR) - coapt the cut nerve to a nearby motor nerve/muscle so the axons have "somewhere to go" - and the regenerative peripheral nerve interface (RPNI) - wrap the nerve end in a free muscle graft. Both markedly reduce neuroma and phantom/residual-limb pain and are now standard in amputation surgery.
Exam point: a painful neuroma is regeneration with no distal target - give the axons a target (primary repair, TMR/RPNI) or bury the stump away from load.
Differential Diagnosis of Acute Limb Weakness or Sensory Loss
- Distribution / Pattern
- Single named-nerve territory (e.g. wrist drop with radial palsy)
- Key Distinguishing Feature
- Maps to one peripheral nerve; mechanism (fracture, laceration, compression)
- Confirmatory Test
- Nerve conduction studies / EMG; advancing Tinel's sign
- Distribution / Pattern
- Dermatomal/myotomal (single root)
- Key Distinguishing Feature
- Neck pain, radiation in a root pattern, positive Spurling test; reflex loss for that root
- Confirmatory Test
- MRI cervical spine; EMG showing paraspinal involvement
- Distribution / Pattern
- Multiple nerves / whole limb, may be pan-plexal
- Key Distinguishing Feature
- High-energy traction (motorcycle); Horner sign suggests root avulsion
- Confirmatory Test
- MRI / CT myelography; EMG; clinical pattern
- Distribution / Pattern
- Regional, pain out of proportion, passive-stretch pain
- Key Distinguishing Feature
- Tense compartment, pain dominates early; sensory then motor loss late
- Confirmatory Test
- Compartment pressure measurement (clinical diagnosis)
- Distribution / Pattern
- Whole limb distal to occlusion
- Key Distinguishing Feature
- Pulseless, pale, cold, paraesthesia and paralysis (the 6 Ps)
- Confirmatory Test
- Doppler / angiography
- Distribution / Pattern
- Hemibody, often face involved, upper motor neuron signs
- Key Distinguishing Feature
- Upper motor neuron pattern, hyperreflexia, no peripheral nerve mapping
- Confirmatory Test
- CT/MRI brain
A focal peripheral nerve lesion maps to a single named-nerve territory and is confirmed electrodiagnostically; the critical step is to exclude compartment syndrome and acute arterial ischaemia, which are limb-threatening and demand emergency intervention rather than expectant nerve management.
Management Algorithm
Guidelines, Registries & Global Practice
Global Epidemiology
- Peripheral nerve injury (PNI) is an uncommon complication of limb trauma. In the European TraumaRegister DGU cohort of 49,382 severely injured patients with upper-extremity involvement, an associated nerve injury was present in approximately 3.3%.
- PNI clusters in young males (mean age approximately 40 years, around 79% male) and after high-energy mechanisms, with motorcycle accidents the single most common cause in that registry.
- Typical concomitant lesions are humeral (approximately 37%) and ulnar (approximately 20%) fractures, vascular laceration, and extensive soft-tissue damage; PNI roughly doubles inpatient rehabilitation need and lengthens hospital stay.
- In penetrating and ballistic trauma, nerve deficits are common (around 30% of upper-extremity gunshot injuries in one Level 1 trauma series) but are frequently neuropraxic or axonotmetic, with more than half improving spontaneously, supporting initial expectant management of nerve-in-continuity ballistic injuries.
- In limited-resource and conflict settings, blast and gunshot mechanisms predominate and the ulnar nerve is the most frequently injured peripheral nerve.
Classification and Decision Frameworks (Side by Side)
- What it standardises
- Severity grading of nerve injury
- Key recommendation
- Use Seddon for clinical/initial decisions; Sunderland five-degree (plus Mackinnon degree VI mixed) to predict recovery and need for surgery
- Evidence basis
- Foundational anatomical-pathological description; widely adopted worldwide
- What it standardises
- Diagnostic and repair principles
- Key recommendation
- Tension-free coaptation; early exploration of sharp/open transections; autograft or processed allograft for gaps not amenable to direct repair (conduits reserved for short sensory gaps under 25 mm)
- Evidence basis
- Expert consensus and cohort/registry data (e.g. RANGER)
- What it standardises
- Open injuries and nerve repair pathways
- Key recommendation
- Repair clean transections primarily within recommended timeframes; refer complex/closed lesions to specialist nerve units
- Evidence basis
- Standards for trauma and society guidance
- What it standardises
- Nerve in the context of fracture care
- Key recommendation
- Document neurology before and after reduction/fixation; observe most closed fracture-associated palsies; explore if iatrogenic or no recovery by expected window
- Evidence basis
- Educational consensus, observational evidence
- What it standardises
- Brachial plexus and reconstruction
- Key recommendation
- Early referral for traumatic plexus injury; favour nerve transfers for proximal injuries to shorten reinnervation distance
- Evidence basis
- Consensus plus cohort outcome data
Evidence-Based Reconstruction Principles (Global Consensus)
- Timing: clean, sharp transections are repaired primarily and early; closed fracture-associated palsies (e.g. radial nerve palsy with humeral shaft fracture) are usually observed because most are neuropraxia or axonotmesis that recover. Reconstruction should ideally occur within the 12-18 month window before motor endplates and repair Schwann cells degenerate.
- Repair ladder by gap: direct tension-free coaptation is preferred; hollow conduits are reserved for short sensory gaps (typically under 25 mm) in low-demand nerves; processed nerve allograft has registry support for digital nerve gaps of 25-50 mm (around 86% meaningful sensory recovery); autograft (sural nerve) remains the reference standard for longer or critical motor/mixed nerves.
- Nerve transfers (e.g. double fascicular Oberlin-type transfer for elbow flexion, spinal accessory to suprascapular nerve) shorten the distance from coaptation to target muscle and have improved outcomes in proximal and brachial plexus injuries.
- Electrodiagnostics: nerve conduction studies and needle EMG are timed at 2-3 weeks or later after injury, when denervation changes (fibrillations, positive sharp waves) appear; intraoperative nerve action potentials help decide between neurolysis and resection-grafting for a nerve-in-continuity.
Practice Variation and Resource Setting
- High-resource settings: ready access to microsurgery, intraoperative neuromonitoring, processed allograft and conduits, and specialist peripheral-nerve and brachial-plexus units; increasing use of nerve transfers.
- Limited-resource and conflict settings: predominance of blast/gunshot injuries, delayed presentation, reliance on autograft and tendon transfers rather than commercial conduits/allograft, and emphasis on rehabilitation and protective sensory retraining.
- Across all settings, hand therapy and structured rehabilitation (sensory re-education, prevention of contracture, protective sensation education) are integral to functional outcome.
Exam Relevance (All Boards)
- Nerve anatomy and physiology is a core basic-science topic for FRCS (Tr & Orth), FRACS, EBOT, ABOS, DNB/MS and MRCS candidates.
- Examiners commonly test the three-layer architecture, the ionic basis of the action potential and saltatory conduction, and the Seddon/Sunderland classifications with their clinical implications.
- The highest-yield distinction is Sunderland degree II (good prognosis) versus degree III (poor prognosis) in a nerve that appears in continuity, and the use of intraoperative nerve action potentials to resolve it.
MCQ Practice Points
Q: What are the five grades of the Sunderland nerve injury classification?
A: Grade I (neurapraxia): Local conduction block, myelin injury, full recovery weeks. Grade II (axonotmesis): Axon damage, endoneurium intact, full recovery months. Grade III: Endoneurium damaged. Grade IV: Perineurium damaged. Grade V (neurotmesis): Complete transection. Grades III-V require surgical intervention.
Q: What is the rate of nerve regeneration after injury?
A: Peripheral nerves regenerate at approximately 1mm/day or 1 inch/month. This guides timing expectations for motor recovery. Sunderland Grade II injuries recover at this rate once Wallerian degeneration completes (~3 weeks). More proximal injuries take longer due to greater distance to end organs.
Q: What is Wallerian degeneration?
A: Wallerian degeneration is the organized process of distal nerve segment breakdown following axonal injury. Begins within 24-48 hours, completes by 3 weeks. Involves axon fragmentation, myelin breakdown, and Schwann cell proliferation forming Bands of Büngner to guide regenerating axons. Essential for successful regeneration.
Q: What are the structural layers of a peripheral nerve from inside to outside?
A: From inside out: Axon (nerve fiber), Endoneurium (surrounds individual axons), Perineurium (surrounds fascicles - creates blood-nerve barrier), Epineurium (outermost layer surrounding nerve trunk). The internal epineurium fills space between fascicles. Understanding crucial for nerve repair technique.
Q: What determines nerve conduction velocity?
A: Myelination and axon diameter are primary determinants. Large myelinated fibers (Aα) conduct at 70-120 m/s (motor, proprioception). Small unmyelinated C fibers conduct at 0.5-2 m/s (pain, temperature). Saltatory conduction between nodes of Ranvier enables rapid transmission in myelinated fibers.
At a Glance
Peripheral nerves have a three-layer architecture: epineurium (outer connective tissue), perineurium (surrounds fascicles, forms blood-nerve barrier), and endoneurium (within fascicles, guides regeneration). Fibre classification correlates diameter with function: A-alpha fibres (largest, motor, 70-120 m/s), while C fibres (unmyelinated pain, 0.5-2 m/s). The Sunderland classification grades nerve injury I-V based on which layers are disrupted - Grade I (conduction block) recovers fully, while Grade V (complete transection) requires surgical repair. Wallerian degeneration begins distally within 24-48 hours; regeneration occurs at 1-3mm/day from the proximal stump.
NERVENERVE - Three-Layer Structure
Hook:NERVE layers from outside to inside: Epi-Peri-Endo (like EPE for protection)
ABCDABCD - Nerve Fiber Classification
Hook:A-B-C-D: Alphabetical order = decreasing speed and diameter
WATERWATER - Wallerian Degeneration Steps
Hook:WATER flowing away: Wallerian degeneration flows distal to injury site
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the anatomical structure of a peripheral nerve. What are the three connective tissue layers and their functions?”
“Explain the generation and propagation of an action potential in a myelinated nerve fiber. What is saltatory conduction?”
“A patient has a closed humeral shaft fracture with radial nerve palsy noted immediately after injury. Classify nerve injuries and describe the process of Wallerian degeneration.”
Three-Layer Structure
- Epineurium: outer loose connective tissue, vasa nervorum, 30-75% cross-section, mechanical protection
- Perineurium: 7-15 cell layers with tight junctions, blood-nerve barrier, maintains ionic environment
- Endoneurium: collagen tubes around axons within fascicles, forms Bands of Büngner
- Perineurium critical: intact (Sunderland I-II) = good recovery; disrupted (III-IV) = poor recovery
Nerve Fiber Classification
- A-alpha: largest (12-20 μm), fastest (70-120 m/s), motor and proprioception
- A-beta: medium (6-12 μm), 35-75 m/s, touch and vibration
- A-delta: small (1-5 μm), 5-30 m/s, sharp pain and temperature
- C fibers: smallest (0.2-1.5 μm), slowest (0.5-2 m/s), dull pain (unmyelinated)
- Large fibers most vulnerable to compression; small fibers most resistant
Action Potential
- Resting potential: -70 mV (Na+/K+-ATPase maintains gradients)
- Threshold: -55 mV triggers voltage-gated Na+ channels
- Depolarization: Na+ influx to +40 mV (0.5-1 ms)
- Repolarization: K+ efflux returns to -70 mV (1-2 ms)
- Absolute refractory: 0.5-1 ms (Na+ channels inactivated)
- Saltatory conduction: action potential jumps node to node (50x faster than continuous)
Seddon Classification
- Neuropraxia: conduction block, myelin injury, axon intact, full recovery (hours to 12 weeks)
- Axonotmesis: axon disrupted, endoneurium intact, good recovery at 1 mm/day
- Neurotmesis: complete transection, no recovery without surgery
Sunderland Classification
- Grade I: myelin only (neuropraxia), complete recovery
- Grade II: axon + myelin, endoneurium intact, excellent recovery (90%)
- Grade III: axon + endoneurium disrupted, perineurium intact, variable recovery (50-80%), may need neurolysis
- Grade IV: only epineurium intact, poor recovery (less than 25%), needs grafting
- Grade V: complete transection, requires surgical repair
- Mackinnon Grade VI: mixed injury (different grades in different fascicles)
Wallerian Degeneration
- Distal axon degenerates 24-48 hours after injury
- Schwann cells phagocytose debris, form Bands of Büngner (1-4 weeks)
- Bands of Büngner: Schwann cell columns guide regenerating axons
- Neurotrophic factors: NGF, BDNF, GDNF support regeneration
- EMG denervation changes (fibrillations) appear at 2-3 weeks
- Window for repair: 12-18 months (optimal Schwann support and muscle endplate viability)
Axonal Regeneration
- Regeneration rate: 1-3 mm/day (average 1 mm/day clinically)
- Initial delay: 3-4 weeks (growth cone formation, crossing scar)
- Tinel's sign: tracks advancing regeneration (percussion causes tingling)
- Factors for good recovery: young age, distal injury, sharp laceration, early repair (less than 3 months)
- Factors for poor recovery: proximal injury, crush/avulsion, delayed repair (greater than 12 months)
Evidence Base
Anatomy and Physiology of Nerve Injury (Sunderland's Five-Degree System)
- Microstructure of nerve trunks underpins a five-degree classification of injury severity, with partial and mixed types each having defined pathology and clinical features
- Tensile strength and capacity to resist traction reside in the fascicular (perineurial) tissue; the epineurium provides a cushion against compression
- Fascicular plexuses redistribute and mix branch fibres along the nerve, complicating fascicular matching at repair
- After transection, changes in axons, endoneurial tubes, fasciculi and the nerve trunk together determine the outcome of regeneration
Double Crush in Nerve Entrapment Syndromes
- Original description of the double crush hypothesis: a single axon compressed at two sites is more vulnerable than at either site alone
- Proposed that proximal impairment of axoplasmic flow renders distal segments susceptible to a second compression
- Frequently invoked for coexisting cervical radiculopathy and carpal tunnel syndrome
- Predicts that treating only one compression site may not fully resolve symptoms
Repair Schwann Cell, c-Jun and Bands of Büngner
- Nerve injury reprograms myelin and Remak Schwann cells into a dedicated repair phenotype that supports neuronal survival and axon regrowth
- Repair cells up-regulate trophic factors and cytokines, drive myelin clearance (autophagy and macrophage recruitment), and form Bands of Büngner to guide axons
- This repair programme is controlled transcriptionally by c-Jun, rapidly up-regulated after injury
- Without c-Jun, a dysfunctional repair cell forms, leading to neuronal death and failure of functional recovery
Double Nerve Transfer for Elbow Flexion (Oberlin Plus)
- Double fascicular transfer (ulnar fascicle to biceps motor branch plus median fascicle to brachialis branch) for upper-trunk brachial plexus palsy
- Grade 4 (MRC) elbow flexion restored in all 10 patients with adequate follow-up
- Patients could lift 1-5 kg with no secondary loss of grip strength or sensation
- Distal donor-to-target coaptation shortens reinnervation distance compared with proximal repair or grafting
Processed Nerve Allograft for Digital Nerve Gaps (RANGER Registry)
- Fifty digital nerve repairs with gaps of 25-50 mm (mean 35 mm) reconstructed with processed nerve allograft
- Meaningful recovery (MRC S3 or greater) achieved in 86% of repairs
- Results compared favourably with historical autograft recovery (reported 60-88%) without donor-site morbidity
- Processed allograft extends the gap range previously reserved for autograft, beyond the under-25 mm limit of hollow conduits
Peripheral Nerve Injury in Severe Upper-Limb Trauma (TraumaRegister DGU)
- Among 49,382 severely injured patients with upper-extremity involvement, 3.3% had an associated peripheral nerve injury
- Nerve-injured patients were younger (mean 40.6 versus 47.2 years) and more often male (78.6%)
- Motorcycle accidents were the single most common mechanism (32.5%); humeral (37.2%) and ulnar (20.3%) fractures were the typical concomitant lesions
- Nerve injury was associated with longer hospital stay (30.6 versus 24.2 days) and greater need for inpatient rehabilitation