RYR1 Channelopathy | Hypermetabolic Crisis | Dantrolene Rescue | Orthopaedic Relevance
- RYR1 gene mutation causes uncontrolled sarcoplasmic Ca2+ release from skeletal muscle SR
- Triggers: ALL volatile agents (sevoflurane, desflurane, isoflurane, halothane) and suxamethonium
- Earliest signs: rising EtCO2 (unexplained), tachycardia, masseter rigidity
- Dantrolene: 2.5 mg/kg IV bolus, repeat every 5 min up to 10 mg/kg, then 1 mg/kg every 6 hours
- Total IV anaesthesia (TIVA) with propofol is safe in MH-susceptible patients
- Malignant hyperthermia is a clinical diagnosis: treat FIRST, investigate LATER
- “Rising EtCO2 with no change in ventilation is the cardinal early sign
- “Masseter muscle rigidity after suxamethonium may herald MH - stop triggers immediately
- “Dantrolene works by inhibiting RYR1-mediated Ca2+ release, not by central action
- “Hyperkalaemia, not hyperthermia, is the principal cause of early cardiac arrest in MH
Rising EtCO2 is the most sensitive and specific early sign. Unexplained tachycardia follows. Masseter rigidity after suxamethonium is a warning sentinel. Temperature rise is a LATE sign - do not wait for it.
ALL volatile anaesthetic agents (sevoflurane, desflurane, isoflurane, halothane, enflurane). Suxamethonium (succinylcholine). Safe agents: propofol, nitrous oxide, local anaesthetics, opioids, benzodiazepines, non-depolarising muscle relaxants.
Reconstitute and give IMMEDIATELY. Dose: 2.5 mg/kg IV bolus. Repeat every 5 min (max cumulative 10 mg/kg). Then 1 mg/kg every 6-12 h for 24-48 h. Each vial contains 20 mg; a 70 kg patient needs 9 vials for the first dose alone.
Long cases, tourniquet use, and repetitive suxamethonium dosing raise MH risk. Orthopaedic patients with undiagnosed myopathies (e.g. Duchenne, Becker) are at elevated risk. Surgeons must recognise the intraoperative crisis and support anaesthetic management.
- Diagnosis
- Probable evolving MH crisis
- Immediate Action
- STOP volatile agent, hyperventilate with 100% O2, give dantrolene 2.5 mg/kg IV
- Key Pearl
- Do NOT wait for temperature rise
- Diagnosis
- Sentinel MH event (may be isolated or prodrome)
- Immediate Action
- Abandon intubation attempt, switch to non-triggering technique, monitor closely
- Key Pearl
- Up to 50% of masseter rigidity cases progress to fulminant MH
- Diagnosis
- Fulminant MH crisis
- Immediate Action
- Dantrolene IV maximum dose, active cooling, treat hyperkalaemia, ICU
- Key Pearl
- Mortality rises dramatically with delayed dantrolene
CHOPPEDRecognising Malignant Hyperthermia
Hook:CHOPPED by volatile agents - the anaesthetic chops down the calcium gate!
SAFE-TRIGGERSSafe vs Unsafe Agents in MH-Susceptible Patients
Hook:SAFE-TRIGGERS tells you what is safe and what triggers MH!
Overview and Epidemiology
Malignant hyperthermia (MH) is a pharmacogenetic disorder of skeletal muscle presenting as a hypermetabolic crisis when a genetically susceptible individual is exposed to volatile anaesthetic agents or suxamethonium. Although primarily managed by anaesthetists, orthopaedic surgeons must recognise the crisis, support resuscitation, and understand which of their patients carry elevated risk - particularly those with undiagnosed myopathies (Duchenne, Becker) who may present for orthopaedic procedures. MH remains a core basic science viva topic across FRCS, FRACS, and ABOS examinations.
- Incidence: approximately 1 in 100,000 adult anaesthetics involving volatile agents; higher in children (1 in 30,000)
- Mortality: less than 5% with prompt dantrolene treatment; historically 70-80% before dantrolene
- Genetics: autosomal dominant with variable penetrance; RYR1 mutations account for approximately 70% of cases; CACNA1S mutations approximately 1%
- Sex: males more frequently affected (higher muscle mass amplifies the hypermetabolic response)
- Long surgical cases: prolonged volatile exposure increases risk
- Myopathy patients: Duchenne and Becker muscular dystrophy carry elevated MH-like risk (distinct mechanism but overlapping crisis)
- Tourniquet use: may mask or delay recognition of limb rigidity
- Scoliosis surgery: neuromuscular scoliosis patients (e.g. Duchenne) are a high-risk group
- Post-operative pain: opioid-safe analgesia is important; regional techniques preferred
Pathophysiology
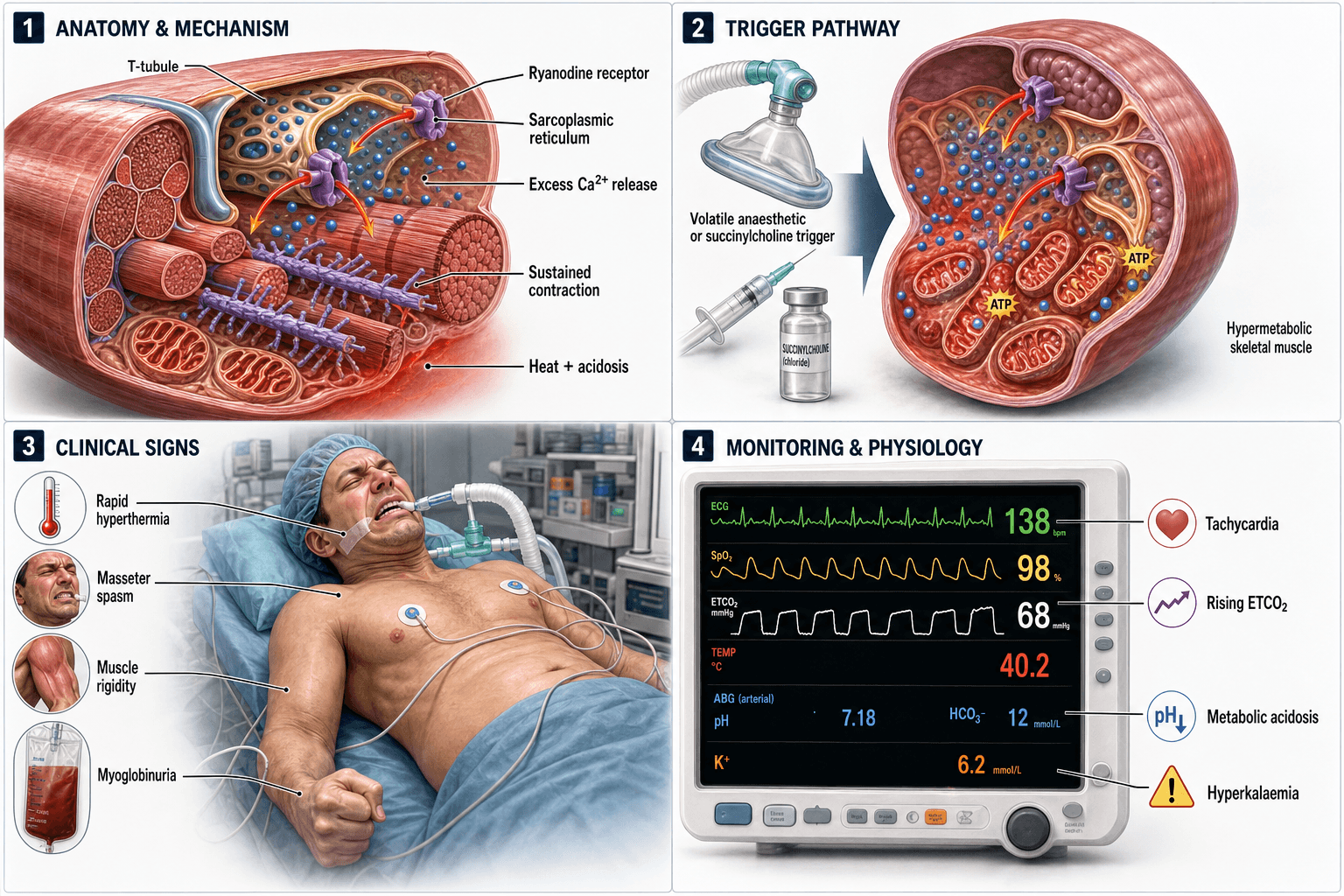
Malignant hyperthermia results from a defect in the ryanodine receptor type 1 (RYR1), the major calcium release channel of the sarcoplasmic reticulum (SR) in skeletal muscle. In normal physiology, depolarisation of the motor endplate activates dihydropyridine receptors (DHPR) on the T-tubule membrane, which mechanically couple to RYR1, triggering brief Ca2+ release from the SR. SERCA pumps then actively sequester Ca2+ back into the SR, restoring baseline. In MH-susceptible individuals, RYR1 mutations render the channel hyper-responsive to triggering agents: volatile anaesthetics and suxamethonium cause prolonged, uncontrolled Ca2+ release. The result is sustained myofibrillar contraction (rigidity), massive ATP consumption, and a hypermetabolic cascade producing heat, CO2, lactate, and potassium.
- Event
- Volatile agent or suxamethonium binds RYR1 complex
- Clinical Correlate
- Onset: within minutes of exposure
- Time Course
- Minutes to hours
- Event
- RYR1 channel locked open, massive SR calcium efflux
- Clinical Correlate
- Masseter rigidity, then generalized muscle rigidity
- Time Course
- 5-30 minutes
- Event
- ATP consumed by SERCA and myosin ATPase at extreme rates
- Clinical Correlate
- Rising EtCO2, tachycardia, metabolic acidosis
- Time Course
- 10-40 minutes
- Event
- Muscle contraction generates heat; impaired thermoregulation
- Clinical Correlate
- Core temperature rising up to 1-2 degrees Celsius every 5 min
- Time Course
- 15-60 minutes
- Event
- ATP depletion causes membrane failure; Ca2+ overload activates proteases
- Clinical Correlate
- Hyperkalaemia, CK rise, myoglobinuria, DIC
- Time Course
- 30-90 minutes
- Event
- Arrhythmias from hyperkalaemia; renal failure from myoglobin; cerebral oedema
- Clinical Correlate
- Cardiac arrest, acute kidney injury, compartment syndrome
- Time Course
- Hours
RYR1 gene (chromosome 19q13.2): encodes the ryanodine receptor type 1
- Over 400 variants identified; approximately 30 are causally linked to MH
- Autosomal dominant inheritance with variable penetrance
- Most common pathogenic variants: R614C, G2434R, R2163C, T2206M
CACNA1S gene (chromosome 1q32.1): encodes the DHPR alpha-1 subunit
- Less common (approximately 1% of cases)
- Links the voltage sensor to RYR1 opening
Inheritance: 50% chance of transmission to offspring; however, penetrance is variable and many mutation carriers never develop a crisis
- No diagnostic histological features on routine H+E staining in MH-susceptible muscle
- In vitro contracture test (IVCT): European protocol exposes fresh muscle biopsy strips to halothane and caffeine; a positive contracture confirms susceptibility
- North American protocol (CHCT): similar principle with caffeine-halothane contracture test
- Central core disease: a myopathy caused by RYR1 mutations that is strongly associated with MH susceptibility - key exam link
- Multi-minicore disease: another RYR1-related myopathy with MH risk
MH susceptibility is not confined to the operating theatre. Two examinable associations extend the RYR1 spectrum:
- King-Denborough syndrome: a rare congenital RYR1-related myopathy with characteristic dysmorphism (short stature, webbed neck, low-set ears, ptosis, pectus deformity, cryptorchidism, skeletal abnormalities) and strong MH susceptibility - a recognisable syndromic flag that the child is at high anaesthetic risk.
- Awake / exertional phenotypes: certain RYR1 variants predispose not only to anaesthetic MH but to exertional heat illness / heat stroke and exertional (and statin- or fever-related) rhabdomyolysis with no anaesthetic trigger at all. A personal or family history of unexplained exertional collapse, heat stroke, or recurrent rhabdomyolysis should raise the possibility of underlying MH susceptibility and prompt the same trigger-free anaesthetic precautions.
Together with central core disease and multi-minicore disease (the classic RYR1 myopathies), these define a continuum of RYR1-related disease in which the same channel defect manifests as myopathy, anaesthetic MH, and/or exertional crises.
Classification and Types
Patterns of MH Presentation
- Onset
- Rapid (minutes)
- Key Features
- Generalised rigidity, hyperthermia greater than 39 degrees, rapid EtCO2 rise, arrhythmias
- Outcome
- High mortality if dantrolene delayed
- Onset
- Gradual (20-60 min)
- Key Features
- Slow EtCO2 rise, unexplained tachycardia, mild acidosis
- Outcome
- Good outcome if recognised early
- Onset
- PACU recovery
- Key Features
- Rigidity, fever, dark urine, cardiac instability in recovery
- Outcome
- Often initially misdiagnosed as sepsis
- Onset
- After suxamethonium
- Key Features
- Jaw clonus/rigidity preventing intubation, with or without progression
- Outcome
- 50% progress to MH; observe minimum 12 hours
- Onset
- Variable
- Key Features
- Mild symptoms that self-resolve when trigger withdrawn
- Outcome
- Must still investigate for MH susceptibility
Not every MH episode follows a textbook cascade. The clinical picture ranges from mild abortive episodes to fulminant crisis.
Clinical Assessment
- Rising EtCO2: unexplained increase despite unchanged ventilation settings (most sensitive sign)
- Tachycardia: unexplained, often the first vital sign change
- Masseter rigidity: jaw stiffness after suxamethonium administration
- Mixed respiratory and metabolic acidosis: on blood gas analysis
- Tachypnoea: if spontaneously breathing
- Generalised skeletal muscle rigidity: trunk and limbs
- Hyperthermia: core temperature rising 1-2 degrees Celsius every 5 min; may exceed 40 degrees
- Dark urine: myoglobinuria (cola-coloured)
- Cardiac arrhythmias: ventricular tachycardia/fibrillation from hyperkalaemia
- Skin mottling, sweating, cyanosis
Hyperthermia is NOT an early sign of MH. By the time core temperature is significantly elevated, the hypermetabolic crisis is well established. Waiting for fever to make the diagnosis delays life-saving treatment. The earliest signs are rising EtCO2 and unexplained tachycardia in a patient receiving a volatile agent.
- Expected Change
- Markedly elevated (doubling or more)
- Mechanism
- Massive CO2 production from hypermetabolism
- Clinical Significance
- Most sensitive real-time indicator
- Expected Change
- Mixed respiratory and metabolic acidosis
- Mechanism
- CO2 accumulation + lactic acidosis
- Clinical Significance
- Base deficit greater than 8 suggests evolving crisis
- Expected Change
- Elevated (may be markedly high)
- Mechanism
- Muscle cell lysis releases intracellular K+
- Clinical Significance
- Principal cause of cardiac arrhythmias and arrest
- Expected Change
- Massively elevated (greater than 20,000 U/L)
- Mechanism
- Skeletal muscle destruction
- Clinical Significance
- Peak at 12-24 hours; degree reflects rhabdomyolysis severity
- Expected Change
- Elevated; cola-coloured urine
- Mechanism
- Muscle breakdown product released into circulation
- Clinical Significance
- Risk of acute tubular necrosis and renal failure
- Expected Change
- Disseminated intravascular coagulation
- Mechanism
- Tissue factor release from damaged muscle
- Clinical Significance
- DIC is a late, life-threatening complication
When MH is suspected, the Larach Clinical Grading Scale provides a structured, largely retrospective estimate of how likely an adverse anaesthetic event truly was MH - useful for documentation, audit and deciding who needs susceptibility testing. It is not a real-time treatment trigger: in the acute setting you still treat on suspicion. Points are awarded across six "process" categories:
- Muscle rigidity (generalised rigidity; masseter rigidity).
- Muscle breakdown (raised CK; cola-coloured urine/myoglobinuria; marked hyperkalaemia).
- Respiratory acidosis (rapidly rising EtCO2; raised PaCO2).
- Temperature increase (rapid rise; inappropriately high core temperature).
- Cardiac involvement (unexplained tachycardia; ventricular arrhythmia).
- Family history - plus credit for rapid reversal of signs with dantrolene.
The summed raw score maps to an MH rank from 1 (almost never) to 6 (almost certain). The exam point: the CGS formalises the same clinical features you act on, and a high score after the event mandates referral for IVCT/genetic testing.
Investigations
Investigation Pathway
End-tidal CO2 monitoring: continuous; rapid rise is diagnostic
Core temperature monitoring: oesophageal, nasopharyngeal, or bladder
Arterial blood gas: metabolic and respiratory acidosis, hyperkalaemia, rising lactate
ECG: arrhythmia detection (peaked T-waves from hyperkalaemia)
Serum CK: baseline and serial; levels over 20,000 U/L confirm significant rhabdomyolysis
Serum and urine myoglobin: myoglobinuria indicates ongoing muscle destruction
Coagulation profile: fibrinogen, D-dimer, INR for DIC surveillance
Renal function: creatinine and urea for acute kidney injury
In vitro contracture test (IVCT): European MH Group protocol; fresh muscle biopsy exposed to halothane and caffeine in the laboratory; sensitivity approximately 99%, specificity approximately 94%
Caffeine-halothane contracture test (CHCT): North American MH Group equivalent
Genetic testing: targeted RYR1 and CACNA1S sequencing; identifies causative variant in approximately 70% of cases; if a pathogenic variant is found, family screening is possible without biopsy
The IVCT remains the gold standard for confirming MH susceptibility. It requires a fresh (not frozen) muscle biopsy specimen, typically from the vastus lateralis, performed in a specialised centre. Genetic testing is increasingly used first-line in families where a known pathogenic variant exists. A positive genetic test in a first-degree relative of a confirmed MH survivor is sufficient to label the patient MH-susceptible without biopsy.
- Sensitivity
- Approximately 99%
- Specificity
- Approximately 94%
- Invasive
- Yes - open muscle biopsy under local
- Availability
- Specialised MH centres only
- Sensitivity
- Approximately 97%
- Specificity
- Approximately 78%
- Invasive
- Yes - open muscle biopsy under local
- Availability
- Limited centres in North America
- Sensitivity
- Approximately 70% (identifies known variants only)
- Specificity
- High for known pathogenic variants
- Invasive
- No - blood sample
- Availability
- Widely available; cost decreasing
Management Algorithm
Immediate Management of MH Crisis
Goal: Stop the hypermetabolic cascade with dantrolene while providing supportive care
Treatment Protocol
STOP all volatile anaesthetic agents immediately
DO NOT give suxamethonium
Hyperventilate with 100% oxygen at high flow (greater than 10 L/min) to flush volatile agent
Call for help and request dantrolene immediately
Inform the surgeon - may need to abort or rapidly complete the procedure
Prepare: each 20 mg vial requires mixing with 60 mL sterile water (warmed if possible for faster dissolution)
Administer: 2.5 mg/kg IV bolus
Repeat: every 5 minutes until symptoms abate, up to cumulative 10 mg/kg
Note: a 70 kg adult needs approximately 9 vials for the initial dose alone; organise a team for rapid reconstitution
Active cooling: cold IV saline (4 degrees Celsius), surface cooling (ice packs to groins, axillae, neck), cold body cavity lavage if needed
Treat hyperkalaemia: calcium chloride 10 mL of 10% IV, insulin 10 units with 50 mL 50% dextrose, sodium bicarbonate 1-2 mmol/kg
Treat arrhythmias: standard ACLS algorithms; avoid calcium channel blockers (may worsen hyperkalaemia or interact with dantrolene)
Continue dantrolene: 1 mg/kg IV every 6-12 hours for 24-48 hours
ICU monitoring: minimum 24 hours observation for recrudescence
Serial labs: CK, K+, ABG, urine output, coagulation every 2-4 hours initially
Maintain urine output: target greater than 1-2 mL/kg/hour with IV fluids and mannitol to prevent myoglobin-induced renal failure
Dantrolene sodium works by directly inhibiting RYR1-mediated calcium release from the sarcoplasmic reticulum. It does NOT act centrally. It causes mild muscle weakness but does not produce full paralysis. Newer formulations (e.g. Ryanodex) allow reconstitution in much smaller volumes, dramatically speeding administration. The key exam fact: dantrolene is the ONLY specific treatment for MH and must be given as rapidly as possible.
DANTROLENEMH Treatment Steps
Hook:DANTROLENE spells the treatment - from first dose to post-crisis care!
Complications
- Incidence
- Principal early cause of death
- Risk Factors
- Severe rhabdomyolysis, delayed dantrolene
- Management
- ACLS with aggressive K+ lowering; calcium chloride, insulin/dextrose, bicarbonate
- Incidence
- Common in severe cases
- Risk Factors
- Myoglobinuria, hypovolaemia
- Management
- Aggressive IV fluids, mannitol, maintain urine output
- Incidence
- Late complication
- Risk Factors
- Massive tissue destruction, shock
- Management
- Blood product support, treat underlying cause
- Incidence
- In limbs with severe rhabdomyolysis
- Risk Factors
- Muscle oedema within fascial compartments
- Management
- Fasciotomies if compartment pressures elevated
- Incidence
- Severe cases with prolonged hypoxia
- Risk Factors
- Hyperthermia, hypotension, cardiac arrest
- Management
- Neurocritical care, targeted temperature management
- Incidence
- Approximately 20% of cases
- Risk Factors
- Inadequate dantrolene dosing or early cessation
- Management
- Resume full dantrolene protocol; ICU monitoring minimum 24 h
Although the condition is called "malignant hyperthermia," it is hyperkalaemia from rhabdomyolysis that causes the lethal cardiac arrhythmias in the early phase. Aggressive potassium management (calcium chloride for membrane stabilisation, insulin-dextrose for intracellular K+ shift, bicarbonate) is as critical as dantrolene itself. The hyperthermia reflects the hypermetabolic state but is not the primary cause of death.
Outcomes and Prognosis
- Expected Outcome
- Rapid resolution of hypermetabolism
- Complication Rate
- Low (less than 10%)
- Mortality
- Less than 2%
- Expected Outcome
- Moderate rhabdomyolysis, possible AKI
- Complication Rate
- Moderate (20-40%)
- Mortality
- Less than 5%
- Expected Outcome
- Severe rhabdomyolysis, DIC, multi-organ failure risk
- Complication Rate
- High (greater than 50%)
- Mortality
- 10-30%
- Expected Outcome
- Fulminant crisis, cardiac arrest likely
- Complication Rate
- Near universal
- Mortality
- Greater than 70%
Best prognosis: Early recognition (rising EtCO2), immediate dantrolene within 10 minutes, young healthy patient, abortive form
Poor prognosis: Delayed recognition, fulminant presentation, extreme hyperthermia (greater than 41 degrees), pre-existing myopathy, limited dantrolene availability
Key threshold: Dantrolene administration within 10 minutes of symptom onset is associated with near-zero mortality. Every 10-minute delay significantly increases mortality.
Guidelines, Registries & Global Practice
- Incidence: approximately 1 per 100,000 adult anaesthetics; 1 per 30,000 paediatric anaesthetics where volatile agents are used
- Geographic variation: incidence reporting varies by country and depends on anaesthetic practices (volatile vs TIVA use rates)
- Registries: North American MH Registry (MHAUS), European MH Group registry, Japanese MH registry, and Australian/New Zealand case reports contribute to global data
- Mortality: less than 5% with prompt dantrolene; historically 70-80% before dantrolene era
- High-resource settings: TIVA widely available, dantrolene stocked in all ORs, IVCT and genetic testing accessible, specialist MH centres for follow-up
- Limited-resource settings: volatile anaesthesia predominates (cheaper, simpler), dantrolene may not be immediately available, IVCT centres are scarce
- Critical gap: dantrolene availability varies enormously worldwide; some regions rely on Dan-Alarm or MHAUS hotline networks for guidance
- Universal principle: regardless of resources, early recognition (rising EtCO2) and stopping volatile agents saves lives even before dantrolene arrives
- Trigger avoidance
- All volatiles and suxamethonium contraindicated; propofol TIVA safe
- Dantrolene dosing
- 2.5 mg/kg bolus, repeat to 10 mg/kg; then 1 mg/kg q6h for 24-48h
- Testing strategy
- Genetic testing first if familial variant known; IVCT if not
- Trigger avoidance
- Identical trigger avoidance; Ryanodex (nanocrystalline dantrolene) approved and recommended for faster reconstitution
- Dantrolene dosing
- Same dosing; Ryanodex allows 250 mg/vial vs 20 mg/vial conventional
- Testing strategy
- CHCT (caffeine-halothane contracture test) is the biopsy standard; genetic testing complementary
- Trigger avoidance
- Aligns with EMHG guidance; dantrolene must be available within minutes in every OR
- Dantrolene dosing
- EMHG-aligned dosing
- Testing strategy
- Referral to one of the UK MH investigation units (Leeds, St George's) for IVCT
- Trigger avoidance
- Aligns with EMHG; mandatory dantrolene availability in all facilities providing general anaesthesia
- Dantrolene dosing
- EMHG-aligned dosing
- Testing strategy
- Referral to MH investigation units; genetic testing increasingly used first-line
There is no single global MH implant registry (as MH is a pharmacogenetic event, not a device-related condition). However, the North American MH Registry (maintained by MHAUS) and the European MH Group registry are the two largest databases capturing MH events, outcomes, and genotype-phenotype correlations. These registries demonstrated that mortality fell from approximately 70% in the 1970s to less than 5% with modern dantrolene protocols.
Dantrolene availability remains inconsistent worldwide. In many limited-resource settings, dantrolene is not stocked in every OR, and reconstitution time with conventional formulations (20 mg/vial requiring 60 mL sterile water each) is a significant barrier. Ryanodex (250 mg/vial, reconstitutes in seconds) addresses this but is not universally available. Orthopaedic surgeons operating in settings without guaranteed dantrolene access should advocate for its inclusion in OR emergency supplies.
Controversies & Areas of Uncertainty
Patients with Duchenne, Becker, and other myopathies develop rhabdomyolysis and hyperkalaemic cardiac arrest under volatile agents via membrane instability (absent or abnormal dystrophin) rather than RYR1 channelopathy. The clinical overlap with MH is significant, dantrolene is still used, but the underlying mechanism differs. This distinction is important for genetic counselling and family screening.
Genetic testing identifies a causative variant in only approximately 70% of MH-susceptible individuals because not all pathogenic variants have been characterised. A negative genetic test does NOT exclude MH susceptibility if clinical suspicion is high - IVCT is still required. The trend toward genetics-first testing is growing but the IVCT remains the definitive investigation when genetics is inconclusive.
The risk of recrudescence after an MH crisis is approximately 20%, typically occurring within 6-24 hours. Most guidelines recommend ICU observation for a minimum of 24 hours, but the optimal duration of continuing dantrolene (24 vs 48 hours) and the safe discharge threshold are not defined by randomised evidence.
Statins have been implicated in rare cases of drug-induced myopathy that may unmask or complicate MH susceptibility. The interaction between statin myopathy and MH risk is poorly characterised. Current guidance does not recommend stopping statins pre-operatively in MH-susceptible patients, but clinicians should be aware of the potential for additive myotoxicity.
MCQ Practice Points
Q: What is the molecular basis of malignant hyperthermia? A: MH is caused by mutations in the RYR1 gene (approximately 70% of cases) encoding the ryanodine receptor type 1 on the sarcoplasmic reticulum of skeletal muscle. These mutations render the calcium release channel hyper-responsive to volatile anaesthetic agents and suxamethonium, causing sustained uncontrolled Ca2+ efflux from the SR. The resulting hypermetabolism produces heat, CO2, lactate, and muscle cell lysis.
Q: What is the earliest and most sensitive sign of MH during anaesthesia? A: Rising end-tidal CO2 (EtCO2) despite unchanged ventilation settings. This reflects the massive CO2 production from skeletal muscle hypermetabolism. Unexplained tachycardia typically follows. Hyperthermia is a LATE sign and should not be awaited before initiating treatment.
Q: What is the dose and mechanism of dantrolene in MH? A: Dose: 2.5 mg/kg IV bolus, repeated every 5 minutes up to 10 mg/kg cumulative, then 1 mg/kg every 6-12 hours for 24-48 hours. Mechanism: dantrolene directly inhibits RYR1-mediated calcium release from the sarcoplasmic reticulum, breaking the hypermetabolic cascade. It does not act centrally. It causes mild muscle weakness but not full paralysis.
Q: Which anaesthetic agents are safe in MH-susceptible patients? A: Safe: propofol, all opioids, nitrous oxide, local anaesthetics, non-depolarising muscle relaxants (rocuronium, atracurium, vecuronium), benzodiazepines, ketamine. Unsafe (triggering): ALL volatile agents (sevoflurane, desflurane, isoflurane, halothane) and suxamethonium. The safest overall technique is total IV anaesthesia with propofol or regional anaesthesia.
Q: What is the inheritance pattern and genetic testing strategy for MH? A: Autosomal dominant with variable penetrance. RYR1 mutations account for approximately 70% of cases, CACNA1S approximately 1%. Genetic testing of RYR1/CACNA1S is offered first-line in families with a known proband variant. If no variant is identified, the in vitro contracture test (IVCT) on fresh muscle biopsy (vastus lateralis) is the gold standard diagnostic test with approximately 99% sensitivity.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are assisting at a total knee arthroplasty in a 55-year-old male under general anaesthesia with sevoflurane. Forty minutes into the case, the anaesthetist reports a rapidly rising end-tidal CO2 from 38 to 65 mmHg despite unchanged ventilation settings, unexplained tachycardia to 120 bpm, and the patient feels warm. What is your diagnosis and what do you do?”
“A 14-year-old boy with Duchenne muscular dystrophy (DMD) is scheduled for scoliosis correction. His anaesthetist asks your opinion on the risk of MH during the case. What are the specific risks, how should anaesthesia be conducted, and what preparations are mandatory?”
Pathophysiology
- RYR1 mutation (chromosome 19) causes uncontrolled Ca2+ release from skeletal muscle SR
- Triggers: ALL volatile agents + suxamethonium cause sustained channel opening
- Hypermetabolism: massive ATP consumption produces heat, CO2, lactate, K+
- Rhabdomyolysis and hyperkalaemia are the lethal downstream effects
Clinical Recognition
- Earliest: rising EtCO2 (most sensitive) + unexplained tachycardia
- Masseter rigidity after suxamethonium is a sentinel warning
- Late: generalised rigidity, hyperthermia, dark urine, arrhythmias
- Temperature rise is LATE - never wait for it before treating
Dantrolene Protocol
- 2.5 mg/kg IV bolus immediately, repeat every 5 min up to 10 mg/kg
- Mechanism: inhibits RYR1-mediated Ca2+ release (not central action)
- Then 1 mg/kg IV every 6-12 hours for 24-48 hours post-crisis
- Each 20 mg vial needs 60 mL sterile water; 70 kg patient needs 9 vials for first dose
Safe and Unsafe Agents
- UNSAFE: ALL volatiles (sevoflurane, desflurane, isoflurane, halothane) + suxamethonium
- SAFE: propofol, opioids, N2O, local anaesthetics, non-depolarising relaxants, benzodiazepines
- Safest technique: propofol TIVA or regional anaesthesia
- Machine preparation: remove vaporisers, flush circuit 20 min, replace CO2 absorber
Diagnosis and Testing
- Clinical diagnosis: treat first, investigate later
- IVCT (European) or CHCT (North American): gold standard on fresh muscle biopsy
- Genetic testing: RYR1/CACNA1S identifies approximately 70% of cases
- Autosomal dominant inheritance; 50% risk to first-degree relatives; offer family screening
Evidence Base and Key Trials
Malignant hyperthermia: a review
- Comprehensive review establishing RYR1 as the primary gene responsible for MH susceptibility
- Over 400 RYR1 variants identified, with approximately 30 confirmed causative
- Dantrolene reduces mortality from approximately 70% to less than 5%
- IVCT remains the diagnostic gold standard with approximately 99% sensitivity
Cardiac arrests and deaths associated with malignant hyperthermia in north america from 1987 to 2006
- Analysis of the North American MH Registry identifying risk factors for cardiac arrest and death
- Increased risk with greater than 6 hour delay between symptom onset and dantrolene administration
- Muscle rigidity at onset and extreme temperature elevation were independent predictors of mortality
- Body mass index and myopathy history were additional risk factors
Availability of dantrolene for the management of malignant hyperthermia crises: European Malignant Hyperthermia Group guidelines
- EMHG consensus guidelines on dantrolene availability and dosing for MH crisis management
- Confirmed dantrolene 2.5 mg/kg initial bolus with repeat dosing as the gold standard
- Recommended minimum 36 vials of conventional dantrolene be immediately available wherever general anaesthesia is administered
- Highlighted that reconstitution time is a critical barrier and nanocrystalline formulations address this
European Malignant Hyperthermia Group guidelines for investigation of malignant hyperthermia susceptibility
- Recommended genetic testing as first-line investigation in families with a known proband variant
- IVCT remains the gold standard when no familial variant is identified or genetic testing is inconclusive
- RYR1 screening identifies causative variants in approximately 70% of MH-susceptible individuals
- Defined criteria for interpreting IVCT results and classifying MH susceptibility