Assess Biology vs Mechanics | Rule Out Infection | Diamond Concept | CORA for Deformity
- Every nonunion is infected until proven otherwise - check CRP/ESR, intraoperative cultures
- Hypertrophic nonunion = good biology, needs stability (exchange nail or compression plate)
- Atrophic nonunion = poor biology, needs bone graft AND stability
- Diamond Concept: Scaffold + Cells + Signals + Stability (+ Vascularity)
- Strain theory: less than 2% strain for primary healing, 2-10% for secondary healing
- “Tibia is the most common long bone nonunion (poor soft tissue coverage)
- “Smoking cessation is non-negotiable for elective nonunion surgery
- “Exchange nailing works by reaming autograft effect + larger stiffer nail
- “Masquelet technique induces biological membrane over 6-8 weeks
Until proven otherwise. You must verify CRP/ESR and obtain intraoperative cultures (5+ samples) before proceeding with definitive metalwork or grafting. Missing an infection leads to catastrophic failure.
Treatment is fundamentally different. Hypertrophic (elephant foot callus) has good biology but needs stability. Atrophic (no callus, sealed canal) has no biology and needs graft PLUS fixation.
Non-negotiable for elective surgery. Smoking increases nonunion risk by 2.3x. Carbon monoxide causes hypoxia; nicotine inhibits neovascularisation. Will not operate electively on active smokers.
Over 90% union rate for hypertrophic femoral/tibial shaft nonunions. Key: ream to 1-2mm larger than previous and use a nail 1-2mm greater diameter. The reaming deposits autograft.
- Assessment
- Is it infected?
- Decision
- Check CRP, ESR, history
- Action
- If yes: staged debridement, antibiotics, then reconstruction
- Assessment
- Is it hypertrophic?
- Decision
- Abundant callus on X-ray
- Action
- Needs STABILITY only - exchange nail or compression plate
- Assessment
- Is it atrophic?
- Decision
- No callus, sealed canal
- Action
- Needs BIOLOGY (graft) + stability
- Assessment
- Is there a deformity?
- Decision
- Malunion component
- Action
- CORA analysis, osteotomy + fixation
- Assessment
- Is there a defect?
- Decision
- Bone loss over 3-4cm
- Action
- Masquelet technique or bone transport
DIAMONDDIAMOND - Fracture Healing Requirements
Hook:DIAMOND concept reminds you that fracture healing is multifactorial - missing any element leads to nonunion
ARTSARTS - Malunion Deformity Analysis
Hook:Evaluate every malunion with ARTS - miss one component and your correction will fail
STRAINSTRAIN - Perren Strain Theory
Hook:STRAIN theory explains why too stiff (no callus) or too loose (no bone) both cause nonunion
Overview and Epidemiology
Fracture healing complications represent a significant burden in orthopaedic trauma. Understanding the pathophysiology and systematic approach to assessment is critical for successful management.
Definitions:
- Delayed union: Fracture has not healed in expected timeframe (3-6 months) but shows potential to heal
- Nonunion: Cessation of healing with no radiographic progression for 3 months, typically after 9 months (FDA definition)
- Malunion: Fracture healed in a position that is functionally or cosmetically unacceptable
The economic burden of nonunion is substantial, driven by repeated surgery, prolonged rehabilitation and lost productivity. The contemporary overall nonunion rate is approximately 5% (4.9% across 309,330 fractures; Zura 2016, PMID 27603155), and the tibia plus fibula and femur are among the highest-risk sites owing to precarious blood supply and limited soft-tissue coverage.
Risk Factors for Nonunion:
- Fracture Factors
- Open fractures
- Treatment Factors
- Inadequate fixation
- Fracture Factors
- High-energy mechanism
- Treatment Factors
- Excessive soft tissue stripping
- Fracture Factors
- Bone loss
- Treatment Factors
- Infection
- Fracture Factors
- Segmental fractures
- Treatment Factors
- Poor reduction
- Fracture Factors
- Tibial shaft location
- Treatment Factors
- Delayed surgery
Anatomy and Biomechanics
The Diamond Concept (Giannoudis):
Successful fracture healing requires four key elements, with vascularity as the fifth:
- Osteogenic cells: Mesenchymal stem cells from periosteum and bone marrow
- Osteoinductive mediators: BMPs, PDGF, TGF-beta, cytokines
- Osteoconductive scaffold: Structural matrix (collagen, hydroxyapatite) for bone growth
- Mechanical stability: Adequate fixation creating optimal strain environment
- Vascularity: Adequate blood supply is paramount for healing
Strain = Change in Length / Original Length (dL/L)
- Under 2% strain: Bone forms (primary/intramembranous healing)
- 2-10% strain: Cartilage forms, then bone (secondary/endochondral healing with callus)
- Over 10% strain: Only granulation/fibrous tissue forms (nonunion)
A small fracture gap implies high strain for even minimal movement. Paradoxically, increasing the gap (L) can decrease strain and promote callus, assuming stable fixation.
- Smoking: Carbon monoxide causes tissue hypoxia; nicotine inhibits neovascularisation. Increases nonunion risk by 2.3x
- Diabetes: Microvascular disease and impaired cellular function
- NSAIDs: COX-2 inhibitors may delay healing in animal models; clinical data is mixed
- Metabolic: Vitamin D deficiency (under 50 nmol/L), hypothyroidism, hyperparathyroidism
- Instability: Excessive motion (over 10% strain) prevents calcification leading to hypertrophic nonunion
- Excessive stiffness: Too rigid fixation (locked plating with no gap) prevents callus formation
- Gap: Soft tissue interposition or bone loss prevents healing
The tibia is particularly vulnerable due to its subcutaneous position and dependence on nutrient artery and periosteal blood supply. Open fractures, circumferential stripping, and high-energy injury all compromise vascularity.
The Diamond concept (scaffold + cells + signals) maps directly onto the four properties of bone graft - an examinable framework for choosing a graft for an atrophic nonunion:
- Osteogenic = contains living cells (osteoblasts/MSCs) that form bone - only fresh autograft (iliac crest, RIA) and bone marrow aspirate.
- Osteoinductive = contains signals (BMP-2/-7, TGF-beta) that recruit and differentiate host cells - autograft, demineralised bone matrix (DBM), and recombinant BMP.
- Osteoconductive = provides a passive scaffold for ingrowth - autograft, allograft, DBM, ceramics (hydroxyapatite, tricalcium phosphate), bioglass, collagen.
- Osteopromotive/structural = augments the environment (e.g. PRP) or provides structural support (cortical allograft/strut).
The key teaching points: autograft (iliac crest) is the gold standard because it is the only graft with ALL three biological properties (osteogenic + osteoinductive + osteoconductive); RIA gives a large autograft volume with lower donor-site morbidity; allograft is essentially osteoconductive (and structural) with minimal induction and no living cells; ceramics are purely osteoconductive; and rhBMP is purely osteoinductive. Match the property to the deficiency - an atrophic nonunion lacking cells and signals needs an osteogenic + osteoinductive autograft, not a ceramic scaffold alone.
Classification Systems
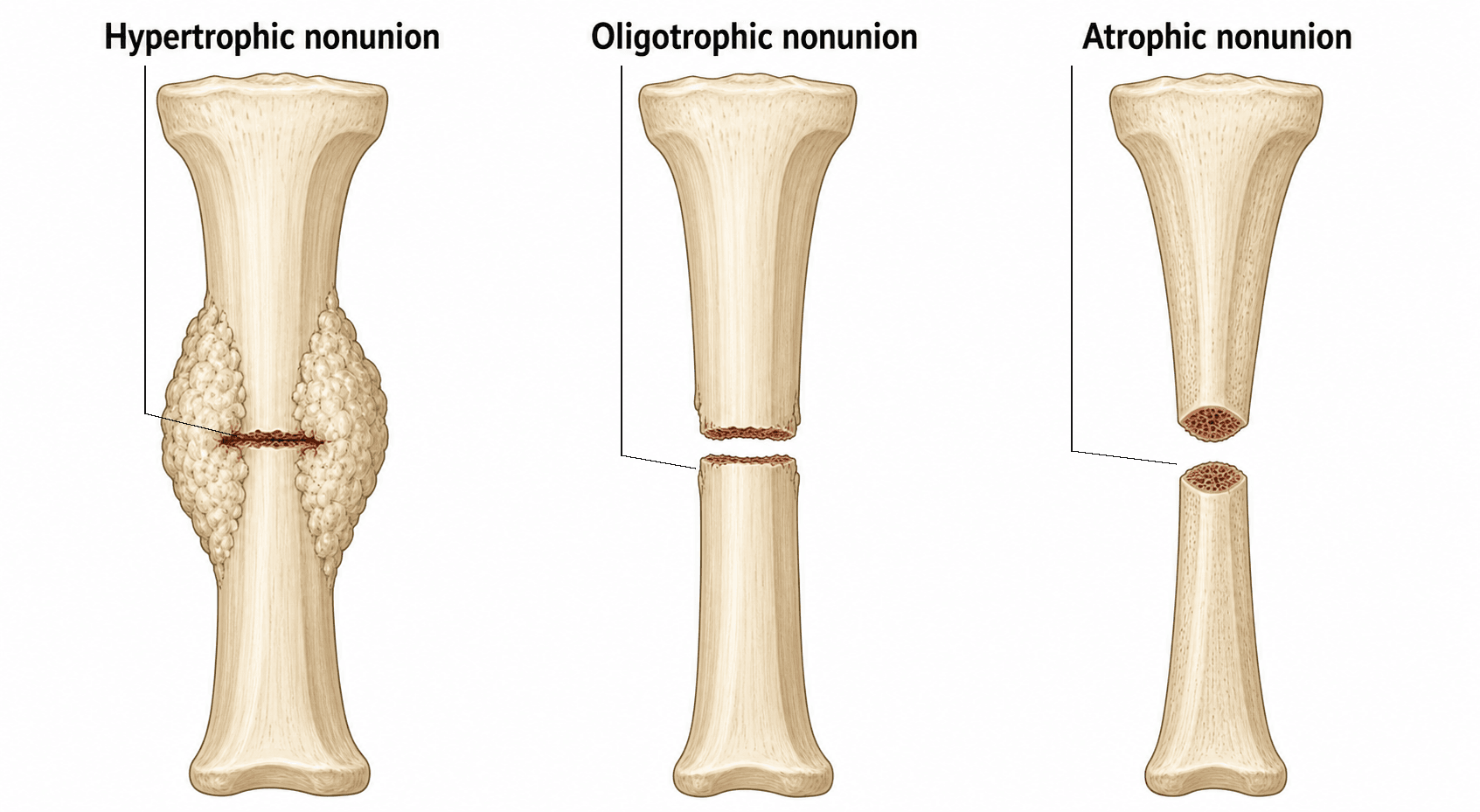
Weber-Cech Classification - Based on vascularity and callus formation
Vascular (Hypertrophic) Nonunions:
- Appearance
- Abundant hypertrophic callus, wide bone ends
- Cause
- Good blood supply but insufficient stability
- Treatment
- STABILITY (exchange nail, compression plate)
- Appearance
- Mildly hypertrophic, moderate callus
- Cause
- Slightly unstable
- Treatment
- STABILITY
- Appearance
- No callus on X-ray but vascular (bone scan positive)
- Cause
- Major instability or poor apposition
- Treatment
- STABILITY
Avascular (Atrophic) Nonunions:
- Appearance
- One side healed, intermediate fragment avascular
- Cause
- Devascularised wedge fragment
- Treatment
- BIOLOGY + Stability
- Appearance
- Necrotic intermediate fragments
- Cause
- Multiple avascular fragments
- Treatment
- BIOLOGY + Stability
- Appearance
- Bone loss beyond critical size
- Cause
- Bone loss from injury or infection
- Treatment
- Masquelet or bone transport
- Appearance
- Rounded, sclerotic bone ends, sealed canal
- Cause
- Complete loss of biological activity
- Treatment
- BIOLOGY + Stability
Hypertrophic = has biology, needs stability. Atrophic = no biology, needs graft plus stability. Oligotrophic appears avascular on X-ray but bone scan is positive - treat as hypertrophic.
This classification is the foundation of treatment.
WEBERWEBER-CECH - Nonunion Classification
Hook:WEBER classification guides treatment - wet needs stability, dry needs biology
Clinical Presentation and Assessment
History:
- Pain: Persistent pain at fracture site, especially with weight-bearing; start-up pain is characteristic
- Function: Inability to progress weight-bearing or activity level
- Constitutional symptoms: Fevers, sweats (screen for infection)
- Risk factors: Smoking history, medications (steroids, NSAIDs), diet
- Previous surgery: Review operative notes for complications, infection, or poor reduction
Physical Examination:
- Significance
- Clinical hallmark of nonunion
- Action
- Confirms diagnosis
- Significance
- Gross instability (false joint/pseudarthrosis)
- Action
- Surgical stabilisation required
- Significance
- Active infection
- Action
- Staged surgical management
- Significance
- Malunion component
- Action
- Deformity analysis required
- Significance
- Chronic disuse
- Action
- Rehabilitation planning
- Significance
- Secondary contracture
- Action
- May need arthrolysis
Every nonunion is infected until proven otherwise.
- Bloods: WCC, CRP (most sensitive), ESR (tracks chronic course)
- History: Any wound drainage is highly predictive of infection
- Biopsy: Gold standard - obtain 5 or more samples from nonunion site at surgery for culture
- Nuclear medicine: Combined WBC/bone marrow scan is gold standard nuclear test for distinguishing septic vs aseptic
Infection eradication is the priority before any reconstruction.
Investigations
Imaging Modalities:
- Role
- First line
- Key Findings
- Fracture line persistence, callus assessment (Weber-Cech), implant failure
- Role
- Detailed assessment
- Key Findings
- Fine detail of bridging bone (over 3 cortices = united), rotational profile, sequestrum
- Role
- Distinguish septic vs aseptic
- Key Findings
- Combined WBC/bone marrow scan is gold standard nuclear test
- Role
- Infection/soft tissue
- Key Findings
- High sensitivity for osteomyelitis, edema, abscess (requires MARS sequences for metal)
Plain Radiograph Assessment:
- Four views: AP, lateral, and obliques plus joints above and below
- Look for fracture line persistence (visible gap)
- Assess callus formation (hypertrophic vs atrophic pattern)
- Check for implant failure (broken screws, bent plate, nail fracture)
Bridging bone on over 3 cortices on orthogonal views suggests union. However, CT often over-calls nonunion due to artefact. Clinical correlation (pain, tenderness, motion) is vital. Always assess rotational profile if malunion suspected.
Laboratory Workup:
- FBC, CRP, ESR (mandatory)
- Vitamin D level (under 50 nmol/L associated with delayed healing)
- HbA1c (diabetic control)
- Albumin, prealbumin (nutritional status)
- Thyroid function tests (if metabolic cause suspected)
Differential Diagnosis of the Persistently Painful or Non-Healing Fracture Site:
- Distinguishing features
- Rest pain, sinus/drainage, raised CRP/ESR, sequestrum or lysis
- Key investigation
- CRP/ESR, intraoperative cultures (5+ samples), WBC/marrow scan
- Action
- Staged debridement and antibiotics before reconstruction
- Distinguishing features
- No callus, sclerotic/rounded ends, sealed canal, normal inflammatory markers
- Key investigation
- Plain films and CT; normal CRP/ESR
- Action
- Biology (graft) plus stable fixation
- Distinguishing features
- Abundant callus (elephant foot), good vascularity, mechanical instability
- Key investigation
- Plain films; implant assessment
- Action
- Stability alone (exchange nail or compression plate)
- Distinguishing features
- Progressive callus, improving pain, within 3-6 months
- Key investigation
- Serial radiographs showing progression
- Action
- Continued optimisation and observation
- Distinguishing features
- Atypical history, lytic or destructive lesion, systemic features
- Key investigation
- MRI, biopsy, oncological staging
- Action
- Investigate and treat underlying lesion before fixation
- Distinguishing features
- Pain localised over hardware, fracture radiographically united
- Key investigation
- CT confirming bridging across 3+ cortices
- Action
- Consider hardware removal after solid union
- Distinguishing features
- Disproportionate pain, allodynia, vasomotor/trophic changes
- Key investigation
- Clinical (Budapest criteria); fracture appears to be progressing
- Action
- Multidisciplinary pain management, not revision surgery
Management Algorithm
The Personality of the Nonunion:
Treatment depends on answering four key questions:
- Is it infected? If yes, staged management: debridement, antibiotics, then reconstruction
- Is it hypertrophic? It has biology but needs stability (fix it stiffer)
- Is it atrophic? It has no biology - needs stability AND biology (graft + fixation)
- Is there a deformity? Needs correction (osteotomy) + fixation
Limited role for established nonunion (over 9 months):
- LIPUS (Low-Intensity Pulsed Ultrasound): Evidence is conflicting. The TRUST trial (BMJ 2016) showed no benefit in fresh tibial fractures. Weak evidence for established nonunions
- Electrical stimulation: Capacitive coupling or pulsed electromagnetic fields. Weak evidence
- Metabolic optimisation: Vitamin D replacement, smoking cessation, protein supplementation
Non-negotiable for elective reconstruction. Most surgeons will not operate electively on active smokers for nonunion surgery. Refer patients to structured cessation support (behavioural counselling plus nicotine-replacement therapy).
Conservative management is primarily adjunctive.
When bone transport or lengthening is used, examiners expect the biology and the practical numbers of distraction osteogenesis (Ilizarov):
- The principle: Ilizarov's law of tension-stress - gradual, controlled distraction of a low-energy corticotomy (preserving periosteal and endosteal blood supply) stimulates new bone (regenerate) formation in the gap.
- The three phases: (1) Latency - a wait of about 5-7 days after corticotomy before distraction, to let the early callus/haematoma organise; (2) Distraction - lengthening at a rate of ~1 mm/day, delivered as a rhythm of ~0.25 mm four times daily (more frequent smaller increments give better regenerate than one big daily turn); (3) Consolidation - the regenerate mineralises, classically taking roughly 1-2 months per cm gained (the high "healing index").
- The regenerate zones (histology): a central radiolucent fibrous interzone (longitudinally oriented collagen and proliferating cells) flanked by two mineralisation fronts maturing into new cortical bone - distraction osteogenesis is intramembranous ossification, not endochondral.
- Getting rate/rhythm wrong: distracting too fast thins the regenerate (poor/failed bone, even a cyst); too slow causes premature consolidation of the corticotomy.
Exam point: corticotomy -> latency ~1 week -> distract ~1 mm/day in ~0.25 mm x4 -> consolidate ~1-2 months/cm; the regenerate has a central fibrous interzone between two mineralisation fronts, and getting the rate/rhythm wrong causes thin regenerate or premature consolidation.
Surgical Technique
- Supine on traction table (femur) or supine on radiolucent table (tibia)
- Image intensifier positioned for AP and lateral views
- Ensure same brand nailing system available (to remove old nail)
- Incision: Use previous incision over nail entry point
- Expose nail: Identify end cap or locking screws
- Remove hardware: Remove end cap and locking screws
- Extract nail: Use appropriate extraction device
- Assess canal: Pass flexible reamer to assess nonunion site
- Over-ream: Ream to 1-2mm larger than previous reamer size
- Collect reaming debris: This is autograft
- Insert larger nail: 1-2mm greater diameter than previous
- Lock nail: Static initially; may dynamise later
- Poller screws: Consider if canal is wide or unstable
- Do not strip soft tissue at nonunion site
- Larger nail is critical for increased stiffness
- Blocking screws improve alignment in metaphyseal extensions
Exchange nailing is minimally invasive and highly effective.
Complications
- Incidence
- 5-15%
- Prevention/Management
- Address both biology and stability; consider revision technique
- Incidence
- 3-5%
- Prevention/Management
- Staged approach; adequate debridement; culture-directed antibiotics
- Incidence
- Up to 30%
- Prevention/Management
- Consider RIA as alternative; limit harvest volume
- Incidence
- Rare
- Prevention/Management
- High index of suspicion with acute correction or lengthening
- Incidence
- 1-3%
- Prevention/Management
- Peroneal nerve at risk with valgus correction; radial nerve with humeral plating
- Incidence
- 5-10%
- Prevention/Management
- Accurate CORA planning; intraoperative assessment
- Incidence
- 3-5%
- Prevention/Management
- Adequate plate length; protected weight bearing
- Chronic pain: up to 30%
- Hematoma: 5-10%
- Nerve injury: LFCN (anterior), cluneal nerves (posterior)
- Fracture: rare but reported with large harvest
- Consider RIA for large graft volumes (lower morbidity)
- Limit anterior iliac crest harvest to inner table
- Posterior approach for larger volumes with less pain
- Close periosteum to reconstruct contour
Postoperative Care and Rehabilitation
- Touch weight bearing typically
- Wound surveillance
- VTE prophylaxis
- Continue smoking cessation
- Optimise nutrition
- X-ray assessment for callus
- Progress weight bearing as callus forms
- Range of motion exercises for adjacent joints
- Consider dynamisation of nail if delayed healing
- Serial radiographic assessment
- Full weight bearing once bridging callus visible
- Progressive strengthening
- Return to light activities
- CT if union uncertain on X-ray
- Address any residual stiffness
- Hardware removal if symptomatic (after solid union)
- Return to sport or manual work
Key Rehabilitation Principles:
- Smoking cessation: Continued abstinence is vital for healing
- Nutrition: Protein and calcium supplementation; vitamin D replacement if deficient
- Dynamisation: For nails, consider removing locking screws at 3-6 months if healing is slow
- Weight bearing: Tailored to fixation stability and healing response
Outcomes and Prognosis
Union Rates by Treatment:
- Union Rate
- Over 90%
- Time to Union
- 4-6 months
- Union Rate
- 85-90%
- Time to Union
- 6-9 months
- Union Rate
- 85-95%
- Time to Union
- 4-6 months
- Union Rate
- 80-90%
- Time to Union
- 6-12 months
- Union Rate
- 80-90%
- Time to Union
- Prolonged (1 month/cm)
- Hypertrophic pattern
- No infection
- Non-smoker
- Good nutrition
- Single previous surgery
- Atrophic pattern
- Active or previous infection
- Continued smoking
- Multiple previous surgeries
- Large bone defect
- Immunocompromised
Under 5% of nonunions ultimately require amputation. This is reserved for cases with uncontrollable infection, severe limb shortening, or patient preference after multiple failed procedures.
Guidelines, Registries & Global Practice
Global Epidemiology (evidence-based):
The most robust contemporary data come from the Zura et al. inception cohort of 309,330 fractures across 18 bones (JAMA Surgery 2016, PMID 27603155), which reported an overall nonunion rate of 4.9%, consistent with the widely quoted 5-10% range for diaphyseal long-bone fractures. The highest-risk anatomical sites were the scaphoid, the tibia plus fibula, and the femur. The tibial shaft remains the prototypical problem fracture worldwide owing to its subcutaneous position, watershed blood supply and frequent open injury.
- Figure
- 4.9%
- Source
- Zura 2016 (PMID 27603155)
- Figure
- 5-10%
- Source
- Zura 2016; consistent across series
- Figure
- 2.32 (95% CI 1.76-3.06)
- Source
- Scolaro 2014 (PMID 24740664)
- Figure
- 1.66
- Source
- Zura 2016 (PMID 27603155)
- Figure
- 1.40
- Source
- Zura 2016 (PMID 27603155)
Smoking is the single most important modifiable risk factor globally (adjusted OR 2.32; Scolaro 2014). Cessation support should be offered to every patient with delayed or nonunion before elective reconstruction.
Guideline & Society Guidance (side-by-side):
- Position on nonunion / fracture healing
- Systematic biology-versus-mechanics assessment; autograft remains gold standard; rhBMP-2 reserved for selected open tibial fractures
- Evidence level
- Based on Level I RCTs (BESTT, SPRINT)
- Position on nonunion / fracture healing
- Senior decision-making, early specialist referral for nonunion, structured MDT for limb reconstruction; does not endorse LIPUS for routine healing
- Evidence level
- Guideline (GRADE-based)
- Position on nonunion / fracture healing
- Open-fracture and limb-reconstruction standards: combined orthoplastic care, debridement and early soft-tissue cover to prevent nonunion
- Evidence level
- Consensus standard
- Position on nonunion / fracture healing
- Diamond Concept framework (scaffold, cells, signals, stability, vascularity); strain theory guides fixation
- Evidence level
- Expert/educational consensus
- Position on nonunion / fracture healing
- Endorses induced-membrane (Masquelet) and distraction osteogenesis for segmental defects; emphasises infection exclusion
- Evidence level
- Narrative/consensus
There is no dedicated international nonunion implant registry; high-quality evidence is trial-driven. Practice is anchored by the SPRINT RCT (reamed nailing reduces reoperation in closed tibial fractures; PMID 19047701), the BESTT RCT (rhBMP-2 in open tibial fractures; PMID 12473698) and the TRUST RCT (LIPUS ineffective; PMID 27797787). National joint replacement registries (AOANJRR, NJR, AJRR) capture arthroplasty but not diaphyseal nonunion outcomes.
Exchange nailing predominates for hypertrophic shaft nonunions across high-income systems. The Masquelet/induced-membrane technique and Ilizarov bone transport are both used for segmental defects, with choice driven by surgeon expertise, defect size and infection status; distraction osteogenesis is relatively more common in centres with established limb-reconstruction units. rhBMP-2 use varies widely with cost and regulatory access.
- Adult daily-smoking prevalence in high-income populations is around 10-11%, and is higher in regional and remote communities where trauma rates are also elevated, reinforcing the need for routine cessation counselling before elective reconstruction.
- The Reamer-Irrigator-Aspirator (RIA) is used at major trauma centres internationally for large-volume autograft harvest with lower donor-site morbidity than iliac crest.
Be prepared to discuss the systematic approach to nonunion: infection screen, classification (Weber-Cech), treatment selection (biology versus mechanics), and patient optimisation (especially smoking cessation). Know exchange nailing technique and the Masquelet technique for defects, and be able to quote the landmark trials (SPRINT, BESTT, TRUST) and the contemporary nonunion rate of approximately 5% (Zura 2016).
MCQ Practice Points
Q: Smoking increases nonunion risk by approximately how much? A: 2.3x increased risk. Carbon monoxide causes tissue hypoxia; nicotine inhibits neovascularisation. This is the single most important modifiable risk factor.
Q: An elephant foot appearance on X-ray represents which type of nonunion? A: Hypertrophic (vascular) nonunion. This has good blood supply and abundant callus but lacks stability. Treatment is mechanical - exchange nail or compression plate. No graft needed.
Q: What does an atrophic nonunion require that hypertrophic does not? A: Biological augmentation (bone graft). Atrophic nonunion has no biological activity (sealed canal, no callus). It needs graft PLUS stability. Hypertrophic needs stability only.
Q: What is the key technical principle of exchange nailing? A: Over-ream by 1-2mm and insert a nail 1-2mm larger diameter. This provides biological effect (reaming autograft) and mechanical effect (larger stiffer nail).
Q: According to Perren strain theory, what strain is required for primary bone healing? A: Under 2% strain. 2-10% strain produces secondary healing with callus. Over 10% strain produces only fibrous tissue.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old male presents with persistent pain 9 months after intramedullary nailing for a closed tibial shaft fracture. He is a smoker. X-rays show a visible fracture line with minimal callus. The nail appears intact.”
“A 45-year-old woman presents with a tibial nonunion 12 months after a Grade IIIB open fracture treated with external fixation and flap coverage. X-rays show atrophic bone ends with a 4cm segmental defect. CRP is normal.”
“A 28-year-old woman presents 18 months after a distal femoral fracture with a united but malunited fracture. She has 15 degrees of varus deformity and 2cm of shortening. She complains of medial knee pain and difficulty with stairs.”
DEFINITIONS
- Delayed union: Not healed by 3-6 months but progressing
- Nonunion: Over 9 months with no progress for 3 months
- Malunion: Healed in unacceptable position (ARTS analysis)
INFECTION SCREEN
- Every nonunion is infected until proven otherwise
- Bloods: CRP (most sensitive), ESR, WCC
- Biopsy: 5+ samples at surgery for culture
- Nuclear medicine: Combined WBC/marrow scan
WEBER-CECH CLASSIFICATION
- Hypertrophic (Elephant foot): Good biology, needs STABILITY
- Oligotrophic: Appears avascular but bone scan positive - treat as hypertrophic
- Atrophic: No biology, sealed canal, needs GRAFT + stability
TREATMENT ALGORITHM
- Infected: Staged debridement then reconstruction
- Hypertrophic: Exchange nail or compression plate (stability only)
- Atrophic: Plate + graft (biology + stability)
- Defect over 4cm: Masquelet or bone transport
EXCHANGE NAILING
- Indication: Aseptic hypertrophic femur/tibia shaft nonunion
- Over-ream 1-2mm larger than previous
- Insert nail 1-2mm larger diameter
- Success rate over 90%
KEY NUMBERS
- Smoking risk: 2.3x increased nonunion
- Primary healing strain: Under 2%
- Secondary healing strain: 2-10%
- ICBG chronic pain: Up to 30%
Evidence Base
- Inception cohort of 309,330 fractures across 18 bones in a US payer database
- Overall nonunion rate 4.9%
- Highest-risk sites: scaphoid, tibia plus fibula, and femur
- Independent risk factors included open fracture (OR 1.66), diabetes (OR 1.40), smoking (OR 1.20) and NSAID plus opioid use (OR 1.84)
- Blinded, sham-controlled RCT of 501 operatively managed tibial fractures across 43 centres
- No difference in time to radiographic healing (hazard ratio 1.07, 95% CI 0.86 to 1.34)
- No improvement in SF-36 physical component or other functional measures at 1 year
- Multicentre blinded RCT of 1319 tibial shaft fractures
- Reamed nailing reduced reoperation in closed fractures (relative risk 0.67, 95% CI 0.47 to 0.96)
- No benefit of reaming in open fractures
- Delaying reoperation for nonunion until at least 6 months reduced the need for surgery
- RCT of 450 open tibial fractures comparing standard care with rhBMP-2 on an absorbable collagen sponge
- 1.50 mg/mL rhBMP-2 reduced risk of secondary intervention by 44% (relative risk 0.56)
- Faster fracture and wound healing and fewer infections in Gustilo type-III injuries
- Systematic review of 19 cohort studies (7 prospective, 12 retrospective) of long-bone fractures
- Adjusted odds ratio of nonunion in smokers 2.32 (95% CI 1.76 to 3.06)
- Higher nonunion in smokers with tibial fractures (OR 2.16) and open fractures (OR 1.95)
- Longer mean healing time in smokers (30.2 vs 24.1 weeks)
- Retrospective cohort of 50 aseptic femoral nonunions previously treated with an intramedullary nail
- Systematic protocol: exchange nail at least 2 mm larger, different manufacturer, static interlocking, correction of metabolic/endocrine abnormality, secondary dynamisation if slow
- 100% union rate; mean time to union 7 months