Life first, limb second, function always
- A mangled extremity is a severe limb injury involving combinations of bone, vascular, nerve, muscle, skin and contamination problems.
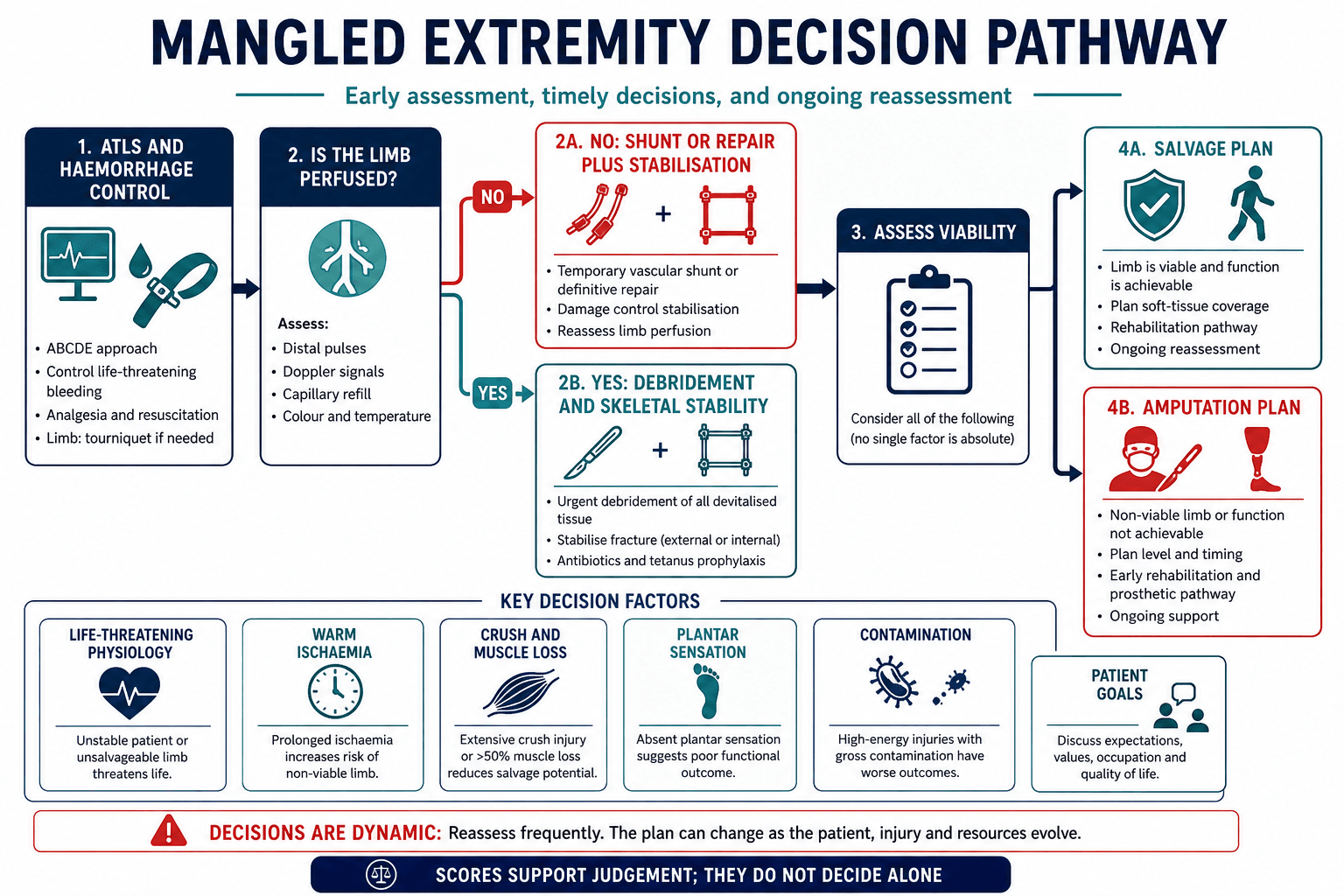
- The first decision is not salvage versus amputation; it is whether the patient can survive the injury and whether the limb is perfused.
- Temporary vascular shunting can reduce ischaemia time and buy time for skeletal stabilisation, transfer or definitive repair.
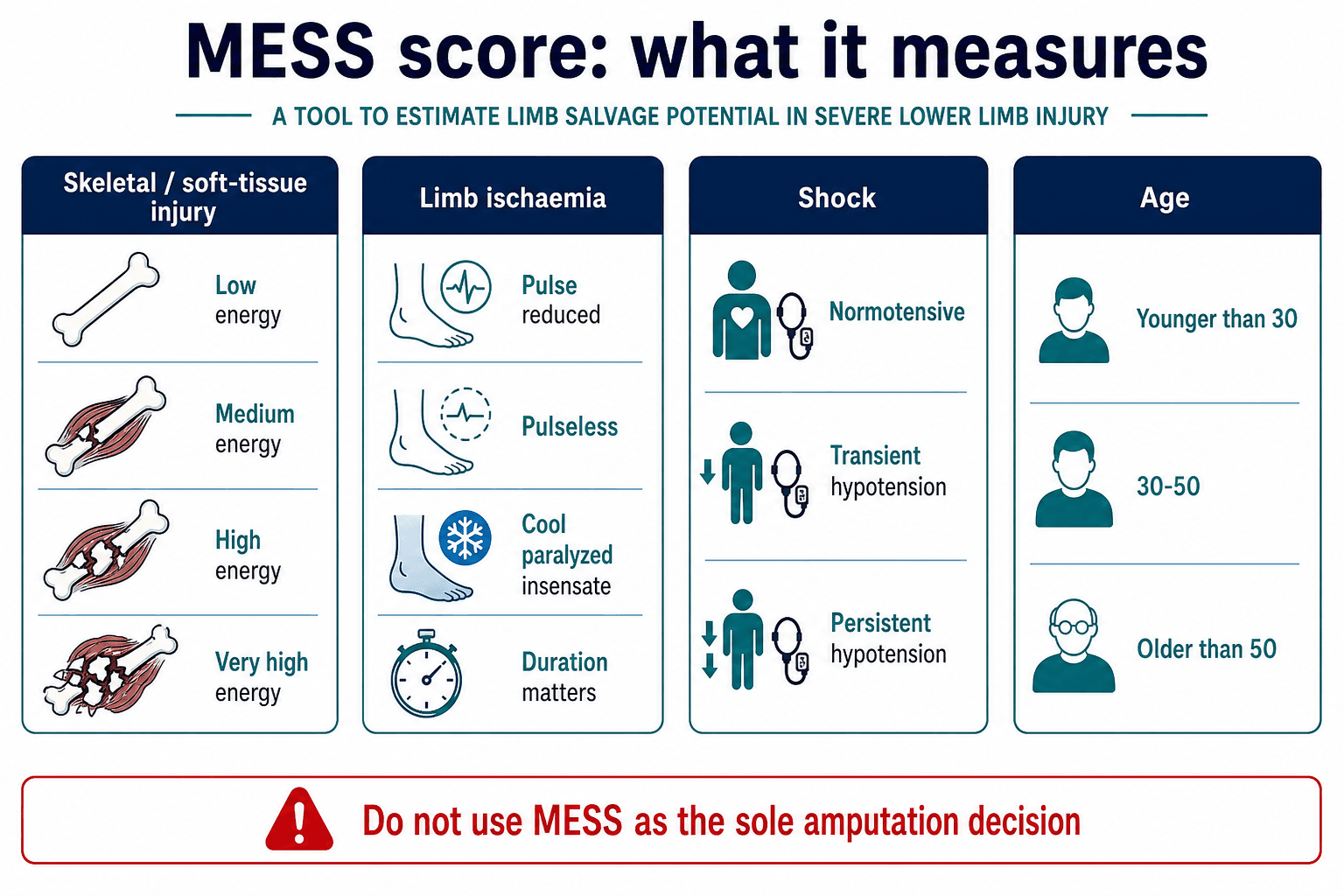
- MESS and similar scores support discussion but should not be used as the sole amputation decision.
- A functional amputation may be better than a painful, infected, insensate, non-functional salvage.
- “The plan can change after debridement because muscle viability and contamination become clearer in theatre.
- “Open wounds do not exclude compartment syndrome; reperfusion increases risk.
- “Absent plantar sensation alone is not an automatic amputation indication, but it is an important prognostic feature.
- “Counselling should compare realistic salvage against realistic amputation, not ideal salvage against failed amputation.
Mangled Extremity and Limb Salvage Decision-Making
Scoring systems are useful because they force a structured assessment. They are unsafe when used as a substitute for senior multidisciplinary judgement, serial examination, patient physiology and patient-centred counselling.
Overview/Epidemiology
A mangled extremity is a severe limb injury in which multiple tissue systems are damaged: bone, joint, artery, vein, nerve, muscle, skin and soft-tissue envelope. It is not simply an open fracture. It is a limb-threatening and sometimes life-threatening trauma state.
Common mechanisms include:
- motorcycle and road trauma
- crush injuries
- industrial and agricultural accidents
- ballistic and blast trauma
- train or machinery injuries
- high-energy falls
The lower limb is the classic decision-making problem because loss of a painful lower limb can sometimes be functionally better than survival of a poorly sensate, infected, stiff and non-weight-bearing limb. Upper-limb salvage often has a lower threshold because even limited hand sensation and positioning can be highly valuable, but the principles of viability, infection control and patient-centred function still apply.
Anatomy/Biomechanics
Mangled limb decision-making requires understanding which structures are essential for useful function.
Vascularity
Arterial inflow is essential for survival of muscle, nerve and skin. Venous outflow matters because severe venous injury can cause swelling, thrombosis and flap failure. Reperfusion after ischaemia can produce swelling, acidosis, hyperkalaemia, myoglobinuria and compartment syndrome.
Muscle
Muscle is the key viability tissue. Devitalised muscle becomes infected, releases myoglobin and prevents healing. Extensive muscle loss reduces functional potential even if bone and vessels can be reconstructed.
Nerve
Nerve injury affects sensation, motor control and pain. A foot with absent protective sensation may ulcerate and fail functionally, but early absent plantar sensation is not always permanent. The decision should consider mechanism, examination reliability, nerve continuity and serial recovery.
Bone and soft-tissue envelope
Bone can often be reconstructed with frames, transport, grafting or induced membrane techniques, but reconstruction only works if infection is controlled and the soft-tissue envelope is durable.
Classification Systems
No classification system can fully decide salvage versus amputation. Use them to structure communication.
The Mangled Extremity Severity Score combines skeletal and soft-tissue injury, limb ischaemia, shock and age. It is easy to remember but unreliable as a sole amputation rule.
- Main variables
- Skeletal and soft-tissue injury, ischaemia, shock, age
- Use
- Most widely known and easy to apply
- Limitation
- Poor standalone prediction in modern vascular and orthoplastic care
- Main variables
- Arterial, nerve, bone, skin, muscle, warm ischaemia
- Use
- Detailed limb-injury severity description
- Limitation
- Less commonly used clinically
- Main variables
- Extent of limb injury and physiological factors
- Use
- Historical structured tool
- Limitation
- Limited validation for modern decision-making
- Main variables
- Nerve injury, ischaemia, soft tissue, skeletal injury, shock, age
- Use
- Highlights nerve injury
- Limitation
- Still not a substitute for judgement
- Main variables
- Hannover fracture scale
- Use
- Detailed severe limb trauma scoring
- Limitation
- Complex and less practical at bedside
The safest statement is: use scores as prompts for senior discussion, documentation and counselling; do not use them as the sole determinant of amputation.
The MESS Score in Detail
Because the MESS is the score the examiner will name, you should be able to reproduce its four components - while still framing it as a prompt, not a verdict.
- Grading
- Low (simple, stab) / medium (open or multiple fractures, dislocation) / high (close-range shotgun, crush) / very high (above plus gross contamination or avulsion)
- Points
- 1 / 2 / 3 / 4
- Grading
- Reduced pulse but normal perfusion / pulseless, paraesthesia, slow refill / cool, paralysed, insensate
- Points
- 1 / 2 / 3 (doubled if prolonged)
- Grading
- Systolic BP always over 90 / transient hypotension / persistent hypotension
- Points
- 0 / 1 / 2
- Grading
- Under 30 years / 30 to 50 years / over 50 years
- Points
- 0 / 1 / 2
In the original Johansen series a total of 7 or more predicted amputation (100% in that small cohort, with a mean MESS of about 4 in salvaged versus about 9 in amputated limbs).
MESS = skeletal/soft-tissue energy (1-4) + limb ischaemia (1-3, DOUBLED beyond 6 hours) + shock (0-2) + age (0-2). A total of 7 or more historically predicted amputation, but that threshold was derived in small cohorts before modern revascularisation and orthoplastic care and must not be used alone - a high MESS in a perfusable, viable limb still warrants a salvage attempt.
Gustilo-Anderson Classification of Open Fractures
The differential above hinges on the Gustilo grade, and the examiner expects you to define it - especially that the IIIC grade (vascular injury) is the one that turns an open fracture into the mangled-extremity decision.
- Wound and soft tissue
- Clean wound under 1 cm, minimal soft-tissue damage, simple pattern
- Key implication
- Low contamination; lowest infection risk
- Wound and soft tissue
- Wound 1 to 10 cm, moderate soft-tissue damage, no extensive devitalisation
- Key implication
- Moderate; usually closable without a flap
- Wound and soft tissue
- High-energy, or wound over 10 cm, but adequate soft-tissue coverage of bone
- Key implication
- Extensive injury yet bone can be covered locally
- Wound and soft tissue
- Extensive soft-tissue loss with periosteal stripping and bone exposure
- Key implication
- Requires flap coverage; high contamination and infection risk
- Wound and soft tissue
- ANY open fracture with an arterial injury requiring repair
- Key implication
- Vascular injury - the trigger for the limb-salvage-versus-amputation question
Infection risk rises steeply with grade (roughly a few percent for type I-II up to tens of percent for type III). Management principles: early intravenous antibiotics (gram-positive cover for I-II, adding gram-negative cover for type III, with anaerobic/penicillin cover for farmyard or grossly contaminated wounds), tetanus prophylaxis, urgent debridement, skeletal stabilisation and a planned orthoplastic soft-tissue strategy.
Gustilo I (under 1 cm, clean), II (1 to 10 cm, moderate) and III (high-energy or over 10 cm), with III subdivided: IIIA (bone coverable), IIIB (needs a flap, periosteal stripping), IIIC (arterial injury requiring repair). The IIIC grade is precisely where revascularisation, ischaemia time and muscle viability dominate - this is the open fracture that becomes a salvage-versus-amputation decision, and the grade is only finalised after debridement.
Clinical Assessment
The first assessment is structured and repeated.
Primary survey
- control haemorrhage
- resuscitate shock
- identify head, chest, abdominal, pelvic and spinal injuries
- treat hypothermia, acidosis and coagulopathy
- decide whether the patient can tolerate limb reconstruction
Limb assessment
Document:
- mechanism and contamination
- ischaemia time and any prehospital tourniquet use
- pulses, Doppler signals, capillary refill and limb temperature
- motor function of major nerve groups
- plantar sensation and protective sensation when assessable
- muscle crush, skin loss and degloving
- compartment tension and pain pattern
- bone loss, joint destruction and instability
- associated open fracture classification
Investigations
Investigations should answer urgent decisions without delaying life- or limb-saving care.
Imaging
- plain radiographs of the injured limb with joint above and below
- CT for complex periarticular injury when the patient is stable
- CT angiography for vascular mapping when it will not delay revascularisation
- intraoperative angiography or direct exploration when needed
Blood tests
- full blood count
- renal function and electrolytes
- coagulation profile
- lactate, base deficit and blood gas in major trauma
- creatine kinase and urine myoglobin when crush injury is suspected
- group and crossmatch
Avoid false precision
Imaging can show fracture and vessel anatomy. It cannot reliably prove muscle viability. The decision often becomes clearer only after debridement, reperfusion and serial reassessment.
Differential of the Severe Limb Injury
The clinical question is not a single diagnosis but which injury pattern is in front of you, because each carries a different decision pathway. Distinguishing these patterns at presentation prevents both unnecessary amputation and futile salvage.
- Defining features
- Open fracture with soft-tissue injury but intact distal perfusion
- Why it changes the decision
- Usually salvageable with orthoplastic care; not a primary amputation question
- Defining features
- Open fracture plus arterial injury requiring repair to maintain viability
- Why it changes the decision
- Time-critical revascularisation; ischaemia time and muscle viability dominate the decision
- Defining features
- Extensive muscle and skin devitalisation, often deceptively viable-looking skin
- Why it changes the decision
- Viability declares late; serial debridement needed before any salvage commitment
- Defining features
- Multiple systems destroyed: bone, vessel, nerve, muscle and cover all compromised
- Why it changes the decision
- True salvage-versus-amputation problem requiring multidisciplinary judgement
- Defining features
- Limb already detached or attached by non-viable tissue only
- Why it changes the decision
- Completion or formal amputation; salvage rarely realistic
- Defining features
- Insensate or paralysed but well-perfused, reconstructable limb
- Why it changes the decision
- Sensation may recover; not an amputation indication on its own
Management Algorithm
Treat life-threatening haemorrhage, shock, hypothermia, acidosis and coagulopathy before committing to prolonged reconstruction.
Decision points
- If the patient is dying, choose the fastest life-saving option.
- If the limb is non-viable, amputation is treatment, not failure.
- If the limb is perfused and viable but complex, staged salvage may be reasonable.
- If both options are possible, the decision is shared and should include expected operations, function, pain and rehabilitation.
Vascular Injury
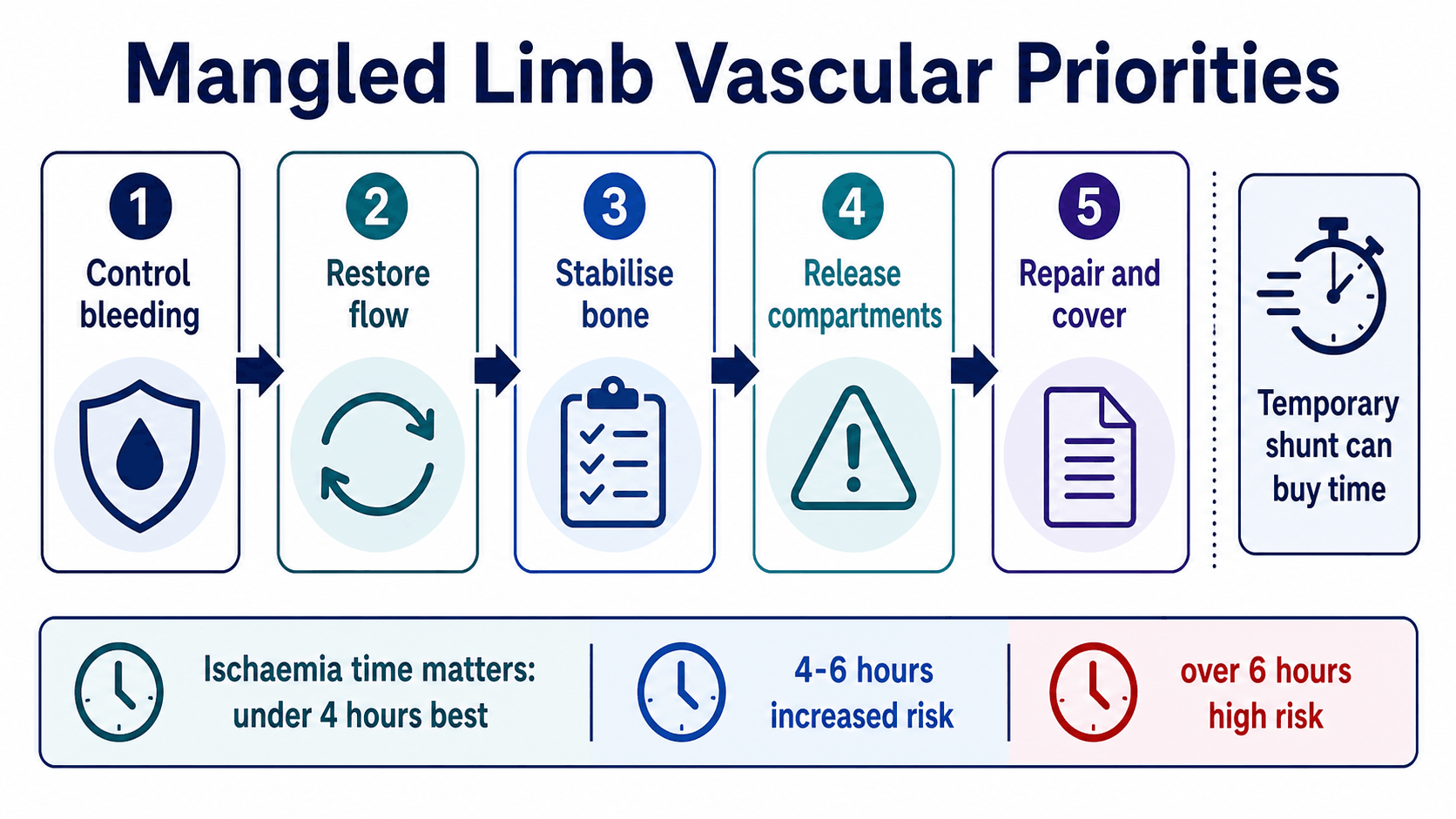
Practical sequence
- Control haemorrhage with direct pressure, packing, tourniquet or operative control.
- Resuscitate and correct physiology.
- Decide whether salvage is plausible.
- Use temporary vascular shunt if definitive repair will be delayed by skeletal stabilisation, transfer or contamination control.
- Stabilise the skeleton sufficiently to protect the repair.
- Repair artery with primary repair, patch, interposition graft or bypass as appropriate.
- Perform fasciotomy when ischaemia-reperfusion or compartment risk is significant.
- Plan soft-tissue coverage and serial reassessment.
Surgical Technique
The surgical technique is usually staged.
Rapid haemorrhage control, gross contamination removal, temporary shunt if needed, external fixation and fasciotomy when indicated.
Salvage reconstruction options
- serial debridement
- temporary or definitive external fixation
- vascular repair or bypass
- fasciotomy and delayed closure or grafting
- local or free flap coverage
- bone transport or shortening then relengthening
- induced membrane reconstruction
- arthrodesis when joints are destroyed
Amputation technique principles
- do not leave devitalised tissue to preserve length
- preserve the most distal functional level that will heal
- create durable soft-tissue cover
- manage nerves deliberately to reduce neuroma pain
- shape bone for prosthetic fitting
- involve rehabilitation and prosthetics early
Salvage Versus Amputation Counselling
Counselling should include:
- survival and immediate safety
- number and type of expected operations
- infection, nonunion and flap risks
- pain and chronic opioid risk
- expected weight-bearing timeline
- work, driving, sport and family responsibilities
- prosthetic options and limitations
- possibility of late amputation after failed salvage
- psychological support
The phrase "we can save the leg" is incomplete. The better question is whether the team can create a limb that is durable, sensate enough, pain-controlled and useful for the patient's life.
Complications
- Mechanism
- Haemorrhage, shock, sepsis, reperfusion injury
- Prevention or response
- Damage control, resuscitation, early source control
- Mechanism
- Return of flow to ischaemic muscle
- Prevention or response
- Limit ischaemia, fasciotomy, renal and metabolic monitoring
- Mechanism
- Crush, swelling, reperfusion, bleeding
- Prevention or response
- Serial assessment and fasciotomy when indicated
- Mechanism
- Contamination, devitalised tissue, dead space, unstable bone
- Prevention or response
- Antibiotics, debridement, stability, coverage and staged reconstruction
- Mechanism
- Bone loss, infection, poor biology
- Prevention or response
- Frame, transport, induced membrane, grafting or revision
- Mechanism
- Failed salvage, pain, infection, non-function
- Prevention or response
- Early realistic counselling and reassessment
Postoperative Care
Postoperative care depends on the pathway chosen.
Salvage pathway
- serial wound and flap monitoring
- vascular observations and anticoagulation plan where relevant
- renal monitoring after crush or reperfusion
- pin-site or implant surveillance
- staged bone reconstruction planning
- early joint motion when safe
- pain service and psychological support
- realistic weight-bearing progression
Amputation pathway
- residual limb oedema control
- wound healing and infection surveillance
- contracture prevention
- desensitisation and mirror therapy where appropriate
- early prosthetic and rehabilitation review
- phantom pain prevention and management
- peer support and psychological care
Outcomes/Prognosis
Outcome is shaped by injury severity, patient factors and social context. LEAP highlighted that long-term results after severe lower-limb trauma are not explained by limb survival alone. Pain, rehospitalisation, socioeconomic factors, smoking, education, litigation, psychological resilience and access to rehabilitation all influence recovery.
Poor prognostic features include:
- prolonged warm ischaemia
- massive muscle loss
- severe contamination
- major nerve disruption
- severe bone loss
- infection
- need for multiple unplanned procedures
- poor social support
- active smoking or major comorbidity
Guidelines, Registries & Global Practice
Global epidemiology
Severe open lower-limb trauma is a worldwide problem driven by road traffic crashes, falls, industrial and agricultural machinery, and conflict-related blast and ballistic injury. The burden is disproportionately high in low- and middle-income countries, where road trauma and limited prehospital and vascular services raise both injury severity and amputation rates. In high-income trauma systems, motorcycle and high-energy vehicle crashes dominate civilian mangled-extremity presentations, while military experience has heavily shaped damage-control and revascularisation practice.
Side-by-side guidance
- Region
- UK
- Emphasis
- Combined orthoplastic care, senior decision-making, early antibiotics, debridement at a specialist centre and definitive skeletal fixation only with simultaneous soft-tissue cover
- Region
- US
- Emphasis
- Limb salvage versus amputation guided by patient physiology and serial assessment rather than a single score; LEAP-informed counselling
- Region
- Global
- Emphasis
- Damage-control orthopaedics, staged debridement, temporary external fixation and reconstruction ladder for bone and soft tissue
- Region
- US / global
- Emphasis
- Early revascularisation, liberal temporary intravascular shunting and a low threshold for fasciotomy after ischaemia-reperfusion
- Region
- Global / conflict
- Emphasis
- Tourniquet-first haemorrhage control, shunting during evacuation and damage-control resuscitation before definitive reconstruction
Registry and system notes
No dedicated mangled-extremity registry exists, but trauma registries (for example TARN in the UK and the US National Trauma Data Bank) and amputation/prosthetic datasets track outcomes, and arthroplasty-style implant registries do not capture this population. The most influential dataset remains the LEAP cohort, which underpins modern counselling worldwide.
High- versus limited-resource practice
- Well-resourced systems: regional major-trauma networks with on-site or rapidly available vascular, plastic and intensive-care support, free-flap capability, microbiology and prosthetic rehabilitation; salvage is attempted more often because the supporting services exist.
- Limited-resource settings: prolonged prehospital times, scarce vascular and microsurgical services and limited prosthetic provision shift the balance; a well-performed early amputation that the patient can rehabilitate from may be safer than an under-supported salvage attempt that fails late.
Universal principles
- Do not delay haemorrhage control or revascularisation for non-essential imaging.
- Give early intravenous antibiotics and tetanus prophylaxis for open injury per local protocol.
- Document neurovascular findings before and after every transfer or manipulation.
- Escalate early and transfer to a centre that can provide combined orthoplastic and vascular care when local resources cannot.
Common Traps
- Calling the decision "salvage versus amputation" before resuscitation and perfusion are addressed.
- Using MESS as an absolute rule.
- Forgetting that muscle viability is often clearer only after debridement and reperfusion.
- Assuming absent plantar sensation always means amputation.
- Trying to preserve limb length while leaving dead tissue behind.
- Discussing salvage without discussing pain, infection, nonunion, work, family and rehabilitation.
- Describing amputation as failure rather than a reconstructive option.
Controversies and Areas of Uncertainty
Examiners reward candidates who can hold genuine uncertainty rather than reciting a fixed rule.
- The role of scoring systems. All scores (MESS, LSI, NISSSA, HFS-97) were derived in small historical cohorts and validated poorly when re-tested in modern revascularised, orthoplastic populations. There is no consensus that any score should independently mandate amputation. Their defensible role is structured documentation and communication.
- Time-to-decision versus damage control. Whether to commit early to amputation in an unstable patient or to attempt staged damage-control salvage is judgement-dependent. The same limb may warrant opposite decisions in different physiological states.
- Ischaemia-time thresholds. The traditional "six-hour" warm-ischaemia limit is a guide, not an absolute; partial perfusion, temperature, age and shunting all modify it, and shunting can extend the salvageable window.
- Primary versus delayed amputation in salvageable limbs. Some evidence suggests selected patients are better served by early amputation than by prolonged salvage that fails late, but predicting which patient will fail salvage remains unreliable.
- Upper versus lower limb thresholds. Salvage thresholds are lower in the upper limb because even limited hand function is valuable; the same score carries different weight by anatomy.
- Outcome measurement. Function, pain, return to work and psychological recovery, rather than limb survival, are increasingly the accepted success metrics, but they are harder to predict at presentation.
MCQ Practice Points
Q: Can a MESS of 7 or greater be used alone to mandate amputation? A: No. Historical cut-offs are unreliable in modern practice; the score supports structured judgement.
Q: Is absent plantar sensation at presentation an absolute indication for amputation? A: No. It is important prognostically, but early sensory loss may recover and must be interpreted in context.
Q: What can reduce ischaemia time when definitive repair is delayed? A: Temporary intraluminal shunting, combined with rapid skeletal stabilisation and definitive vascular repair when feasible.
Q: Why is fasciotomy commonly considered after revascularisation? A: Ischaemia-reperfusion and swelling increase compartment pressure and can destroy otherwise salvageable muscle.
At a Glance Table
- Key questions
- Is the patient in shock, coagulopathic, hypothermic or unstable?
- Decision impact
- Damage control or amputation may be safer than prolonged reconstruction
- Key questions
- Is there distal flow? How long has the limb been ischaemic?
- Decision impact
- Urgent vascular repair, temporary shunt, fasciotomy or amputation decision
- Key questions
- How much muscle is crushed or devitalised? Is cover possible?
- Decision impact
- Determines debridement extent, flap need and salvage potential
- Key questions
- Is there segmental bone loss, articular destruction or non-reconstructable instability?
- Decision impact
- Determines fixation, bone transport, arthrodesis, prosthetic or amputation strategy
- Key questions
- Is protective sensation and motor function likely to recover?
- Decision impact
- A limb can survive but still be non-functional
- Key questions
- What outcome is acceptable to the patient?
- Decision impact
- Shared decision-making is central when both paths are possible
LIFEImmediate Priorities
Hook:Do not let a dramatic limb distract from life-threatening trauma.
VIABLESalvage Feasibility
Hook:A viable-looking limb is not enough; it must become a useful limb.
FAILEDWhen Amputation May Be Better
Hook:FAILED salvage can harm the patient more than a planned functional amputation.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A young motorcyclist arrives with a mangled lower limb, open tibial fracture and absent distal pulses.”
“A patient has a severe open tibial injury with a MESS of 8, but after resuscitation the limb is perfused and muscle appears viable.”
“A patient is three weeks into attempted salvage with recurrent infection, non-viable muscle and progressive systemic illness.”
First priorities
- ATLS and haemorrhage control.
- Assess perfusion and ischaemia time.
- Start antibiotics and tetanus prophylaxis for open injury.
- Escalate to orthopaedic, vascular, plastic surgery and anaesthesia teams.
Salvage factors
- Viable muscle after debridement.
- Restorable arterial inflow and venous outflow.
- Controllable contamination.
- Reconstructable bone and soft-tissue envelope.
- Useful function realistically achievable.
Amputation factors
- Patient physiology cannot tolerate reconstruction.
- Irreversible ischaemic muscle death.
- Uncontrollable infection or contamination.
- Non-functional painful limb expected after salvage.
- Patient preference after informed counselling.
Counselling
- Compare realistic salvage with realistic amputation.
- Explain number of operations and complication risk.
- Include prosthetic and rehabilitation input early.
- Document patient goals and shared decisions.
“Mangled limb care is successful when the team saves life first, restores perfusion when appropriate, reassesses tissue viability honestly and chooses the pathway most likely to give the patient useful function.”
Evidence Base
LEAP: reconstruction versus amputation at two years
- 569 patients with severe leg injuries; at two years the Sickness Impact Profile did not differ between amputation and reconstruction (12.6 versus 11.8, P=0.53).
- Reconstruction patients were rehospitalised more often than amputation patients (47.6 versus 33.9 percent, P=0.002).
- Poorer outcome was predicted by major complications, low education, poverty, lack of insurance, weak social support, low self-efficacy, smoking and litigation.
Original MESS: objective amputation criteria
- MESS combines skeletal/soft-tissue damage, limb ischaemia, shock and age in a simple bedside scale.
- In the original two-centre series a MESS of 7 or greater predicted amputation with 100 percent accuracy.
- Mean MESS was 4.0 in salvaged limbs versus 8.8 in amputated limbs.
Insensate foot is not an amputation indication
- Among 55 limbs insensate at presentation, salvaged limbs did not have worse outcomes than amputated or sensate control limbs at 12 and 24 months.
- About 55 percent of salvaged limbs had normal plantar sensation at two years regardless of admission sensation; only one salvaged insensate limb remained insensate.
- Initial plantar sensation did not predict long-term sensory or functional status.
MESS does not predict amputation in popliteal artery injury
- 50 patients with isolated popliteal artery injury; revascularisation was attempted in all with an 88 percent limb-salvage rate.
- MESS did not differ between amputated and salvaged limbs (8.4 versus 8.1, P=0.765).
- Fasciotomy was performed far more often in higher-MESS limbs and is emphasised as a key salvage measure.
Contemporary MESS reliability
- 31 limbs with MESS of 7 to 8 underwent salvage attempts; 13 were saved and 18 amputated.
- Salvage rate was 62.5 percent in upper-limb and 20 percent in lower-limb trauma.
- MESS was a poor predictor of amputation in upper-limb trauma and more useful in the lower limb.
Recent advances and the future of abdominopelvic and lower extremity vascular injury management
- Temporary intravascular shunts restore early perfusion to ischaemic limbs and can increase limb-salvage rates.
- Shunts are valuable when skeletal stabilisation, damage control or interhospital transfer would otherwise prolong ischaemia.
- Autologous vein remains the gold-standard conduit for definitive repair of lower-limb vascular injury.
Orthoplastic timing of flap coverage in open tibia
- 296 Gustilo III open tibial fractures requiring flaps; 32.4 percent became infected.
- Time from definitive fixation to flap coverage was the delay measure most associated with infection.
- Flap failure carried the highest odds of infection (OR 6.83); temporary internal fixation did not increase infection risk.
Useful source anchors:
- LEAP outcomes of reconstruction or amputation (NEJM): PubMed 12477942
- LEAP best available evidence review: PubMed 20399362
- LEAP lessons and outcome factors: PubMed 17003200
- Insensate foot after severe lower-extremity trauma: PubMed 16322607
- Original MESS description: PubMed 2342140
- Contemporary MESS reliability: PubMed 36637105
- MESS and popliteal artery injury: PubMed 36449024
- Orthoplastic flap timing in open tibia: PubMed 34267149