Deltoid Ligament | Eversion Injuries | Underdiagnosed Entity
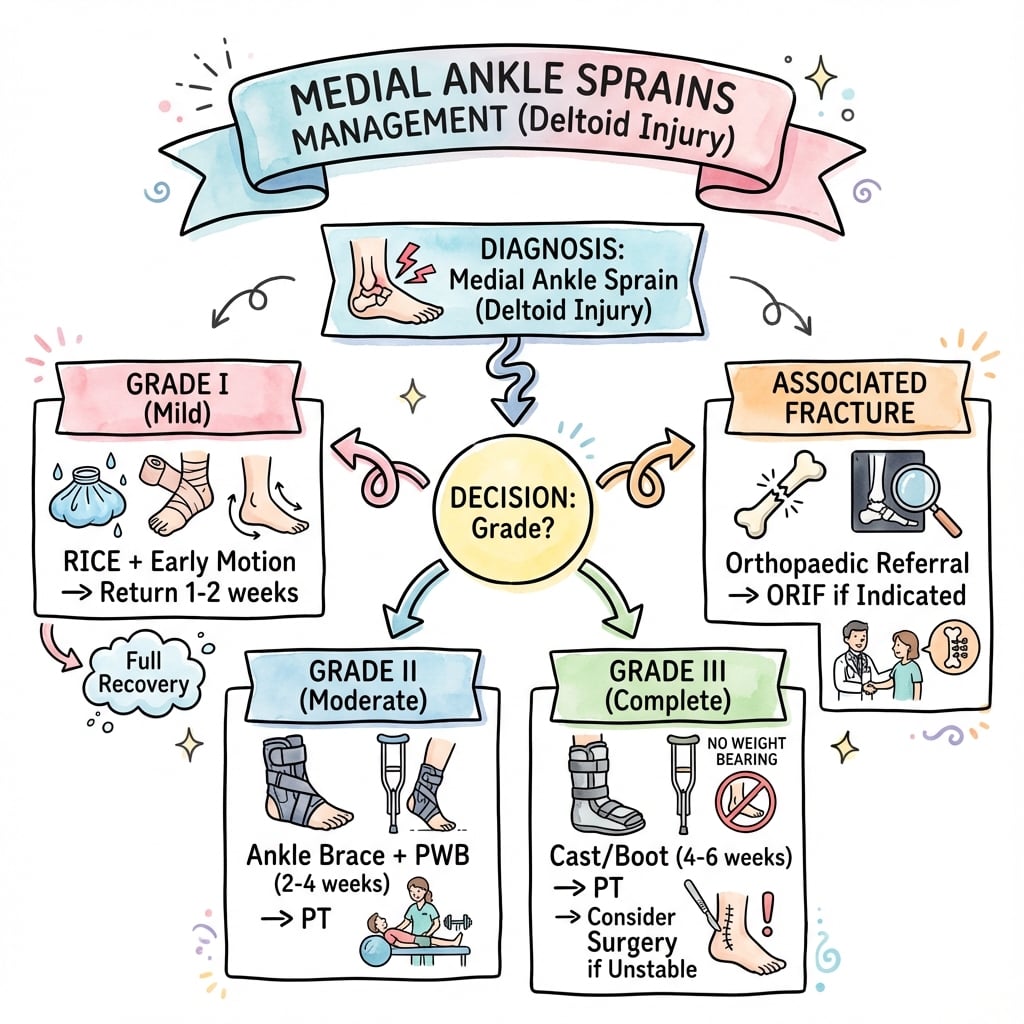
Deltoid Ligament Injury Grades
Critical Must-Knows
- Deltoid is STRONGEST ankle ligament - rarely injured in isolation
- Deep deltoid (ATTL) = primary stabilizer against lateral talar shift
- Always suspect syndesmosis and/or fibula fracture with deltoid injury
- Medial clear space greater than 4mm = abnormal (weight-bearing films)
- Isolated deltoid tears CAN cause chronic instability if missed
Clinical Pearls
- "Eversion stress test = gold standard clinical exam
- "Gravity stress views to assess medial clear space
- "MRI to differentiate superficial vs deep layer tears
- "Associated fractures: Weber B/C, Maisonneuve, SER pattern
Critical Deltoid Ligament Exam Points
Anatomy is Key
Superficial deltoid (4 bands: tibionavicular, tibiocalcaneal, tibiospring, posterior tibiotalar) resists eversion. Deep deltoid (ATTL + PTTL) resists lateral talar translation - this is critical for ankle stability.
Always Exclude
Isolated deltoid injuries are rare. Always examine: syndesmosis (squeeze test, external rotation), proximal fibula (Maisonneuve), and obtain stress radiographs. Missing associated injuries = poor outcomes.
Imaging Pitfalls
Non-weight-bearing films miss instability. Always obtain weight-bearing or gravity stress views. Medial clear space greater than 4mm or greater than 1mm asymmetry = deltoid incompetence.
Surgical Indications
Consider repair if: persistent medial clear space widening despite syndesmosis fixation, chronic medial instability, or associated tibialis posterior dysfunction. Most heal with conservative management.
Quick Decision Guide
| Clinical Scenario | Investigation | Key Finding | Management |
|---|---|---|---|
| Medial pain, no swelling, minimal laxity | Weight-bearing XR | MCS normal | Functional rehab 2-4 weeks |
| Moderate swelling, positive eversion stress | Stress XR + MRI | MCS widened, partial tear | Boot, protected WB 6 weeks |
| Severe swelling, lateral fibula fracture | Full ankle series | MCS greater than 4mm, Weber B/C | ORIF + consider deltoid repair |
| High fibula pain, medial tenderness | Full tibia/fibula XR | Maisonneuve fracture | Syndesmosis fixation |
TNCSSuperficial Deltoid Bands
| T | Tibionavicular Most anterior, resists eversion |
| N | (tibio)calcaneal Middle, longest component |
| C | tibio-Calcaneonavicular (Spring) Supports spring ligament |
| S | Superficial posterior tibiotalar Most posterior superficial |
| T | Tibionavicular Most anterior, resists eversion | C | tibio-Calcaneonavicular (Spring) Supports spring ligament |
| N | (tibio)calcaneal Middle, longest component | S | Superficial posterior tibiotalar Most posterior superficial |
Hook:TNCS = The Navicular Connects Subtalar - all superficial bands!
APDeep Deltoid Components
| A | Anterior Tibiotalar Ligament (ATTL) Deep, primary stabilizer against lateral shift |
| P | Posterior Tibiotalar Ligament (PTTL) Deep, resists posterior translation |
| A | Anterior Tibiotalar Ligament (ATTL) Deep, primary stabilizer against lateral shift |
| P | Posterior Tibiotalar Ligament (PTTL) Deep, resists posterior translation |
Hook:AP = Anteroposterior deep layer controls TALAR position!
SMASHAssociated Injuries to Exclude
| S | Syndesmosis injury High ankle sprain, squeeze test |
| M | Maisonneuve fracture Proximal fibula, full leg films |
| A | Ankle fracture (Weber B/C) Lateral malleolus fracture |
| S | Spring ligament injury Assess medial arch |
| H | Hidden osteochondral lesion Medial talar dome |
| S | Syndesmosis injury High ankle sprain, squeeze test | S | Spring ligament injury Assess medial arch |
| M | Maisonneuve fracture Proximal fibula, full leg films | H | Hidden osteochondral lesion Medial talar dome |
| A | Ankle fracture (Weber B/C) Lateral malleolus fracture |
Hook:SMASH the differential - deltoid injuries rarely come alone!
Overview and Epidemiology
Medial ankle sprains (deltoid ligament injuries) are significantly less common than lateral ankle sprains due to the deltoid's strength and the biomechanics of ankle injury. However, they carry important clinical significance due to their frequent association with other injuries and the critical role of the deep deltoid in ankle stability.
Why So Rare?
Deltoid is the strongest ankle ligament - requires significant force to injure. Most mechanisms that stress the deltoid also fracture the lateral malleolus or injure the syndesmosis first. Truly isolated deltoid injuries typically occur with forced eversion or external rotation on a planted foot.
High-Risk Activities
- Contact sports (football, rugby)
- Landing on inverted ankle
- External rotation injuries
- Motor vehicle accidents
- Falls from height
Risk Factors
- Previous ankle injury
- Hindfoot valgus alignment
- Ligamentous laxity
- Inadequate proprioception
- Poor neuromuscular control
Pathophysiology and Mechanisms
Critical Anatomy
The deltoid ligament is a fan-shaped complex originating from the medial malleolus with two distinct layers. The superficial layer (4 bands) resists eversion, while the deep layer (ATTL + PTTL) is the primary restraint against lateral talar translation - the key to ankle stability.
Deltoid Ligament Components
| Layer | Component | Origin | Insertion | Function |
|---|---|---|---|---|
| Superficial | Tibionavicular | Anterior colliculus | Navicular tuberosity | Resists eversion, ER |
| Superficial | Tibiocalcaneal | Anterior colliculus | Sustentaculum tali | Longest, resists valgus |
| Superficial | Tibiospring | Anterior colliculus | Spring ligament | Supports medial arch |
| Superficial | Superficial PTT | Posterior colliculus | Talus (superficial) | Resists ER |
| Deep | ATTL | Intercollicular groove | Talus (medial) | PRIMARY STABILIZER |
| Deep | PTTL | Posterior colliculus | Talus (posteromedial) | Resists posterior shift |
Deep vs Superficial
Deep layer (ATTL) attaches directly to talus and is the PRIMARY restraint against lateral talar shift - this is what keeps the talus centered in the mortise. Superficial layer primarily resists eversion. A competent deep deltoid can maintain mortise stability even if superficial layer is torn.
Medial Malleolus Anatomy
- Anterior colliculus: Superficial deltoid origin
- Posterior colliculus: Deep PTTL origin
- Intercollicular groove: Deep ATTL origin
- Critical for surgical planning
Biomechanical Function
- Resists valgus tilt (superficial)
- Resists lateral talar translation (deep)
- Contributes 20-50% mortise stability
- Works with lateral complex for balance
Classification Systems
Standard Ligament Sprain Classification
| Grade | Pathology | Clinical Features | Stability | Recovery |
|---|---|---|---|---|
| I (Mild) | Stretch, microscopic tears | Mild pain, minimal swelling | Stable | 2-4 weeks |
| II (Moderate) | Partial macroscopic tear | Moderate pain, swelling, ecchymosis | Mild laxity | 6-8 weeks |
| III (Severe) | Complete rupture | Severe pain, significant swelling | Unstable | 3+ months |
Clinical-Imaging Correlation
Grade III injuries may paradoxically have less pain due to complete ligament disruption. Always correlate with stress radiographs - clinical examination alone underestimates severity in 30% of cases.
Grading guides rehabilitation intensity and return-to-activity timelines.
Clinical Assessment
History
- Mechanism: Eversion, external rotation, landing awkwardly
- Onset: Acute vs chronic instability
- Location: Medial ankle swelling and tenderness
- Associated: Did you hear/feel a pop? Able to weight-bear?
Examination
- Inspection: Swelling, ecchymosis (medial)
- Palpation: Deltoid ligament, medial malleolus, proximal fibula
- ROM: Often limited by pain and swelling
- Stress tests: Eversion stress, external rotation stress
Complete Examination Required
ALWAYS examine: proximal fibula (Maisonneuve), squeeze test (syndesmosis), lateral ligaments, and assess for tenderness along entire fibula length. A medial-sided injury with proximal fibula fracture = unstable pattern requiring surgery.
Clinical Tests for Deltoid Integrity
| Test | Technique | Positive Finding | Interpretation |
|---|---|---|---|
| Eversion stress | Stabilize leg, apply valgus stress to hindfoot | Increased medial opening vs contralateral | Deltoid laxity |
| External rotation stress | Foot in neutral, externally rotate | Medial pain, lateral opening | Combined deltoid/syndesmosis |
| Palpation | Along deltoid origin and insertion | Point tenderness | Localize injury level |
| Squeeze test | Compress tibia/fibula mid-leg | Pain at syndesmosis | Associated syndesmosis injury |
Ottawa Ankle Rules
Ottawa rules focus on fracture exclusion. Even if no fracture indication, persistent medial tenderness with mechanism of injury warrants stress imaging to assess deltoid competence and mortise stability.
Differential Diagnosis of Medial Ankle Pain
| Diagnosis | Discriminating Features | Key Investigation | Distinguishing Point |
|---|---|---|---|
| Deltoid ligament injury | Eversion/ER mechanism, medial swelling, positive eversion stress | Weight-bearing/gravity stress XR, MRI | Widened medial clear space, layer-specific tear on MRI |
| Medial malleolus fracture | Bony point tenderness, inability to weight-bear | Plain radiograph | Cortical break; deltoid avulsion variant possible |
| Maisonneuve fracture | Medial pain + proximal fibula tenderness | Full-length tibia/fibula XR | High fibula fracture with syndesmotic disruption |
| Tibialis posterior dysfunction | Chronic, progressive flatfoot, too-many-toes sign | MRI, single heel-raise test | Tendon (not ligament) pathology, arch collapse |
| Medial talar osteochondral lesion | Deep ache, mechanical catching, effusion | MRI / CT | Subchondral lesion on imaging, no MCS widening |
| Spring (CN) ligament tear | Plantar-medial pain, arch sag | MRI | Talonavicular sag; often coexists with deltoid/PTT |
| Medial ankle impingement | Anteromedial pain on dorsiflexion, post-traumatic | MRI, diagnostic injection | Soft-tissue/osteophyte impingement, stable mortise |
Investigations
Imaging Protocol
AP, lateral, and mortise views. Non-weight-bearing views miss instability. Measure medial clear space (MCS) on mortise view - normal is less than 4mm and equal to superior clear space. MCS greater than 4mm or greater than 1mm asymmetry = deltoid incompetence.
Gravity stress view (lateral decubitus, affected side down) or manual eversion stress. Essential when clinical suspicion high but standard films normal. Confirms mortise instability.
Gold standard for soft tissue assessment. Distinguishes superficial vs deep layer involvement. Identifies associated injuries (syndesmosis, OLT, tendon pathology). Grade tear severity.
Medial Clear Space
MCS greater than 4mm = deltoid incompetence. MCS greater than superior clear space by greater than 1mm = abnormal. These findings indicate mortise instability requiring operative intervention even without visible fracture. Weight-bearing films are ESSENTIAL.
Radiographic Findings
- MCS widening (greater than 4mm)
- Talar tilt on stress views
- Associated fractures (fibula, syndesmosis)
- Avulsion from medial malleolus
MRI Findings
- Superficial layer: Edema, partial/complete tear
- Deep layer: ATTL and PTTL integrity
- Associated: OLT, syndesmosis, tibialis posterior
- Bone marrow edema: Medial malleolus stress
Management Algorithm
Non-Operative Management Protocol
Goal: Protect healing, restore ROM, strength, and proprioception.
Rehabilitation Phases
Protection and inflammation control: RICE protocol. CAM boot or stirrup brace for Grade II-III. Weight-bearing as tolerated with crutches. Gentle ROM exercises once swelling subsides.
Progressive loading: Transition to supportive footwear. Isometric and isotonic strengthening. Proprioception exercises. Pool therapy for unloading.
Functional progression: Resistance training. Balance and agility drills. Sport-specific activities. Address any residual stiffness.
Criteria-based return: Full strength (greater than 90% vs contralateral). Pain-free sport-specific activity. Normal proprioception. Consider taping/bracing initially.
Success Factors
Good outcomes with conservative management for isolated Grade I-II injuries with intact deep layer. Poor prognostic factors: deep layer involvement, associated fracture, chronic instability, MCS widening despite bracing.
Most isolated deltoid injuries heal well with conservative treatment - surgery reserved for specific indications.
Surgical Technique
Acute Deltoid Ligament Repair
Surgical Steps
Supine position, bump under ipsilateral hip. Thigh tourniquet. Ensure adequate exposure of medial ankle.
Curved medial incision centered on medial malleolus. Protect saphenous vein and nerve. Identify tibialis posterior tendon sheath (retract posteriorly).
Identify torn ligament ends. Assess deep vs superficial layer involvement. Debride frayed tissue minimally. Assess footprint on malleolus and talar attachments.
Suture anchor technique preferred: Place 2-3 anchors in anterior colliculus (superficial) and intercollicular groove (deep). Pass sutures through ligament substance. Repair in layers - deep first, then superficial.
Tension repair with ankle in neutral dorsiflexion and slight inversion. Confirm mortise reduction with intraoperative imaging. Ensure no over-tightening.
Technical Pearls
Deep layer repair is critical for restoring stability. Use at least one anchor in intercollicular groove for ATTL. Avoid aggressive debridement - preserve tissue for repair. Consider augmentation if tissue quality poor.
Post-repair immobilization in CAM boot for 6 weeks with protected weight-bearing.
Complications
Potential Complications
| Complication | Risk Factors | Prevention | Management |
|---|---|---|---|
| Chronic instability | Missed diagnosis, inadequate rehab | Early diagnosis, complete rehabilitation | Reconstruction if symptomatic |
| Stiffness | Prolonged immobilization | Early ROM, progressive loading | Physiotherapy, possible MUA |
| Nerve injury (saphenous) | Surgical approach | Careful dissection, protect nerve | Observation, most resolve |
| Osteochondral lesion | Missed initial OLT | MRI in persistent symptoms | Microfracture, OATS if needed |
| Medial gutter impingement | Over-tightened repair, scarring | Appropriate tensioning | Debridement if symptomatic |
Missed Associated Injuries
The most significant complication is missing associated injuries - syndesmosis instability, Maisonneuve fracture, or lateral malleolus fracture. Always examine the entire leg and obtain appropriate imaging. Missed injuries lead to chronic instability and early arthritis.
Chronic Medial Instability
Underdiagnosed entity. Patients present with vague medial pain, giving way, difficulty on uneven ground. Key exam finding: positive eversion stress test. May require reconstruction if symptomatic despite rehabilitation.
Postoperative Care
Rehabilitation Protocol (Post-Repair/Reconstruction)
Immobilization: CAM boot, non-weight-bearing. Elevate limb. Gentle toe ROM. Wound care. Control swelling with ice and compression.
Protected mobilization: CAM boot weight-bearing as tolerated. Begin ankle ROM exercises in boot. Isometric strengthening. Pool therapy if wound healed.
Progressive loading: Wean from boot to supportive footwear. Progressive resistance training. Balance and proprioception exercises. Gait training.
Return to activity: Sport-specific drills. Agility and plyometric progression. Criteria-based return to sport (strength greater than 90%, pain-free, normal proprioception).
Conservative Rehab
- Grade I: Functional brace, WBAT, 2-4 weeks
- Grade II: CAM boot 4-6 weeks, progressive rehab
- Grade III: CAM boot 6+ weeks, consider surgery if unstable
- All grades: proprioception focus
Surgical Rehab
- NWB 2 weeks (wound healing)
- WBAT in boot weeks 2-6
- Boot wean at 6 weeks
- Sport 4-6 months post-op
Outcomes and Prognosis
Prognostic Factors
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Layer involvement | Superficial only | Deep layer (ATTL) involved |
| Associated injuries | Isolated deltoid injury | Fracture, syndesmosis involvement |
| Stability | Stable on stress views | Persistent MCS widening |
| Treatment timing | Early diagnosis and treatment | Delayed diagnosis, chronic instability |
Long-Term Outcomes
Most isolated deltoid injuries heal well with appropriate conservative treatment. Risk factors for chronic instability: deep layer involvement, missed associated injuries, inadequate rehabilitation, premature return to sport. Chronic medial instability may require reconstruction for definitive management.
Evidence Base
- Dissection of 12 cadaveric ankles defined five main bundles (tibiospring, tibiocalcaneal, anterior and posterior deep tibiotalar, superficial posterior tibiotalar)
- Tibiocalcaneal and tibiospring ligaments are the longest; tibiocalcaneal and posterior deep tibiotalar are the thickest
- Tibionavicular 'ligament' is a thickened capsular fold rather than a discrete band
- The deltoid–spring ligament complex is the primary restraint against pronation/valgus and medial arch collapse
- Posterior tibial tendon is a secondary stabilizer whose load rises sharply once ligamentous restraints fail
- Tibionavicular tenodesis can over-constrain physiologic hindfoot pronation — favour anatomic reconstruction of the tibiocalcaneonavicular ligament
- Twelve studies pooled; ultrasonography (AUC highest, sensitivity 1.00) and gravity stress radiography (sensitivity 0.71–1.00) were the most accurate tests
- Plain mortise radiography was insensitive (0.33–0.57); clinical examination alone was unreliable (sensitivity 0.20–0.90)
- MRI sensitivity 0.57–0.85, specificity 0.81–1.00
- Against intraoperative direct visualization, an injury-film medial clear space over 5 mm predicted deep deltoid rupture with 95% accuracy
- When MCS was under 5 mm, stress-view MCS was far less accurate than MRI (46% vs 79%) with an 80% false-positive rate
- Supports operative fixation without further imaging when injury-film MCS is over 5 mm
- Nine studies, N=508; deltoid repair lowered syndesmotic malreduction (0–9% vs 20–35%) versus trans-syndesmotic screws
- Implant-removal rate was lower after repair (5.8% vs 41%) at the cost of 16–20 min longer operating time
- Pain, ROM, function and MCS were equivalent or better with repair
- Eight studies; functional outcomes equivalent between repair and no-repair/syndesmotic fixation
- Five of six studies reporting radiographs showed reduced medial clear space and fewer malreductions after repair
- Authors conclude high-quality evidence is lacking and a multicentre RCT is warranted
- Fourteen feet with advanced flatfoot and large spring-ligament tears; allograft tibiocalcaneonavicular reconstruction added to bony correction
- FAAM-ADL improved 69.3 to 90.1 and SF-36 pain 44.6 to 93.1 at mean 24 months
- Radiographic deformity (talo-first metatarsal, talonavicular coverage, Meary angle) significantly corrected
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Ankle Fracture with Medial Clear Space Widening
"A 45-year-old man sustains a twisting injury playing soccer. X-rays show a Weber B fibular fracture. After ORIF of the fibula, intraoperative stress views show persistent medial clear space widening of 6mm."
Scenario 2: Isolated Medial Ankle Sprain
"A 28-year-old female basketball player sustains an eversion injury to her ankle during a game. She has significant medial swelling and tenderness over the deltoid ligament. X-rays show no fracture but MCS of 5mm on weight-bearing views."
Scenario 3: Chronic Medial Ankle Instability
"A 35-year-old recreational runner presents with 18 months of medial ankle pain and giving way episodes. He had an ankle sprain 2 years ago treated conservatively. Examination shows positive eversion stress test. MRI shows chronic deltoid attenuation."
Scenario 4: Medial Ankle Pain After Ankle Fracture ORIF
"A 50-year-old woman is 6 months post Weber B ankle fracture ORIF. She has persistent medial ankle pain and difficulty with uneven ground. Radiographs show healed fracture with MCS of 3mm."
MCQ Practice Points
Deltoid Ligament Anatomy
Q: Which component of the deltoid ligament is the PRIMARY restraint against lateral talar translation? A: Anterior Tibiotalar Ligament (ATTL) - The deep ATTL is the primary stabilizer against lateral talar shift, attaching from the intercollicular groove to the medial talus. This is the critical component for ankle mortise stability.
Radiographic Assessment
Q: What is the threshold for abnormal medial clear space on weight-bearing ankle radiographs? A: Greater than 4mm or greater than 1mm difference from superior clear space - These thresholds indicate deltoid ligament incompetence and ankle mortise instability requiring intervention.
Associated Injury Pattern
Q: A patient has isolated medial ankle tenderness with proximal fibula pain after a twisting injury. What diagnosis must be excluded? A: Maisonneuve fracture - This injury pattern (deltoid tear or medial malleolus fracture + proximal fibula fracture + syndesmosis disruption) represents a highly unstable ankle injury requiring syndesmosis fixation.
Imaging Modality
Q: What is the gold standard imaging modality for assessing deltoid ligament layer involvement? A: MRI - MRI accurately differentiates superficial from deep deltoid tears, which is critical for prognosis and treatment planning. Deep layer involvement has worse prognosis.
Surgical Indications
Q: What is the primary indication for deltoid ligament repair during ankle fracture surgery? A: Persistent medial clear space widening greater than 4mm after fibula ORIF - If the mortise is still unstable after lateral fixation, deltoid repair is indicated to restore mortise congruency and prevent post-traumatic arthritis.
Controversies and Areas of Uncertainty
To repair the deltoid or not?
Routine deltoid repair in ankle fractures remains debated. Systematic reviews show equivalent functional outcomes but lower syndesmotic malreduction and hardware-removal rates with repair. High-quality RCT evidence is still lacking, leaving genuine clinical equipoise.
Repair vs syndesmotic fixation
When the medial side is incompetent, some surgeons restore stability by repairing the deltoid, others by trans-syndesmotic fixation (screw or suture-button). Whether one reliably outperforms the other — and whether they should be combined — is unresolved.
MCS threshold and stress testing
The classic 4 mm cut-off is convenient but imperfect. An injury-film MCS over 5 mm is highly predictive of deep rupture, whereas manual stress views in the 4–5 mm range carry a high false-positive rate. The optimal confirmatory test (stress XR vs ultrasound vs MRI) is not standardized.
Chronic medial instability
A genuinely underdiagnosed entity with no agreed classification or validated reconstruction algorithm. Graft choice, single- vs dual-tunnel technique, and the role of concomitant bony realignment (calcaneal osteotomy) are all surgeon-dependent.
Guidelines, Registries & Global Practice
Global Epidemiology
Medial (deltoid) sprains account for roughly 5–10% of ankle sprains, dwarfed by lateral injuries. The deep deltoid is the strongest ankle ligament, so isolated rupture is uncommon; most deltoid injuries accompany supination-external-rotation or pronation-external-rotation fracture patterns. Ankle fractures are among the most common operatively managed fractures worldwide, making deltoid competence a high-volume decision point.
Side-by-Side Guidance (Societies & Consensus)
| Body | Region | Emphasis on Deltoid / Medial Instability |
|---|---|---|
| AO Foundation | Global | Stability-based fracture management; medial clear space and syndesmotic integrity drive operative decisions; deltoid repair optional where reduction is blocked or instability persists |
| AAOS | US | Evidence-based ankle-fracture care; recognises limited high-level evidence for routine deltoid repair |
| BOA / BOAST | UK | Standards for open and closed ankle fracture care emphasise anatomic mortise reduction and early weight-bearing rehabilitation |
| ESSKA / EFORT | Europe | Consensus on ankle instability favours anatomic repair/reconstruction and structured functional rehabilitation |
Registry & Evidence Notes
- No dedicated ligament registry; evidence comes from RCTs, cohorts and systematic reviews
- Ankle-fracture outcome data (e.g. national audit datasets) inform mortise-reduction quality benchmarks
- Functional outcomes broadly equivalent across repair strategies; radiographic reduction favours deltoid repair
High- vs Limited-Resource Practice
- Well-resourced: stress XR, MRI/ultrasound, suture-anchor repair, graft reconstruction available
- Limited-resource: rely on weight-bearing/gravity stress radiographs and clinical stress testing; MRI may be unavailable
- Functional rehabilitation and accurate mortise reduction remain the universal, low-cost priorities
Exam Focus (Global)
Examiners across boards (FRCS, FRACS, EBOT, ABOS, DNB/MS) will expect: deltoid anatomy (superficial vs deep), recognition of associated injury patterns, appropriate imaging protocols (weight-bearing/gravity stress views), the medial-clear-space concept, and evidence-based indications for surgical intervention. Maisonneuve fracture recognition is universally emphasized.
MEDIAL ANKLE SPRAINS
Clinical summary
Key Anatomy
- •SUPERFICIAL deltoid: 4 bands (TNCS) - resist eversion
- •DEEP deltoid: ATTL + PTTL - resist lateral talar shift (PRIMARY STABILIZER)
- •ATTL from intercollicular groove = key for mortise stability
- •Anterior colliculus: superficial origin; Posterior: deep PTTL origin
Critical Imaging
- •WEIGHT-BEARING films essential - NWB films miss instability
- •MCS greater than 4mm = deltoid incompetence
- •MCS greater than SCS by greater than 1mm = abnormal
- •MRI for layer involvement (superficial vs deep)
Associated Injuries (SMASH)
- •Syndesmosis injury - squeeze test, external rotation
- •Maisonneuve fracture - ALWAYS examine proximal fibula
- •Ankle fracture (Weber B/C) - lateral malleolus
- •Spring ligament injury - medial arch collapse
- •Hidden OLT - medial talar dome
Surgical Indications
- •Persistent MCS widening after fibula ORIF
- •Isolated Grade III with symptomatic instability failing conservative
- •Chronic medial instability after rehab failure
- •Acute: Repair (suture anchors); Chronic: Reconstruction (graft)
Exam Pearls
- •Deltoid is STRONGEST ankle ligament - isolated injury RARE
- •Deep layer (ATTL) integrity determines prognosis
- •Truly isolated = pure eversion mechanism, uncommon
- •Chronic medial instability is UNDERDIAGNOSED