Valgus Stress | Grade I-III | Usually Conservative | Combined ACL
MCL GRADING (Valgus Stress)
Critical Must-Knows
- sMCL is PRIMARY restraint to valgus at 30 degrees
- Most MCL injuries heal conservatively (90%+)
- Combined MCL/ACL: treat ACL, MCL heals with rehab
- Surgery indicated: chronic instability, Grade III with ACL, multiligament
- Test at 30 degrees flexion to isolate MCL
Clinical Pearls
- "Test at 0 degrees: posteromedial corner involvement if unstable
- "Stener lesion equivalent: sMCL displaces over pes anserinus
- "sMCL femoral attachment lies just proximal-posterior to medial epicondyle
- "POL (posterior oblique ligament) is the key dynamic posteromedial stabiliser
Clinical Imaging
Imaging Gallery




Critical Exam Concepts
Conservative First
90%+ of MCL injuries heal without surgery. Even Grade III isolated MCL usually heals. Functional bracing and early ROM is key.
Test at 30 Degrees
Valgus stress at 30 degrees isolates the MCL. At 0 degrees, posteromedial corner and cruciates also contribute. Compare sides.
Combined MCL/ACL
Address ACL surgically, MCL usually heals. Exception: Grade III MCL with valgus laxity at 0 degrees may need MCL surgery at same time.
Surgical Indications
Surgery for: chronic instability, failed conservative, multiligament injury, Stener equivalent with MCL trapped.
MCL Injury Treatment Guide
| Grade | Laxity | Endpoint | Treatment |
|---|---|---|---|
| Grade I | None | Firm | Functional brace, early ROM |
| Grade II | 1-5mm increased | Present | Hinged brace 4-6 weeks, rehab |
| Grade III Isolated | 5-10mm increased | Absent | Hinged brace 6-8 weeks, usually heals |
| Grade III + ACL | Significant | Absent | ACL reconstruction, MCL usually heals (may need repair) |
VALMCL Injury Mechanism
| V | Valgus Force pushing knee inward |
| A | Applied laterally Blow to lateral knee |
| L | Ligament stretches medially MCL fails tensile load |
| V | Valgus Force pushing knee inward |
| A | Applied laterally Blow to lateral knee |
| L | Ligament stretches medially MCL fails tensile load |
Hook:VAL-gus stress causes MCL injury!
TWOMCL Examination
| T | Thirty degrees Isolates MCL from cruciates |
| W | Wide open Compare to contralateral side |
| O | Zero degrees Checks posteromedial corner too |
| T | Thirty degrees Isolates MCL from cruciates |
| W | Wide open Compare to contralateral side |
| O | Zero degrees Checks posteromedial corner too |
Hook:Test at TWO positions - 30 and 0 degrees!
SDPLayers of Medial Knee
| S | Superficial Sartorius, gracilis, STJ |
| D | Deep to superficial sMCL layer |
| P | Proper capsule dMCL, posteromedial capsule |
| S | Superficial Sartorius, gracilis, STJ |
| D | Deep to superficial sMCL layer |
| P | Proper capsule dMCL, posteromedial capsule |
Hook:SDP - Warren layers of the medial knee!
Overview and Epidemiology
MCL Healing Capacity
MCL has excellent healing capacity due to extraarticular location and good blood supply. Even Grade III tears usually heal with bracing and rehabilitation. This differentiates it from ACL/PCL.
Epidemiology
- Most common knee ligament injury
- Contact sports: football, rugby, hockey
- Skiing (combined ACL/MCL common)
- Males greater than females
- Often combined injuries
Mechanism
- Valgus stress: Most common
- Contact: Blow to lateral knee
- Non-contact: Cutting, pivoting
- External rotation: May also injure
- Combined ACL: Common mechanism
Pathophysiology and Mechanisms
Medial Knee Complex Anatomy
The medial side is best understood as three primary static stabilisers (LaPrade quantitative anatomy): the superficial MCL, the deep MCL and the posterior oblique ligament.
Superficial MCL (sMCL):
- Primary static restraint to valgus and a key secondary restraint to external/internal tibial rotation
- Femoral attachment lies just proximal and posterior to the medial epicondyle (a small depression, on average a few mm from the epicondyle), NOT several cm proximal to the joint
- Average ligament length around 9 to 10 cm
- Two tibial attachments: a proximal soft-tissue (meniscal) attachment and a distal firm bony attachment roughly 6 cm distal to the joint line, deep to the pes anserinus
Deep MCL (dMCL):
- A capsular thickening with meniscofemoral and meniscotibial components
- Firmly anchors the body of the medial meniscus
- Contributes mainly to anteromedial rotatory restraint
Posterior oblique ligament (POL):
- Fan-shaped condensation posterior to the sMCL, blending with the semimembranosus
- Principal restraint to valgus and rotation near full extension and the key structure in posteromedial corner (PMC) injury
Valgus at 0 Degrees = More Severe
Valgus laxity at 0 degrees extension indicates injury to posteromedial corner and possibly cruciates in addition to MCL. This is a more severe injury pattern requiring careful evaluation.
Classification Systems
MCL Injury Grading
| Grade | Pathology | Examination | Laxity |
|---|---|---|---|
| I | Fiber stretch, intact | Tender, firm endpoint | 0-5mm, no increase |
| II | Partial tear | Lax with endpoint | 5-10mm increased |
| III | Complete rupture | Lax without endpoint | Greater than 10mm increased |
Compare to contralateral side - absolute values vary between individuals.
Clinical Assessment
History
- Mechanism: Valgus blow, contact
- Pain: Medial knee, at time of injury
- Swelling: Often localized medial
- Instability: Giving way with valgus
- Associated injuries: Pop (ACL), locking (meniscus)
Examination
- Tenderness: Along MCL course
- Valgus stress 30 degrees: Isolates MCL
- Valgus stress 0 degrees: PMC involved if lax
- ACL tests: Lachman, pivot shift
- Meniscus: McMurray, joint line
Valgus Stress Test Technique
Patient supine. At 30 degrees flexion, stabilize thigh, apply valgus force to ankle. Compare opening and endpoint to contralateral side. Repeat at 0 degrees - laxity here indicates posteromedial corner injury.
Key Clinical Pearls
Palpate the MCL: Tenderness along course helps identify injury location - femoral, mid-substance, or tibial.
Check ACL: Always perform Lachman and pivot shift. Combined injuries are common.
Differential Diagnosis of Acute Medial Knee Pain
Distinguishing MCL Injury from Mimics
| Diagnosis | Key Distinguishing Feature | Best Test |
|---|---|---|
| MCL injury | Valgus laxity at 30 degrees, tenderness along MCL course | Valgus stress at 30 degrees |
| Medial meniscus tear | Joint-line tenderness, mechanical locking, effusion | McMurray, MRI |
| Posteromedial corner injury | Valgus laxity at 0 degrees plus rotatory instability | Valgus stress at 0 degrees, MRI |
| Medial tibial plateau fracture | Inability to weight bear, bony tenderness | Radiograph, CT |
| Pes anserine bursitis | Tenderness over pes insertion, no laxity, often overuse | Clinical, no valgus laxity |
| Saphenous neuritis | Burning medial pain, no laxity, sensory change | Clinical, Tinel along adductor canal |
| Patellar dislocation (medial) | MPFL tenderness, apprehension, haemarthrosis | Apprehension test, MRI |
Investigations
MRI Assessment
Sensitivity: Excellent for MCL injuries.
Findings: Edema surrounding MCL, discontinuity, thickening.
Tear location: Femoral, mid-substance, tibial.
Associated injuries: ACL, meniscus, cartilage, bone bruise.
MRI not always required for isolated MCL but helps define Grade III and associated injuries.
Pellegrini-Stieda Lesion
Pellegrini-Stieda lesion = calcification at MCL femoral origin. Represents chronic MCL injury with calcification of hematoma. Visible on X-ray. May be asymptomatic.
Management Algorithm
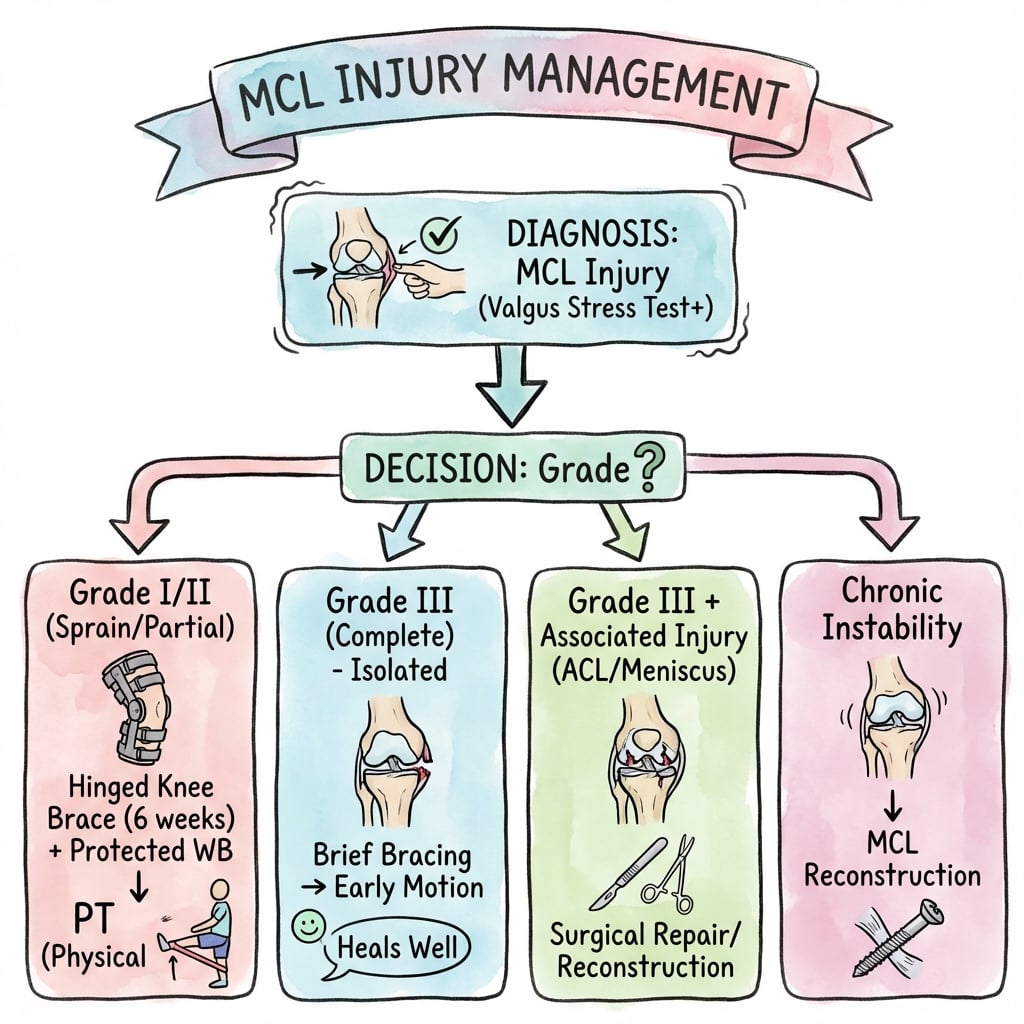
MCL Injury Management
Treatment Pathway
RICE, brace in extension. Examine for associated injuries. Consider MRI if Grade III or associated injury suspected.
Hinged brace allowing ROM. Early physiotherapy. Weight bearing as tolerated. Return to sport 2-6 weeks.
Hinged brace 6-8 weeks. Protected weight bearing initially. Supervised rehabilitation. Most heal.
ACL reconstruction if indicated. MCL usually heals during ACL recovery. Surgery if Grade III with laxity at 0 degrees.
Surgical Technique
MCL Repair Techniques
Acute femoral avulsion: Suture anchors or bone tunnels to restore origin.
Acute tibial avulsion: Screw with soft tissue washer.
Mid-substance tear: Primary repair with non-absorbable sutures if acute.
Augmentation with graft may be added for severe injuries.
Avoid Overtensioning MCL
When repairing or reconstructing MCL, avoid overtensioning which leads to loss of flexion and lateral compartment overload. Tension at 20-30 degrees flexion with slight valgus.
Complications
| Complication | Cause | Prevention | Management |
|---|---|---|---|
| Stiffness | Prolonged immobilization | Early ROM | Physiotherapy, MUA if severe |
| Chronic laxity | Inadequate healing | Appropriate bracing duration | Late reconstruction |
| Calcification | Hematoma | Early ROM, avoid NSAIDs acutely | Usually asymptomatic |
| Saphenous nerve | Surgery | Careful dissection | Neuroma management |
Stiffness Prevention
Early ROM is key to preventing stiffness. Even Grade III injuries benefit from hinged bracing allowing motion rather than cast immobilization. Stiffness is the enemy.
Postoperative Care
Rehabilitation Protocol
Hinged brace locked initially. Toe touch weight bearing. Quad sets, SLR.
Progressive ROM in brace. Increase weight bearing. Gentle strengthening.
Full ROM. Progressive resistance. Proprioception. Wean brace.
Sport-specific training. Functional testing. Full return when stable.
Conservative vs Surgical Rehab
Conservative: Faster progression, early ROM encouraged. Surgical (reconstruction): More protected initially, similar final timeline. Both aim for full ROM and strength before return to sport.
Outcomes and Prognosis
Outcomes by Grade
Grade I: Excellent outcomes. Return to sport 1-2 weeks. Minimal long-term sequelae.
Grade II: Good outcomes. Return to sport 4-6 weeks. Bracing during sport initially helpful.
Grade III Isolated: Most heal with bracing. Some chronic laxity may persist but often asymptomatic.
Combined Injuries: Outcomes depend on addressing all pathology. ACL reconstruction with MCL healing typical.
Controversies and Areas of Uncertainty
Timing of ACL Reconstruction in Combined Injury
Most surgeons allow the MCL to recover full extension and resolve acute valgus laxity before ACL reconstruction (typically a few weeks), citing arthrofibrosis risk with very early combined surgery. The optimal window remains debated, and some advocate earlier reconstruction once motion is restored.
Repair versus Reconstruction in Acute High-Grade Injury
For acute distal (tibial-sided / Stener-equivalent) sMCL avulsions and complete posteromedial corner disruption, primary repair has historically had higher failure rates than for lateral-side injuries. There is growing interest in repair with suture augmentation versus primary reconstruction, but high-level comparative data are lacking.
Grade III Isolated MCL: Always Conservative?
Landmark series support non-operative care even for complete isolated tears, yet a subset develops chronic valgus or anteromedial rotatory instability. Identifying which complete tears (e.g. distally based, multi-structure POL involvement) will fail bracing is unresolved.
Role of Stress Radiography and Cut-offs
Side-to-side valgus opening on stress radiographs helps grade severity, but published cut-offs distinguishing isolated sMCL from combined sMCL plus POL injury vary between studies, limiting a single agreed threshold.
Evidence Base and Key Studies
Non-Operative Treatment of Complete (Grade III) Isolated MCL Tears
- Comparative study of operative versus non-operative care of complete isolated MCL tears
- Non-operatively treated knees achieved results comparable to surgically repaired knees
- Functional treatment avoided the morbidity and stiffness of surgery and casting
- Helped establish non-operative care as standard for isolated complete MCL injury
Combined ACL/Grade III MCL: Operative vs Non-Operative MCL (RCT)
- Level 1 RCT: 47 patients with combined ACL + grade III MCL, all had early ACL reconstruction
- MCL treated operatively (n=23) versus non-operatively (n=24)
- No significant difference in stability, ROM, muscle power, Lysholm or IKDC at ~2 years
- AP stability excellent in both groups
Early Operative MCL Repair Slows Recovery (Companion RCT)
- Same RCT cohort analysed for ROM and quadriceps power
- Flexion deficit greater after combined ligament repair at 6, 12 and 36 weeks
- Quadriceps power deficit larger in the repair group at 52 weeks (30.7% vs 20.5%)
- Differences resolved by 104 weeks
Early Functional Rehabilitation of Isolated Grade III MCL in Athletes
- Prospective 5-year follow-up of 35 athletes with isolated grade III MCL sprains
- Treated with lateral hinged brace and early ROM, no immobilisation or surgery
- Mean HSS knee score 45.9 of 50 at mean 5.3 years
- Results comparable to surgery or immobilisation with faster return to sport
Quantitative Anatomy of the Medial Part of the Knee
- Cadaveric quantitative mapping of the medial knee structures
- sMCL femoral attachment lies just proximal-posterior to the medial epicondyle; mean length ~94.8 mm
- sMCL has two tibial attachments, the distal one ~61 mm distal to the joint
- Defined POL and deep MCL (meniscofemoral/meniscotibial) attachments and the gastrocnemius tubercle landmark
Surgical and Non-Surgical Outcomes of Medial Knee Injuries (Review)
- Synthesis of operative and non-operative outcome literature for medial-sided knee injury
- Isolated partial and complete MCL injuries do well with bracing and early motion
- RCT evidence supports non-operative MCL care in combined ACL-MCL injury
- Knee dislocations and posteromedial corner injuries do better with surgical reconstruction
Society Guidance and Standard References
- Isolated MCL injury (all grades): functional bracing and early ROM as first-line care
- Reserve surgery for chronic symptomatic instability, distal Stener-type avulsion and multiligament injury
- Combined ACL-MCL: reconstruct the ACL, manage the MCL non-operatively in most cases
- Posteromedial corner disruption should be anatomically addressed at multiligament surgery
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Contact Sports Injury
"A 22-year-old rugby player sustains a valgus blow to his knee during a tackle. He has medial knee pain and swelling. Examination shows Grade II laxity at 30 degrees with a firm endpoint. Lachman is negative. How would you manage this?"
Scenario 2: Combined ACL/MCL Injury
"A 28-year-old skier with a twisting fall presents with a swollen knee. Examination shows Grade III MCL laxity and positive Lachman with pivot shift. MRI confirms ACL rupture and Grade III MCL tear. What is your treatment plan?"
Scenario 3: Chronic MCL Instability
"A 35-year-old presents with ongoing medial knee instability 6 months after an MCL injury that was treated conservatively. He has failed prolonged rehabilitation. Valgus stress shows Grade II laxity at 30 degrees. What would you recommend?"
MCQ Practice Points
Primary MCL Function
Q: What is the primary function of the sMCL? A: Primary static restraint to valgus stress - in classic sectioning studies the sMCL provides roughly three-quarters of valgus restraint at about 25 degrees of flexion, far more than at full extension.
Why Test at 30 Degrees
Q: Why test MCL at 30 degrees flexion? A: Isolates the MCL. At 0 degrees, posteromedial capsule and cruciates also contribute. Laxity at 0 degrees indicates more severe injury.
MCL Healing
Q: Why does MCL heal better than ACL? A: Extraarticular location and good blood supply. Not bathed in synovial fluid. Forms healing scar tissue.
Combined ACL/MCL
Q: How should combined ACL/MCL injury be treated? A: ACL reconstruction, MCL heals conservatively. Exception is Grade III MCL with laxity at 0 degrees may need surgical MCL.
Pellegrini-Stieda
Q: What is Pellegrini-Stieda lesion? A: Calcification at MCL femoral origin from chronic injury with hematoma calcification. Visible on X-ray.
Stener Equivalent
Q: What is the MCL Stener equivalent? A: sMCL displaces over pes anserinus preventing healing. Indication for surgical reduction.
Guidelines, Registries & Global Practice
Global Epidemiology
- The MCL is the most commonly injured knee ligament worldwide
- Peak incidence in young, active populations and contact/collision and pivoting sports (football/soccer, rugby, American football, skiing, wrestling)
- Higher reported rates in males, largely reflecting sport-participation patterns
- Skiing classically produces combined valgus-external-rotation ACL/MCL injuries
- Most are low-grade (I to II) and managed entirely in primary or sports-medicine care
Registry and Outcome Context
- No dedicated national MCL registry exists; isolated MCL injury rarely reaches an implant/arthroplasty registry
- Relevant registry signal is indirect: combined ACL/MCL is captured within national ACL reconstruction registries (Scandinavian, UK NLR, others)
- Those datasets reinforce ACL reconstruction with non-operative MCL care as the dominant combined-injury pathway
- Surgical MCL/POL work concentrates in multiligament and knee-dislocation cohorts
Side-by-Side Guidance (where emphasis differs)
Society and System Perspectives on MCL Injury
| Body / System | First-line | Surgical emphasis |
|---|---|---|
| AAOS / AMSSM (US) | Functional brace and early ROM for isolated injury | Selective: chronic instability, distal avulsion, multiligament |
| BOA / UK sports practice | Bracing and graded rehab; physiotherapy-led | PMC and multiligament patterns to specialist units |
| AO Foundation / trauma | Non-operative for isolated; ROM-preserving | Repair/augment in dislocation and combined trauma |
| EFORT / European consensus | Conservative isolated MCL; reconstruct chronic laxity | Anatomic sMCL/POL reconstruction for failed conservative |
High- vs Limited-Resource Practice Variation
- Well-resourced settings: ready access to MRI and hinged functional bracing, supervised physiotherapy and graded return-to-sport testing; specialist reconstruction available for the minority who need it.
- Limited-resource settings: diagnosis relies more on careful clinical valgus stress testing (which is sufficient for most isolated injuries); improvised or non-hinged bracing and home-based rehab are used; MRI and reconstruction are reserved for combined/multiligament injury. Because isolated MCL injury heals well without surgery, clinical-examination-led conservative care travels well across resource settings.
Orthopaedic Exam Relevance
MCL injuries are common viva topics. Know the conservative treatment algorithm, when NOT to operate, how to manage combined injuries, the LaPrade medial-knee anatomy and the grading system.
MEDIAL COLLATERAL LIGAMENT INJURIES
Clinical summary
Grading (Valgus at 30 degrees)
- •Grade I: Tender, firm endpoint, no laxity
- •Grade II: Laxity with endpoint
- •Grade III: Laxity without endpoint
- •Compare to contralateral side
Examination Key Points
- •Test at 30 degrees: Isolates MCL
- •Test at 0 degrees: PMC if unstable here
- •Always check ACL (Lachman, pivot)
- •Palpate along MCL course
Treatment Algorithm
- •Grade I-II: Conservative (90%+ heal)
- •Grade III isolated: Usually conservative
- •Combined ACL/MCL: ACL surgery, MCL heals
- •Surgery: chronic instability, Stener, multilig
Anatomy Pearls
- •sMCL: primary valgus restraint
- •Origin 5cm proximal to joint line
- •dMCL: part of posteromedial capsule
- •Warren layers: 3 layers medial knee
Return to Sport
- •Grade I: 1-2 weeks
- •Grade II: 4-6 weeks
- •Grade III: 8-12 weeks
- •Protective brace may help initially