Boxer's Fracture | Rotation vs Angulation | Fight Bites | 10-10-30-50 Rule
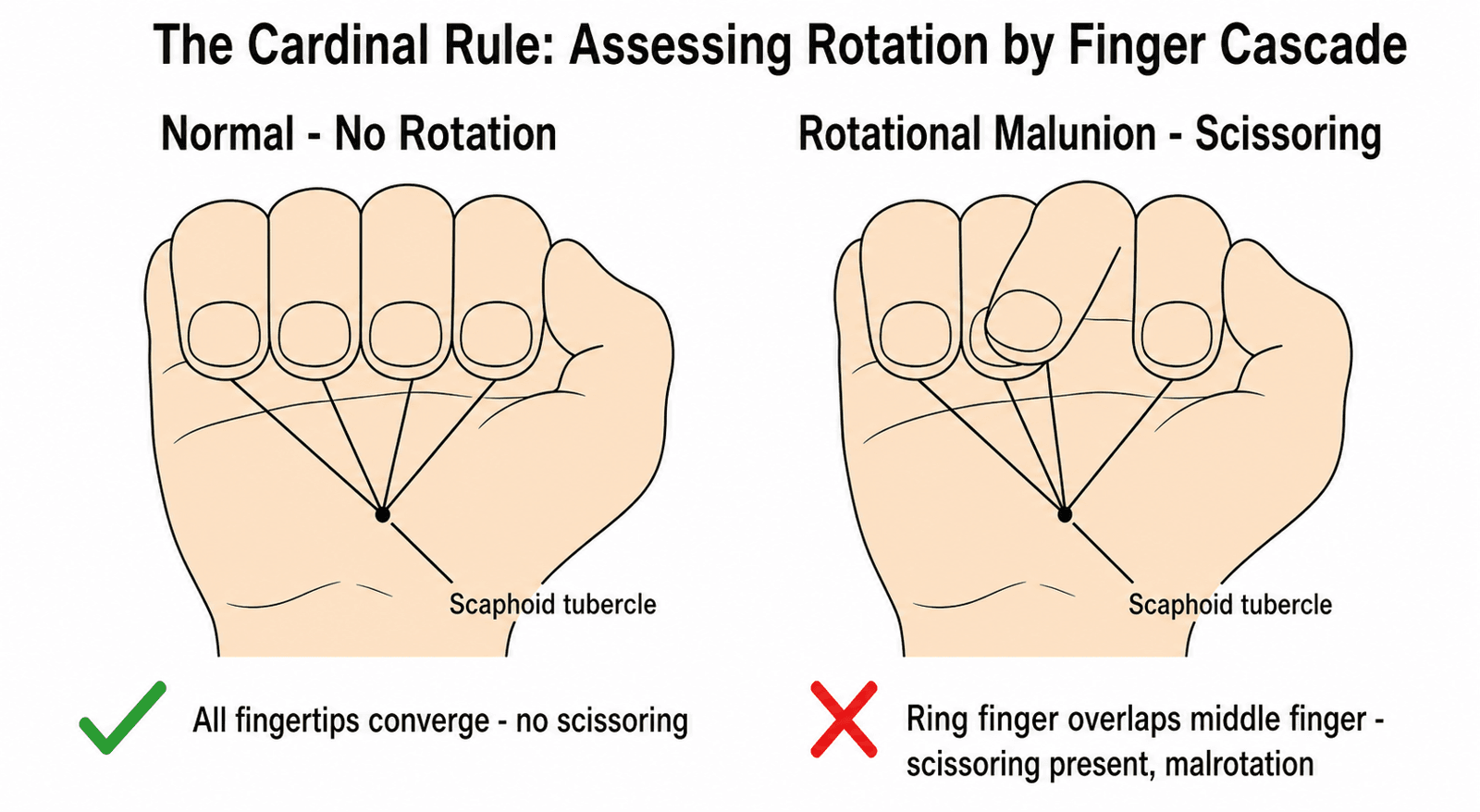
- Cardinal rule: NO degree of rotation is acceptable - fingers must converge to scaphoid tubercle on flexion without scissoring
- 10-10-30-50 rule for acceptable neck angulation: 2nd=10°, 3rd=10°, 4th=30°, 5th=50° (increases ulnarly due to CMC mobility)
- Interossei cause apex dorsal angulation (head drops volar, shaft points dorsally)
- Fight bite (laceration over MCP) = human bite until proven otherwise - Eikenella corrodens - requires formal washout + Augmentin
- Shortening causes ~7° of MCP extensor lag per 2mm (Strauch) - tolerance ~5mm before functional loss
- “Jahss manoeuvre: Flex MCP + PIP to 90°, push dorsally on proximal phalanx to reduce neck fracture
- “Why 4th/5th tolerate more angulation? CMC joints have 20-30° flexion-extension arc to compensate
- “X-ray CANNOT assess rotation - must check clinically (nail planes, finger cascade, scissoring)
- “Never suture a fight bite wound tightly - leave open for drainage
Metacarpal Fractures
The cardinal rule of metacarpal fractures: No degree of rotation is acceptable. Fingers must converge to the scaphoid tubercle on flexion. If they cross (scissoring), surgical correction is needed. Angulation is tolerated progressively from radial to ulnar (2nd < 3rd < 4th < 5th) due to CMC mobility. Boxer's fracture can tolerate up to 40-50 degrees neck angulation.
Deforming Forces
- Origin from shafts
- Flex MCP, Extend IPJ
- In fractures: Flex the distal fragment
- Result: Apex Dorsal Angulation (Head drops volar)
- Index (2nd): less than 10-15° (Rigid CMC)
- Middle (3rd): less than 10-15° (Rigid CMC)
- Ring (4th): less than 30-40° (Mobile CMC)
- Little (5th): less than 50-60° (Mobile CMC) - Boxer's
Why the Difference?
- 4th/5th CMC joints have 20-30° flexion/extension arc
- Allows compensation for fixed deformity (pseudoclawing)
- 2nd/3rd CMC joints are rigid pillars
Overview & Epidemiology
Metacarpal fractures account for roughly 18-44% of all hand fractures (Kollitz), with the 5th metacarpal neck (Boxer's fracture) being the most common pattern in young males. The cardinal rule is that no degree of rotation is acceptable - fingers must converge to the scaphoid tubercle on flexion without scissoring. Acceptable angulation increases from radial to ulnar (10° for 2nd/3rd, 30° for 4th, 50° for 5th) due to progressive CMC joint mobility. The interossei cause apex dorsal angulation, and any laceration over the MCP joint should be treated as a human "fight bite" requiring washout and antibiotics covering Eikenella corrodens.
Fracture Patterns
Metacarpal Fracture Overview
- 18-44% of all hand fractures (Kollitz review); ~88% involve non-thumb metacarpals
- Most common: 5th metacarpal neck (Boxer's fracture)
- Peak incidence: Young males (10-29 years)
- Common mechanisms: Punch, fall, crush
- Rotation is NEVER acceptable (cardinal rule)
- Angulation tolerance increases from radial to ulnar
- Mobile 4th/5th CMC joints compensate for apex dorsal angulation
- Pattern
- Apex dorsal angulation (Boxer's)
- Treatment
- Usually conservative
- Pattern
- Transverse, oblique, spiral
- Treatment
- Assess rotation carefully
- Pattern
- Intra-articular (CMC joint)
- Treatment
- May need surgery if displaced
- Pattern
- Intra-articular (MCP joint)
- Treatment
- Often need ORIF
Pathophysiology & Anatomy
Metacarpal Anatomy
- Five metacarpals (1st = thumb, 2nd-5th = fingers)
- Each has head, neck, shaft, and base
- 2nd and 3rd CMC joints are rigid (fixed pillars)
- 4th and 5th CMC joints are mobile (20-30° arc)
- Interossei muscles originate from shafts
- Extensor tendons run dorsally over MCP joint
- Sagittal bands stabilise extensor over metacarpal head
- CMC Mobility
- Rigid
- Angulation Tolerance
- 10-15°
- CMC Mobility
- Rigid
- Angulation Tolerance
- 10-15°
- CMC Mobility
- Mobile
- Angulation Tolerance
- 30-40°
- CMC Mobility
- Mobile
- Angulation Tolerance
- 50-70°
Fracture Types
Classification by Location
- Head fractures (intra-articular MCP)
- Neck fractures (most common = Boxer's)
- Shaft fractures (transverse, oblique, spiral, comminuted)
- Base fractures (intra-articular CMC or extra-articular)
- Transverse: Prone to angulation, stable in rotation
- Oblique: Intermediate stability
- Spiral: Prone to rotation and shortening
- Comminuted: Unstable, often need surgery
- Deformity Risk
- Apex dorsal angulation
- Fixation Preference
- Plate or IM screws
- Deformity Risk
- Shortening, rotation
- Fixation Preference
- Lag screws
- Deformity Risk
- Rotation, shortening
- Fixation Preference
- Lag screws or plate
- Deformity Risk
- Shortening, instability
- Fixation Preference
- Plate +/- bone graft
Clinical Presentation & Examination
Inspection:
- Swelling (dorsal hand)
- Loss of knuckle prominence (depressed head)
- Rotational Alignment:
- Ask patient to make a fist
- Fingertips should all point to Scaphoid Tubercle
- Look for scissoring/overlap
- Compare fingernail planes (should be parallel)
- Sensation (Digital nerves)
- Perfusion
- "Fight Bite": Laceration over MCP joint from tooth
- Assume infected human bite (Eikenella corrodens)
- Needs washout + antibiotics (Augmentin)
Any laceration over an MCP joint in a young male is a human bite until proven otherwise. The tooth penetrates the joint capsule in flexion, dragging bacteria in. When the finger extends, the tract seals. These require formal washout (often in theatre) and antibiotics covering Eikenella.
Clinical Context: Never suture a fight bite wound tightly.
Investigations & Radiographic Assessment
Imaging Assessment
- PA (posteroanterior) of hand
- Lateral of hand
- Oblique of hand
- Assess all 5 metacarpals systematically
- Fracture location (head, neck, shaft, base)
- Angulation (apex dorsal = most common)
- Shortening (compare to adjacent metacarpal)
- Rotation (cannot assess on X-ray - clinical only)

- Indication
- MCP collateral ligament injury
- What It Shows
- Collateral ligament avulsions
- Indication
- Metacarpal head assessment
- What It Shows
- Articular surface fractures
- Indication
- Complex base fractures
- What It Shows
- CMC joint involvement
Differential Diagnosis
The dorsal hand injury is rarely a true diagnostic dilemma, but the exam tests whether you can separate the metacarpal fracture from look-alikes that change management.
- Distinguishing features
- Apex-dorsal angulation, lost knuckle prominence, punch mechanism
- Why it matters
- Usually conservative; high angulation tolerance
- Distinguishing features
- Laceration over MCP, often a denied bite, joint signs/pus
- Why it matters
- Surgical emergency: washout, never close
- Distinguishing features
- Thumb CMC pain, intra-articular base fracture-dislocation
- Why it matters
- Needs anatomic reduction +/- fixation
- Distinguishing features
- 5th CMC, base displaced by ECU pull
- Why it matters
- Often unstable - pinning/ORIF
- Distinguishing features
- Carpometacarpal step-off, missed on PA, seen on lateral/oblique
- Why it matters
- Easily overlooked; needs reduction
- Distinguishing features
- Extensor subluxation, no fracture on X-ray, painful MCP
- Why it matters
- Soft-tissue injury - splint vs repair, not a fracture
- Distinguishing features
- Tenderness distal to MCP, finger-level deformity
- Why it matters
- Different alignment and rehab principles
Conservative Management
- Stable fractures
- Acceptable angulation
- No rotation
- Buddy Strapping: For stable shaft fractures
- Ulnar Gutter Splint: For 4th/5th Metacarpal
- Radial Gutter Splint: For 2nd/3rd Metacarpal
- Position of Safety (Not for fractures!): Intrinsic plus position usually used for immobilisation, BUT:
- Some evidence suggests buddy taping alone allows earlier return to work for Boxer's fractures.
- 3-4 weeks immobilisation
- X-ray check at 1 week for position
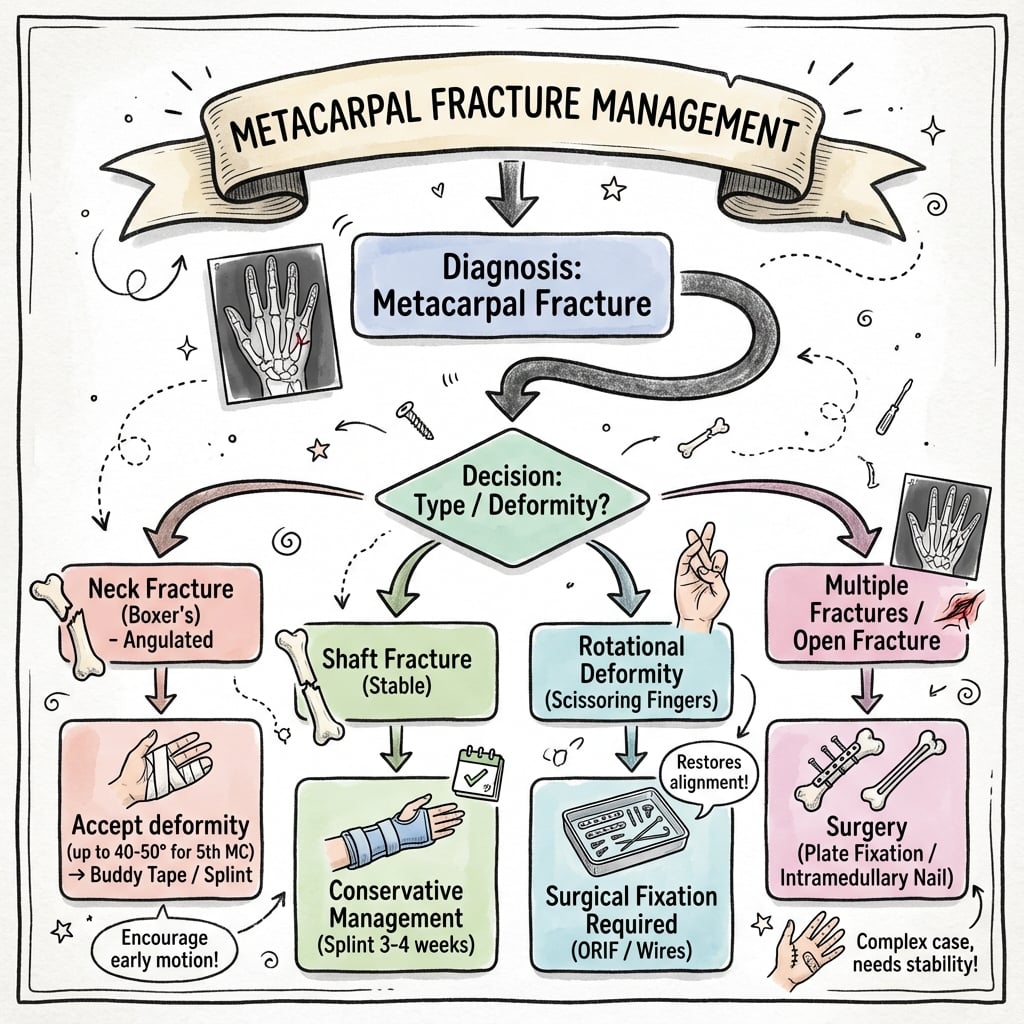
Treatment Algorithm
Treatment Algorithm
- Stable fractures with acceptable angulation
- No rotational deformity
- Closed injury (no fight bite)
- Buddy taping: Simple, allows early motion
- Ulnar gutter splint: 4th/5th metacarpal
- Radial gutter splint: 2nd/3rd metacarpal
- Duration: 3-4 weeks
- ANY rotational deformity (cardinal rule)
- Unacceptable angulation for the ray
- Shortening greater than 5mm
- Open fractures
- Multiple metacarpal fractures
- Intra-articular displacement
- First-Line
- Buddy tape or ulnar gutter
- Surgical Option
- Rarely needed
- First-Line
- Surgery indicated
- Surgical Option
- K-wires or plate
- First-Line
- Often surgery
- Surgical Option
- Lag screws or plate
- First-Line
- Assess stability
- Surgical Option
- K-wires or ORIF
Surgical Management
- Rotational deformity (ANY)
- Unacceptable angulation (e.g., greater than 50° in 5th neck)
- Shortening greater than 5mm (relative)
- Open fractures
- Multiple metacarpal fractures
- Intra-articular displacement
-
K-wire Fixation:
- Retrograde (intramedullary) or Transverse (pinning to adjacent bone)
- Minimally invasive, wire removal later
-
ORIF (Plate/Screws):
- For shaft fractures, unstable patterns
- Anatomical reduction
- Risk: Tendon adhesions, prominent hardware
-
Intramedullary Screw:
- Newer technique for neck/shaft
- Headless compression screw
Metacarpal Head Fractures: the Intra-articular Pattern
The classification and surgical-indication lists repeatedly single out the head fracture as the intra-articular pattern that "often needs ORIF," but it deserves development in its own right because it behaves very differently from the far commoner neck and shaft fractures.
- Metacarpal head fractures are uncommon (of the order of one in a hundred hand fractures), but they involve the small, highly congruent MCP joint, so they carry a real risk of stiffness, articular incongruity and post-traumatic arthritis, and — with comminution — avascular necrosis of the head.
- The index metacarpal head is the most frequently involved, and a laceration over the joint should raise the suspicion of a fight bite with cartilage penetration.
- The metacarpal head has a largely terminal, dorsally entering blood supply, which is why a comminuted head fragment can be devascularised.
epiphyseal fractures; collateral-ligament avulsion fractures; oblique (sagittal, unicondylar) fractures; vertical (coronal-plane) fractures; comminuted fractures; a boxer's neck fracture extending into the head; fractures with bone loss; and fractures associated with joint or soft-tissue loss. The scheme is descriptive rather than prognostic, but it maps directly onto treatment.
- Undisplaced: brief immobilisation followed by early protected motion to preserve the articular cartilage and prevent MCP stiffness.
- Displaced unicondylar (sagittal/coronal) split: open reduction and internal fixation with headless compression screws, mini-fragment screws, K-wires or bioabsorbable pins, aiming for anatomic joint restoration and a construct stable enough for early motion.
- Severely comminuted: internal fixation may be impossible; distraction external fixation using ligamentotaxis maintains joint space and allows motion, with osteochondral reconstruction or arthroplasty reserved for salvage.
A displaced intra-articular metacarpal head fragment (articular step-off of about 1 mm or more, or an unstable unicondylar split) is an indication for open reduction and internal fixation, because an incongruent MCP joint leads to stiffness and early arthritis. Comminuted head fractures carry the highest risk of avascular necrosis given the head's terminal blood supply, and are often better served by distraction external fixation than by attempting rigid internal fixation of small devascularised fragments. Any laceration over the MCP joint with a head fracture is a fight bite until proven otherwise.
Why Multiple and Border-Ray Fractures Are Unstable
The ROMI mnemonic and every operative-indication list flag multiple metacarpal fractures as a reason to operate, but the underlying reason is an anatomical one worth stating explicitly, because it also explains why some isolated fractures are so forgiving.
- Each metacarpal is tethered to its neighbours proximally by the interosseous muscles and distally, at the level of the heads, by the deep transverse metacarpal (intermetacarpal) ligament, which links the volar plates of the index-to-little MCP joints.
- Intact adjacent metacarpals therefore act as internal splints, resisting shortening, angulation and rotation at a fracture in the ray between them. This is why an isolated central (middle or ring) metacarpal shaft fracture is one of the most stable fractures in the hand.
- When two or more adjacent metacarpals are fractured, the splinting buttress is lost on both sides, so the injury is inherently unstable and far more likely to shorten, angulate and rotate — hence the lower threshold for fixation and the place of "multiple fractures" on the operative list.
- The border rays (index and little finger) are held by the intermetacarpal ligament on only one side, so isolated second and fifth metacarpal fractures are less well splinted and more prone to displacement and malrotation than the well-protected central rays.
If asked why an isolated third or fourth metacarpal shaft fracture is usually treated non-operatively but a double or triple metacarpal fracture is fixed, the answer is the loss of the splinting effect of the adjacent intact rays and the deep transverse intermetacarpal ligament. The same principle explains why border-ray (index and little finger) fractures displace and rotate more readily than central-ray fractures, and why any suspicion of instability lowers the threshold for operative fixation.
Complications
Complications of Metacarpal Fractures
Rotational malunion: every 5° of rotation at the metacarpal produces ~1.5cm of fingertip overlap; correct with a dorsal-approach derotation osteotomy and plate fixation. Stiffness from tendon adhesions is the most common post-surgical complication - mitigate with stable fixation and early protected motion. Hardware issues: dorsal plates cause adhesions/prominence, K-wires cause pin-site infection and migration.
Postoperative Care
Rehabilitation Protocol
- Splint protection (ulnar or radial gutter)
- Elevation to reduce swelling
- Active finger ROM if fixation stable
- Avoid heavy loading
- K-wire removal at 4-6 weeks
- Wean from splint
- Active ROM exercises
- Hand therapy referral
- Progressive grip strengthening
- Return to light activities
- Functional exercises
- Immobilisation
- Immediate ROM
- Return to Work
- 1-2 weeks light duties
- Immobilisation
- 3-4 weeks
- Return to Work
- 4-6 weeks
- Immobilisation
- 4-6 weeks to removal
- Return to Work
- 6-8 weeks
- Immobilisation
- 1-2 weeks splint
- Return to Work
- 8-12 weeks manual
Outcomes
Functional Outcomes
- Excellent outcomes for most metacarpal fractures
- 95% union rate with appropriate treatment
- Stiffness is main complication, especially after surgery
- Excellent function even with radiographic malunion
- Loss of knuckle prominence is cosmetic only
- Surgery not superior to conservative for typical patterns
- Good outcomes if rotation corrected
- Stiffness risk higher with plate fixation
- K-wires associated with less stiffness but less rigid fixation
- Union Rate
- Greater than 95%
- Main Concern
- Cosmetic only
- Union Rate
- Greater than 95%
- Main Concern
- Pin complications
- Union Rate
- Greater than 95%
- Main Concern
- Stiffness, adhesions
- Union Rate
- 90-95%
- Main Concern
- MCP arthritis
Guidelines, Registries & Global Practice
Global Epidemiology
- Metacarpal fractures are 18-44% of all hand fractures; the hand accounts for ~20% of all skeletal fractures presenting to emergency departments worldwide.
- Strong young-male preponderance (peak 10-29 years), reflecting interpersonal violence/punch and sports mechanisms; an alcohol-related, weekend, urban pattern is reported across high- and middle-income settings.
- The fifth metacarpal neck (Boxer's fracture) is the single most common pattern; non-thumb metacarpals comprise ~88% of metacarpal fractures.
- Position on Boxer's & shaft fractures
- Non-operative for most isolated closed neck/shaft fractures with acceptable alignment
- Emphasis
- Rotation and intra-articular displacement drive surgery
- Position on Boxer's & shaft fractures
- Functional treatment and early motion for stable Boxer's fractures
- Emphasis
- Avoid over-immobilisation; hand-therapy access
- Position on Boxer's & shaft fractures
- Operative options (lag screw, plate, antegrade IM nail/screw) defined by pattern and stability
- Emphasis
- Anatomic reduction of rotation; absolute vs relative stability
- Position on Boxer's & shaft fractures
- Conservative-first; IM techniques increasingly favoured when fixation needed
- Emphasis
- Minimise stiffness, early rehabilitation
There is broad international agreement (and no major guideline disagreement) on the core principles: zero tolerance of rotation, ray-dependent angulation thresholds, and conservative-first management of stable fractures. Differences are largely in surgical technique preference rather than indications.
Controversies & Areas of Uncertainty
- Angulation thresholds are eminence-based, not evidence-based. The widely quoted 10-10-30-50 (or 10-20-30-40) figures vary between texts; the Cochrane review (Poolman) found no high-quality data defining a precise cut-off, and many patients tolerate angulation well beyond classic limits with good function.
- Best non-operative method is unsettled. Poolman found no regimen (buddy taping, soft wrap, ulnar gutter, functional brace) superior to another. Practice varies from immediate mobilisation to 3-4 weeks of splinting.
- IM screw vs K-wire vs plate. Antegrade headless IM screws give excellent union and motion (Beck), but evidence is largely Level III-IV; concerns include articular cartilage violation at the entry point and cost. No adequately powered RCT defines the optimal implant.
- Shortening tolerance. Strauch quantifies ~7° extensor lag per 2 mm shortening, but the clinically "acceptable" limit (commonly cited as ~5 mm) is extrapolated, and MCP hyperextension may compensate.
- Fight-bite antibiotic duration and washout setting. Universal agreement on washout plus amoxicillin-clavulanate, but optimal antibiotic duration and whether minor early injuries can be managed without theatre remain debated.
Conservative Treatment of Fifth Metacarpal Neck Fractures (Cochrane)
- Five randomised/quasi-randomised trials, 252 participants, comparing functional treatment with immobilisation
- No single non-operative regimen was statistically superior to another in result
- Trials were of limited quality and size; validated hand function was not reported in any study
Rotational Deformity Following Metacarpal Fracture
- Prospective series of 91 patients with 98 metacarpal fractures
- A quarter had minor rotation under 10 degrees; only 5 had more, and just 2 needed operative correction for rotational instability
- Rotation must be assessed with an end-on view of the fingernail, as MCP joint motion is often restricted after fracture
Effect of Metacarpal Shortening on the Extensor Mechanism
- Cadaver model (9 hands), 2nd and 5th metacarpal shaft fractures shortened in 2 mm increments to 10 mm
- Average of 7 degrees of MCP extensor lag produced for every 2 mm of metacarpal shortening
- MCP hyperextension capacity may clinically compensate for some of this lag
Human Bite Wounds and Eikenella corrodens
- Clenched-fist (fight-bite) injuries to the hand carry far higher infection and complication rates than bites elsewhere
- Infections are polymicrobial; Eikenella corrodens is the characteristic pathogen of human bites
- Hand bites warrant aggressive irrigation/debridement and beta-lactam plus beta-lactamase-inhibitor cover
Intramedullary Screw Fixation of Metacarpal Fractures
- Systematic review of 9 studies, 169 metacarpal fractures (74% small finger; mostly neck fractures)
- Radiographic union in 100% of reported cases; mean MCP flexion 86 degrees and grip 96% of contralateral
- No serious complications; only minor complications including asymptomatic hardware removal
Metacarpal Fractures: Treatment and Complications
- Metacarpal fractures comprise 18-44% of all hand fractures; the fifth finger is most commonly involved
- Around 88% of metacarpal fractures involve the non-thumb metacarpals; most are simple, closed and stable
- Persistent controversy and limited high-level evidence to define the optimal treatment algorithm
Key Mnemonics
10-10-30-50Acceptable Angulation
Hook:Increases ulnarly due to mobile CMCs - 1-1-3-5 easy to remember
ROMISurgical Indications
Hook:ROMI goes to theatre - Rotation, Open, Multiple, Intra-articular
WASHFight Bite Management
Hook:WASH the fight bite properly - don't believe the glass story
MCQ Practice Points
Q: What is the maximum acceptable angulation for a fifth metacarpal neck fracture (boxer's fracture) treated non-operatively?
A: Up to 70 degrees of apex dorsal angulation is acceptable for fifth metacarpal neck fractures due to the compensatory motion at the 4th and 5th CMC joints (30-40 degrees of flexion-extension). The fourth metacarpal accepts up to 40 degrees, the third metacarpal 15 degrees, and the second metacarpal (index) only 10-15 degrees because the 2nd and 3rd CMC joints have minimal motion. Rotational deformity is never acceptable and always requires correction.
Q: What is the indication for surgical fixation of metacarpal shaft fractures?
A: Surgical indications include: Rotational malrotation (any degree - clinical scissoring), angulation exceeding acceptable limits (varies by ray), multiple metacarpal fractures, open fractures, intra-articular fractures with displacement, and shortening greater than 5mm (causes extensor lag). Spiral fractures are prone to rotational deformity while transverse fractures are prone to angular deformity. Lag screws are ideal for long oblique/spiral patterns; plates for transverse/short oblique/comminuted patterns.
Q: How do you clinically assess for rotational malalignment in metacarpal fractures?
A: Finger cascade test: With the MCP joints flexed, all fingers should point toward the scaphoid tubercle. Scissoring: Overlapping of fingers during flexion indicates malrotation. Each 5 degrees of rotational deformity at the metacarpal level results in approximately 1.5cm of digital overlap at the fingertip. Compare tenodesis effect (passive wrist extension causes finger flexion) to the contralateral hand. Rotational deformity is the most poorly tolerated malunion and requires correction.
Q: What is the difference between a Bennett's fracture and a Rolando's fracture?
A: Bennett's fracture: Intra-articular fracture-dislocation at the thumb CMC joint with a single volar-ulnar fragment attached to the AOL while the metacarpal shaft subluxates radially and proximally due to APL pull. Rolando's fracture: Comminuted intra-articular fracture at the same location with T or Y pattern (at least 3 fragments). Both require anatomic reduction. Bennett's is typically fixed with K-wires or screw, while Rolando's may need plate fixation or external fixation for severe comminution.
Q: What is the reverse Bennett fracture and how is it managed?
A: Reverse Bennett fracture is an intra-articular fracture-dislocation at the fifth CMC joint with a volar-ulnar fragment remaining attached to the hamate while the metacarpal base displaces dorsally and proximally (pulled by ECU). Also called a baby Bennett. Treatment follows similar principles to thumb Bennett's: closed reduction and percutaneous pinning if anatomic reduction achieved, or ORIF for irreducible or significantly displaced fractures. Maintain reduction with splinting in slight flexion.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old rugby player presents with a swollen right hand after punching a wall. X-ray shows a 5th metacarpal neck fracture with 40 degrees of volar angulation. There is no rotational deformity clinically. How do you manage this?”
“A 30-year-old presents 5 days after a fall onto his hand. X-rays show a short oblique fracture of the third metacarpal shaft with minimal displacement and approximately 15 degrees of apex dorsal angulation. However, on clinical examination, when he makes a fist, you notice that the middle finger crosses over the index finger and the fingernail plane is rotated compared to the adjacent fingers. What is your management?”
“A 24-year-old presents to the emergency department 3 days after 'cutting his hand on glass' at a bar. He has a 1cm laceration over the dorsum of his right 3rd MCP joint that he cleaned himself. The wound now has purulent discharge, the MCP joint is swollen and erythematous, and he has pain and restricted motion. He is febrile at 38.5 degrees. X-rays show soft tissue swelling but no fracture or gas. What is your assessment and management?”
Acceptable Angulation
- Index/Middle: less than 10-15 degrees (Rigid)
- Ring: less than 30-40 degrees
- Little: less than 50-70 degrees (Mobile)
Operation Indications
- ANY Rotation (fingers scissor)
- Open fracture
- Multiple fractures
- Intra-articular step-off
Fight Bite
- Laceration over MCP joint
- Eikenella corrodens
- Formal washout required
Evidence Base
Key Studies
- Conservative treatment effective for Boxer's fractures
- No difference between immobilisation methods
- Surgery adds risk without clear benefit for standard patterns
- Rotation tolerance: Zero degrees acceptable
- 5° rotation = 1.5cm fingertip overlap
- Shortening greater than 5mm causes extensor lag
- Key Finding
- Conservative = surgical for Boxer's
- Clinical Impact
- Avoid unnecessary surgery
- Key Finding
- K-wire biomechanics effective
- Clinical Impact
- K-wires are reasonable fixation
- Key Finding
- Review of treatment options
- Clinical Impact
- Algorithm-based approach
References
- Ali A, et al. Biomechanical stability of intramedullary K-wire fixation of metacarpal neck fractures. J Hand Surg Br. 2005.
- Kollitz KM, et al. Metacarpal fractures: treatment and complications. Hand (NY). 2014.